

Pulse Pressure Is Associated with Rapid Cognitive Decline over 4 Years: A Population-Based Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
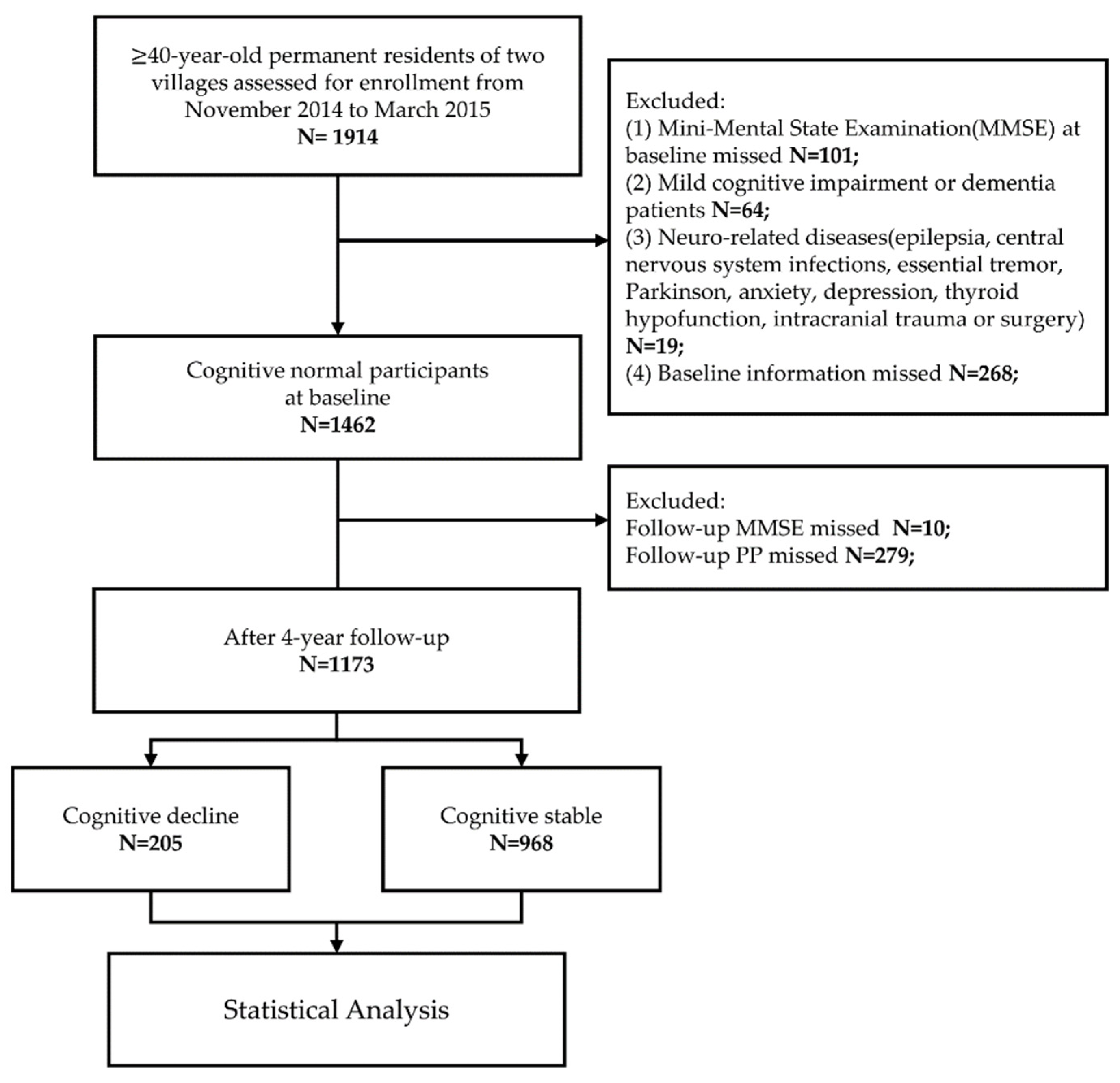
2.2. Study Population
2.3. Standard Interview and Follow-Up
2.4. Cognitive Assessment
2.5. Blood Pressure Measurement
2.6. Laboratory Evaluation
2.7. Definition of Variates
2.8. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population at Baseline
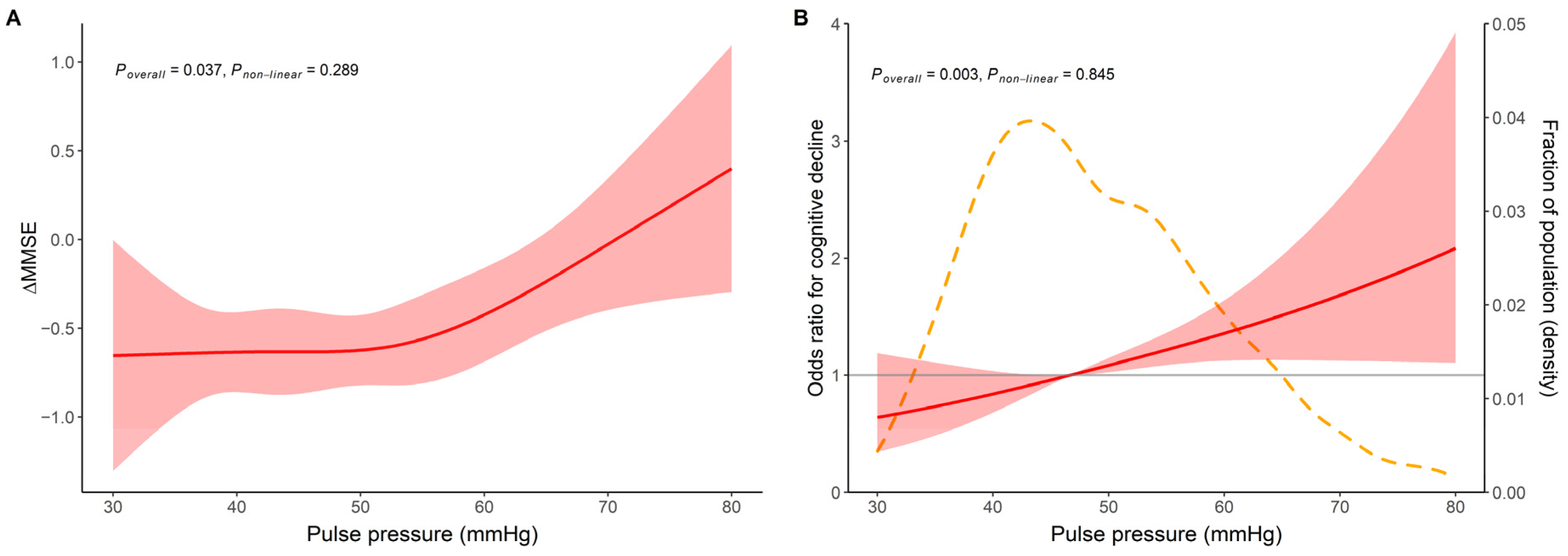
3.2. The Relationship between PP and Cognitive Decline
3.3. Subgroup Analysis of PP and Cognitive Decline
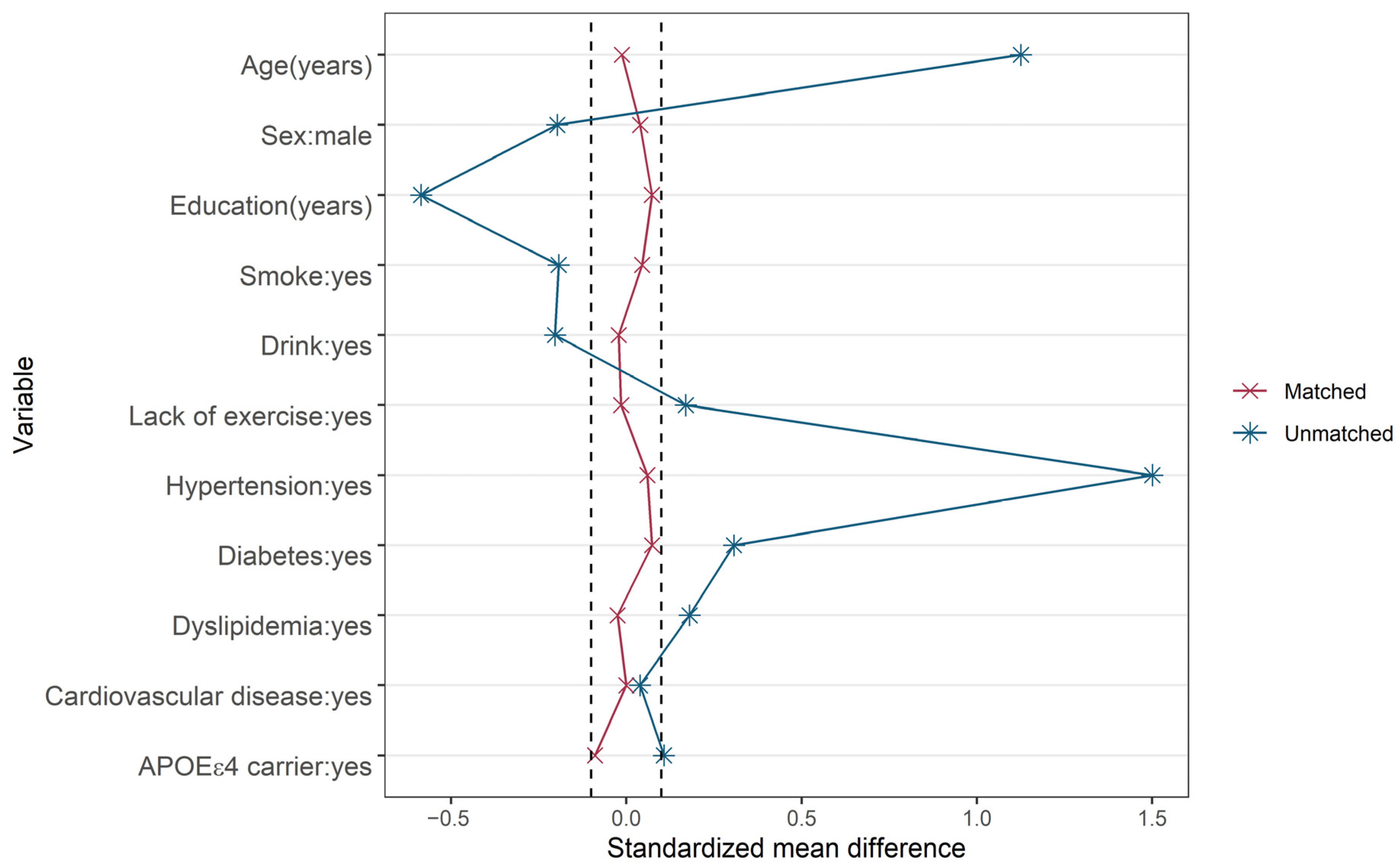
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Association. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement 2021, 17, 327–406. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Faraco, G.; Iadecola, C. Hypertension: A harbinger of stroke and dementia. Hypertension 2013, 62, 810–817. [Google Scholar] [CrossRef] [Green Version]
- Hughes, D.; Judge, C.; Murphy, R.; Loughlin, E.; Costello, M.; Whiteley, W.; Bosch, J.; O’Donnell, M.J.; Canavan, M. Association of Blood Pressure Lowering With Incident Dementia or Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA 2020, 323, 1934–1944. [Google Scholar] [CrossRef]
- Launer, L.J.; Masaki, K.; Petrovitch, H.; Foley, D.; Havlik, R.J.J.J. The association between midlife blood pressure levels and late-life cognitive function: The Honolulu-Asia Aging Study. JAMA 1995, 274, 1846–1851. [Google Scholar] [CrossRef]
- Gottesman, R.F.; Schneider, A.L.; Albert, M.; Alonso, A.; Bandeen-Roche, K.; Coker, L.; Coresh, J.; Knopman, D.; Power, M.C.; Rawlings, A.; et al. Midlife hypertension and 20-year cognitive change: The atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014, 71, 1218–1227. [Google Scholar] [CrossRef] [Green Version]
- Knopman, D.S.; Mosley, T.H.; Catellier, D.J.; Coker, L.H. Atherosclerosis Risk in Communities Study Brain MRI Study. Alzheimers Dement 2009, 5, 207–214. [Google Scholar] [CrossRef]
- Haan, M.N.; Shemanski, L.; Jagust, W.J.; Manolio, T.A.; Kuller, L.J.J. The role of apoe∊ 4 in modulating effects of other risk factors for cognitive decline in elderly persons. JAMA 1999, 282, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Elias, M.F.; Elias, P.K.; Sullivan, L.M.; Wolf, P.A.; D’agostino, R.B. Lower cognitive function in the presence of obesity and hypertension: The Framingham heart study. Int. J. Obes. 2003, 27, 260–268. [Google Scholar] [CrossRef]
