
Alzheimer’s Disease and SARS-CoV-2: Pathophysiological Analysis and Social Context

 , and
, and
Abstract
1. Introduction
2. Effect of SARS-CoV-2 in AD Patients
3. Effect of AD on the Severity of Patients with SARS-CoV-2 in Patients
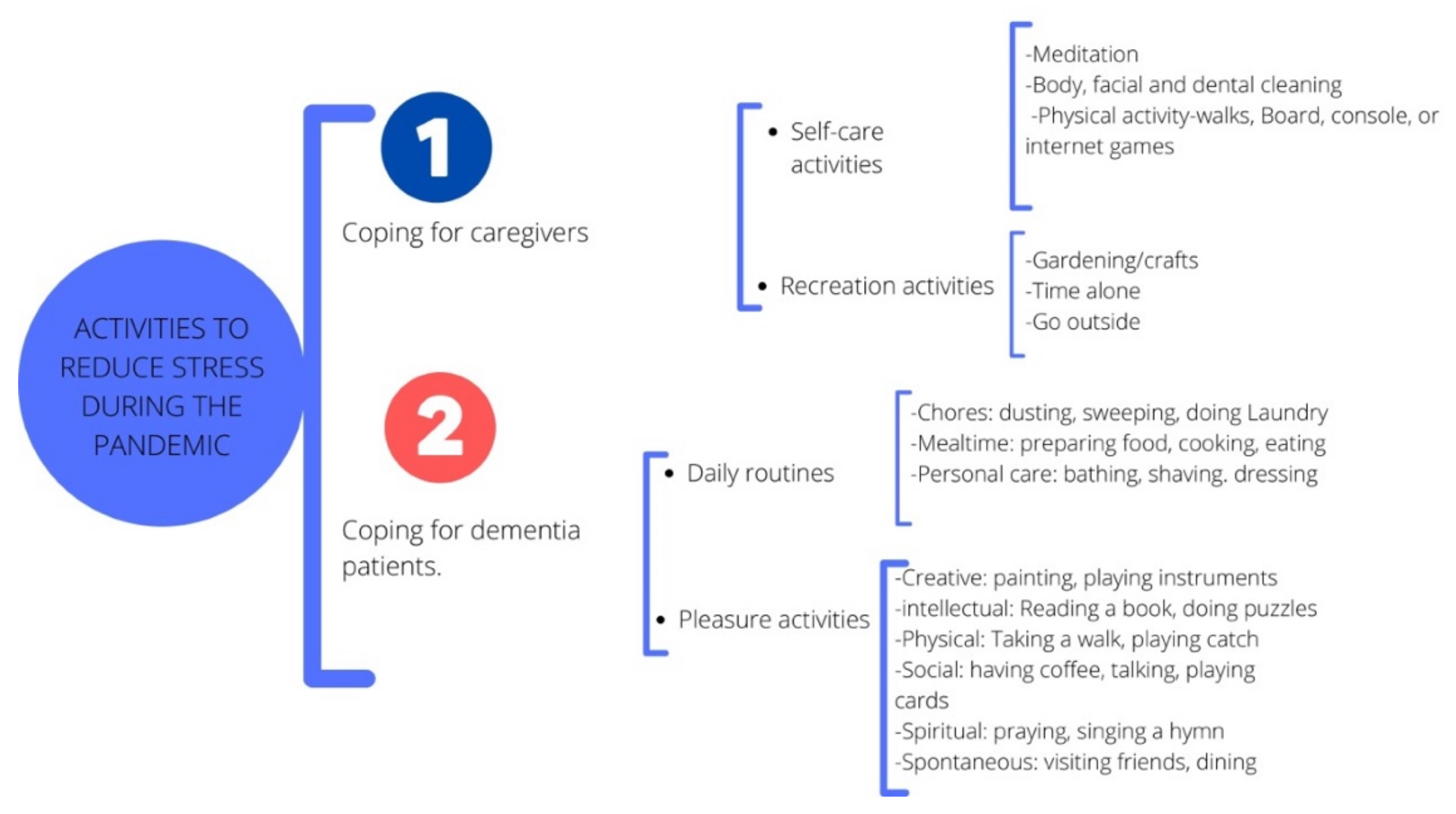
4. Patients with AD in the COVID-19 Pandemic
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garzón, S.J.; Camacho, M.; Tapiero, J.A.; Reina, K.D. Características cognitivas y oculares en enfermedad de Alzheimer. Nova 2018, 16, 101–114. [Google Scholar] [CrossRef][Green Version]
- Kumar, A.; Sidhu, J.; Goyal, A.; Tsao, J.W. Alzheimer Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Mohs, R.C.; Schmeidler, J.; Aryan, M. Longitudinal studies of cognitive, functional and behavioural change in patients with Alzheimer’s disease. Stat. Med. 2000, 19, 1401–1409. [Google Scholar] [CrossRef]
- Barthelson, K.; Pederson, S.M.; Newman, M.; Lardelli, M. Brain transcriptome analysis reveals subtle effects on mitochondrial function and iron homeostasis of mutations in the SORL1 gene implicated in early onset familial Alzheimer’s disease. Mol. Brain 2020, 13, 142. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.A.; Islam, K.; Rahman, S.; Alamin, M. Neurobiochemical cross-talk between COVID-19 and Alzheimer’s disease. Mol. Neurobiol. 2021, 58, 1017–1023. [Google Scholar] [CrossRef]
- Abeysinghe, A.A.D.T.; Deshapriya, R.D.U.S.; Udawatte, C. Alzheimer’s disease; a review of the pathophysiological basis and therapeutic interventions. Life Sci. 2020, 256, 117996. [Google Scholar] [CrossRef]
- AAIC. Global Dementia Cases Forecasted to Triple by 2050 | AAIC 2021. Alzheimer’s Association International Conference (AAIC) 2021 Press Release. 27 July 2021. Available online: https://aaic.alz.org/releases_2021/global-prevalence.asp (accessed on 16 July 2022).
