
Apathy in Parkinson’s Disease: Defining the Park Apathy Subtype


Abstract
1. Introduction
2. Materials and Methods
3. Prevalence of Apathy during the Disease Course

{kind=link}
{kind=link}
| Author (Year) | Rate of Apathy (%) | Disease Stage (Mean ± SD (Years)) | Measuring Tool |
|---|---|---|---|
| Prodromal stage | |||
| Pont-Sunyer et al. (2015) [2] | 50% | −10–2 years | Patient perception |
| Gaenslen et al. (2011) [54] | 23.7% | −8.8 years | Patient perception |
| Darweesh et al. (2017) [53] | NA (case-control) | −7.7 years | IADL–traveling subscore |
| Durcan et al. (2019) [55] | 14.3% | −2.1–0.7 years | NMSQuest |
| High-risk populations | |||
| Barber et al. (2018) [43] | 46% | RBD | LARS |
| De novo, untreated | |||
| De La Riva et al. (2014) [39] | 16.7% | ±0.5 | UPDRS |
| Hinkle et al. (2021) [11] | 16.9% | 0.5 ± 0.5 | UPDRS |
| Liu et al. (2017) [37] | 17.29% * | 1.26 ± 1.25 | LARS |
| Dujardin et al. (2014) [4] | 13.7% * | 1.3 ± 0.9 | LARS |
| Oh et al. (2021) [41] | 30.1% | 1.6 ± 1.9 | NPI |
| Santangelo et al. (2015) [30] | 33.3% | <2 | Diagnostic criteria [66] |
| Cho et al. (2018) [38] | 58.8% | 2.1 ± 1.97 | NMSS |
| Leiknes et al. (2010) [20] | 29.1% | 2.3 [0.4–10] | NPI |
| Early disease stage | |||
| Benito-León et al. (2012) [21] | 21.7% * | 1.3 ± 0.6 | LARS |
| Cubo et al. (2012) [22] | 33.4% | 1.3 ± 0.6 | LARS |
| Ou et al. (2021) [23] | 18.6% | 1.5 | LARS |
| De La Riva (2014) [39] | 30.2% | ±3 | UPDRS |
| Mild disease | |||
| Isella et al. (2002) [25] | 43.3% | 4.9 ± 4.4 | AES-S |
| Eglit et al. (2021) [29] | 71.7% | 5.5 ± 5.2 | AS |
| Kulisevsky et al. (2008) [26] | 48.3% | 5.65 ± 4.94 | NPI |
| Lieberman et al. (2006) [28] | 44% * | 6.2 ± 5.9 | NPI |
| Oguru et al. (2010) [27] | 17% * | 6.3 ± 4.4 | AS |
| Kirsch-Darrow et al. (2006) [24] | 28.8% * | 6.4 ± 5.7 | AES |
| Butterfield et al. (2010) [33] | 14.7% * | 7.07 ± 4.96 | AES-S |
| Kirsch-Darrow et al. (2009) [31] | 31.4% * | 8.1 ± 5.9 | AS |
| Advanced disease | |||
| Aarsland et al. (1999) [34] | 16.5% 4.3% * | 12.6 ± 5.1 | NPI |
| Stella et al. (2009) [32] | 38% | 12.7 ± 6.2 | NPI |
| Pedersen et al. (2009) [14] | 13.9% | 13.0 ± 4.7 | NPI |
4. Pathophysiology
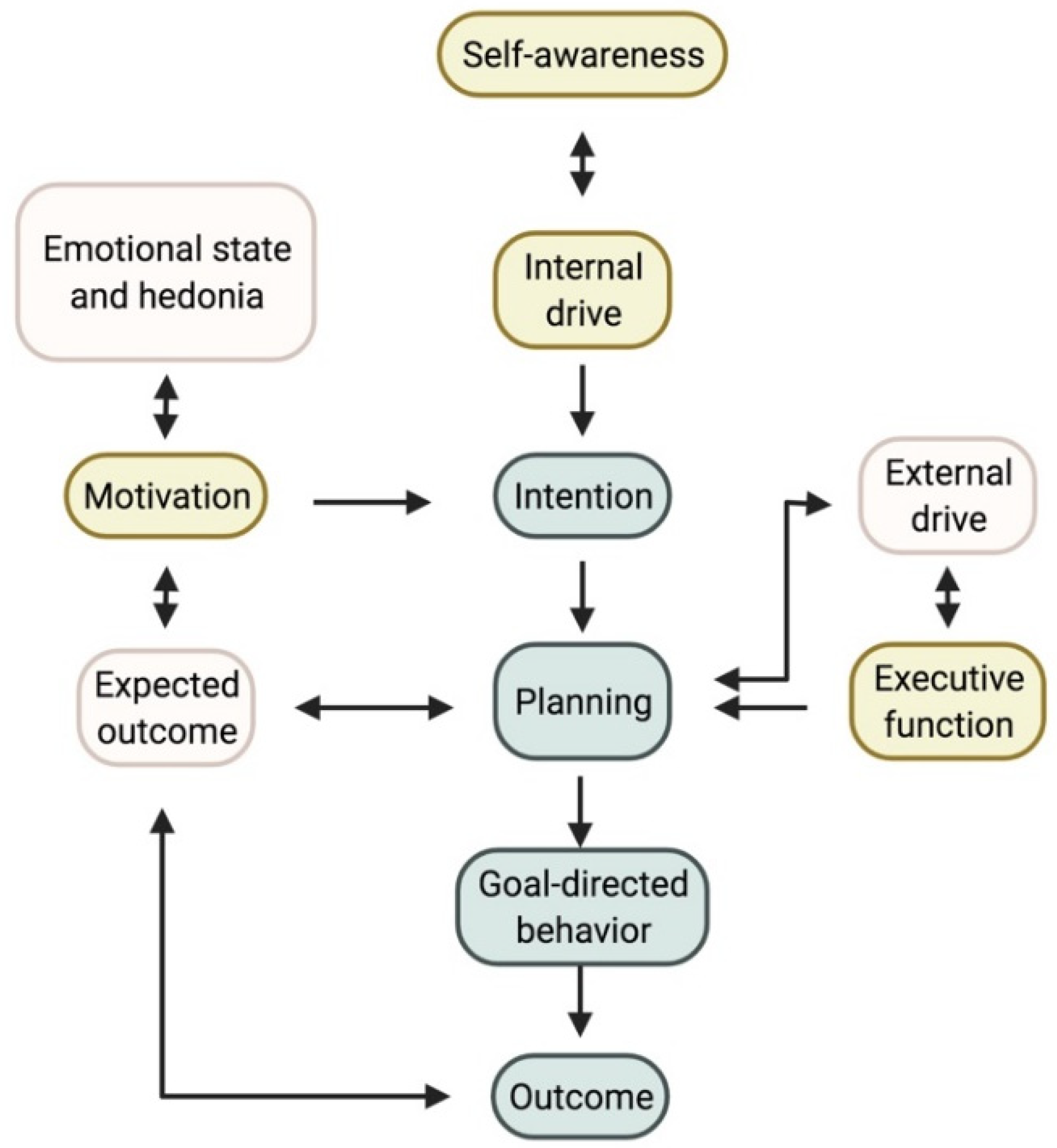
4.1. Psychological Model
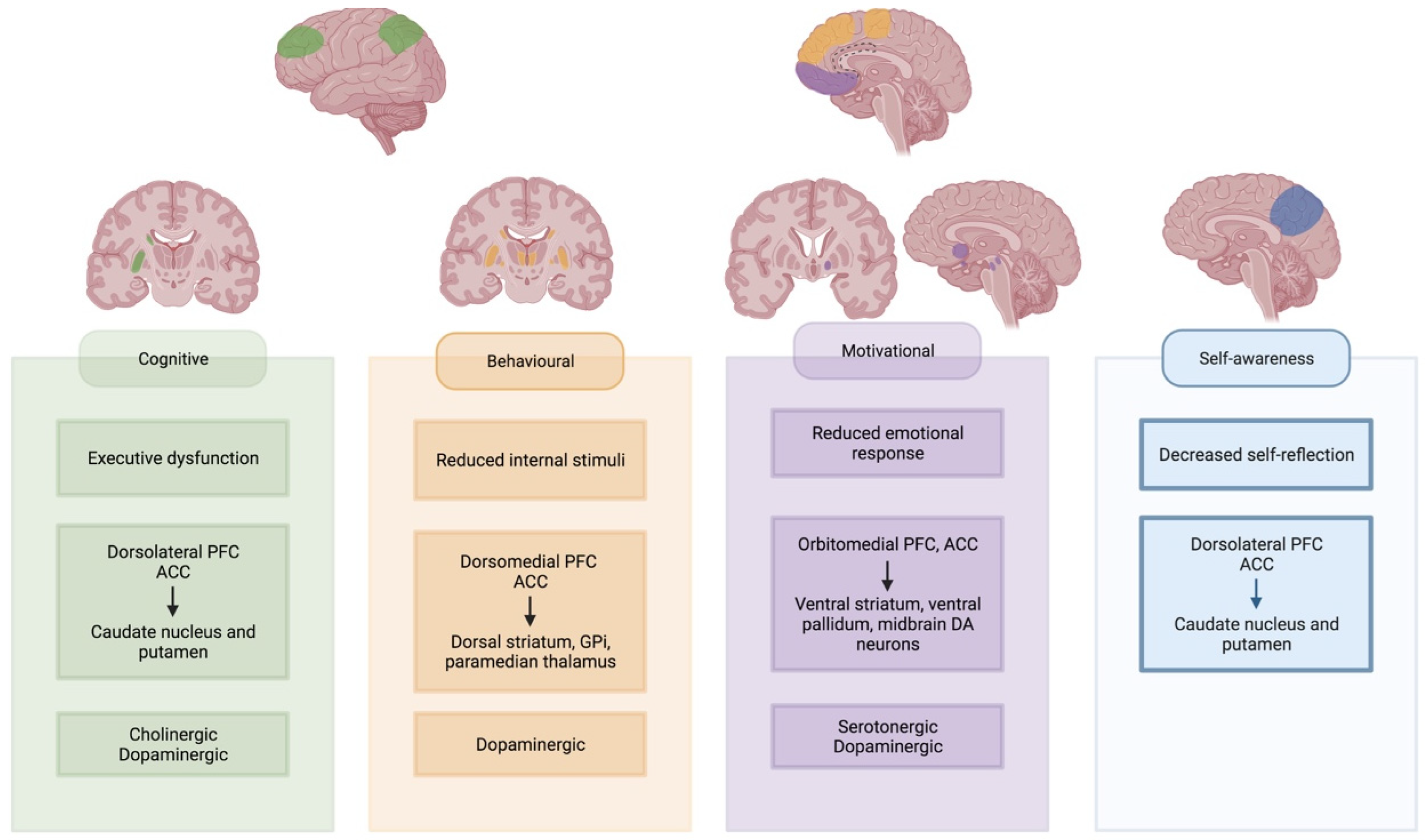
4.2. Neural Networks
4.3. Imaging Biomarkers
5. Park Apathy
6. Treatment
6.1. Pharmacological
6.2. Non-Pharmacological
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sauerbier, A.; Lenka, A.; Aris, A.; Pal, P.K. Nonmotor Symptoms in Parkinson’s Disease: Gender and Ethnic Differences. In International Review of Neurobiology; Chaudhuri, K.R., Titova, N., Eds.; Academic Press: Cambridge, MA, USA, 2017; Volume 133, pp. 417–446. ISBN 9780128137086. [Google Scholar]
- Pont-Sunyer, C.; Hotter, A.; Gaig, C.; Seppi, K.; Compta, Y.; Katzenschlager, R.; Mas, N.; Hofeneder, D.; Brücke, T.; Bayés, A.; et al. The Onset of Nonmotor Symptoms in Parkinson’s Disease (the Onset Pd Study). Mov. Disord. 2015, 30, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Sauerbier, A.; Jenner, P.; Todorova, A.; Chaudhuri, K.R. Non Motor Subtypes and Parkinson’s Disease. Park. Relat. Disord. 2016, 22, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, K.; Langlois, C.; Plomhause, L.; Carette, A.S.; Delliaux, M.; Duhamel, A.; Defebvre, L. Apathy in Untreated Early-Stage Parkinson Disease: Relationship with Other Non-Motor Symptoms. Mov. Disord. 2014, 29, 1796–1801. [Google Scholar] [CrossRef]
- Rabins, P.V. Psychopathology of Parkinson’s Disease. Compr. Psychiatry 1982, 23, 421–429. [Google Scholar] [CrossRef]
- Aarsland, D.; Brønnick, K.; Ehrt, U.; De Deyn, P.P.; Tekin, S.; Emre, M.; Cummings, J.L. Neuropsychiatric Symptoms in Patients with Parkinson’s Disease and Dementia: Frequency, Profile and Associated Care Giver Stress. J. Neurol. Neurosurg. Psychiatry 2007, 78, 36–42. [Google Scholar] [CrossRef]
- Pedersen, K.F.; Alves, G.; Brønnick, K.; Aarsland, D.; Tysnes, O.B.; Larsen, J.P. Apathy in Drug-Naïve Patients with Incident Parkinson’s Disease: The Norwegian ParkWest Study. J. Neurol. 2010, 257, 217–223. [Google Scholar] [CrossRef]
- Terashi, H.; Ueta, Y.; Kato, H.; Mitoma, H.; Aizawa, H. Characteristics of Apathy in Treatment-Naïve Patients with Parkinson’s Disease. Int. J. Neurosci. 2019, 129, 16–21. [Google Scholar] [CrossRef]
- Dujardin, K.; Sockeel, P.; Delliaux, M.; Destée, A.; Defebvre, L. Apathy May Herald Cognitive Decline and Dementia in Parkinson’s Disease. Mov. Disord. 2009, 24, 2391–2397. [Google Scholar] [CrossRef]
- Barone, P.; Antonini, A.; Colosimo, C.; Marconi, R.; Morgante, L.; Avarello, T.P.; Bottacchi, E.; Cannas, A.; Ceravolo, G.; Ceravolo, R.; et al. The PRIAMO Study: A Multicenter Assessment of Nonmotor Symptoms and Their Impact on Quality of Life in Parkinson’s Disease. Mov. Disord. 2009, 24, 1641–1649. [Google Scholar] [CrossRef]
- Hinkle, J.T.; Perepezko, K.; Gonzalez, L.L.; Mills, K.A.; Pontone, G.M. Apathy and Anxiety in De Novo Parkinson’s Disease Predict the Severity of Motor Complications. Mov. Disord. Clin. Pract. 2021, 8, 76–84. [Google Scholar] [CrossRef]
- Ellmers, T.J.; Maslivec, A.; Young, W.R. Fear of Falling Alters Anticipatory Postural Control during Cued Gait Initiation. Neuroscience 2020, 438, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, K.; Sockeel, P.; Devos, D.; Delliaux, M.; Krystkowiak, P.; Destée, A.; Defebvre, L. Characteristics of Apathy in Parkinson’s Disease. Mov. Disord. 2007, 22, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.F.; Alves, G.; Aarsland, D.; Larsen, J.P. Occurrence and Risk Factors for Apathy in Parkinson Disease: A 4-Year Prospective Longitudinal Study. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1279–1282. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Forjaz, M.J.; Frades-Payo, B.; Agüera-Ortiz, L.; Weintraub, D.; Riesco, A.; Kurtis, M.M.; Chaudhuri, K.R. Neuropsychiatric Symptoms and Caregiver’s Burden in Parkinson’s Disease. Park. Relat. Disord. 2015, 21, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.D.; Pontone, G.M. “Pseudo-Syndromes” Associated with Parkinson Disease, Dementia, Apathy, Anxiety, and Depression. Neurol. Clin. Pract. 2019, 9, 354–359. [Google Scholar] [CrossRef]