- Hebert, L.; Scherr, P.; Bennett, D.; Bienias, J.; Wilson, R.; Morris, M.; Evans, D.J.N. Blood pressure and late-life cognitive function change: A biracial longitudinal population study. Neurology 2004, 62, 2021–2024. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, A.; Baldereschi, M.; Amaducci, L.; Maggi, S.; Grigoletto, F.; Scarlato, G.; Inzitari, D. Cognitive impairment without dementia in older people: Prevalence, vascular risk factors, impact on disability. The Italian Longitudinal Study on Aging. J. Am. Geriatr. Soc. 2000, 48, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.A.; Sharrett, A.R.; Wu, A.; Schneider, A.L.C.; Albert, M.; Lutsey, P.L.; Bandeen-Roche, K.; Coresh, J.; Gross, A.L.; Windham, B.G.; et al. Association of Midlife to Late-Life Blood Pressure Patterns With Incident Dementia. JAMA 2019, 322, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Thorin-Trescases, N.; Thorin, E. Lifelong Cyclic Mechanical Strain Promotes Large Elastic Artery Stiffening: Increased Pulse Pressure and Old Age-Related Organ Failure. Can. J. Cardiol. 2016, 32, 624–633. [Google Scholar] [CrossRef]
- Dart, A.M.; Kingwell, B.A. Pulse pressure—A review of mechanisms and clinical relevance. J. Am. Coll. Cardiol. 2001, 37, 975–984. [Google Scholar] [CrossRef] [Green Version]
- Thorin-Trescases, N.; de Montgolfier, O.; Pincon, A.; Raignault, A.; Caland, L.; Labbe, P.; Thorin, E. Impact of pulse pressure on cerebrovascular events leading to age-related cognitive decline. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H1214–H1224. [Google Scholar] [CrossRef]
- Franklin, S.S.; Khan, S.A.; Wong, N.D.; Larson, M.G.; Levy, D. Is pulse pressure useful in predicting risk for coronary heart Disease? The Framingham heart study. Circulation 1999, 100, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.D.; Shen, X.L.; Zhao, R.; Tao, X.X.; Wang, S.; Zhou, J.J.; Zheng, B.; Zhang, Q.T.; Yao, Q.; Zhao, Y.; et al. Pulse pressure as an independent predictor of stroke: A systematic review and a meta-analysis. Clin. Res. Cardiol. 2016, 105, 677–686. [Google Scholar] [CrossRef]