- Hardan, L.; Filtchev, D.; Kassem, R.; Bourgi, R.; Lukomska-Szymanska, M.; Tarhini, H.; Salloum-Yared, F.; Mancino, D.; Kharouf, N.; Haikel, Y. COVID-19 and Alzheimer’s disease: A literature review. Medicina 2021, 57, 1159. [Google Scholar] [CrossRef]
- Armstrong, A.R. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019, 57, 87–105. [Google Scholar] [CrossRef]
- Mazon, J.N.; de Mello, A.H.; Ferreira, G.K.; Rezin, G.T. The impact of obesity on neurodegenerative diseases. Life Sci. 2021, 182, 22–28. [Google Scholar] [CrossRef]
- Chakraborty, A.; Sami, S.A.; Marma, K.K.S. A comprehensive review on RAGE-facilitated pathological pathways connecting Alzheimer’s disease, diabetes mellitus, and cardiovascular diseases. Egypt. J. Intern. Med. 2021, 33, 47. [Google Scholar] [CrossRef]
- Kellar, D.; Craft, S. Brain insulin resistance in Alzheimer’s disease and related disorders: Mechanisms and therapeutic approaches. Lancet Neurol. 2020, 19, 758–766. [Google Scholar] [CrossRef]
- Jeong, W.; Lee, H.; Cho, S.; Seo, J. ApoE4-Induced Cholesterol Dysregulation and Its Brain Cell Type-Specific Implications in the Pathogenesis of Alzheimer’s Disease. Mol. Cells 2019, 42, 739–746. [Google Scholar] [CrossRef]
- Ciaccio, M.; Lo Sasso, B.; Scazzone, C.; Gambino, C.M.; Ciaccio, A.M.; Bivona, G.; Piccoli, T.; Giglio, R.V.; Agnello, L. COVID-19 and Alzheimer’s disease. Brain Sci. 2021, 11, 305. [Google Scholar] [CrossRef]
- Castro-Suarez, S.; Custodio, N. Posibles complicaciones del SARS-COV-2 sobre las funciones neurocognitivas. Rev. Neuro Psiquiatr. 2021, 84, 73–74. [Google Scholar] [CrossRef]
- Bombón-Albán, P.E.; Suárez-Salazar, J.V. Manifestaciones cognitivas y neuropsiquiátricas de COVID-19 en el Adulto Mayor con y sin demencia: Revisión de la literatura. Rev. Neuro Psiquiatr. 2022, 85, 117–126. [Google Scholar] [CrossRef]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 257–261. [Google Scholar] [CrossRef]
- Kouhpayeh, S.; Shariati, L.; Boshtam, M.; Rahimmanesh, I.; Mirian, M.; Esmaeili, Y.; Najaflu, M.; Khanahmad, N.; Zeinalian, M.; Trovato, M.; et al. The molecular basis of COVID-19 pathogenesis, conventional and nanomedicine therapy. Int. J. Mol. Sci. 2021, 22, 5438. [Google Scholar] [CrossRef]
- Pastrian-Soto, G. Bases genéticas y moleculares del COVID-19 (SARS-CoV-2). Mecanismos de patogénesis y de respuesta inmune. Int. J. Odontostomatol. 2020, 14, 331–337. [Google Scholar] [CrossRef]
- Novikov, F.N.; Stroylov, V.S.; Svitanko, I.V.; Nebolsin, V.E. Molecular basis of COVID-19 pathogenesis. Russ. Chem. Rev. 2020, 89, 858. [Google Scholar] [CrossRef]
- WHO. COVID-19 Weekly Epidemiological Update. 16 September 2022. Available online: https://apps.who.int/iris/bitstream/handle/10665/363125/nCoV-weekly-sitrep21Sep22-eng.pdf?sequence=1&isAllowed=y (accessed on 16 July 2022).