- Mele, B.; Van, S.; Holroyd-Leduc, J.; Ismail, Z.; Pringsheim, T.; Goodarzi, Z. Diagnosis, Treatment and Management of Apathy in Parkinson’s Disease: A Scoping Review. BMJ Open 2020, 10, e037632. [Google Scholar] [CrossRef]
- Levy, R.; Dubois, B. Apathy and the Functional Anatomy of the Prefrontal Cortex-Basal Ganglia Circuits. Cereb. Cortex 2006, 16, 916–928. [Google Scholar] [CrossRef]
- Ou, R.; Hou, Y.; Wei, Q.; Lin, J.; Liu, K.; Zhang, L.; Jiang, Z.; Cao, B.; Zhao, B.; Song, W.; et al. Longitudinal Evolution of Non-Motor Symptoms in Early Parkinson’s Disease: A 3-Year Prospective Cohort Study. NPJ Park. Dis. 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Leiknes, I.; Tysnes, O.B.; Aarsland, D.; Larsen, J.P. Caregiver Distress Associated with Neuropsychiatric Problems in Patients with Early Parkinson’s Disease: The Norwegian ParkWest Study. Acta Neurol. Scand. 2010, 122, 418–424. [Google Scholar] [CrossRef]
- Benito-León, J.; Cubo, E.; Coronell, C.; Rodríguez-Fernández, R.; Pego-Reigosa, R.; Paz-González, J.M.; Cebrián-Pérez, E.; Suarez-Gil, P.; Marey-López, J.; Corredera-García, E.; et al. Impact of Apathy on Health-Related Quality of Life in Recently Diagnosed Parkinson’s Disease: The ANIMO Study. Mov. Disord. 2012, 27, 211–218. [Google Scholar] [CrossRef]
- Cubo, E.; Benito-León, J.; Coronell, C.; Armesto, D. Clinical Correlates of Apathy in Patients Recently Diagnosed with Parkinson’s Disease: The ANIMO Study. Neuroepidemiology 2012, 38, 48–55. [Google Scholar] [CrossRef]
- Ou, R.; Lin, J.; Liu, K.; Jiang, Z.; Wei, Q.; Hou, Y.; Zhang, L.; Cao, B.; Zhao, B.; Song, W.; et al. Evolution of Apathy in Early Parkinson’s Disease: A 4-Years Prospective Cohort Study. Front. Aging Neurosci. 2021, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kirsch-Darrow, L.; Fernandez, H.H.; Marsiske, M.; Okun, M.S.; Bowers, D. Dissociating Apathy and Depression in Parkinson Disease. Neurology 2006, 67, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Isella, V.; Melzi, P.; Grimaldi, M.; Iurlaro, S.; Piolti, R.; Ferrarese, C.; Frattola, L.; Appollonio, I. Clinical, Neuropsychological, and Morphometric Correlates of Apathy in Parkinson’s Disease. Mov. Disord. 2002, 17, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Kulisevsky, J.; Pagonbarraga, J.; Pascual-Sedano, B.; García-Sánchez, C.; Gironell, A. Prevalence and Correlates of Neuropsychiatric Symptoms in Parkinson’s Disease without Dementia. Mov. Disord. 2008, 23, 1889–1896. [Google Scholar] [CrossRef]
- Oguru, M.; Tachibana, H.; Toda, K.; Okuda, B.; Oka, N. Apathy and Depression in Parkinson Disease. J. Geriatr. Psychiatry Neurol. 2010, 23, 35–41. [Google Scholar] [CrossRef]
- Lieberman, A. Are Dementia and Depression in Parkinson’s Disease Related? J. Neurol. Sci. 2006, 248, 138–142. [Google Scholar] [CrossRef]
- Eglit, G.M.L.; Lopez, F.; Schiehser, D.M.; Pirogovsky-Turk, E.; Litvan, I.; Lessig, S.; Filoteo, J.V. Delineation of Apathy Subgroups in Parkinson’s Disease: Differences in Clinical Presentation, Functional Ability, Health-Related Quality of Life, and Caregiver Burden. Mov. Disord. Clin. Pract. 2021, 8, 92–99. [Google Scholar] [CrossRef]
- Santangelo, G.; Vitale, C.; Trojano, L.; Picillo, M.; Moccia, M.; Pisano, G.; Pezzella, D.; Cuoco, S.; Erro, R.; Longo, K.; et al. Relationship between Apathy and Cognitive Dysfunctions in de Novo Untreated Parkinson’s Disease: A Prospective Longitudinal Study. Eur. J. Neurol. 2015, 22, 253–260. [Google Scholar] [CrossRef]
- Kirsch-Darrow, L.; Zahodne, L.B.; Hass, C.; Mikos, A.; Okun, M.S.; Fernandez, H.H.; Bowers, D. How Cautious Should We Be When Assessing Apathy with the Unified Parkinson’s Disease Rating Scale? Mov. Disord. 2009, 24, 684–688. [Google Scholar] [CrossRef]
- Stella, F.; Banzato, C.E.M.; Quagliato, E.M.A.B.; Viana, M.A.; Christofoletti, G. Psychopathological Features in Patients with Parkinson’s Disease and Related Caregivers’ Burden. Int. J. Geriatr. Psychiatry 2009, 24, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, L.C.; Cimino, C.R.; Oelke, L.E.; Hauser, R.A.; Sanchez-Ramos, J. The Independent Influence of Apathy and Depression on Cognitive Functioning in Parkinson’s Disease. Neuropsychology 2010, 24, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Larsen, J.P.; Lim, N.G.; Janvin, C.; Karlsen, K.; Tandberg, E.; Cummings, J.L. Range of Neuropsychiatric Disturbances in Patients with Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 1999, 67, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, Validity, and Clinical Correlates of Apathy in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Wee, N.; Kandiah, N.; Acharyya, S.; Chander, R.J.; Ng, A.; Au, W.L.; Tan, L.C.S. Baseline Predictors of Worsening Apathy in Parkinson’s Disease: A Prospective Longitudinal Study. Park. Relat. Disord. 2016, 23, 95–98. [Google Scholar] [CrossRef]
- Liu, H.; Ou, R.; Wei, Q.; Hou, Y.; Zhang, L.; Cao, B.; Zhao, B.; Song, W.; Shang, H. Apathy in Drug-Naïve Patients with Parkinson’s Disease. Park. Relat. Disord. 2017, 44, 28–32. [Google Scholar] [CrossRef]
- Cho, B.H.; Choi, S.M.; Kim, J.T.; Kim, B.C. Association of Coffee Consumption and Non-Motor Symptoms in Drug-Naïve, Early-Stage Parkinson’s Disease. Park. Relat. Disord. 2018, 50, 42–47. [Google Scholar] [CrossRef]
- De La Riva, P.; Smith, K.; Xie, S.X.S.X.; Weintraub, D. Course of Psychiatric Symptoms and Global Cognition in Early Parkinson Disease. Neurology 2014, 83, 1096–1103. [Google Scholar] [CrossRef]
- Wang, F.; Pan, Y.; Zhang, M.; Hu, K. Predicting the Onset of Freezing of Gait in de Novo Parkinson’s Disease. medRxiv 2021, 2021.03.11.21253192. [Google Scholar]
- Oh, Y.S.; Kim, J.H.; Yoo, S.W.; Hwang, E.J.; Lyoo, C.H.; Lee, K.S.; Kim, J.S. Neuropsychiatric Symptoms and Striatal Monoamine Availability in Early Parkinson’s Disease without Dementia. Neurol. Sci. 2021, 42, 711–718. [Google Scholar] [CrossRef]