- Nation, D.A.; Edmonds, E.C.; Bangen, K.J.; Delano-Wood, L.; Scanlon, B.K.; Han, S.D.; Edland, S.D.; Salmon, D.P.; Galasko, D.R.; Bondi, M.W. Pulse pressure in relation to tau-mediated neurodegeneration, cerebral amyloidosis, and progression to dementia in very old adults. JAMA Neurol. 2015, 72, 546–553. [Google Scholar] [CrossRef]
- Lee, A.T.; Chan, W.C.; Chiu, H.F.; Richards, M.; Ng, S.P.; Hui, L.Y.; Chan, W.M.; Lam, L.C. Widened pulse pressure is a potential risk factor for significant cognitive impairment among community-dwelling Chinese younger old people. J. Alzheimer’s Dis. 2013, 35, 687–696. [Google Scholar] [CrossRef]
- Waldstein, S.R.; Rice, S.C.; Thayer, J.F.; Najjar, S.S.; Scuteri, A.; Zonderman, A.B. Pulse pressure and pulse wave velocity are related to cognitive decline in the Baltimore Longitudinal Study of Aging. Hypertension 2008, 51, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, D.A.; Galecki, A.T.; Langa, K.M.; Unverzagt, F.W.; Kabeto, M.U.; Giordani, B.; Cushman, M.; McClure, L.A.; Safford, M.M.; Wadley, V.G. Blood Pressure and Cognitive Decline Over 8 Years in Middle-Aged and Older Black and White Americans. Hypertension 2019, 73, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Pase, M.P.; Pipingas, A.; Kras, M.; Nolidin, K.; Gibbs, A.L.; Wesnes, K.A.; Scholey, A.B.; Stough, C. Healthy middle-aged individuals are vulnerable to cognitive deficits as a result of increased arterial stiffness. J. Hypertens. 2010, 28, 1724–1729. [Google Scholar] [CrossRef] [PubMed]
- Sha, T.; Cheng, W.; Yan, Y. Prospective associations between pulse pressure and cognitive performance in Chinese middle-aged and older population across a 5-year study period. Alzheimers Res. Ther. 2018, 10, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hensel, A.; Angermeyer, M.C.; Riedel-Heller, S.G. Measuring cognitive change in older adults: Reliable change indices for the Mini-Mental State Examination. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1298–1303. [Google Scholar] [CrossRef]
- Stein, J.; Luppa, M.; Maier, W.; Wagner, M.; Wolfsgruber, S.; Scherer, M.; Köhler, M.; Eisele, M.; Weyerer, S.; Werle, J.; et al. Assessing cognitive changes in the elderly: Reliable change indices for the Mini-Mental State Examination. Acta Psychiatr. Scand. 2012, 126, 208–218. [Google Scholar] [CrossRef]
