
Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery

 ,
,  , , ,
, , ,  ,
, 
Abstract
1. Introduction
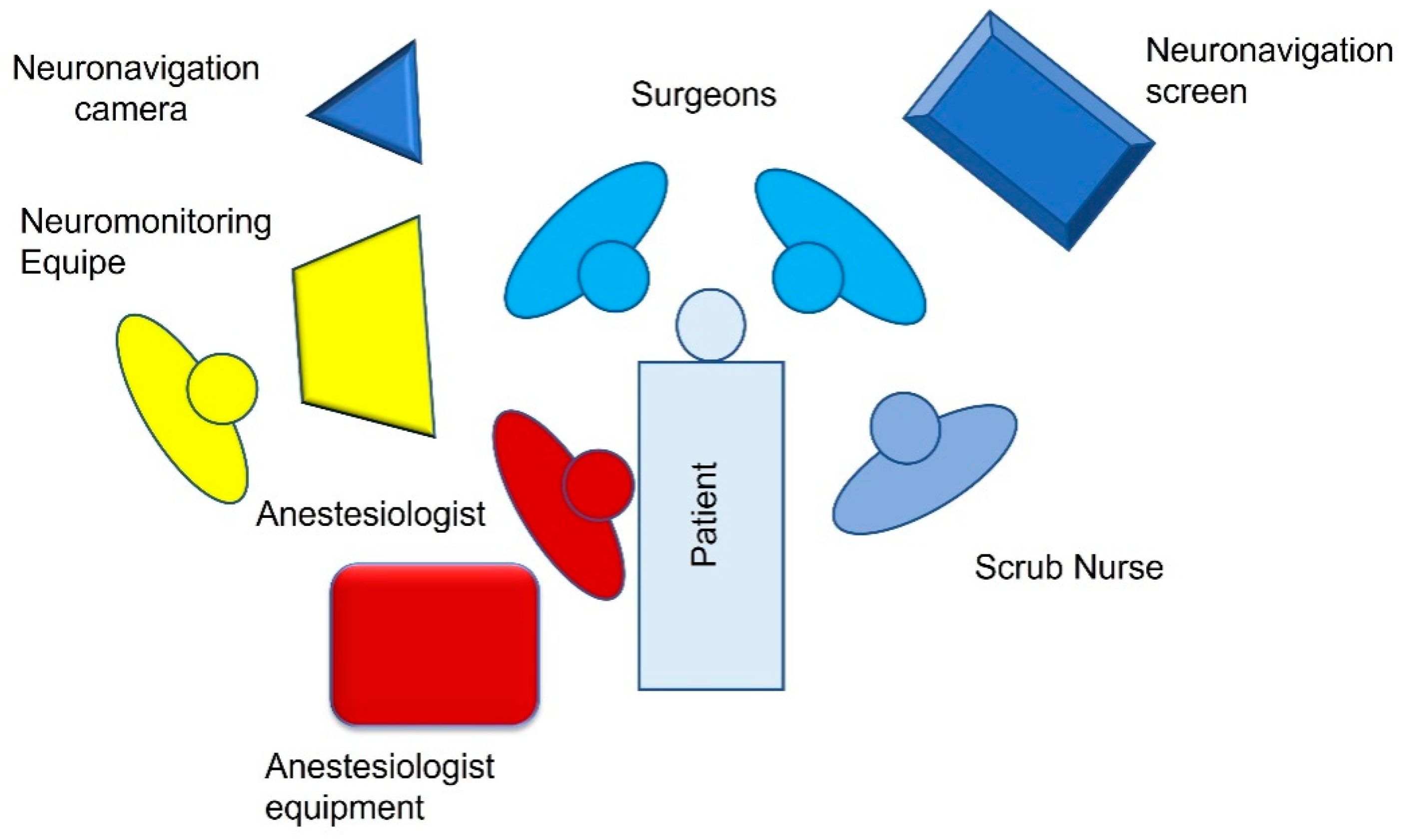
2. Operating Room Tools
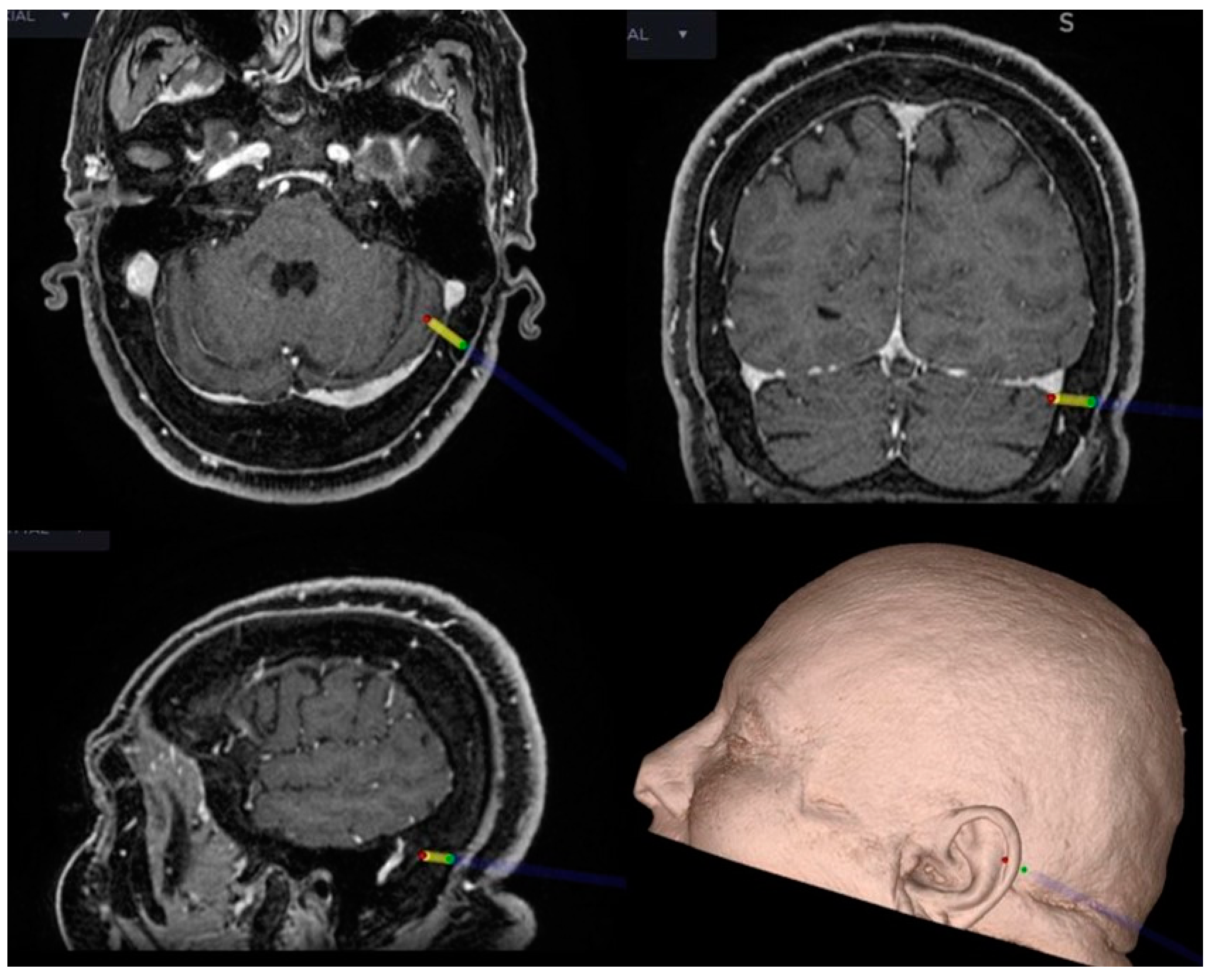
2.1. Neuronavigation
2.2. Intraoperative Neuromonitoring (IONM)
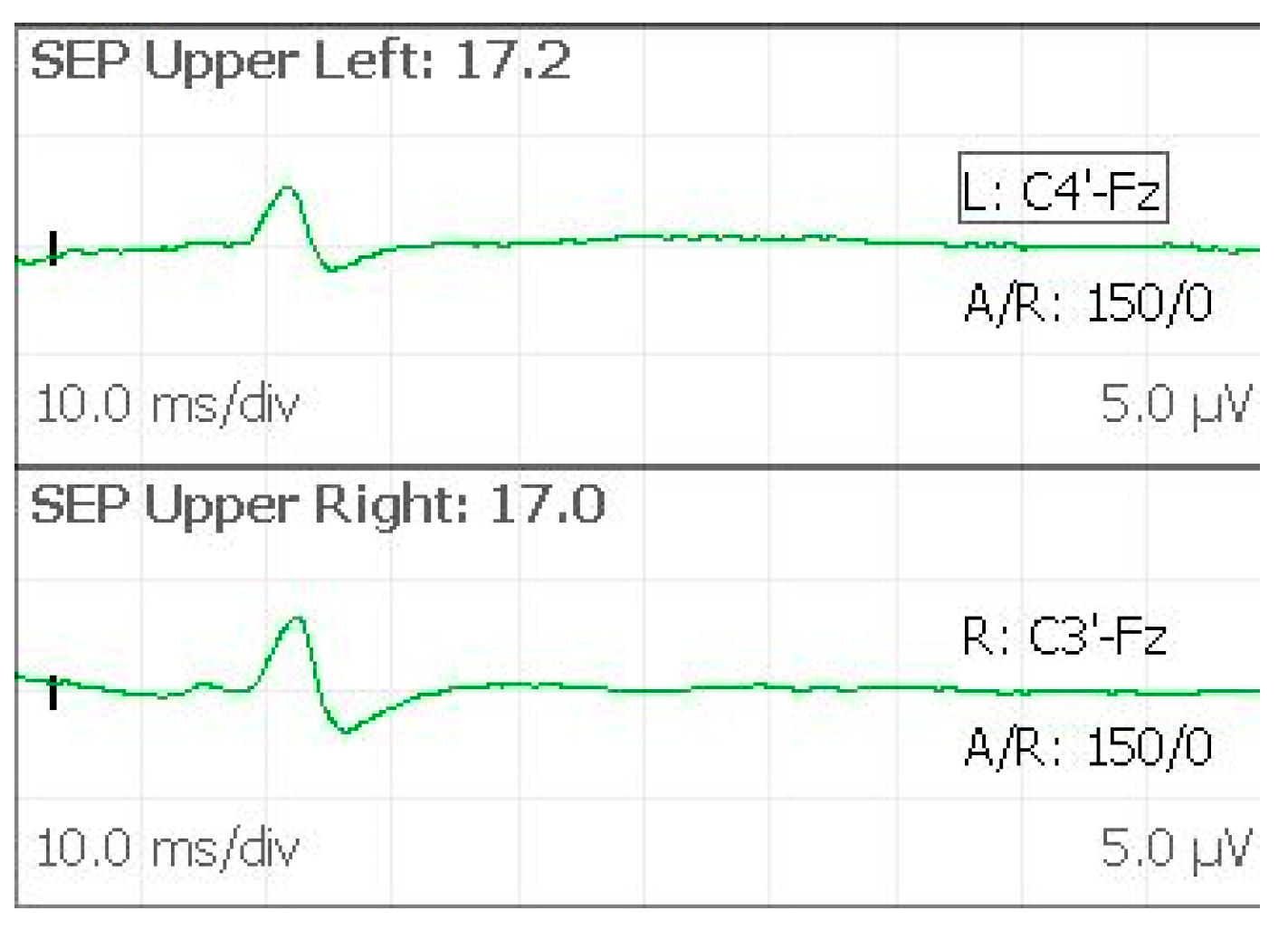
- Somatosensory evoked potentials (SEPs);
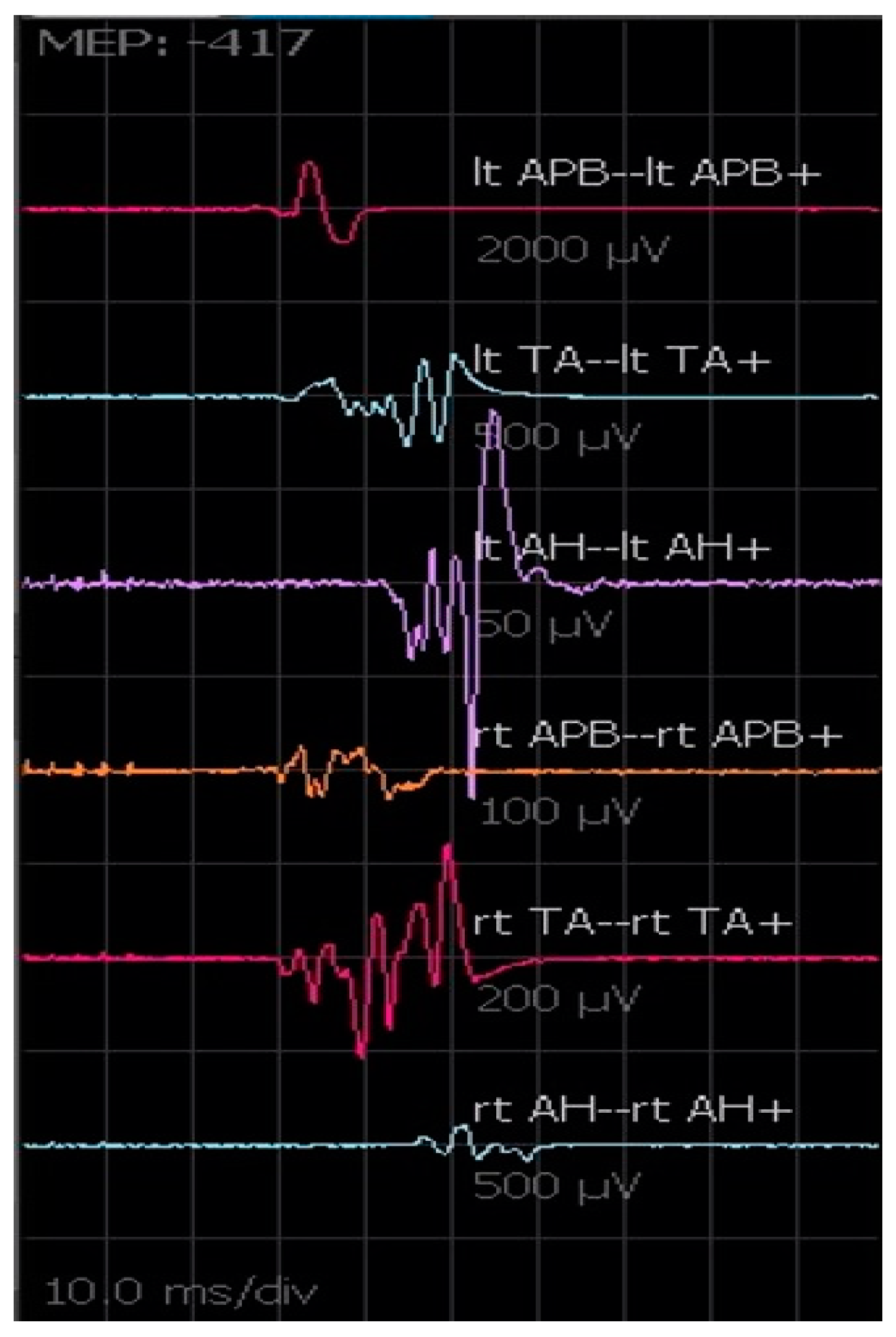
- Motor evoked potentials (MEPs);
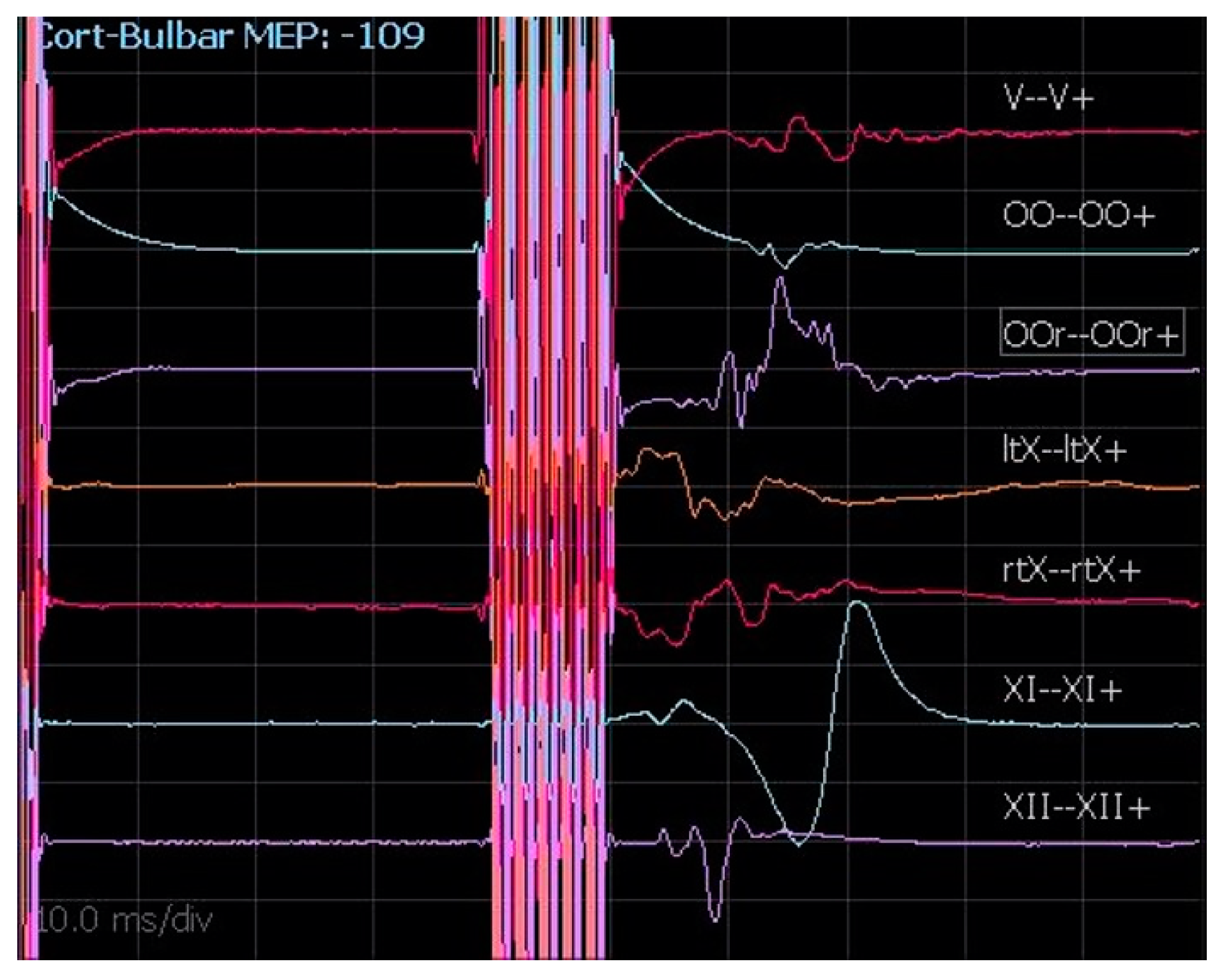
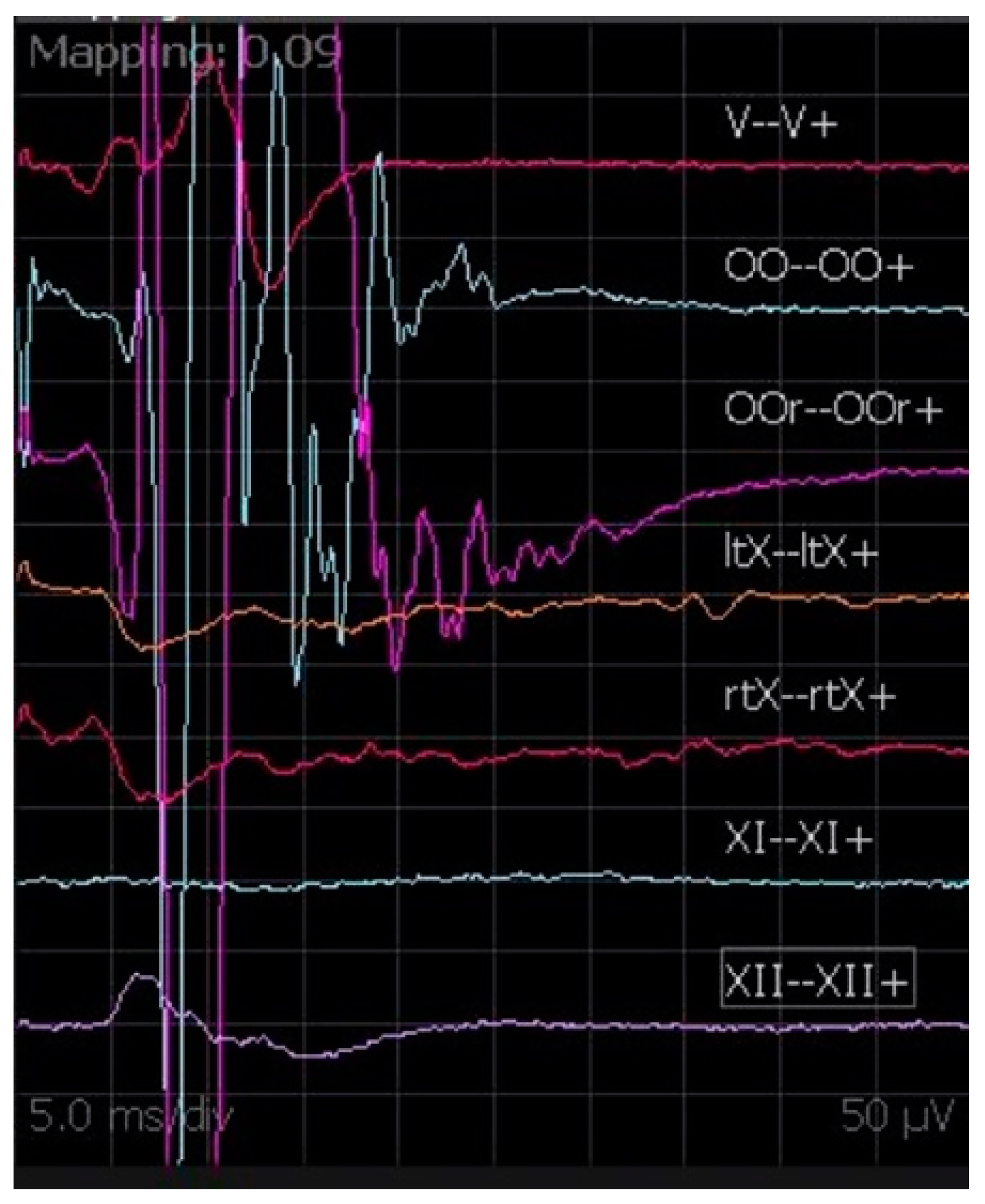
- Cortico-bulbar motor evoked potentials (cMEPs);
- Brainstem auditory evoked potentials (BAEPs);