- Radakovic, R.; Harley, C.; Abrahams, S.; Starr, J.M. A Systematic Review of the Validity and Reliability of Apathy Scales in Neurodegenerative Conditions. Int. Psychogeriatr. 2015, 27, 903–923. [Google Scholar] [CrossRef]
- Barber, T.R.; Muhammed, K.; Drew, D.; Lawton, M.; Crabbe, M.; Rolinski, M.; Quinnell, T.; Zaiwalla, Z.; Ben-Shlomo, Y.; Husain, M.; et al. Apathy in Rapid Eye Movement Sleep Behaviour Disorder Is Common and Under-Recognized. Eur. J. Neurol. 2018, 25, 469-e32. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.; Xie, S.; Karlawish, J.; Siderowf, A. Differences in Depression Symptoms in Patients with Alzheimer’s and Parkinson’s Diseases: Evidence from the 15-Item Geriatric Depression Scale (GDS-15). Int. J. Geriatr. Psychiatry 2007, 22, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Van Wanrooij, L.L.; Borsboom, D.; Moll Van Charante, E.P.; Richard, E.; Van Gool, W.A. A Network Approach on the Relation between Apathy and Depression Symptoms with Dementia and Functional Disability. Int. Psychogeriatr. 2019, 31, 1655–1663. [Google Scholar] [CrossRef] [PubMed]
- Szymkowicz, S.M.; Ellis, L.J.; May, P.E. The 3-Item “Apathy” Subscale Within the GDS-15 Is Not Supported in De Novo Parkinson’s Disease Patients: Analysis of the PPMI Cohort. J. Geriatr. Psychiatry Neurol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Forjaz, M.J.; Kurtis, M.M.; Skorvanek, M. Measurement of Nonmotor Symptoms in Clinical Practice. In International Review of Neurobiology; Chaudhuri, K.R., Titova, N., Eds.; Academic Press: Cambridge, MA, USA, 2017; Volume 133, pp. 291–345. ISBN 0074-7742. [Google Scholar]
- Leentjens, A.F.G.; Dujardin, K.; Marsh, L.; Martinez-Martin, P.; Richard, I.H.; Starkstein, S.E.; Weintraub, D.; Sampaio, C.; Poewe, W.; Rascol, O.; et al. Apathy and Anhedonia Rating Scales in Parkinson’s Disease: Critique and Recommendations. Mov. Disord. 2008, 23, 2015–2025. [Google Scholar] [CrossRef] [PubMed]
- Sockeel, P.; Dujardin, K.; Devos, D.; Denève, C.; Destée, A.; Defebvre, L. The Lille Apathy Rating Scale (LARS), a New Instrument for Detecting and Quantifying Apathy: Validation in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 579–584. [Google Scholar] [CrossRef]
- Groeneweg-Koolhoven, I.; De Waal, M.W.M.; Van Der Weele, G.M.; Gussekloo, J.; Van Der Mast, R.C. Quality of Life in Community-Dwelling Older Persons with Apathy. Am. J. Geriatr. Psychiatry 2014, 22, 186–194. [Google Scholar] [CrossRef]
- Clarke, D.E.; Ko, J.Y.; Lyketsos, C.; Rebok, G.W.; Eaton, W.W. Apathy and Cognitive and Functional Decline in Community-Dwelling Older Adults: Results from the Baltimore ECA Longitudinal Study. Int. Psychogeriatr. 2010, 22, 819–829. [Google Scholar] [CrossRef]
- Martin, G.P.; McDonald, K.R.; Allsop, D.; Diggle, P.J.; Leroi, I. Apathy as a Behavioural Marker of Cognitive Impairment in Parkinson’s Disease: A Longitudinal Analysis. J. Neurol. 2020, 267, 214–227. [Google Scholar] [CrossRef]
- Darweesh, S.K.L.; Verlinden, V.J.A.; Stricker, B.H.; Hofman, A.; Koudstaal, P.J.; Ikram, M.A. Trajectories of Prediagnostic Functioning in Parkinson’s Disease. Brain 2017, 140, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Gaenslen, A.; Swid, I.; Liepelt-Scarfone, I.; Godau, J.; Berg, D. The Patients’ Perception of Prodromal Symptoms before the Initial Diagnosis of Parkinson’s Disease. Mov. Disord. 2011, 26, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Durcan, R.; Wiblin, L.; Lawson, R.A.; Khoo, T.K.; Yarnall, A.J.; Duncan, G.W.; Brooks, D.J.; Pavese, N.; Burn, D.J. Prevalence and Duration of Non-Motor Symptoms in Prodromal Parkinson’s Disease. Eur. J. Neurol. 2019, 26, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Iranzo, A.; Fernández-Arcos, A.; Tolosa, E.; Serradell, M.; Molinuevo, J.L.; Valldeoriola, F.; Gelpi, E.; Vilaseca, I.; Sánchez-Valle, R.; Lladó, A.; et al. Neurodegenerative Disorder Risk in Idiopathic REM Sleep Behavior Disorder: Study in 174 Patients. PLoS ONE 2014, 9, e89741. [Google Scholar] [CrossRef]
- Barber, T.R.; Lawton, M.; Rolinski, M.; Evetts, S.; Baig, F.; Ruffmann, C.; Gornall, A.; Klein, J.C.; Lo, C.; Dennis, G.; et al. Prodromal Parkinsonism and Neurodegenerative Risk Stratification in REM Sleep Behavior Disorder. Sleep 2017, 40, 11–13. [Google Scholar] [CrossRef]
- Boeve, B.F.; Silber, M.H.; Saper, C.B.; Ferman, T.J.; Dickson, D.W.; Parisi, J.E.; Benarroch, E.E.; Ahlskog, J.E.; Smith, G.E.; Caselli, R.C.; et al. Pathophysiology of REM Sleep Behaviour Disorder and Relevance to Neurodegenerative Disease. Brain 2007, 130, 2770–2788. [Google Scholar] [CrossRef]
- Bargiotas, P.; Ntafouli, M.; Lachenmayer, M.L.; Krack, P.; Schüpbach, W.M.M.; Bassetti, C.L.A. Apathy in Parkinson’s Disease with REM Sleep Behavior Disorder. J. Neurol. Sci. 2019, 399, 194–198. [Google Scholar] [CrossRef]
- Iijima, M.; Okuma, Y.; Suzuki, K.; Yoshii, F.; Nogawa, S.; Osada, T.; Hirata, K.; Kitagawa, K.; Hattori, N. Associations between Probable REM Sleep Behavior Disorder, Olfactory Disturbance, and Clinical Symptoms in Parkinson’s Disease: A Multicenter Cross-Sectional Study. PLoS ONE 2021, 16, 0247443. [Google Scholar] [CrossRef]
- Haehner, A.; Masala, C.; Walter, S.; Reichmann, H.; Hummel, T. Incidence of Parkinson’s Disease in a Large Patient Cohort with Idiopathic Smell and Taste Loss. J. Neurol. 2019, 266, 339–345. [Google Scholar] [CrossRef]
- Morley, J.F.; Weintraub, D.; Mamikonyan, E.; Moberg, P.J.; Siderowf, A.D.; Duda, J.E. Olfactory Dysfunction Is Associated with Neuropsychiatric Manifestations in Parkinson’s Disease. Mov. Disord. 2011, 26, 2051–2057. [Google Scholar] [CrossRef]
- Hong, J.Y.; Sunwoo, M.K.; Ham, J.H.; Lee, J.J.; Lee, P.H.; Sohn, Y.H. Apathy and Olfactory Dysfunction in Early Parkinson’s Disease. J. Mov. Disord. 2015, 8, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Solla, P.; Liscia, A.; Defazio, G.; Saba, L.; Cannas, A.; Cavazzana, A.; Hummel, T.; Haehner, A. Correlation among Olfactory Function, Motors’ Symptoms, Cognitive Impairment, Apathy, and Fatigue in Patients with Parkinson’s Disease. J. Neurol. 2018, 265, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Ojagbemi, A.A.; Akinyemi, R.O.; Baiyewu, O. Neuropsychiatric Symptoms in Nigerian Patients with Parkinson’s Disease. Acta Neurol. Scand. 2013, 128, 9–16. [Google Scholar] [CrossRef]