- Mahley, R.W.; Rall, S.C., Jr. Apolipoprotein E: Far more than a lipid transport protein. Annu. Rev. Genom. Hum. Genet. 2000, 1, 507–537. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr. RMS: Regression Modeling Strategies. R package version 6.3-0. Available online: https://CRAN.R-project.org/package=rms (accessed on 20 August 2022).
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. Available online: https://www.R-project.org/ (accessed on 20 August 2022).
- Li, X.; Lyu, P.; Ren, Y.; An, J.; Dong, Y. Arterial stiffness and cognitive impairment. J. Neurol. Sci. 2017, 380, 1–10. [Google Scholar] [CrossRef]
- Riba-Llena, I.; Nafría, C.; Filomena, J.; Tovar, J.L.; Vinyoles, E.; Mundet, X.; Jarca, C.I.; Vilar-Bergua, A.; Montaner, J.; Delgado, P. High daytime and nighttime ambulatory pulse pressure predict poor cognitive function and mild cognitive impairment in hypertensive individuals. J. Cereb. Blood Flow Metab. 2016, 36, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Yaneva-Sirakova, T.; Tarnovska-Kadreva, R.; Traykov, L. Pulse pressure and mild cognitive impairment. J. Cardiovasc. Med. 2012, 13, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wong, A.; Liu, W.; Yang, J.; Chu, W.C.; Au, L.; Lau, A.; Xiong, Y.; Mok, V.C. Pulse Pressure and Cognitive Decline in Stroke Patients With White Matter Changes. J. Clin. Hypertens. 2015, 17, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Rouch, L.; Cestac, P.; Sallerin, B.; Piccoli, M.; Benattar-Zibi, L.; Bertin, P.; Berrut, G.; Corruble, E.; Derumeaux, G.; Falissard, B.; et al. Visit-to-Visit Blood Pressure Variability Is Associated With Cognitive Decline and Incident Dementia: The S.AGES Cohort. Hypertension 2020, 76, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. Test-retest reliable coefficients and 5-year change scores for the MMSE and 3MS. Arch. Clin. Neuropsychol. 