
The Effect of Cannabis-Based Medicine on Neuropathic Pain and Spasticity in Patients with Multiple Sclerosis and Spinal Cord Injury: Study Protocol of a National Multicenter Double-Blinded, Placebo-Controlled Trial

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
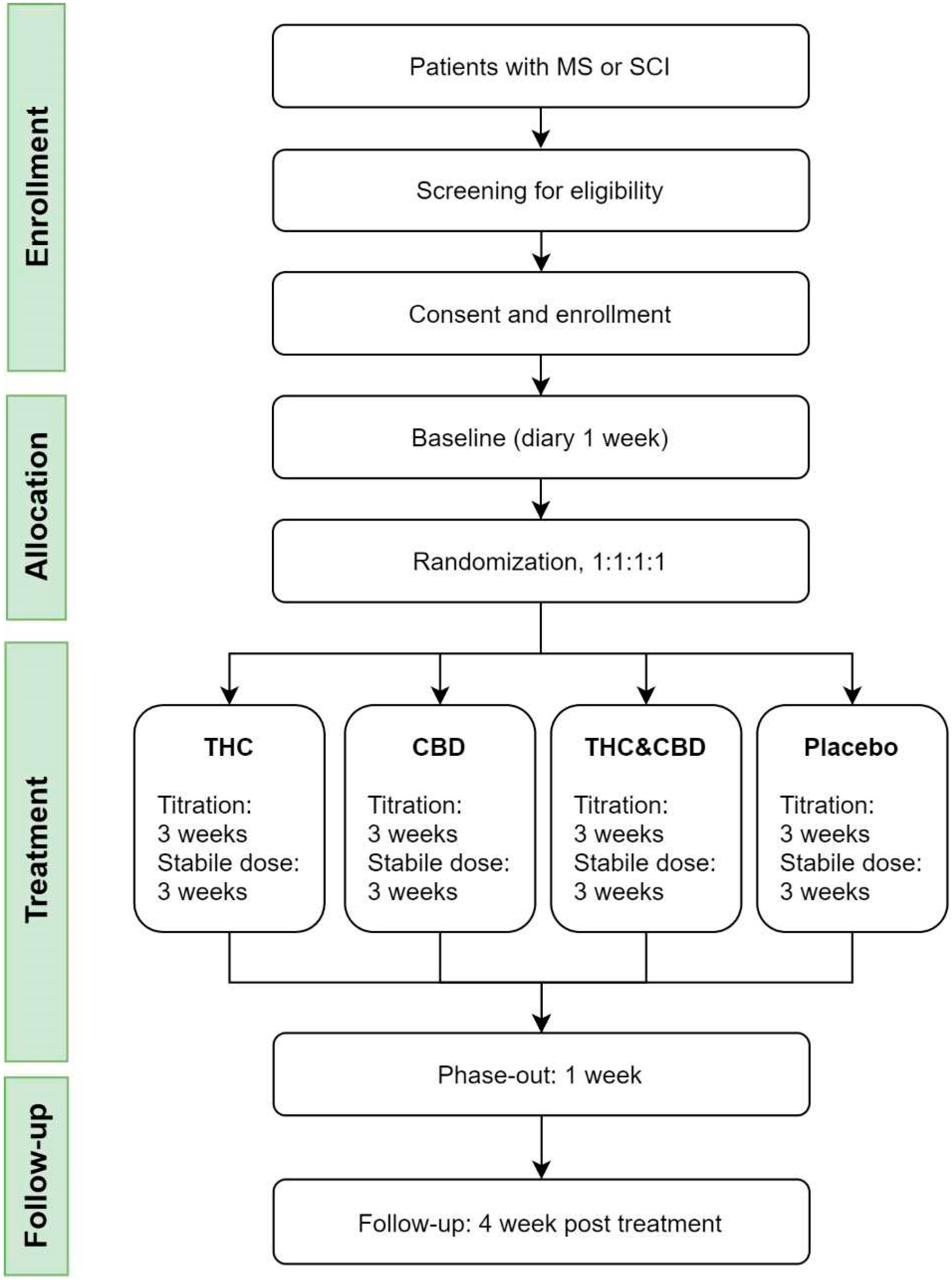
2.1. Study Design and Settings
2.2. Study Subjects
2.2.1. The Main Study
2.2.2. The Sub-Study
2.3. Study Visits
2.4. Randomization and Blinding
2.5. Intervention
- (1)
- Dronabinol (THC): Dronabinol natural DAC 2.5 mg (maximum daily dose 22.5 mg); or
- (2)
- Cannabidiol (CBD): Cannabidiol, synthetic DAC 5 mg or (maximum daily dose 45 mg); or
- (3)
- Dronabinol (THC) + Cannabidiol (CBD): Dronabinol natural DAC 2.5 mg and Cannabidiol, synthetic DAC 5 mg (maximum daily dose 22.5 mg THC and 45 mg CBD); or
- (4)
- Placebo: No active components.
