
Entropy Metrics Correlating with Higher Residual Functioning in Patients with Chronic Disorders of Consciousness

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. EEG Recordings and Analysis
2.3. Statistical Analysis
3. Results
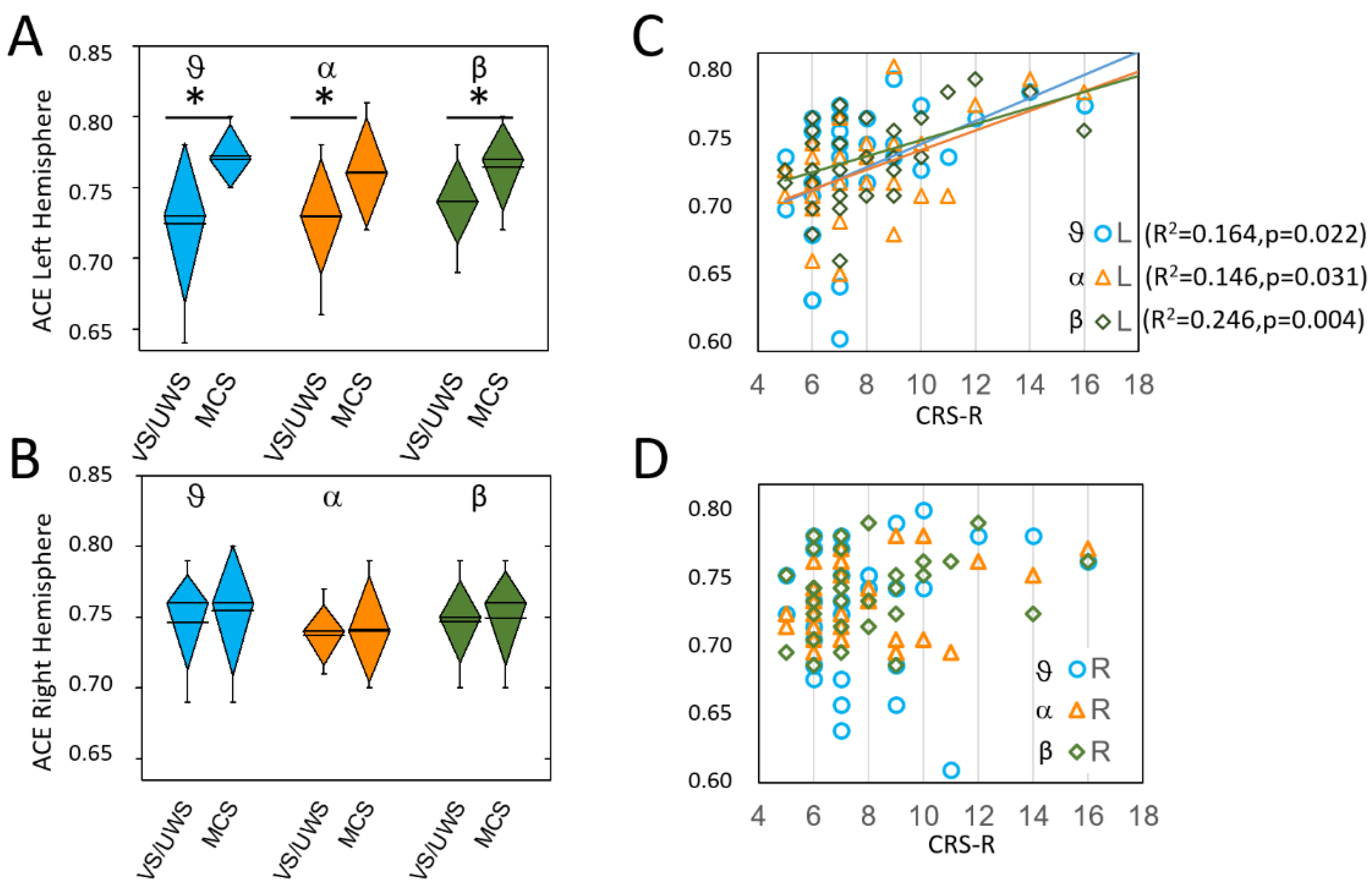
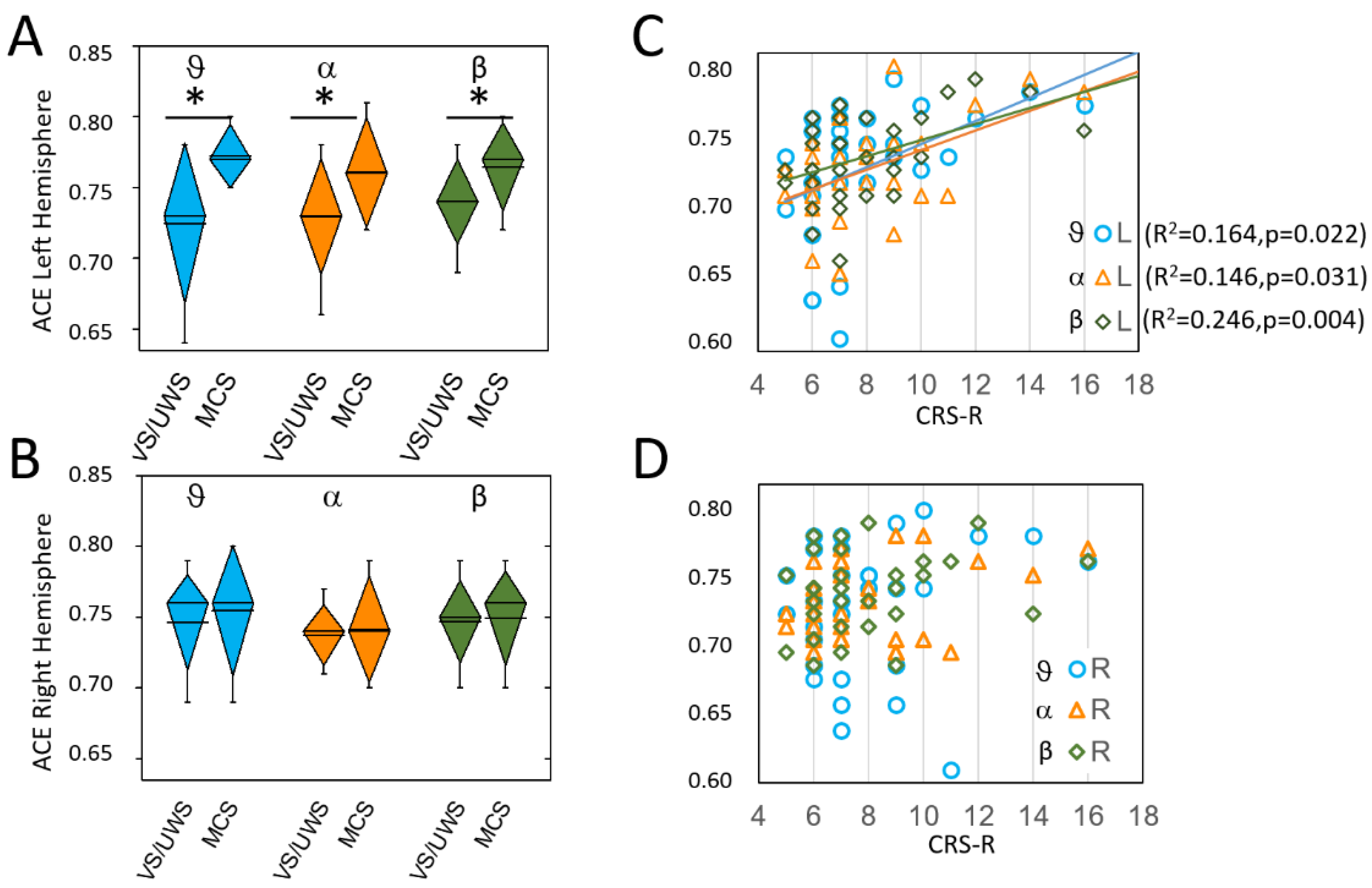
3.1. Interhemispheric Differences
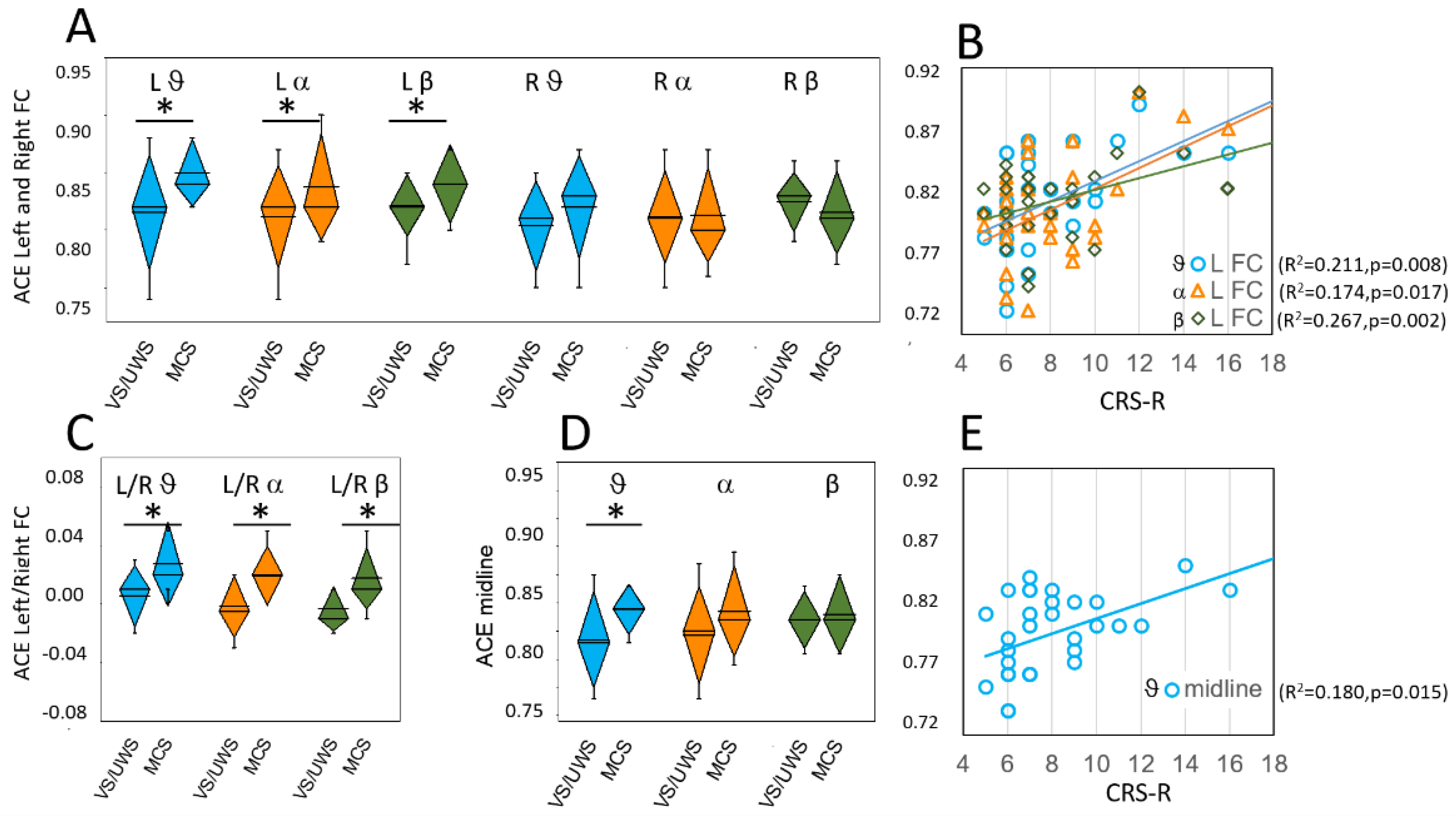
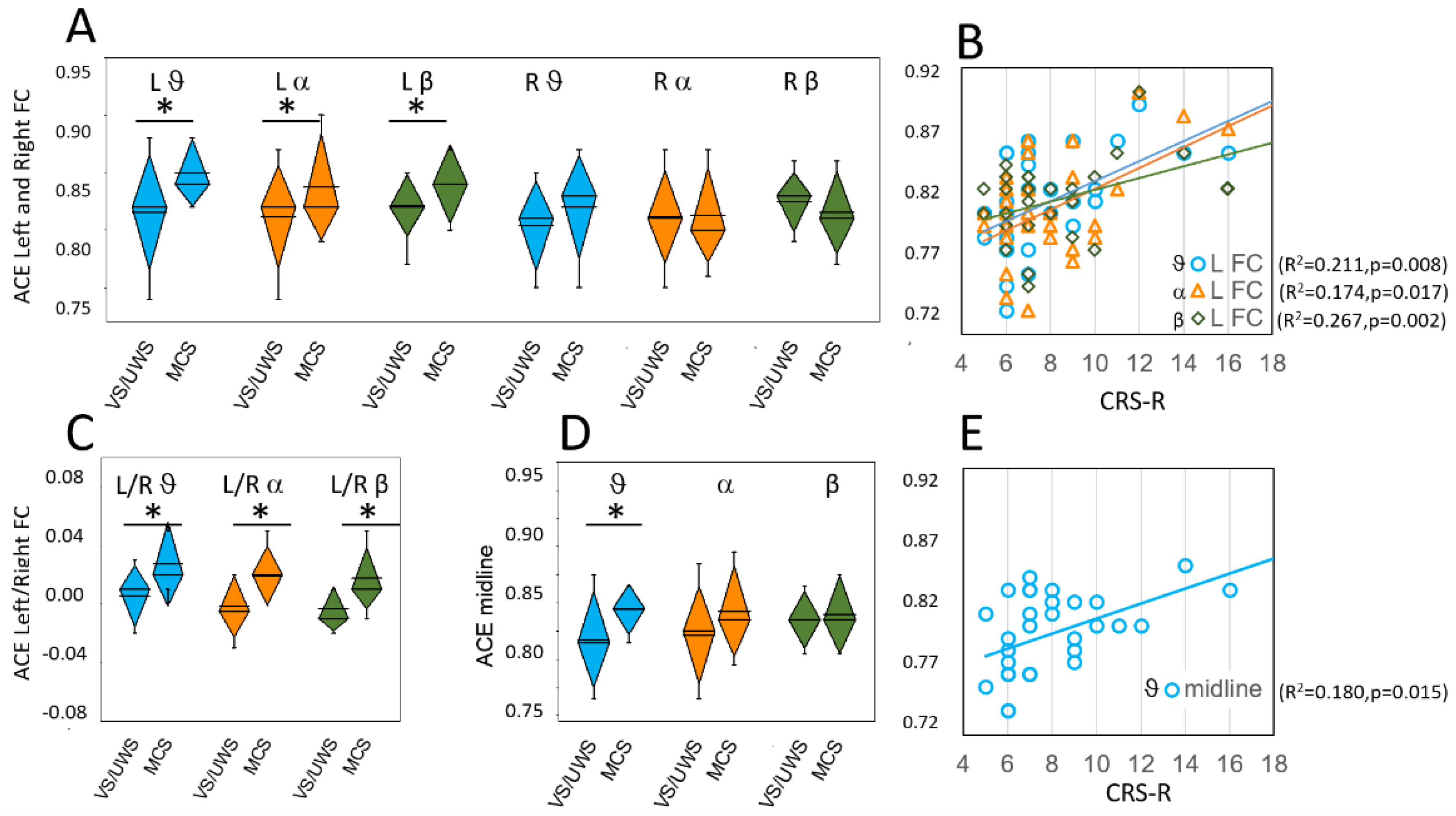
3.2. Selected ROIs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Comanducci, A.; Boly, M.; Claassen, J.; De Lucia, M.; Gibson, R.; Juan, E.; Laureys, S.; Naccache, L.; Owen, A.; Rosanova, M.; et al. Clinical and advanced neurophysiology in the prognostic and diagnostic evaluation of disorders of consciousness: Review of an IFCN-endorsed expert group. Clin. Neurophysiol. 2020, 131, 2736–2765. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Lin, Y.; Ziemann, U. Managing disorders of consciousness: The role of electroencephalography. J. Neurol. 2021, 268, 4033–4065. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Ramakrishnan, A.G. Electrophysiological and Neuroimaging Studies—During Resting State and Sensory Stimulation in Disorders of Consciousness: A Review. Front. Neurosci. 2020, 14, 555093. [Google Scholar] [CrossRef] [PubMed]
- Engemann, D.A.; Raimondo, F.; King, J.-R.; Rohaut, B.; Louppe, G.; Faugeras, F.; Annen, J.; Cassol, H.; Gosseries, O.; Fernandez-Slezak, D.; et al. Robust EEG-based cross-site and cross-protocol classification of states of consciousness. Brain 2018, 141, 3179–3192. [Google Scholar] [CrossRef] [Green Version]