2005, 20, 485–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopecek, M.; Bezdicek, O.; Sulc, Z.; Lukavsky, J.; Stepankova, H. Montreal Cognitive Assessment and Mini-Mental State Examination reliable change indices in healthy older adults. Int. J. Geriatr. Psychiatry 2017, 32, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Lipnicki, D.M.; Makkar, S.R.; Crawford, J.D.; Thalamuthu, A.; Kochan, N.A.; Lima-Costa, M.F.; Castro-Costa, E.; Ferri, C.P.; Brayne, C.; Stephan, B.; et al. Determinants of cognitive performance and decline in 20 diverse ethno-regional groups: A COSMIC collaboration cohort study. PLoS Med. 2019, 16, e1002853. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Singh, M. Sex differences in cognitive impairment and Alzheimer’s disease. Front. Neuroendocrinol. 2014, 35, 385–403. [Google Scholar] [CrossRef] [Green Version]
- Ji, H.; Kim, A.; Ebinger, J.E.; Niiranen, T.J.; Claggett, B.L.; Bairey Merz, C.N.; Cheng, S. Sex Differences in Blood Pressure Trajectories Over the Life Course. JAMA Cardiol. 2020, 5, 19–26. [Google Scholar] [CrossRef]
- Licher, S.; Ahmad, S.; Karamujić-Čomić, H.; Voortman, T.; Leening, M.J.G.; Ikram, M.A.; Ikram, M.K. Genetic predisposition, modifiable-risk-factor profile and long-term dementia risk in the general population. Nat. Med. 2019, 25, 1364–1369. [Google Scholar] [CrossRef]
- Frisoni, G.B.; Altomare, D.; Thal, D.R.; Ribaldi, F.; van der Kant, R.; Ossenkoppele, R.; Blennow, K.; Cummings, J.; van Duijn, C.; Nilsson, P.M.; et al. The probabilistic model of Alzheimer disease: The amyloid hypothesis revised. Nat. Rev. Neurosci. 2022, 23, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F. Effects of central arterial aging on the structure and function of the peripheral vasculature: Implications for end-organ damage. J. Appl. Physiol. 2008, 105, 1652–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muiesan, M.L.; Salvetti, M.; Rizzoni, D.; Paini, A.; Agabiti-Rosei, C.; Aggiusti, C.; Bertacchini, F.; Stassaldi, D.; Gavazzi, A.; Porteri, E.; et al. Pulsatile hemodynamics and microcirculation: Evidence for a close relationship in hypertensive patients. Hypertension 2013, 61, 130–136. [Google Scholar] [CrossRef] [Green Version]