- Free-running electromyography (EMG);
- Lateral spread response (LSR);
- Direct electrical stimulation (DES) of the nerves.
2.2.1. Electrode Placements
- Biceps brachii;
- Abductor pollicisbrevis muscles;
- Tibialis anterior;
- Quadriceps;
- Abductor hallucis.
- Orbicularis oris (VII C.N);
- Orbicularis oculi (VII C.N);
- Masseter (V C.N);
- Trapezius (IX C.N);
- Vocal cords (using The NIM TriVantage® EMG Tube (Medtronic)) (X C.N);
- Tongue (XII C.N).
2.2.2. SEPs
2.2.3. MEPs
2.2.4. cMEPs
2.2.5. BAEPs
2.2.6. Free-Running EMG
2.2.7. LSR
2.2.8. DES
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaye, A.H.; Briggs, R.J.; Morokoff, A.P. Acoustic neurinoma (vestibular schwannoma). Brain Tumors 2012, 518–569. [Google Scholar] [CrossRef]
- Rhoton, A.L., Jr. The cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach. Neurosurgery 2000, 47 (Suppl. 3), S93–S129. [Google Scholar] [CrossRef] [PubMed]
- Sop, F.Y.L.; D’Ercole, M.; Izzo, A.; Rapisarda, A.; Ioannoni, E.; Caricato, A.; Olivi, A.; Montano, N. The Impact of Neuronavigation on the Surgical Outcome of Microvascular Decompression for Trigeminal Neuralgia. World Neurosurg. 2021, 149, 80–85. [Google Scholar] [CrossRef]