- Chennu, S.; Annen, J.; Wannez, S.; Thibaut, A.; Chatelle, C.; Cassol, H.; Martens, G.; Schnakers, C.; Gosseries, O.; Menon, D.; et al. Brain networks predict metabolism, diagnosis and prognosis at the bedside in disorders of consciousness. Brain 2017, 140, 2120–2132. [Google Scholar] [CrossRef]
- Casarotto, S.; Comanducci, A.; Rosanova, M.; Sarasso, S.; Fecchio, M.; Napolitani, M.; Pigorini, A.; Casali, A.G.; Trimarchi, P.D.; Boly, M.; et al. Stratification of unresponsive patients by an independently validated index of brain complexity. Ann. Neurol. 2016, 80, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef]
- Bruhn, J.; Bouillon, T.; Radulescu, L.; Hoeft, A.; Bertaccini, E.; Shafer, S. Correlation of Approximate Entropy, Bispectral Index, and Spectral Edge Frequency 95 (SEF95) with Clinical Signs of “Anesthetic Depth” during Coadministration of Propofol and Remifentanil. J. Am. Soc. Anesthesiol. 2003, 98, 621–627. [Google Scholar] [CrossRef]
- Wu, D.-Y.; Cai, G.; Yuan, Y.; Liu, L.; Li, G.-Q.; Song, W.-Q.; Wang, M.-B. Application of nonlinear dynamics analysis in assessing unconsciousness: A preliminary study. Clin. Neurophysiol. 2011, 122, 490–498. [Google Scholar] [CrossRef]
- Sebastiano, D.R.; Panzica, F.; Visani, E.; Rotondi, F.; Scaioli, V.; Leonardi, M.; Sattin, D.; D’Incerti, L.; Parati, E.; Strambi, L.F.; et al. Significance of multiple neurophysiological measures in patients with chronic disorders of consciousness. Clin. Neurophysiol. 2015, 126, 558–564. [Google Scholar] [CrossRef]