- de Montgolfier, O.; Pincon, A.; Pouliot, P.; Gillis, M.A.; Bishop, J.; Sled, J.G.; Villeneuve, L.; Ferland, G.; Levy, B.I.; Lesage, F.; et al. High Systolic Blood Pressure Induces Cerebral Microvascular Endothelial Dysfunction, Neurovascular Unit Damage, and Cognitive Decline in Mice. Hypertension 2019, 73, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Davisson, R.L. Hypertension and cerebrovascular dysfunction. Cell Metab. 2008, 7, 476–484. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Meng, L.; Bi, Y.L.; Zhang, W.; Xu, W.; Shen, X.N.; Ou, Y.N.; Ma, Y.H.; Dong, Q.; Tan, L.; et al. Tau pathologies mediate the association of blood pressure with cognitive impairment in adults without dementia: The CABLE study. Alzheimers Dement 2021, 18, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.D.; Zlokovic, B.V. Neurovascular mechanisms and blood-brain barrier disorder in Alzheimer’s disease. Acta Neuropathol. 2009, 118, 103–113. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Shang, S.; Li, P.; Chen, C.; Dang, L.; Wang, J.; Huo, K.; Deng, M.; Wang, J.; Qu, Q. Pulse pressure is associated with plasma amyloid-β transport dysfunction. J. Hypertens. 2018, 36, 569–579. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | Cognitive Decline | Cognitively Stable | t, Z, or χ2 | p | |
|---|---|---|---|---|---|
| n = 1173 | n = 205 | n = 968 | |||
| Age, years M (IQR) | 54.0 (15.0) | 56.0 (15.0) | 54.0 (14.0) | 2.94 | 0.003 |
| Male (n, %) | 477 (40.7) | 75.0 (36.6) | 402 (41.5) | 1.71 | 0.191 |
| Education, years M (IQR) | 8.0 (4.0) | 7.0 (5.0) | 8.0 (4.0) | 3.46 | 0.001 |
| Smoking (n, %) | 331 (28.2) | 56 (27.3) | 275 (28.4) | 0.10 | 0.752 |
| Drinking (n, %) | 163 (13.9) | 27 (13.2) | 136 (14.0) | 0.11 | 0.741 |
| Lack of exercise (n, %) | 194 (16.5) | 31 (15.1) | 163 (16.8) | 0.36 | 0.548 |
| Dyslipidemia (n, %) | 602 (51.3) | 113 (55.1) | 489 (50.5) | 1.44 | 0.231 |
| Diabetes (n, %) | 142 (12.1) | 30 (14.6) | 112 (11.6) | 1.49 | 0.222 |
| Hypertension (n, %) | 587 (50.0) | 108 (52.7) | 479 (48.5) | 0.69 | 0.405 |
| Cardiovascular disease (n, %) | 68 (5.8) | 14 (6.8) | 54 (5.6) | 0.49 | 0.486 |
| Pulse rate, bpm M (IQR) | 75.0 (10.0) | 75.0 (10.0) | 76.0 (10) | 0.40 | 0.688 |
| BMI, kg/m2 ± SD | 25.4 ± 3.1 | 25.5 ± 3.0 | 25.4 ± 3.2 | 0.39 | 0.697 |
| APOEε4 carriers (n, %) | 181 (15.4) | 28 (13.7) | 153 (15.8) | 0.60 | 0.439 |
| SBP, mmHg ± SD | 131.6 ± 17.7 | 133.5 ± 18.3 | 131.2 ± 17.6 | 1.65 | 0.099 |
| DBP, mmHg ± SD | 82.2 ± 10.7 | 82.2 ± 10.6 | 82.2 ± 10.9 | 0.04 | 0.965 |