- Drijgers, R.L.; Dujardin, K.; Reijnders, J.S.A.M.; Defebvre, L.; Leentjens, A.F.G. Validation of Diagnostic Criteria for Apathy in Parkinson’s Disease. Park. Relat. Disord. 2010, 16, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.G.; Pluck, G. Negative Symptoms: The “pathology” of Motivation and Goal-Directed Behaviour. Trends Neurosci. 2000, 23, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Stuss, D.T.; Van Reekum, R.; Murphy, K.J. Differentiation of States and Causes of Apathy. In The Neuropsychology of Emotion; Borod, J.C., Ed.; Series in Affective Science; Oxford University Press: Oxford, UK, 2000; pp. 340–363. ISBN 0-19-511464-7. (Hardcover). [Google Scholar]
- Robert, P.; Onyike, C.U.; Leentjens, A.F.G.; Dujardin, K.; Aalten, P.; Starkstein, S.; Verhey, F.R.J.; Yessavage, J.; Clement, J.P.; Drapier, D.; et al. Proposed Diagnostic Criteria for Apathy in Alzheimer’s Disease and Other Neuropsychiatric Disorders. Eur. Psychiatry 2009, 24, 98–104. [Google Scholar] [CrossRef]
- Laplane, D.; Dubois, B. Auto-Activation Deficit: A Basal Ganglia Related Syndrome. Mov. Disord. 2001, 16, 810–814. [Google Scholar] [CrossRef]
- Lazcano-Ocampo, C.; Wan, Y.M.; van Wamelen, D.J.; Batzu, L.; Boura, I.; Titova, N.; Leta, V.; Qamar, M.; Martinez-Martin, P.; Ray Chaudhuri, K. Identifying and Responding to Fatigue and Apathy in Parkinson’s Disease: A Review of Current Practice. Expert Rev. Neurother. 2020, 20, 477–495. [Google Scholar] [CrossRef]
- Levy, G.; Jacobs, D.M.; Tang, M.X.; Côté, L.J.; Louis, E.D.; Alfaro, B.; Mejia, H.; Stern, Y.; Marder, K. Memory and Executive Function Impairment Predict Dementia in Parkinson’s Disease. Mov. Disord. 2002, 17, 1221–1226. [Google Scholar] [CrossRef]
- Marin, R.S. Apathy: A Neuropsychiatric Syndrome. J. Neuropsychiatry Clin. Neurosci. 1991, 3, 243–254. [Google Scholar] [CrossRef]
- Yuen, G.S.; Gunning, F.M.; Woods, E.; Klimstra, S.A.; Hoptman, M.J.; Alexopoulos, G.S. Neuroanatomical Correlates of Apathy in Late-Life Depression and Antidepressant Treatment Response. J. Affect. Disord. 2014, 166, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hull, J.G.; Levy, A.S. The Organizational Functions of the Self: An Alternative to the Duval and Wicklund Model of Self-Awareness. J. Pers. Soc. Psychol. 1979, 37, 756–768. [Google Scholar] [CrossRef]
- Leritz, E.; Loftis, C.; Crucian, G.; Friedman, W.; Bowers, D. Self-Awareness of Deficits in Parkinson Disease. Clin. Neuropsychol. 2004, 18, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Orfei, M.D.; Assogna, F.; Pellicano, C.; Pontieri, F.E.; Caltagirone, C.; Pierantozzi, M.; Stefani, A.; Spalletta, G. Anosognosia for Cognitive and Behavioral Symptoms in Parkinson’s Disease with Mild Dementia and Mild Cognitive Impairment: Frequency and Neuropsychological/Neuropsychiatric Correlates. Park. Relat. Disord. 2018, 54, 62–67. [Google Scholar] [CrossRef]
- Maier, F.; Prigatano, G.P.; Kalbe, E.; Barbe, M.T.; Eggers, C.; Lewis, C.J.; Burns, R.S.; Morrone-Strupinsky, J.; Moguel-Cobos, G.; Fink, G.R.; et al. Impaired Self-Awareness of Motor Deficits in Parkinson’s Disease: Association with Motor Asymmetry and Motor Phenotypes. Mov. Disord. 2012, 27, 1443–1446. [Google Scholar] [CrossRef]
- Devos, D.; Moreau, C.; Maltête, D.; Lefaucheur, R.; Kreisler, A.; Eusebio, A.; Defer, G.; Ouk, T.; Azulay, J.P.; Krystkowiak, P.; et al. Rivastigmine in Apathetic but Dementia and Depression-Free Patients with Parkinson’s Disease: A Double-Blind, Placebo-Controlled, Randomised Clinical Trial. J. Neurol. Neurosurg. Psychiatry 2014, 85, 668–674. [Google Scholar] [CrossRef]
- Drew, D.S.; Muhammed, K.; Baig, F.; Kelly, M.; Saleh, Y.; Sarangmat, N.; Okai, D.; Hu, M.; Manohar, S.; Husain, M. Dopamine and Reward Hypersensitivity in Parkinson’s Disease with Impulse Control Disorder. Brain 2020, 143, 2502–2518. [Google Scholar] [CrossRef]
- Scott, B.M.; Eisinger, R.S.; Burns, M.R.; Lopes, J.; Okun, M.S.; Gunduz, A.; Bowers, D. Co-Occurrence of Apathy and Impulse Control Disorders in Parkinson Disease. Neurology 2020, 95, e2769–e2780. [Google Scholar] [CrossRef]
- Lansdall, C.J.; Coyle-Gilchrist, I.T.S.; Jones, P.S.; Rodríguez, P.V.; Wilcox, A.; Wehmann, E.; Dick, K.M.; Robbins, T.W.; Rowe, J.B. Apathy and Impulsivity in Frontotemporal Lobar Degeneration Syndromes. Brain 2017, 140, 1792–1807. [Google Scholar] [CrossRef]
- Maillet, A.; Krack, P.; Lhommée, E.; Météreau, E.; Klinger, H.; Favre, E.; Le Bars, D.; Schmitt, E.; Bichon, A.; Pelissier, P.; et al. The Prominent Role of Serotonergic Degeneration in Apathy, Anxiety and Depression in de Novo Parkinson’s Disease. Brain 2016, 139, 2486–2502. [Google Scholar] [CrossRef]
- Prange, S.; Metereau, E.; Maillet, A.; Lhommée, E.; Klinger, H.; Pelissier, P.; Ibarrola, D.; Heckemann, R.A.; Castrioto, A.; Tremblay, L.; et al. Early Limbic Microstructural Alterations in Apathy and Depression in de Novo Parkinson’s Disease. Mov. Disord. 2019, 34, 1644–1654. [Google Scholar] [CrossRef] [PubMed]
- Maillet, A.; Météreau, E.; Tremblay, L.; Favre, E.; Klinger, H.; Lhommée, E.; Le Bars, D.; Castrioto, A.; Prange, S.; Sgambato, V.; et al. Serotonergic and Dopaminergic Lesions Underlying Parkinsonian Neuropsychiatric Signs. Mov. Disord. 2021, 36, 2888–2900. [Google Scholar] [CrossRef] [PubMed]
- Baggio, H.C.; Segura, B.; Garrido-Millan, J.L.; Marti, M.J.; Compta, Y.; Valldeoriola, F.; Tolosa, E.; Junque, C. Resting-State Frontostriatal Functional Connectivity in Parkinson’s Disease-Related Apathy. Mov. Disord. 2015, 30, 671–679. [Google Scholar] [CrossRef]
- Alexander, G.E.; Crutcher, M.D.; Delong, M.R. Basal Ganglia-Thalamocortical Circuits: Parallel Substrates for Motor, Oculomotor, Prefrontal and Limbic Functions. Prog. Brain Res. 1990, 85, 119–149. [Google Scholar]