- Schartner, M.; Seth, A.; Noirhomme, Q.; Boly, M.; Bruno, M.-A.; Laureys, S.; Barrett, A. Complexity of Multi-Dimensional Spontaneous EEG Decreases during Propofol Induced General Anaesthesia. PLoS ONE 2015, 10, e0133532. [Google Scholar] [CrossRef] [PubMed]
- Sattin, D.; Giovannetti, A.M.; Ciaraffa, F.; Covelli, V.; Bersano, A.; Nigri, A.; Ferraro, S.; Minati, L.; Rossi, D.; Duran, D.; et al. Assessment of patients with disorder of consciousness: Do different Coma Recovery Scale scoring correlate with different settings? J. Neurol. 2014, 261, 2378–2386. [Google Scholar] [CrossRef] [PubMed]
- Perrin, F.; Pernier, J.; Bertrand, O.; Echallier, J. Spherical splines for scalp potential and current density mapping. Electroencephalogr. Clin. Neurophysiol. 1989, 72, 184–187. [Google Scholar] [CrossRef]
- Gosseries, O.; Schnakers, C.; Ledoux, D.; Vanhaudenhuyse, A.; Bruno, M.A.; Demertzi, A.; Noirhomme, Q.; Lehembre, R.; Damas, P.; Goldman, S.; et al. Automated EEG entropy measurements in coma, vegetative state/unresponsive wakefulness syndrome and minimally conscious state. Funct. Neurol. 2011, 26, 25–30. [Google Scholar] [PubMed]
- Thul, A.; Lechinger, J.; Donis, J.; Michitsch, G.; Pichler, G.; Kochs, E.F.; Jordan, D.; Ilg, R.; Schabus, M. EEG entropy measures indicate decrease of cortical information processing in Disorders of Consciousness. Clin. Neurophysiol. 2016, 127, 1419–1427. [Google Scholar] [CrossRef]