- Statista. Número de Casos Confirmados de COVID-19 a Nivel Mundial. Uptdate, Junio. 2022. Available online: https://es.statista.com/estadisticas/1107712/covid19-casos-confirmados-a-nivel-mundial-por-region/ (accessed on 16 July 2022).
- Harapan, B.N.; Yoo, H.J. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Thakur, K.T.; Miller, E.H.; Glendinning, M.D.; Al-Dalahmah, O.; Banu, M.A.; Boehme, A.K.; Boubour, A.L.; Bruce, S.S.; Chong, A.M.; Claassen, J.; et al. COVID-19 neuropathology at columbia university irving medical center/New York presbyterian hospital. Brain 2021, 144, 2696–2708. [Google Scholar] [CrossRef]
- Brown, E.E.; Kumar, S.; Rajji, T.K.; Pollock, B.G.; Mulsant, B.H. Anticipating and mitigating the impact of the COVID-19 pandemic on Alzheimer’s disease and related dementias. Am. J. Geriatr. Psychiatry 2020, 28, 712–721. [Google Scholar] [CrossRef]
- Manca, R.; De Marco, M.; Venneri, A. The Impact of COVID-19 Infection and Enforced Prolonged Social Isolation on Neuropsychiatric Symptoms in Older Adults With and Without Dementia: A Review. Front. Psychiatry 2020, 11, 585540. [Google Scholar] [CrossRef]
- Naughton, S.X.; Raval, U.; Pasinetti, G.M. Potential novel role of COVID-19 in Alzheimer’s disease and preventative mitigation strategies. J. Alzheimer’s Dis. 2020, 76, 21–25. [Google Scholar] [CrossRef]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Lancet 2021, 397, 61–67. [Google Scholar] [CrossRef]
- Kelly, M.P. The relation between the social and the biological and COVID-19. Public Health 2021, 196, 18–23. [Google Scholar] [CrossRef]
- Abate, G.; Memo, M.; Uberti, D. Impact of COVID-19 on Alzheimer’s disease risk: Viewpoint for research action. Healthcare 2020, 8, 286. [Google Scholar] [CrossRef]
- Mok, V.C.T.; Pendlebury, S.; Wong, A.; Alladi, S.; Au, L.; Bath, P.M.; Biessels, G.J.; Chen, C.; Cordonnier, C.; Dichgans, M.; et al. Tackling challenges in care of Alzheimer’s disease and other dementias amid the COVID-19 pandemic, now and in the future. Alzheimer’s Dement. 2020, 16, 1571–1581. [Google Scholar] [CrossRef]
- Magusali, N.; Graham, A.C.; Piers, T.M.; Panichnantakul, P.; Yaman, U.; Shoai, M.; Reynolds, R.H.; Botia, J.A.; Brookes, K.J.; Guetta-Baranes, T.; et al. A genetic link between risk for Alzheimer’s disease and severe COVID-19 outcomes via the OAS1 gene. Brain 2021, 144, 3727–3741. [Google Scholar] [CrossRef]
- Li, J.; Long, X.; Huang, H.; Tang, J.; Zhu, C.; Hu, S.; Wu, J.; Li, J.; Lin, Z.; Xiong, N. Resilience of Alzheimer’s Disease to COVID-19. J. Alzheimer’s Dis. 2020, 77, 67–73. [Google Scholar] [CrossRef]
- Jang, H.; Boltz, D.; Sturm-Ramirez, K.; Shepherd, K.R.; Jiao, Y.; Webster, R.; Smeyne, R.J. Highly pathogenic H5N1 influenza virus can enter the central nervous system and induce neuroinflammation and neurodegeneration. Proc. Natl. Acad. Sci. USA 2009, 106, 14063–14068. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Song, W. The challenges of the COVID-19 pandemic: Approaches for the elderly and those with Alzheimer’s disease. MedComm 2020, 1, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Lana, S.; Marquié, M.; Ruiz, A.; Boada, M. Cognitive and Neuropsychiatric Manifestations of COVID-19 and Effects on Elderly Individuals With Dementia. Front. Aging Neurosci. 2020, 12, 588872. [Google Scholar] [CrossRef] [PubMed]
- Koenigsknecht-Talboo, J.; Landreth, G.E. Microglial phagocytosis induced by fibrillar beta-amyloid and IgGs are differentially regulated by proinflammatory cytokines. J. Neurosci. 2005, 25, 8240–8249. [Google Scholar] [CrossRef]