- Cottencin, O.; Guardia, D.; Warembourg, F.; Gaudry, C.; Goudemand, M. Methadone Overdose, Auto-Activation Deficit, and Catatonia:A Case Study. Prim. Care Companion J. Clin. Psychiatry 2009, 11, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Leroy, A.; Petyt, G.; Pignon, B.; Vaiva, G.; Jardri, R.; Amad, A. Research Letter: Auto-Activation Deficit in Schizophrenia: A Case Report. Psychol. Med. 2018, 48, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Ali-Cherif, A.; Royere, M.L.; Gosset, A.; Poncet, M.; Salamon, G.; Khalil, R. Behavior and mental activity disorders after carbon monoxide poisoning. Bilateral pallidal lesions. Rev. Neurol. 1984, 140, 401–405. [Google Scholar]
- Leu-Semenescu, S.; Uguccioni, G.; Golmard, J.L.; Czernecki, V.; Yelnik, J.; Dubois, B.; Forgeot D’Arc, B.; Grabli, D.; Levy, R.; Arnulf, I. Can We Still Dream When the Mind Is Blank? Sleep and Dream Mentations in Auto-Activation Deficit. Brain 2013, 136, 3076–3084. [Google Scholar] [CrossRef]
- David, R.; Koulibaly, M.; Benoit, M.; Garcia, R.; Caci, H.; Darcourt, J.; Robert, P. Striatal Dopamine Transporter Levels Correlate with Apathy in Neurodegenerative Diseases. A SPECT Study with Partial Volume Effect Correction. Clin. Neurol. Neurosurg. 2008, 110, 19–24. [Google Scholar] [CrossRef]
- Mega, M.S.; Cohenour, R.C. Akinetic Mutism: Disconnection of Frontal-Subcortical Circuits. Neuropsychiatry. Neuropsychol. Behav. Neurol. 1997, 10, 254–259. [Google Scholar]
- Bogousslavsky, J.; Regli, F.; Delaloye, B.; Delaloye-Bischof, A.; Assal, G.; Uske, A. Loss of Psychic Self-Activation with Bithalamic Infarction. Acta Neurol. Scand. 1991, 83, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Laplane, D. La perte d’auto-activation psychique. Rev. Neurol. 1990, 146, 397–404. [Google Scholar] [PubMed]
- Habib, M. Athymhormia and Disorders of Motivation in Basal Ganglia Disease. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 509–524. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Leff, A.; Sinha, N.; Turner, C.; Bays, P.; Draganski, B.; Husain, M. Dopamine Reverses Reward Insensitivity in Apathy Following Globus Pallidus Lesions. Cortex 2013, 49, 1292–1303. [Google Scholar] [CrossRef]
- Laine, M.; Tuokkola, T.; Hiltunen, J.; Vorobyev, V.; Bliss, I.; Baddeley, A.; Rinne, J.O. Central Executive Function in Mild Cognitive Impairment: A PET Activation Study: Cognition and Neurosciences. Scand. J. Psychol. 2009, 50, 33–40. [Google Scholar] [CrossRef]
- Kondo, H.; Osaka, N.; Osaka, M. Cooperation of the Anterior Cingulate Cortex and Dorsolateral Prefrontal Cortex for Attention Shifting. Neuroimage 2004, 23, 670–679. [Google Scholar] [CrossRef]
- Baker, S.C.; Rogers, R.D.; Owen, A.M.; Frith, C.D.; Dolan, R.J.; Frackowiak, R.S.J.; Robbins, T.W. Neural Systems Engaged by Planning: A PET Study of the Tower of London Task. Neuropsychologia 1996, 34, 515–526. [Google Scholar] [CrossRef]
- Levy, R.; Friedman, H.R.; Davachi, L.; Goldman-Rakic, P.S. Differential Activation of the Caudate Nucleus in Primates Performing Spatial and Nonspatial Working Memory Tasks. J. Neurosci. 1997, 17, 3870–3882. [Google Scholar] [CrossRef]
- Owen, A.M. Planning and Spatial Working Memory: A Positron Emission Tomography Study in Humans. Eur. J. Neurosci. 1996, 8, 353–364. [Google Scholar] [CrossRef]
- Lucas-Jiménez, O.; Ojeda, N.; Peña, J.; Cabrera-Zubizarreta, A.; Díez-Cirarda, M.; Gómez-Esteban, J.C.; Gómez-Beldarrain, M.Á.; Ibarretxe-Bilbao, N. Apathy and Brain Alterations in Parkinson’s Disease: A Multimodal Imaging Study. Ann. Clin. Transl. Neurol. 2018, 5, 803–814. [Google Scholar] [CrossRef]
- Moretti, R.; Caruso, P.; Dal Ben, M. Rivastigmine as a Symptomatic Treatment for Apathy in Parkinson’s Dementia Complex: New Aspects for This Riddle. Parkinsons. Dis. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Lanctôt, K.L.; Herrmann, N.; Black, S.E.; Ryan, M.; Rothenburg, L.S.; Liu, B.A.; Busto, U.E. Apathy Associated with Alzheimer Disease: Use of Dextroamphetamine Challenge. Am. J. Geriatr. Psychiatry 2008, 16, 551–557. [Google Scholar] [CrossRef]
- Magnard, R.; Vachez, Y.; Carcenac, C.; Krack, P.; David, O.; Savasta, M.; Boulet, S.; Carnicella, S. What Can Rodent Models Tell Us about Apathy and Associated Neuropsychiatric Symptoms in Parkinson’s Disease? Transl. Psychiatry 2016, 6, e753. [Google Scholar] [CrossRef] [PubMed]
- Haber, S.N.; Knutson, B. The Reward Circuit: Linking Primate Anatomy and Human Imaging. Neuropsychopharmacology 2010, 35, 4–26. [Google Scholar] [CrossRef]
- Hong, S.; Hikosaka, O. Pedunculopontine Tegmental Nucleus Neurons Provide Reward, Sensorimotor, and Alerting Signals to Midbrain Dopamine Neurons. Physiol. Behav. 2016, 176, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Horta, S.; Riba, J.; Fernández De Bobadilla, R.; Pagonabarraga, J.; Pascual-Sedano, B.; Antonijoan, R.M.; Romero, S.; Ngel Mañanas, M.A.; García-Sanchez, C.; Kulisevsky, J. Apathy in Parkinson’s Disease: Neurophysiological Evidence of Impaired Incentive Processing. J. Neurosci. 2014, 17, 5918–5926. [Google Scholar] [CrossRef]
- Schultz, W. Behavioral Dopamine Signals. Trends Neurosci. 2007, 30, 203–210. [Google Scholar] [CrossRef]
- Riba, J.; Krämer, U.M.; Heldmann, M.; Richter, S.; Münte, T.F. Dopamine Agonist Increases Risk Taking but Blunts Reward-Related Brain Activity. PLoS ONE 2008, 3, e2479. [Google Scholar] [CrossRef]
- Leentjens, A.F.G.; Koester, J.; Fruh, B.; Shephard, D.T.S.; Barone, P.; Houben, J.J.G. The Effect of Pramipexole on Mood and Motivational Symptoms in Parkinson’s Disease: A Meta-Analysis of Placebo-Controlled Studies. Clin. Ther. 2009, 31, 89–98. [Google Scholar] [CrossRef]
- Barber, T.R.; Griffanti, L.; Muhammed, K.; Drew, D.S.; Bradley, K.M.; McGowan, D.R.; Crabbe, M.; Lo, C.; MacKay, C.E.; Husain, M.; et al. Apathy in Rapid Eye Movement Sleep Behaviour Disorder Is Associated with Serotonin Depletion in the Dorsal Raphe Nucleus. Brain 2018, 141, 2848–2854. [Google Scholar] [CrossRef]
- Cavanna, A.E.; Trimble, M.R. The Precuneus: A Review of Its Functional Anatomy and Behavioural Correlates. Brain 2006, 129, 564–583. [Google Scholar] [CrossRef] [PubMed]
- Shulman, G.L.; Fiez, J.A.; Corbetta, M.; Buckner, R.L.; Miezin, F.M.; Raichle, M.E.; Petersen, S.E. Common Blood Flow Changes across Visual Tasks: II. Decreases in Cerebral Cortex. J. Cogn. Neurosci. 1997, 9, 648–663. [Google Scholar] [CrossRef] [PubMed]