- Liu, B.; Zhang, X.; Wang, L.; Li, Y.; Hou, J.; Duan, G.; Guo, T.; Wu, D. Outcome Prediction in Unresponsive Wakefulness Syndrome and Minimally Conscious State by Non-linear Dynamic Analysis of the EEG. Front. Neurol. 2021, 12, 510424. [Google Scholar] [CrossRef]
- Stam, C. Nonlinear dynamical analysis of EEG and MEG: Review of an emerging field. Clin. Neurophysiol. 2005, 116, 2266–2301. [Google Scholar] [CrossRef]
- Keshmiri, S. Entropy and the Brain: An Overview. Entropy 2020, 22, 917. [Google Scholar] [CrossRef]
- Raichle, M.E. Two views of brain function. Trends Cogn. Sci. 2010, 14, 180–190. [Google Scholar] [CrossRef]
- Farnes, N.; Juel, B.E.; Nilsen, A.S.; Romundstad, L.G.; Storm, J.F. Increased signal diversity/complexity of spontaneous EEG, but not evoked EEG responses, in ketamine-induced psychedelic state in humans. PLoS ONE 2020, 15, e0242056. [Google Scholar] [CrossRef]
- Schartner, M.M.; Pigorini, A.; Gibbs, S.; Arnulfo, G.; Sarasso, S.; Barnett, L.; Nobili, L.; Massimini, M.; Seth, A.; Barrett, A.B. Global and local complexity of intracranial EEG decreases during NREM sleep. Neurosci. Conscious. 2017, 2017, niw022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aamodt, A.; Nilsen, A.S.; Thürer, B.; Moghadam, F.H.; Kauppi, N.; Juel, B.E.; Storm, J.F. EEG Signal Diversity Varies With Sleep Stage and Aspects of Dream Experience. Front. Psychol. 2021, 12, 655884. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.; Massimini, M.; Boly, M.; Tononi, G. Neural correlates of consciousness: Progress and problems. Nat. Rev. Neurosci. 