| MAP, mmHg ± SD | 98.7 ± 12.1 | 99.3 ± 11.9 | 98.5 ± 12.2 | 0.83 | 0.407 |
| TG, mmol/L M (IQR) | 1.5 (1.0) | 1.5 (1.0) | 1.4 (1.0) | 1.04 | 0.297 |
| TC, mmol/L M (IQR) | 5.0 (1.2) | 5.1 (1.3) | 4.9 (1.2) | 1.05 | 0.315 |
| HDL, mmol/L M (IQR) | 1.35 (0.4) | 1.4 ± (0.4) | 1.4 (0.4) | 0.30 | 0.764 |
| LDL, mmol/L M (IQR) | 3.2 (1.1) | 3.3 (1.2) | 3.2 (1.1) | 0.92 | 0.357 |
| FBG, mmol/L M (IQR) | 5.4 (0.8) | 5.4 (0.8) | 5.4 (0.8) | 0.65 | 0.516 |
| MMSE, M (IQR) | 27 (4) | 28 (4) | 27 (3) | 4.136 | <0.001 |
| B | 95% CI for B | Std. Error | t | p | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Unadjusted | 0.017 | 0.003 | 0.031 | 0.007 | 2.451 | 0.014 |
| Model 1 | 0.019 | 0.003 | 0.034 | 0.008 | 2.315 | 0.021 |
| Model 2 | 0.021 | 0.003 | 0.038 | 0.009 | 2.339 | 0.019 |
| Model 3 | 0.021 | 0.003 | 0.038 | 0.009 | 2.323 | 0.020 |
| B | S.E | Wald | p | OR | 95% CI for OR | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Unadjusted | 0.023 | 0.007 | 11.746 | 0.001 | 1.024 | 1.010 | 1.037 |
| Model 1 | 0.016 | 0.008 | 3.943 | 0.047 | 1.016 | 1.000 | 1.032 |
| Model 2 | 0.019 | 0.009 | 4.439 | 0.035 | 1.019 | 1.001 | 1.037 |
| Model 3 | 0.020 | 0.009 | 5.176 | 0.023 | 1.020 | 1.003 | 1.038 |
| Subgroups | B | 95%CI for B | t | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age a | |||||
| ≤65 years | 0.021 | 0.003 | 0.040 | 2.242 | 0.025 |
| >65 years | 0.010 | −0.031 | 0.051 | 0.470 | 0.639 |
| Sex b | |||||
| Male | 0.036 | 0.011 | 0.061 | 2.832 | 0.005 |
| Female | 0.011 | −0.014 | 0.035 | 0.866 | 0.387 |
| School education c | |||||
| ≤6 years | 0.031 | 0.002 | 0.060 | 2.088 | 0.037 |
| >6 years | 0.013 | −0.008 | 0.035 | 1.255 | 0.210 |
| APOE ε4 carrier d | |||||
| Yes | −0.017 | −0.067 | 0.033 | 0.669 | 0.505 |
| No | 0.027 | 0.008 | 0.046 | 2.796 | 0.005 |
| Hypertension e | |||||
| Yes | 0.027 | 0.004 | 0.050 | 2.346 | 0.019 |
| No | 0.006 | −0.025 | 0.037 | 0.385 | 0.700 |
| Subgroups | No. of Events (%) | OR | 95%CI | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age a | |||||
| ≤65 years | 159 (16.2) | 1.022 | 1.002 | 1.042 | 0.033 |
| >65 years | 46 (24.0) | 1.019 | 0.987 | 1.051 | 0.243 |
| Sex b | |||||
| Male | 75 (15.7) | 1.031 | 1.004 | 1.059 | 0.025 |
| Female | 130 (18.7) | 1.011 | 0.988 | 1.035 | 0.351 |
| School education c | |||||