- Mesulam, M.-M. Frontal Cortex and Behavior. Ann. Neurol. 1986, 19, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Shin, S.A.; Lee, J.Y.; Nam, H.; Lim, J.S.; Kim, Y.K. Precuneus Degeneration and Isolated Apathy in Patients with Parkinson’s Disease. Neurosci. Lett. 2017, 653, 250–257. [Google Scholar] [CrossRef]
- Reijnders, J.S.A.M.; Scholtissen, B.; Weber, W.E.J.; Aalten, P.; Verhey, F.R.J.; Leentjens, A.F.G. Neuroanatomical Correlates of Apathy in Parkinson’s Disease: A Magnetic Resonance Imaging Study Using Voxel-Based Morphometry. Mov. Disord. 2010, 25, 2318–2325. [Google Scholar] [CrossRef]
- Newen, A.; Vogeley, K. Self-Representation: Searching for a Neural Signature of Self-Consciousness. Conscious. Cogn. 2003, 12, 529–543. [Google Scholar] [CrossRef]
- Morin, A. Self-Awareness Part 2: Neuroanatomy and Importance of Inner Speech. Soc. Personal. Psychol. Compass 2011, 5, 1004–1017. [Google Scholar] [CrossRef]
- Robert, G.; Le Jeune, F.; Dondaine, T.; Drapier, S.; Péron, J.; Lozachmeur, C.; Sauleau, P.; Houvenaghel, J.F.; Travers, D.; Millet, B.; et al. Apathy and Impaired Emotional Facial Recognition Networks Overlap in Parkinson’s Disease: A PET Study with Conjunction Analyses. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1153–1158. [Google Scholar] [CrossRef]
- Schmidt, L.; D’Arc, B.F.; Lafargue, G.; Galanaud, D.; Czernecki, V.; Grabli, D.; Schüpbach, M.; Hartmann, A.; Lévy, R.; Dubois, B.; et al. Disconnecting Force from Money: Effects of Basal Ganglia Damage on Incentive Motivation. Brain 2008, 131, 1303–1310. [Google Scholar] [CrossRef]
- Carriere, N.; Besson, P.; Dujardin, K.; Duhamel, A.; Defebvre, L.; Delmaire, C.; Devos, D. Apathy in Parkinson’s Disease Is Associated with Nucleus Accumbens Atrophy: A Magnetic Resonance Imaging Shape Analysis. Mov. Disord. 2014, 29, 897–903. [Google Scholar] [CrossRef]
- Wen, M.C.; Wen, M.C.; Thiery, A.; Tseng, W.Y.I.; Kok, T.; Xu, Z.; Chua, S.T.; Tan, L.C.S.; Tan, L.C.S.; Tan, L.C.S. Apathy Is Associated with White Matter Network Disruption and Specific Cognitive Deficits in Parkinson’s Disease. Psychol. Med. 2020, 52, 264–273. [Google Scholar] [CrossRef]
- Alzahrani, H.; Antonini, A.; Venneri, A. Apathy in Mild Parkinson’s Disease: Neuropsychological and Neuroimaging Evidence. J. Parkinsons. Dis. 2016, 6, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wu, J.; Wu, W.; Liu, R.; Pang, L.; Guan, D.; Xu, Y. Reduction of White Matter Integrity Correlates with Apathy in Parkinson’s Disease. Int. J. Neurosci. 2018, 128, 25–31. [Google Scholar] [CrossRef]
- Skidmore, F.M.; Yang, M.; Baxter, L.; von Deneen, K.; Collingwood, J.; He, G.; Tandon, R.; Korenkevych, D.; Savenkov, A.; Heilman, K.M.; et al. Apathy, Depression, and Motor Symptoms Have Distinct and Separable Resting Activity Patterns in Idiopathic Parkinson Disease. Neuroimage 2013, 81, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.H.; Pan, P.L.; Hu, J.B.; Chen, J.; Wang, X.Y.; Liu, C.F. Alterations of Regional Homogeneity in Parkinson’s Disease with “Pure” Apathy: A Resting-State FMRI Study. J. Affect. Disord. 2020, 274, 792–798. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, G.Y.; Zhang, Z.E.; He, A.Q.; Gan, J.; Liu, Z. White Matter Hyperintensities: A Marker for Apathy in Parkinson’s Disease without Dementia? Ann. Clin. Transl. Neurol. 2020, 7, 1692–1701. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.S.; Barrett, M.J.; Flanigan, J.L.; Sperling, S.A. Clinical and Demographic Correlates of Apathy in Parkinson’s Disease. J. Neurol. 2019, 266, 507–514. [Google Scholar] [CrossRef]
- Álvarez-Avellón, T.; Arias-Carrión, Ó.; Menéndez-González, M. Neuropsychiatric Symptoms and Associated Caregiver Stress in Geriatric Patients with Parkinson’s Disease. Neurol. Neurosci. 2015, 201521, 1–8. [Google Scholar] [CrossRef][Green Version]
- Hassan, A.; Vallabhajosula, S.; Zahodne, L.B.; Bowers, D.; Okun, M.S.; Fernandez, H.H.; Hass, C.J. Correlations of Apathy and Depression with Postural Instability in Parkinson Disease. J. Neurol. Sci. 2014, 338, 162–165. [Google Scholar] [CrossRef]
- Reijnders, J.S.A.M.; Ehrt, U.; Lousberg, R.; Aarsland, D.; Leentjens, A.F.G. The Association between Motor Subtypes and Psychopathology in Parkinson’s Disease. Park. Relat. Disord. 2009, 15, 379–382. [Google Scholar] [CrossRef]
- Perez-Lloret, S.; Negre-Pages, L.; Damier, P.; Delval, A.; Derkinderen, P.; Destée, A.; Meissner, W.G.; Schelosky, L.; Tison, F.; Rascol, O. Prevalence, Determinants, and Effect on Quality of Life of Freezing of Gait in Parkinson Disease. JAMA Neurol. 2014, 71, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.; McNamara, P.; Durso, R. Apathy in Patients with Parkinson Disease as a Function of Side of Onset. J. Geriatr. Psychiatry Neurol. 2013, 26, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Skorvanek, M.; Gdovinova, Z.; Rosenberger, J.; Ghorbani Saeedian, R.; Nagyova, I.; Groothoff, J.W.; van Dijk, J.P. The Associations between Fatigue, Apathy, and Depression in Parkinson’s Disease. Acta Neurol. Scand. 2015, 131, 80–87. [Google Scholar] [CrossRef]
- Sáez-Francàs, N.; Hernández-Vara, J.; Roso, M.C.; Martín, J.A.; Brugué, M.C. The Association of Apathy with Central Fatigue Perception in Patients with Parkinson’s Disease. Behav. Neurosci. 2013, 127, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, M.; Trojano, L.; De Micco, R.; Giordano, A.; Russo, A.; Tedeschi, G.; Chiorri, C.; Tessitore, A. Predictors of Fatigue Severity in Early, de Novo Parkinson Disease Patients: A 1-Year Longitudinal Study. Park. Relat. Disord. 2020, 79, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Zimmermann, R.; Gschwandtner, U.; Hatz, F.; Bousleiman, H.; Schwarz, N.; Fuhr, P. Apathy in Parkinson’s Disease Is Related to Executive Function, Gender and Age but Not to Depression. Front. Aging Neurosci. 2015, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; D’Iorio, A.; Maggi, G.; Cuoco, S.; Pellecchia, M.T.; Amboni, M.; Barone, P.; Vitale, C. Cognitive Correlates of “Pure Apathy” in Parkinson’s Disease. Park. Relat. Disord. 2018, 53, 101–104. [Google Scholar] [CrossRef] [PubMed]