- Egbert, A.R.; Cankurtaran, S.; Karpiak, S. Brain abnormalities in COVID-19 acute/subacute phase: A rapid systematic review. Brain Behav. Immun. 2020, 89, 543–554. [Google Scholar] [CrossRef]
- Netland, J.; Meyerholz, D.K.; Moore, S.; Cassell, M.; Perlman, S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J. Virol. 2008, 82, 7264–7275. [Google Scholar] [CrossRef]
- Ismail, I.I.; Kamel, W.A.; Al-Hashel, J.Y. Association of COVID-19 pandemic and rate of cognitive decline in patients with dementia and mild cognitive impairment: A cross-sectional study. Gerontol. Geriatr. Med. 2021, 7, 23337214211005223. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, C.; Sun, Y.; Huang, W.; Ye, K. Cognitive disorders associated with hospitalization of COVID-19: Results from an observational cohort study. Brain Behav. Immun. 2021, 91, 383–392. [Google Scholar] [CrossRef]
- Toniolo, S.; Scarioni, M.; Di Lorenzo, F.; Hort, J.; Georges, J.; Tomic, S.; Nobili, F.; Frederiksen, K.S. Dementia and COVID-19, a bidirectional liaison: Risk factors, biomarkers, and optimal health care. J. Alzheimer’s Dis. 2021, 82, 883–898. [Google Scholar] [CrossRef]
- Mamun, A.A.; Uddin, M.; Bashar, B.; Fahim, M.; Zaman, S.; Begum, Y.; Bulbul, I.J.; Islam, M.S.; Sarwar, M.S.; Mathew, B.; et al. Molecular insight into the therapeutic promise of targeting APOE4 for Alzheimer’s disease. Oxid. Med. Cell. Longev. 2020, 2020, 5086250. [Google Scholar] [CrossRef]
- Kuo, C.-L.; Pilling, L.C.; Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Kuchel, G.A.; Melzer, D. APOE e4 genotype predicts severe COVID-19 in the UK Biobank community cohort. J. Gerontol. Ser. A 2020, 75, 2231–2232. [Google Scholar] [CrossRef]
- Goldstein, M.R.; Poland, G.A.; Graeber, A.C. Does apolipoprotein E genotype predict COVID-19 severity? QJM Int. J. Med. 2020, 113, 529–530. [Google Scholar] [CrossRef]
- Itzhaki, R.F.; Lin, W.R.; Shang, D.; Wilcock, G.K.; Faragher, B.; Jamieson, G.A. Herpes simplex virus type 1 in brain and risk of Alzheimer’s disease. Lancet 1997, 349, 241–244. [Google Scholar] [CrossRef]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Politi, L.S.; Salsano, E.; Grimaldi, M. Magnetic resonance imaging alteration of the brain in a patient with coronavirus disease 2019 (COVID-19) and anosmia. JAMA Neurol. 2020, 77, 1028–1029. [Google Scholar] [CrossRef]
- Amaya-Aguilar, J.A.; Olvera-Arreola, S.S.; Sánchez-Cisneros, N.; Lira-Rodríguez, G.; Paredes-Balderas, G.; González-Flores, N.E.; López-Flores, L.; Quintero-Barrios, M.M. El COVID-19 Ha Cobrado Millones De Muertes… Pero ¿ Qué Complicaciones Se Esperan Para Los Sobrevivientes? Rev. Mex. Enfermería Cardiológica 2020, 28, 76–79. [Google Scholar]
- Ding, Q.; Shults, N.V.; Harris, B.T.; Suzuki, Y.J. Angiotensin-converting enzyme 2 (ACE2) is upregulated in Alzheimer’s disease brain. bioRxiv 2020. [Google Scholar] [CrossRef]
- Wang, H.; Lu, J.; Zhao, X.; Qin, R.; Song, K.; Xu, Y.; Zhang, J.; Chen, Y. Alzheimer’s disease in elderly COVID-19 patients: Potential mechanisms and preventive measures. Neurol. Sci. 2021, 42, 4913–4920. [Google Scholar] [CrossRef]
- Finelli, C. Metabolic Syndrome, Alzheimer’s Disease, and Covid 19: A Possible Correlation. Curr. Alzheimer Res. 2021, 18, 915–924. [Google Scholar] [CrossRef]
- Xia, X.; Wang, Y.; Zheng, J. COVID-19 and Alzheimer’s disease: How one crisis worsens the other. Transl. Neurodegener. 2021, 10, 15. [Google Scholar] [CrossRef]