- Lin, J.; Zhang, Y.; Peng, R.; Ji, X.; Luo, G.; Luo, W.; Wang, M.; Zhu, M.; Sun, X. Preoperative Imaging and Microscopic Navigation During Surgery Can Avoid Unnecessarily Opening the Mastoid Air Cells through Craniotomy Using the Retrosigmoid Approach. World Neurosurg. 2018, 121, e15–e21. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.; Gan, Y.-C. Anatomical localization of the transverse-sigmoid sinus junction: Comparison of existing techniques. Surg. Neurol. Int. 2019, 10, 186. [Google Scholar] [CrossRef]
- Dolati, P.; Gokoglu, A.; Eichberg, D.; Zamani, A.; Golby, A.; Al-Mefty, O. Multimodal navigated skull base tumor resection using image-based vascular and cranial nerve segmentation: A prospective pilot study. Surg. Neurol. Int. 2015, 6, 172. [Google Scholar] [CrossRef]
- Da Silva, E.B.; Leal, A.G.; Milano, J.B.; Da Silva, L.F.M.; Clemente, R.S.; Ramina, R. Image-guided surgical planning using anatomical landmarks in the retrosigmoid approach. Acta Neurochir. 2009, 152, 905–910. [Google Scholar] [CrossRef]
- Bir, S.C.; Konar, S.K.; Maiti, T.K.; Thakur, J.D.; Guthikonda, B.; Nanda, A. Utility of Neuronavigation in Intracranial Meningioma Resection: A Single-Center Retrospective Study. World Neurosurg. 2016, 90, 546–555.e1. [Google Scholar] [CrossRef]
- Auricchio, A.M.; D’Alessandris, Q.G.; Mattogno, P.P.; Marquez, E.M.F.; Lauretti, L. Ct-based intraoperative navigation for quick identification of the stylomastoid foramen during hypoglossal-facial nerve anastomosis. Turk. Neurosurg. 2022; ahead of print. [Google Scholar] [CrossRef]
- Monitoraggio Neurofisiologico Intraoperatorio in Neurochirurgia Raccomandazionidel Gruppo di Lavoro Intersocietario Società Italiana di Neurofisiologia Clinica (SINC)—Società Italiana di Neurochirurgia (SINch). [Online]. Available online: https://www.sinc-italia.it/pdf/DOCUMENTO_INTERSOCIETARIO_IOM_2016.pdf (accessed on 1 May 2022).