2016, 17, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Detyniecki, K.; Blumenfeld, H. Consciousness of seizures and consciousness during seizures: Are they related? Epilepsy Behav. 2014, 30, 6–9. [Google Scholar] [CrossRef]
- Albert, M.L.; Silverberg, R.; Reches, A.; Berman, M. Cerebral Dominance for Consciousness. Arch. Neurol. 1976, 33, 453–454. [Google Scholar] [CrossRef]
- Smith, E.; Reznik, S.; Stewart, J.L.; Allen, J.J. Assessing and conceptualizing frontal EEG asymmetry: An updated primer on recording, processing, analyzing, and interpreting frontal alpha asymmetry. Int. J. Psychophysiol. 2017, 111, 98–114. [Google Scholar] [CrossRef]
- Annen, J.; Filippini, M.M.; Bonin, E.; Cassol, H.; Aubinet, C.; Carrière, M.; Gosseries, O.; Thibaut, A.; Barra, A.; Wolff, A.; et al. Diagnostic accuracy of the CRS-R index in patients with disorders of consciousness. Brain Inj. 2019, 33, 1409–1412. [Google Scholar] [CrossRef]
- Piarulli, A.; Bergamasco, M.; Thibaut, A.; Cologan, V.; Gosseries, O.; Laureys, S. EEG ultradian rhythmicity differences in disorders of consciousness during wakefulness. J. Neurol. 2016, 263, 1746–1760. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Region | Frequency Band | VS/UWS vs MCS ACE | VS/UWS vs MCS SCE | VS/UWS vs MCS LZc |
|---|---|---|---|---|
| t(df), p | t(df), p | t(df), p | ||
| Left Hemisphere | 1–30 Hz | t(26.9) = −3.8, p = 0.001 | t(22.8) = −3.0, p = 0.006 | t(30) = −2.1, p = 0.047 * |