- Amruta, N.; Chastain, W.H.; Paz, M.; Solch, R.J.; Murray-Brown, I.C.; Befeler, J.B.; Gressett, T.E.; Longo, M.T.; Engler-Chiurazzi, E.B.; Bix, G. SARS-CoV-2 mediated neuroinflammation and the impact of COVID-19 in neurological disorders. Cytokine Growth Factor Rev. 2021, 58, 1–15. [Google Scholar] [CrossRef]
- Xiong, N.; Schiller, M.R.; Li, J.; Chen, X.; Lin, Z. Severe COVID-19 in Alzheimer’s disease: APOE4’s fault again? Alzheimers Res. Ther. 2021, 13, 111. [Google Scholar] [CrossRef]
- Bhaskar, S.; Sinha, A.; Banach, M.; Mittoo, S.; Weissert, R.; Kass, J.S.; Rajagopal, S.; Pai, A.R.; Kutty, S. Cytokine Storm in COVID-19-Immunopathological Mechanisms, Clinical Considerations, and Therapeutic Approaches: The REPROGRAM Consortium Position Paper. Front. Immunol. 2020, 11, 1648. [Google Scholar] [CrossRef]
- Ahmad Malik, J.; Ahmed, S.; Shinde, M.; Almermesh, M.H.S.; Alghamdi, S.; Hussain, A.; Anwar, S. The Impact of COVID-19 On Comorbidities: A Review of Recent Updates for Combating It. Saudi J. Biol. Sci. 2022, 29, 3586–3599. [Google Scholar] [CrossRef]
- Boutoleau-Bretonnière, C.; Pouclet-Courtemanche, H.; Gillet, A.; Bernard, A.; Deruet, A.L.; Gouraud, I.; Mazoue, A.; Lamy, E.; Rocher, L.; Kapogiannis, D.; et al. The effects of confinement on neuropsychiatric symptoms in Alzheimer’s disease during the COVID-19 crisis. J. Alzheimer’s Dis. 2020, 76, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Schapira, M. Impacto psicosocial de la pandemia por COVID-19 en adultos mayores con demencia y sus cuidadores. Rev. Argent. Salud Pública 2020, 12, 4. [Google Scholar]
- Simonetti, A.; Pais, C.; Jones, M.; Cipriani, M.C.; Janiri, D.; Monti, L.; Landi, F.; Bernabei, R.; Liperoti, R.; Sani, G. Neuropsychiatric Symptoms in Elderly With Dementia During COVID-19 Pandemic: Definition, Treatment, and Future Directions. Front. Psychiatry 2020, 11, 579842. [Google Scholar] [CrossRef]
- Lara, B.; Carnes, A.; Dakterzada, F.; Benitez, I.; Piñol-Ripoll, G. Neuropsychiatric symptoms and quality of life in Spanish patients with Alzheimer’s disease during the COVID-19 lockdown. Eur. J. Neurol. 2020, 27, 1744–1747. [Google Scholar] [CrossRef]
- Bacsu, J.D.R.; O’Connell, M.E.; Webster, C.; Poole, L.; Wighton, M.B.; Sivananthan, S. A scoping review of COVID-19 experiences of people living with dementia. Can. J. Public Health Rev. Can. Sante Publique 2020, 112, 400–411. [Google Scholar] [CrossRef]
- Canadian Academy of Health Sciences. Improving the Quality of Life and Care of Persons Living with Dementia and Their Caregivers Canadian Academy of Health Sciences’ Assessment of Dementia Care in Canada. Available online: https://cahs-acss.ca/improving-the-quality-of-life-and-care-of-persons-living-with-dementia-and-their-caregivers/ (accessed on 5 July 2022).
- Garrod, L.; Fossey, J.; Henshall, C.; Williamson, S.; Coates, A.; Green, H. Evaluating dementia training for healthcare staff. J. Ment. Health Train. 2019, 14, 277–288. [Google Scholar] [CrossRef]
- Olson, N.L.; Albensi, B.C. Dementia-Friendly “Design”: Impact on COVID-19 Death Rates in Long-Term Care Facilities Around the World. J. Alzheimer’s Dis. JAD 2021, 81, 427–450. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. Actividades en el Hogar. Planificación del Día para una Persona Que vive con Alzheimer en Etapa Media o Avanzada. 2018. Available online: https://www.alz.org/media/documents/activities-alzheimers-spanish-ts.pdf (accessed on 31 July 2022).