- Jafarzadeh, F.; Bashir, M.; Yan, T.; Harrington, D.; Field, M.L.; Kuduvalli, M.; Oo, A.; Desmond, M. Setting up and utilizing a service for measuring perioperative transcranial motor evoked potentials during thoracoabdominal aortic surgery and thoracic endovascular repair. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 748–756. [Google Scholar] [CrossRef][Green Version]
- Levin, K.H.; Chauvel, P. (Eds.) Clinical Neurophysiology: Basis and Technical Aspects; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Nuwer, M.R.; Dawson, E.G.; Carlson, L.G.; Kanim, L.E.; Sherman, J.E. Somatosensory evoked potential spinal cord monitoring reduces neurologic deficits after scoliosis surgery: Results of a large multicenter survey. Electroencephalogr. Clin. Neurophysiol. Potentials Sect. 1995, 96, 6–11. [Google Scholar] [CrossRef]
- Kombos, T.; Suess, O.; Ciklatekerlio, Ö.; Brock, M. Monitoring of intraoperative motor evoked potentials to increase the safety of surgery in and around the motor cortex. J. Neurosurg. 2001, 95, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Sloan, T.B.; Jäntti, V. Anesthetic effects on evoked potentials. In Handbook of Clinical Neurophysiology; Elsevier: Amsterdam, The Netherlands, 2008; Volume 8, pp. 94–126. [Google Scholar] [CrossRef]
- Calancie, B. Intraoperative Neuromonitoring and Alarm Criteria for Judging MEP Responses to Transcranial Electric Stimulation. J. Clin. Neurophysiol. 2017, 34, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.M.; Stifano, V.; D’Alessandris, Q.G.; Menna, G.; Burattini, B.; Di Domenico, M.; Izzo, A.; D’Ercole, M.; Lauretti, L.; Olivi, A.; et al. Intraoperative Corticobulbar Motor Evoked Potential in Cerebellopontine Angle Surgery: A Clinically Meaningful Tool to Predict Early and Late Facial Nerve Recovery. Neurosurgery 2022, 91, 406–413. [Google Scholar] [CrossRef]
- Morota, N.; Ihara, S.; Deletis, V. Intraoperative neurophysiology for surgery in and around the brainstem: Role of brainstem mapping and corticobulbar tract motor-evoked potential monitoring. Child’s Nerv. Syst. 2010, 26, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Deletis, V.; Fernández-Conejero, I.; Ulkatan, S.; Rogić, M.; Carbó, E.L.; Hiltzik, D. Methodology for intra-operative recording of the corticobulbar motor evoked potentials from cricothyroid muscles. Clin. Neurophysiol. 2011, 122, 1883–1889. [Google Scholar] [CrossRef]
- Phillips, D.J.; Kobylarz, E.J.; De Peralta, E.T.; Stieg, P.E.; Selesnick, S.H. Predictive Factors of Hearing Preservation After Surgical Resection of Small Vestibular Schwannomas. Otol. Neurotol. 2010, 31, 1463–1468. [Google Scholar] [CrossRef]
- Yamakami, I.; Yoshinori, H.; Saeki, N.; Wada, M.; Oka, N. Hearing preservation and intraoperative auditory brainstem response and cochlear nerve compound action potential monitoring in the removal of small acoustic neurinoma via the retrosigmoid approach. J. Neurol. Neurosurg. Psychiatry 2009, 80, 218–227. [Google Scholar] [CrossRef]
- López, J.R.; Legatt, A.D. Monitoring surgery around the cranial nerves. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2022; pp. 319–351. [Google Scholar] [CrossRef]
- Strommen, J.A.; Crum, B.A. Intraoperative monitoring with free-running EMG. In Handbook of Clinical Neurophysiology; Elsevier: Amsterdam, The Netherlands, 2008; Volume 8, pp. 396–403. [Google Scholar] [CrossRef]