| 1–4 Hz | t(26.6) = −2.7, p = 0.012 | t(23.6) = −2.3, p = 0.029 * | t(29.3) = −2.8, p = 0.009 | |
| 4–8 Hz | t(25.4) = −3.3, p = 0.003 | t(23.9) = −2.8, p = 0.010 | t(25.8) = −3.2, p = 0.003 | |
| 8–13 Hz | t(30) = −2.8, p = 0.010 | t(30) = −2.0, p = 0.051 | t(30) = −1.8, p = 0.084 | |
| 13–30 Hz | t(30) = −2.3, p = 0.026 * | t(30) = −1.8, p = 0.075 | t(30) = −1.1, p = 0.275 | |
| Right Hemisphere | 1–30 Hz | t(30) = −0.7, p = 0.504 | t(30) = −0.5, p = 0.621 | t(30) = −1.6, p = 0.114 |
| 1–4 Hz | t(30) = −0.4, p = 0.676 | t(30) = −0.8, p = 0.408 | t(30) = 0.1, p = 0.958 | |
| 4–8 Hz | t(30) = −1.0, p = 0.334 | t(30) = −0.8, p = 0.399 | t(30) = −0.9, p = 0.374 | |
| 8–13 Hz | t(17.1) = −0.3, p = 0.371 | t(18.2) = 0.4, p = 0.697 | t(17.2) = −1.2, p = 0.159 | |
| 13–30 Hz | t(30) = −0.1, p = 0.909 | t(30) = −0.9, p = 0.379 | t(30) = −0.7, p = 0.458 | |
| Midline | 1–30 Hz | t(30) = −2.0, p = 0.051 | t(30) = −1.4, p = 0.179 | t(30) = −2.1, p = 0.041 * |
| 1–4 Hz | t(30) = −1.4, p = 0.161 | t(30) = −1.0, p = 0.307 | t(30) = −1.1, p = 0.287 | |
| 4–8 Hz | t(28.4) = −2.7, p = 0.011 | t(30) = −1.9, p = 0.063 | t(27.6) = −3.60, p = 0.001 | |
| 8–13 Hz | t(30) = −1.4, p = 0.166 | t(30) = −1.3, p = 0.188 | t(30) = −2.4, p = 0.022 | |
| 13–30 Hz | t(30) = −0.4, p = 0.665 | t(30) = −0.5, p = 0.632 | t(30) = −0.5, p = 0.631 | |
| Left fronto-central | 1–30 Hz | t(30) = −2.4, p = 0.025 * | t(30) = −1.6, p = 0.115 | t(30) = −1.9, p = 0.069 |
| 1–4 Hz | t(30) = −1.2, p = 0.259 | t(28.1) = −0.8, p = 0.424 | t(30) = 0.1, p = 0.876 | |