- Lee, H.S.; Park, S.W.; Park, Y.J. Effects of Physical Activity Programs on the Improvement of Dementia Symptom: A Meta-Analysis. BioMed. Res. Int. 2016, 2016, 2920146. [Google Scholar] [CrossRef] [PubMed]
- Hung, L.; Levine, H.; Randhawa, P.; Park, J. Protocol: Technology-based group exercise interventions for people living with dementia or mild cognitive impairment: A scoping review protocol. BMJ Open 2022, 12, e055990. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, T.; Okubo, Y.; Woodbury, A.; Lord, S.R.; Delbaere, K. Adherence to Technology-Based Exercise Programs in Older Adults: A Systematic Review. J. Geriatr. Phys. Ther. 2018, 41, 49–61. [Google Scholar] [CrossRef]
- Geddes, M.R.; O’Connell, M.E.; Fisk, J.D.; Gauthier, S.; Camicioli, R.; Ismail, Z.; Alzheimer Society of Canada Task Force on Dementia Care Best Practices for COVID-19. Remote cognitive and behavioral assessment: Report of the Alzheimer Society of Canada Task Force on dementia care best practices for COVID-19. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12111. [Google Scholar] [CrossRef]
- Gosse, P.J.; Kassardjian, C.D.; Masellis, M.; Mitchell, S.B. Virtual care for patients with Alzheimer disease and related dementias during the COVID-19 era and beyond. Can. Med. Assoc. J. 2021, 193, E371–E377. [Google Scholar] [CrossRef]
- Yi, J.S.; Pittman, C.A.; Price, C.L.; Nieman, C.L.; Oh, E.S. Telemedicine and Dementia Care: A Systematic Review of Barriers and Facilitators. J. Am. Med. Dir. Assoc. 2021, 22, 1396–1402.e18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Study | n | Principal Findings and Characteristics of the Study | Reference |
|---|---|---|---|
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6, IL-1 and GAL-9 and 3 in patients with COVID-19 and AD. In contrast, CKAP4 was identified as elevated only in patients with COVID-19. The increase in inflammation was probably related to the increase in mortality due to COVID-19 and the progression of AD by increasing the production of Aβ plates. An increase in GAL-9 and 3 can make it easier for SARS-CoV-2 to enter the lungs. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD, and this may be associated with increased risk of severe stages of COVID-19; allele 4ε increases CNS fibrinogenesis in AD. ACE2: high levels are reported in patients with COVID-19 and AD, which may indicate an increased risk of developing these co-morbidities. Oxidative stress: increased NO production in patients with both co-morbidities. | [5] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6 in patients with COVID-19 and AD. IL-6: positively correlates with the severity of COVID-19, which can have an impact on neurodegeneration. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD. Increased expression of this allele is associated with immunosuppression in patients with SARS-CoV-2 and increased risk of AD. ACE2: high levels are reported in patients with COVID-19 and AD. Highly expressed in patients with AD results in a higher rate of invasion and distribution of SARS-CoV-2. Oxidative stress: increased NO production in patients with both co-morbidities. Elevated concentrations of NO can affect neurotoxicity. | [31] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: the increased levels of IL-6 and TNFα in patients with COVID-19, increased the hyperphosphorylation of the Tau protein and caused the accumulation of plaque Aβ and impaired memory. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD. APOE 4 ε increased risk of infection and mortality by COVID-19 and genetic risk factor of AD. ACE2: high levels are reported only in patients with COVID-19. High expression in neurons and glial cells, possibly associated with neuronal death from SARS-CoV-2 infection. | [37] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: IL-6 levels have increased in patients with COVID-19, which could exacerbate the damage to BBB and neural and glial cells with long-term sequelae. Microglia loses its ability to phagocyte plaque Aβ. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD, its net increase can promote vulnerability to viral infection. ACE2: high levels are reported only in patients with COVID-19, may be associated with damage to neurons. | [16] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Letter to editor | NAP | Pathophysiological response Inflammation: In general, the authors only mention an increase in inflammatory response in patients with COVID-19 and AD. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD. ACE2: high levels are reported in patients with COVID-19 and AD. No additional information is provided for inflammation, APOE 4 ε or ACE2. | [15] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: the author suggests that it is important to evaluate patients who had long-term COVID-19 infection to know the neurological repercussions. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6, IL-1β, IL-12, GAL-3 and TNFα in patients with COVID-19 and AD. Systemic inflammation induces activation of microglia and astrocytes, releasing pro-inflammatory cytokines associated with AD and COVID-19 patients. For GAL-3 elevated levels occur in severe COVID-19 and AD patients, promoting Aβ aggregation. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD, and this is a risk factor for AD and SARS-CoV-2, particularly for developing severe stages. ACE2: high levels are reported in patients with COVID-19 and AD; the increased expression may be a risk factor for SARS-CoV-2 infection mediated by increased oxidative stress. Oxidative stress: increased ROS production in patients with both co-morbidities. | [14] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Systematic review and meta-analysis | NAP | Pathophysiological response Inflammation: increased rates of IL-6 in patients with COVID-19. In all studies analyzed, elevated levels were found, particularly in patients with severe evolution due to SARS-CoV-2, as the level of IL-6 was positively correlated with bilateral lung damage (r = 0.45, P = 0.002). | [48] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Commentary | NAP | Pathophysiological response Inflammation: the authors generally report that a storm of inflammatory cytokines is released in patients with COVID-19. APOE 4 ε: this study shows increased expression for patients with COVID-19. It is reported at a high number of copies predisposing to the development of a more severe stage by SARS-CoV-2. No other information is provided for ACE2 or oxidative stress. | [46] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6, IL-1β, IL-17 and TNFα in patients with COVID-19 and AD. The increased cytokines damage different regions of the brain. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD, it is an allele that increases the risk of developing AD. ACE2: high levels are reported in patients with COVID-19 and AD; greater expression increases the probability of binding with SARS-CoV-2 and its permeability through the BBB. Oxidative stress: increased ROS production in patients with both co-morbidities. | [8] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Letter to editor | 451.367 | Pathophysiological response APOE 4 ε: increased expression is reported in patients with COVID-19 and AD; there is an increase of 14 times more risk of developing AD in European population. The APOE4ε allele increases the risk of serious COVID-19 infection, independent of pre-existing dementia. No other information is provided for inflammation, ACE2 or oxidative stress. | [45] |
| Study specifications Data from the participants and the study: age range between 48 and 86 years; of genetically European descent, the sample size of 451,367 corresponds to 90% of the sample of reference centers in England. A logistic regression model was used. | |||
| Retrospective cohort study | G1: 19G2: 23 | Pathophysiological response ACE2: high levels are reported in patients with COVID-19; the authors report a reduction in the ACE2 receptor in patients with AD and propose a decrease in hospitalization time for patients with COVID-19 and AD. No other information is provided for inflammation, APOE 4 ε or oxidative stress. | [34] |
| Study specifications Data from the participants and the study: This study included 19 patients with AD (G1, Group 1) and 23 patients without AD (G2, Group 2), both from groups with a diagnosis of COVID-19. Participants have an age range of 65 to 100 years, with a value of Minimental >19 points, and patients with other neurological diseases and psychiatric diseases were excluded. | |||
| Original | 2547 | Pathophysiological response Inflammation: increased rates of TNFα and IFNγ in patients with AD. Systemic inflammation leads to increased proinflammatory cytokines associated with more serious phases of COVID-19 and AD. No other information is provided for APOE 4 ε, ACE2 or oxidative stress. | [33] |
| Study specifications Data from the participants and the study: 2547 DNA samples were collected from different UK research institutes of the UK Alzheimer Research Network, which were divided into 1313 AD cases and 1234 controls. | |||
| Postmortem case series | 43 | Pathophysiological response Inflammation: SARS-CoV-2 is linked to an increase in cytokine storm, resulting in neuroimmune stimulation and systemic damage. No other information is provided for inflammation. ACE2: high levels are reported in patients with COVID-19, and it had a higher expression in oligodendrocytes. No additional information is provided for APOE 4 ε, or oxidative stress. | [24] |
| Study specifications Data from the participants and the study: Participants were 51 to 94 years old; inclusion criteria included a positive diagnosis of COVID-19; 16 were female and 27 were male. 13 participants had pre-existing neurologic conditions, with viral pneumonia as the cause of death. | |||
| Commentary | NAP | Pathophysiological response Inflammation: increased levels of IL-1 and IL-6 in patients with COVID-19 and AD. Both patologies activate the microglia and stimulate an increase in the cytokine storm. No other information is provided for APOE 4 ε, ACE2 or oxidative stress. | [28] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of NLRP3, IL-1β, IL-6, IL-17 and TNFα in patients with COVID-19 and AD. NLRP3 stimulates the ORF3 protein of the SARS-CoV-2 virus, which induces inflammatory activation leading to unregulated hyperinflammation, at the same time increasing the production of IL-1β induces neuroinflammation, neural death and cognitive deficiency involved in the pathogenesis of AD. ACE2: high levels are reported in patients with COVID-19 and AD; this study agrees with other authors that ACE2 receptor increases and oxidative stress increases. Oxidative stress: increased ROS production in patients with both co-morbidities. No other information is provided for APOE 4 ε. | [52] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Perspective