| ≤6 years | 102 (21.2) | 1.026 | 1.002 | 1.051 | 0.031 |
| >6 years | 103 (14.9) | 1.006 | 0.978 | 1.035 | 0.668 |
| APOE ε4 carrier d | |||||
| Yes | 28 (15.5) | 0.995 | 0.949 | 1.042 | 0.818 |
| No | 177 (17.8) | 1.017 | 1.001 | 1.034 | 0.042 |
| Hypertension e | |||||
| Yes | 108 (18.4) | 1.030 | 1.008 | 1.053 | 0.007 |
| No | 97 (16.6) | 0.993 | 0.960 | 1.027 | 0.692 |
| Linear Regression Analysis | Logistic Regression Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p | B | 95%CI | p | |||
| Total population | ||||||||
| Unadjusted | 1.932 | 1.310 | 2.812 | <0.001 | 0.525 | 0.106 | 0.943 | 0.014 |
| Model 1 | 1.594 | 1.048 | 2.394 | 0.027 | 0.524 | 0.076 | 0.971 | 0.022 |
| Model 2 | 1.631 | 1.049 | 2.513 | 0.028 | 0.530 | 0.061 | 0.999 | 0.027 |
| Model 3 | 1.622 | 1.044 | 2.498 | 0.029 | 0.491 | 0.024 | 0.957 | 0.039 |
| After PSM | ||||||||
| Unadjusted | 1.807 | 1.058 | 3.130 | 0.032 | 0.611 | 0.003 | 1.219 | 0.049 |
| Model 4 | 1.808 | 1.059 | 3.133 | 0.032 | 0.613 | 0.005 | 1.221 | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, R.; Wei, S.; Wang, Y.; Gao, L.; Dang, L.; Shang, S.; Hu, N.; Peng, W.; Zhao, Y.; Yuan, Y.; et al. Pulse Pressure Is Associated with Rapid Cognitive Decline over 4 Years: A Population-Based Cohort Study. Brain Sci. 2022, 12, 1691. https://doi.org/10.3390/brainsci12121691
Zhou R, Wei S, Wang Y, Gao L, Dang L, Shang S, Hu N, Peng W, Zhao Y, Yuan Y, et al. Pulse Pressure Is Associated with Rapid Cognitive Decline over 4 Years: A Population-Based Cohort Study. Brain Sciences. 2022; 12(12):1691. https://doi.org/10.3390/brainsci12121691
Chicago/Turabian StyleZhou, Rong, Shan Wei, Yanyu Wang, Ling Gao, Liangjun Dang, Suhang Shang, Ningwei Hu, Wei Peng, Yi Zhao, Ye Yuan, and et al. 2022. "Pulse Pressure Is Associated with Rapid Cognitive Decline over 4 Years: A Population-Based Cohort Study" Brain Sciences 12, no. 12: 1691. https://doi.org/10.3390/brainsci12121691
APA StyleZhou, R., Wei, S., Wang, Y., Gao, L., Dang, L., Shang, S., Hu, N., Peng, W., Zhao, Y., Yuan, Y., Wang, J., Wang, J., & Qu, Q. (2022). Pulse Pressure Is Associated with Rapid Cognitive Decline over 4 Years: A Population-Based Cohort Study. Brain Sciences, 12(12), 1691. https://doi.org/10.3390/brainsci12121691