- D’Iorio, A.; Maggi, G.; Vitale, C.; Trojano, L.; Santangelo, G. “Pure Apathy” and Cognitive Dysfunctions in Parkinson’s Disease: A Meta-Analytic Study. Neurosci. Biobehav. Rev. 2018, 94, 1–10. [Google Scholar] [CrossRef]
- Dujardin, K.; Moonen, A.J.H.; Behal, H.; Defebvre, L.; Duhamel, A.; Duits, A.A.; Plomhause, L.; Tard, C.; Leentjens, A.F.G. Cognitive Disorders in Parkinson’s Disease: Confirmation of a Spectrum of Severity. Park. Relat. Disord. 2015, 21, 1299–1305. [Google Scholar] [CrossRef]
- Costa, A.; Peppe, A.; Zabberoni, S.; Scalici, F.; Caltagirone, C.; Carlesimo, G.A. Apathy in Individuals with Parkinson’s Disease Associated with Mild Cognitive Impairment. A Neuropsychological Investigation. Neuropsychologia 2018, 118, 4–11. [Google Scholar] [CrossRef]
- Goldman, J.G.; Holden, S.K.; Litvan, I.; McKeith, I.; Stebbins, G.T.; Taylor, J.P. Evolution of Diagnostic Criteria and Assessments for Parkinson’s Disease Mild Cognitive Impairment. Mov. Disord. 2018, 33, 503–510. [Google Scholar] [CrossRef]
- Baiano, C.; Barone, P.; Trojano, L.; Santangelo, G. Prevalence and Clinical Aspects of Mild Cognitive Impairment in Parkinson’s Disease: A Meta-Analysis. Mov. Disord. 2020, 35, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.C.; Myers, P.S.; Weigand, A.J.; Foster, E.R.; Cairns, N.J.; Jackson, J.J.; Lessov-Schlaggar, C.N.; Perlmutter, J.S. Parkinson Disease Clinical Subtypes: Key Features & Clinical Milestones. Ann. Clin. Transl. Neurol. 2020, 7, 1–12. [Google Scholar] [CrossRef]
- Wang, H.T.; Wang, L.; He, Y.; Yu, G. Rotigotine Transdermal Patch for the Treatment of Neuropsychiatric Symptoms in Parkinson’s Disease: A Meta-Analysis of Randomized Placebo-Controlled Trials. J. Neurol. Sci. 2018, 393, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Castrioto, A.; Thobois, S.; Anheim, M.; Quesada, J.L.; Lhommée, E.; Klinger, H.; Bichon, A.; Schmitt, E.; Durif, F.; Azulay, J.P.; et al. A Randomized Controlled Double-Blind Study of Rotigotine on Neuropsychiatric Symptoms in de Novo PD. NPJ Park. Dis. 2020, 6, 1–6. [Google Scholar] [CrossRef]
- Auffret, M.; Le Jeune, F.; Maurus, A.; Drapier, S.; Houvenaghel, J.F.; Robert, G.H.; Sauleau, P.; Vérin, M. Apomorphine Pump in Advanced Parkinson’s Disease: Effects on Motor and Nonmotor Symptoms with Brain Metabolism Correlations. J. Neurol. Sci. 2017, 372, 279–287. [Google Scholar] [CrossRef]
- Todorova, A.; Martinez-Martin, P.; Martin, A.; Rizos, A.; Reddy, P.; Chaudhuri, K.R. Daytime Apomorphine Infusion Combined with Transdermal Rotigotine Patch Therapy Is Tolerated at 2 Years: A 24-h Treatment Option in Parkinson’s Disease. Basal Ganglia 2013, 3, 127–130. [Google Scholar] [CrossRef]
- Blundo, C.; Gerace, C. Dopamine Agonists Can Improve Pure Apathy Associated with Lesions of the Prefrontal-Basal Ganglia Functional System. Neurol. Sci. 2015, 36, 1197–1201. [Google Scholar] [CrossRef]
- Ganjavi, H.; Macdonald, P.A. On-off Effects of Dopaminergic Therapy on Psychiatric Symptoms in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 2015, 27, e134–e139. [Google Scholar] [CrossRef]
- Zahodne, L.B.; Bernal-Pacheco, O.; Bowers, D.; Ward, H.; Oyama, G.; Limotai, N.; Velez-Lago, F.; Rodriguez, R.L.; Malaty, I.; McFarland, N.R.; et al. Are Selective Serotonin Reuptake Inhibitors Associated with Greater Apathy in Parkinson’s Disease? J. Neuropsychiatry Clin. Neurosci. 2012, 24, 326–330. [Google Scholar] [CrossRef]
- Meloni, M.; Puligheddu, M.; Carta, M.; Cannas, A.; Figorilli, M.; Defazio, G. Efficacy and Safety of 5-Hydroxytryptophan on Depression and Apathy in Parkinson’s Disease: A Preliminary Finding. Eur. J. Neurol. 2020, 27, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Tabu, H.; Ozaki, A.; Hamano, T.; Takeshima, T. Antidepressants for Depression, Apathy, and Gait Instability in Parkinson’s Disease: A Multicenter Randomized Study. Intern. Med. 2019, 58, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Bullock, R.; Cameron, A. Rivastigmine for the Treatment of Dementia and Visual Hallucinations Associated with Parkinson’s Disease: A Case Series. Curr. Med. Res. Opin. 2002, 18, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.-S.; Kim, J.-S.; Lee, P.H. Effect of Rivastigmine on Behavioral and Psychiatric Symptoms of Parkinson’s Disease Dementia. J. Mov. Disord. 2015, 8, 98–102. [Google Scholar] [CrossRef]
- Litvinenko, I.V.; Odinak, M.M.; Mogil’naya, V.I.; Emelin, A.Y.U. Efficacy and Safety of Galantamine (Reminyl) for Dementia in Patients with Parkinson’s Disease (an Open Controlled Trial). Neurosci. Behav. Physiol. 2008, 38, 937–945. [Google Scholar] [CrossRef]
- Lanctot, K.L.; Chau, S.A.; Herrmann, N.; Drye, L.T.; Rosenberg, P.B.; Scherer, R.W.; Black, S.E.; Vaidya, V.; Bachman, D.L.; Mintzer, J.E. Effect of Methylphenidate on Attention in Apathetic AD Patients in a Randomized, Placebo-Controlled Trial. Int. Psychogeriatr. 2014, 26, 239–246. [Google Scholar] [CrossRef]
- Nagayama, H.; Kano, O.; Murakami, H.; Ono, K.; Hamada, M.; Toda, T.; Sengoku, R.; Shimo, Y.; Hattori, N. Effect of Istradefylline on Mood Disorders in Parkinson’s Disease. J. Neurol. Sci. 2019, 396, 78–83. [Google Scholar] [CrossRef]
- Krishna, R.; Ali, M.; Moustafa, A.A. Effects of Combined MAO-B Inhibitors and Levodopa vs Monotherapy in Parkinson’s Disease. Front. Aging Neurosci. 2014, 6, 180. [Google Scholar] [CrossRef]
- Hatano, T.; Hattori, N.; Kawanabe, T.; Terayama, Y.; Suzuki, N.; Iwasaki, Y.; Fujioka, T. An Exploratory Study of the Efficacy and Safety of Yokukansan for Neuropsychiatric Symptoms in Patients with Parkinson’s Disease. J. Neural Transm. 2014, 121, 275–281. [Google Scholar] [CrossRef]
- Athauda, D.; MacLagan, K.; Budnik, N.; Zampedri, L.; Hibbert, S.; Skene, S.S.; Chowdhury, K.; Aviles-Olmos, I.; Limousin, P.; Foltynie, T. What Effects Might Exenatide Have on Non-Motor Symptoms in Parkinson’s Disease: A Post Hoc Analysis. J. Parkinsons. Dis. 2018, 8, 247–258. [Google Scholar] [CrossRef]