- Hatem, J.; Sindou, M.; Vial, C. Intraoperative monitoring of facial EMG responses during microvascular decompression for hemifacial spasm. Prognostic value for long-term outcome: A study in a 33-patient series. Br. J. Neurosurg. 2001, 15, 496–499. [Google Scholar] [CrossRef]
- Miller, L.; Miller, V.M. Safety and effectiveness of microvascular decompression for treatment of hemifacial spasm: A systematic review. Br. J. Neurosurg. 2011, 26, 438–444. [Google Scholar] [CrossRef]
- Menna, G.; Battistelli, M.; Rapisarda, A.; Izzo, A.; D’Ercole, M.; Olivi, A.; Montano, N. Factors Related to Hemifacial Spasm Recurrence in Patients Undergoing Microvascular Decompression—A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 583. [Google Scholar] [CrossRef] [PubMed]
- Goldbrunner, R.H.; Schlake, H.-P.; Milewski, C.; Tonn, J.-C.; Helms, J.; Roosen, K. Quantitative Parameters of Intraoperative Electromyography Predict Facial Nerve Outcomes for Vestibular Schwannoma Surgery. Neurosurgery 2000, 46, 1140–1148. [Google Scholar] [CrossRef] [PubMed]
- Stechison, M.T.; Møller, A.; Lovely, T.J. Intraoperative Mapping of the Trigeminal Nerve Root: Technique and Application in the Surgical Management of Facial Pain. Neurosurgery 1996, 38, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Arlt, F.; Kasper, J.; Winkler, D.; Jähne, K.; Fehrenbach, M.K.; Meixensberger, J.; Sander, C. Facial Nerve Function After Microsurgical Resection in Vestibular Schwannoma under Neurophysiological Monitoring. Front. Neurol. 2022, 13, 850326. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stimulation | Registration | |
|---|---|---|
| SEPs | single pulse, 300–500 µs pulse duration 4.1 Hz; 10–25 mA | C3′–Fz (right stimulus) C4′–Fz (left stimulus) |
| MEPs | train of stimuli 5–7 pulse 500 µs pulse duration 250–500 Hz; 150–300 V | C1–C2 (anodal) |
| cMEPs | single pulse 350–500 µs; train of pulses 4–7 stimuli, 350–500 µs, 500–700 Hz, delivered at 40 ms from the first single pulse; 75–150 V | C3-Fz (right cranial nerves) C4-Fz (left cranial nerves) |
| Causes of SEPs Variation | |
|---|---|
| Technical | Electrode disconnection |
| Equipment malfunction | |
| Local interference | |
| Systemic | Hypoxia |
| Hypotension | |
| Surgical | Direct blunt trauma Excessive compression or traction Thermic damage Hypoperfusion |
| Anesthesiological | Propofol bolus Halogenated inhalational agents NO2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izzo, A.; Stifano, V.; Della Pepa, G.M.; Di Domenico, M.; D'Alessandris, Q.G.; Menna, G.; D'Ercole, M.; Lauretti, L.; Olivi, A.; Montano, N. Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery. Brain Sci. 2022, 12, 1167. https://doi.org/10.3390/brainsci12091167
Izzo A, Stifano V, Della Pepa GM, Di Domenico M, D'Alessandris QG, Menna G, D'Ercole M, Lauretti L, Olivi A, Montano N. Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery. Brain Sciences. 2022; 12(9):1167. https://doi.org/10.3390/brainsci12091167
Chicago/Turabian StyleIzzo, Alessandro, Vito Stifano, Giuseppe Maria Della Pepa, Michele Di Domenico, Quintino Giorgio D'Alessandris, Grazia Menna, Manuela D'Ercole, Liverana Lauretti, Alessandro Olivi, and Nicola Montano. 2022. "Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery" Brain Sciences 12, no. 9: 1167. https://doi.org/10.3390/brainsci12091167
APA StyleIzzo, A., Stifano, V., Della Pepa, G. M., Di Domenico, M., D'Alessandris, Q. G., Menna, G., D'Ercole, M., Lauretti, L., Olivi, A., & Montano, N. (2022). Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery. Brain Sciences, 12(9), 1167. https://doi.org/10.3390/brainsci12091167