| 4–8 Hz | t(30) = −2.9, p = 0.007 | t(30) = −2.4, p = 0.021 * | t(27.8) = −2.1, p = 0.045 * | |
| 8–13 Hz | t(30) = −3.0, p = 0.005 | t(30) = −2.2, p = 0.039 * | t(30) = −2.1, p = 0.042 * | |
| 13–30 Hz | t(30) = −2.6, p = 0.014 * | t(30) = −1.5, p = 0.131 | t(30) = −0.5, p = 0.598 | |
| Right fronto-central | 1–30 Hz | t(30) = −0.5, p = 0.597 | t(30) = −0.3, p = 0.802 | t(30) = −1.9, p = 0.069 |
| 1–4 Hz | t(30) = −0.3, p = 0.744 | t(30) = −0.6, p = 0.536 | t(30) = 0.8, p = 0.453 | |
| 4–8 Hz | t(30) = −1.3, p = 0.208 | t(30) = −0.8, p = 0.426 | t(30) = −1.3, p = 0.214 | |
| 8–13 Hz | t(30) = −0.2, p = 0.827 | t(30) = −0.1, p = 0.960 | t(30) = −1.8, p = 0.073 | |
| 13–30 Hz | t(30) = 0.7, p = 0.468 | t(30) = 1.0, p = 0.298 | t(30) = −0.4, p = 0.715 | |
| Left parieto-occipital | 1–30 Hz | t(29.6) = −1.9, p = 0.071 | t(30) = −1.5, p = 0.139 | t(30) = −1.7, p = 0.105 |
| 1–4 Hz | t(30) = −1.9, p = 0.064 | t(30) = −1.7, p = 0.101 | t(30) = −1.4, p = 0.157 | |
| 4–8 Hz | t(30) = −1.4, p = 0.182 | t(30) = −1.2, p = 0.236 | t(30) = −1.5, p = 0.188 | |
| 8–13 Hz | t(30) = −0.5, p = 0.619 | t(30) = −0.2, p = 0.842 | t(30) = −0.7, p = 0.470 | |
| 13–30 Hz | t(30) = −1.8, p = 0.089 | t(30) = −0.9, p = 0.374 | t(30) = −0.3, p = 0.723 | |
| Right parieto-occipital | 1–30 Hz | t(30) = −0.7, p = 0.487 | t(30) = −0.7, p = 0.504 | t(30) = −1.5, p = 0.145 |
| 1–4 Hz | t(30) = −0.4, p = 0.702 | t(30) = −0.9, p = 0.366 | t(30) = 0.9, p = 0.376 | |
| 4–8 Hz | t(30) = −0.8, p = 0.448 | t(30) = −0.6, p = 0.536 | t(30) = −1.3, p = 0.215 | |