- Smith, K.M.; Eyal, E.; Weintraub, D. Combined Rasagiline and Antidepressant Use in Parkinson Disease in the ADAGIO Study: Effects on Nonmotor Symptoms and Tolerability. JAMA Neurol. 2015, 72, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Fahn, S. Methylphenidate Treats Apathy in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 461–462. [Google Scholar] [CrossRef]
- Gelderblom, H.; Wüstenberg, T.; McLean, T.; Mütze, L.; Fischer, W.; Saft, C.; Hoffmann, R.; Süssmuth, S.; Schlattmann, P.; Van Duijn, E.; et al. Bupropion for the Treatment of Apathy in Huntington’s Disease: A Multicenter, Randomised, Double-Blind, Placebocontrolled, Prospective Crossover Trial. PLoS ONE 2017, 12, 0173872. [Google Scholar] [CrossRef] [PubMed]
- Maier, F.; Spottke, A.; Bach, J.P.; Bartels, C.; Buerger, K.; Dodel, R.; Fellgiebel, A.; Fliessbach, K.; Frölich, L.; Hausner, L.; et al. Bupropion for the Treatment of Apathy in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e206027. [Google Scholar] [CrossRef] [PubMed]
- Rea, R.; Carotenuto, A.; Traini, E.; Fasanaro, A.M.; Manzo, V.; Amenta, F. Apathy Treatment in Alzheimer’s Disease: Interim Results of the ASCOMALVA Trial. J. Alzheimers. Dis. 2015, 48, 377–383. [Google Scholar] [CrossRef]
- Laplane, D.; Baulac, M.; Widlocher, D.; Dubois, B. Pure Psychic Akinesia with Bilateral Lesions of Basal Ganglia. J. Neurol. Neurosurg. Psychiatry 1984, 47, 377–385. [Google Scholar] [CrossRef]
- Goodwin, V.A.; Richards, S.H.; Taylor, R.S.; Taylor, A.H.; Campbell, J.L. The Effectiveness of Exercise Interventions for People with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Mov. Disord. 2008, 23, 631–640. [Google Scholar] [CrossRef]
- Bloem, B.R.; de Vries, N.M.; Ebersbach, G. Nonpharmacological Treatments for Patients with Parkinson’s Disease. Mov. Disord. 2015, 30, 1504–1520. [Google Scholar] [CrossRef]
- Ng, S.Y.-E.; Chia, N.S.-Y.; Abbas, M.M.; Saffari, E.S.; Choi, X.; Heng, D.L.; Xu, Z.; Tay, K.-Y.; Au, W.-L.; Tan, E.-K.; et al. Physical Activity Improves Anxiety and Apathy in Early Parkinson’s Disease: A Longitudinal Follow-Up Study. Front. Neurol. 2021, 11, 625897. [Google Scholar] [CrossRef]
- King, L.A.; Wilhelm, J.; Chen, Y.; Blehm, R.; Nutt, J.; Chen, Z.; Serdar, A.; Horak, F.B. Effects of Group, Individual, and Home Exercise in Persons With Parkinson Disease: A Randomized Clinical Trial. J. Neurol. Phys. Ther. 2015, 39, 204–212. [Google Scholar] [CrossRef]
- Cugusi, L.; Solla, P.; Serpe, R.; Carzedda, T.; Piras, L.; Oggianu, M.; Gabba, S.; Di Blasio, A.; Bergamin, M.; Cannas, A.; et al. Effects of a Nordic Walking Program on Motor and Non-Motor Symptoms, Functional Performance and Body Composition in Patients with Parkinson’s Disease. NeuroRehabilitation 2015, 37, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Wang, Y.; Juan, Z.; Cong, Y.; Niu, Y.; Yang, J.; Huang, S. Effects of Dance Therapy on Non-Motor Symptoms in Patients with Parkinson ’ s Disease: A Systematic Review and Meta-Analysis. Aging Clin. Exp. Res. 2021, 34, 1201–1208. [Google Scholar] [CrossRef]
- Subramanian, I. Complementary and Alternative Medicine and Exercise in Nonmotor Symptoms of Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 134, 1163–1188. [Google Scholar] [PubMed]
- Manera, V.; Abrahams, S.; Agüera-Ortiz, L.; Bremond, F.; David, R.; Fairchild, K.; Gros, A.; Hanon, C.; Husain, M.; König, A.; et al. Recommendations for the Nonpharmacological Treatment of Apathy in Brain Disorders. Am. J. Geriatr. Psychiatry 2020, 28, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Oguro, H.; Nakagawa, T. Randomized Trial of Repetitive Transcranial Magnetic Stimulation for Apathy and Depression in Parkinson’s Disease. J. Neurol. Neurophysiol. 2014, 5, 1–6. [Google Scholar] [CrossRef]
- Maruo, T.; Hosomi, K.; Shimokawa, T.; Kishima, H.; Oshino, S.; Morris, S.; Kageyama, Y.; Yokoe, M.; Yoshimine, T.; Saitoh, Y. High-Frequency Repetitive Transcranial Magnetic Stimulation over the Primary Foot Motor Area in Parkinson’s Disease. Brain Stimul. 2013, 6, 884–891. [Google Scholar] [CrossRef]
- Wei, W.; Yi, X.; Ruan, J.; Duan, X.; Luo, H. The Efficacy of Repetitive Transcranial Magnetic Stimulation on Emotional Processing in Apathetic Patients with Parkinson’s Disease: A Placebo-Controlled ERP Study. J. Affect. Disord. 2021, 282, 776–785. [Google Scholar] [CrossRef]
- Montoya-Murillo, G.; Ibarretxe-Bilbao, N.; Peña, J.; Ojeda, N. Effects of Cognitive Rehabilitation on Cognition, Apathy, Quality of Life, and Subjective Complaints in the Elderly: A Randomized Controlled Trial. Am. J. Geriatr. Psychiatry 2020, 28, 518–529. [Google Scholar] [CrossRef]
- Díez-Cirarda, M.; Ojeda, N.; Peña, J.; Cabrera-Zubizarreta, A.; Lucas-Jiménez, O.; Gómez-Esteban, J.C.; Gómez-Beldarrain, M.; Ibarretxe-Bilbao, N. Long-Term Effects of Cognitive Rehabilitation on Brain, Functional Outcome and Cognition in Parkinson’s Disease. Eur. J. Neurol. 2018, 25, 5–12. [Google Scholar] [CrossRef]
- Peña, J.; Ibarretxe-Bilbao, N.; García-Gorostiaga, I.; Gomez-Beldarrain, M.A.; Díez-Cirarda, M.; Ojeda, N. Improving Functional Disability and Cognition in Parkinson Disease Randomized Controlled Trial. Neurology 2014, 83, 2167–2174. [Google Scholar] [CrossRef]
- Butterfield, L.C.; Cimino, C.R.; Salazar, R.; Sanchez-Ramos, J.; Bowers, D.; Okun, M.S. The Parkinson’s Active Living (PAL) Program: A Behavioral Intervention Targeting Apathy in Parkinsons Disease. J. Geriatr. Psychiatry Neurol. 2017, 30, 11–25. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Waele, S.; Cras, P.; Crosiers, D. Apathy in Parkinson’s Disease: Defining the Park Apathy Subtype. Brain Sci. 2022, 12, 923. https://doi.org/10.3390/brainsci12070923
De Waele S, Cras P, Crosiers D. Apathy in Parkinson’s Disease: Defining the Park Apathy Subtype. Brain Sciences. 2022; 12(7):923. https://doi.org/10.3390/brainsci12070923
Chicago/Turabian StyleDe Waele, Ségolène, Patrick Cras, and David Crosiers. 2022. "Apathy in Parkinson’s Disease: Defining the Park Apathy Subtype" Brain Sciences 12, no. 7: 923. https://doi.org/10.3390/brainsci12070923
APA StyleDe Waele, S., Cras, P., & Crosiers, D. (2022). Apathy in Parkinson’s Disease: Defining the Park Apathy Subtype. Brain Sciences, 12(7), 923. https://doi.org/10.3390/brainsci12070923