article | NAP | Pathophysiological response Inflammation: increased rates of TNFα, IL-6, IL-8, IL-10 and NLRP3 in patients with COVID-19 and AD. Increased levels of inflammation are associated with mortality and severe progression of SARS-CoV-2 and its responsiveness to infection control. Additionally, chronic inflammation is linked to the onset of AD. No additional information is provided for inflammation. No other information is provided for APOE 4 ε, ACE2 and oxidative stress. | [53] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-1 IL-6, TNFα and IFNγ in patients with COVID-19 and AD. SARS-CoV-2 activates the procapoptotic pathway through hyperinflammation and a cytokines storm that can trigger a systemic inflammatory response. Regarding Alzheimer’s, it is unclear if neuroinflammation is an underlying cause or if neuroinflammation contributes to the development of Alzheimer’s. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD, and APOE 4 ε is a higher-risk gene of AD that may be implicated in severe SARS-CoV-2 infection. ACE2: high levels are reported in patients with COVID-19 and AD. High ACE2 synthesis in patients with AD may facilitate the invasion of SARS-CoV-2 into the CNS and speed up viral transmission. Oxidative stress: increased ROS production in patients with both co-morbidities. | [54] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6, IL-10, and TNFα in patients with COVID-19 and AD. A heightened inflammatory response affects neural damage and induces neurological changes. APOE 4 ε: increased expression is reported in patients with COVID-19 and AD. APOE 4 ε increases the risk of COVID-19 infection. ACE2: high levels are reported in patients with COVID-19 and AD. This increase has an impact on vulnerability to infiltration and SARS-CoV-2 infection. Oxidative stress: increased ROS production in patients with both co-morbidities. | [55] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Commentary | NAP | Pathophysiological response APOE 4 ε: increased expression is reported in patients with COVID-19 and AD. This is a variant that increases the risk not only of developing AD, but also of being susceptible to SARS-CoV-2 infection. ACE2: have been missed in this study. No other information is provided for inflammation and oxidative stress. | [56] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. The authors worked with a MetaCore analysis, with a sample size of ten patients with AD, in a cohort study. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-6, TNFα, IL-1β, IL-8 and NLRP3 in patients with COVID-19 and AD. The authors suggest SARS-CoV-2-induced hyperinflammatory status. ACE2: high levels are reported in patients with COVID-19 and lower rates in patients with AD. For this study, the authors suggest lower levels of ACE2 in CNS tissues, such that it is assumed that SARS-CoV-2 generates little CNS inflammation. Oxidative stress: increased ROS production in patients with both co-morbidities. The authors support other studies described here about oxidative levels. No other information is provided for APOE 4 ε. | [57] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. | |||
| Review | NAP | Pathophysiological response Inflammation: increased rates of IL-2, IL-6, IL-15, and TNFα in patients with COVID-19 and SNC. In this study, SARS-CoV-2 is reported to increase pro-inflammatory status within the CNS. ACE2: high levels are reported in patients with COVID-19 and lower rates in SNC. In this study, the high number of ACE2 receptors facilitates entry to SARS-CoV-2, and the authors suggest that the distribution of receptors in the CNS is not enough to describe viral neurotropism. Oxidative stress: increased ROS production in patients with COVID-19. The authors support the oxidative response described in other studies included in this table. No other information is provided for APOE 4 ε. | [58] |
| Study specifications Statistical data: NAP; Progression stage of patients with AD: NAP; Age range of participants: NAP; Long-term effects: NA. |
| Area | Improvement |
|---|---|
| Lighting |
|
| Colors |
|
| Signage |
|
| Outdoor spaces |
|
| Others |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz, G.G.; Velázquez-Brizuela, I.E.; Ortiz-Velázquez, G.E.; Ocampo-Alfaro, M.J.; Salazar-Flores, J.; Delgado-Lara, D.L.C.; Torres-Sanchez, E.D. Alzheimer’s Disease and SARS-CoV-2: Pathophysiological Analysis and Social Context. Brain Sci. 2022, 12, 1405. https://doi.org/10.3390/brainsci12101405
Ortiz GG, Velázquez-Brizuela IE, Ortiz-Velázquez GE, Ocampo-Alfaro MJ, Salazar-Flores J, Delgado-Lara DLC, Torres-Sanchez ED. Alzheimer’s Disease and SARS-CoV-2: Pathophysiological Analysis and Social Context. Brain Sciences. 2022; 12(10):1405. https://doi.org/10.3390/brainsci12101405
Chicago/Turabian StyleOrtiz, Genaro Gabriel, Irma E. Velázquez-Brizuela, Genaro E. Ortiz-Velázquez, María J. Ocampo-Alfaro, Joel Salazar-Flores, Daniela L. C. Delgado-Lara, and Erandis D. Torres-Sanchez. 2022. "Alzheimer’s Disease and SARS-CoV-2: Pathophysiological Analysis and Social Context" Brain Sciences 12, no. 10: 1405. https://doi.org/10.3390/brainsci12101405
APA StyleOrtiz, G. G., Velázquez-Brizuela, I. E., Ortiz-Velázquez, G. E., Ocampo-Alfaro, M. J., Salazar-Flores, J., Delgado-Lara, D. L. C., & Torres-Sanchez, E. D. (2022). Alzheimer’s Disease and SARS-CoV-2: Pathophysiological Analysis and Social Context. Brain Sciences, 12(10), 1405. https://doi.org/10.3390/brainsci12101405