| 8–13 Hz | t(30) = −0.7, p = 0.501 | t(30) = 0.5, p = 0.597 | t(30) = −1.7, p = 0.098 | |
| 13–30 Hz | t(30) = −0.9, p = 0.368 | t(30) = 0.1, p = 0.960 | t(30) = −0.8, p = 0.430 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visani, E.; Luria, G.; Sattin, D.; Rossi Sebastiano, D.; Ferraro, S.; Panzica, F.; Leonardi, M.; Franceschetti, S. Entropy Metrics Correlating with Higher Residual Functioning in Patients with Chronic Disorders of Consciousness. Brain Sci. 2022, 12, 332. https://doi.org/10.3390/brainsci12030332
Visani E, Luria G, Sattin D, Rossi Sebastiano D, Ferraro S, Panzica F, Leonardi M, Franceschetti S. Entropy Metrics Correlating with Higher Residual Functioning in Patients with Chronic Disorders of Consciousness. Brain Sciences. 2022; 12(3):332. https://doi.org/10.3390/brainsci12030332
Chicago/Turabian StyleVisani, Elisa, Gianvittorio Luria, Davide Sattin, Davide Rossi Sebastiano, Stefania Ferraro, Ferruccio Panzica, Matilde Leonardi, and Silvana Franceschetti. 2022. "Entropy Metrics Correlating with Higher Residual Functioning in Patients with Chronic Disorders of Consciousness" Brain Sciences 12, no. 3: 332. https://doi.org/10.3390/brainsci12030332
APA StyleVisani, E., Luria, G., Sattin, D., Rossi Sebastiano, D., Ferraro, S., Panzica, F., Leonardi, M., & Franceschetti, S. (2022). Entropy Metrics Correlating with Higher Residual Functioning in Patients with Chronic Disorders of Consciousness. Brain Sciences, 12(3), 332. https://doi.org/10.3390/brainsci12030332