2.6. Outcome Measures
- (1)
- Pain intensity (PI): Average pain score in the diary during the past 7 days of active treatment at a stable dose (week 6) compared with the 7-day baseline period (NRS 0–10, where 0 is no pain and 10 is the worst possible pain).
- (2)
- Degree of spasticity: Average spasticity score in the diary during the past 7 days of active treatment at a stable dose (week 6) compared with the 7-day baseline period (NRS 0–10, where 0 is no spasticity and 10 is the worst possible spasticity).
- (1)
- Patient Global Impression of Change (PGIC, 7-point scale from greatly worsened to greatly improved)
- (2)
- Quality of Life (EQ-5D) [53]
- (1)
- Number of responders with 50% pain reduction/50% reduction of spasticity (diary)
- (2)
- Pain relief and relief of spasticity (complete, good, moderate, mild, no, worsening, diary)
- (3)
- The effect on various pain symptoms (NPSI) [54]
- (4)
- Use of escape medicine (paracetamol, diary)
- (5)
- Spasticity assessed on the Modified Ashworth Scale [55]
- (6)
- The influence of pain and spasticity on activities, mood, and sleep (NRS 0–10, diary)
- (7)
- Sleep (rated with NRS; 0: No sleep problems; 10: Worst possible sleep problems, diary)
- (8)
- Sleep (PROMIS, diary) [56]
- (9)
- Stress (PASAT, questionnaire) [57]
- (10)
- Cognition (SDMT, Symbol Digit Modalities Test) [58]
- (11)
- Coordination (MS), 9-hole peg test [59]
- (12)
- Anxiety and depression (PROMIS, diary) [60]
- (13)
- Patient’s expectation of pain relief (diary) (predictor)
- (14)
- Trail Making Test A and B [61]
- (15)
- Blinding (the patient must indicate what he/she thinks he/she has received at week 3 and 6)
- (16)
- Side-effects (e-diary and visits) (list; dry mouth, headache, depression, nightmare, euphoria, dizziness, tinnitus, anxiety, hallucinations, fatigue/drowsiness, palpitations, flushing of the face, stomach ache, nausea, diarrhea, muscle pain, visual disturbances, and other (open question)).
- (1)
- PK and PD (maximum plasma concentration (Cmax), minimum plasma concentration (Cmin), average plasma concentration (Cavg), mean steady-state area under the curve (AUC0-24), Tmax, Tmin).
- (2)
- The pharmacodynamic parameters: Pain intensity (PI), pain intensity difference (PID), pain relief, patient and investigator global evaluation.
- (3)
- Pain registration on a NRS 0–10
- (4)
- At the same time as the pain assessment, general questions are answered on a NRS of 0–10.
2.7. Statistics
2.8. Sample Size
2.9. Ethical Considerations and Safety
2.10. Publication
3. Trial Status
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.L.H.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T.; et al. Neuropathic pain: An updated grading system for research and clinical practice. Pain 2016, 157, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Foley, P.L.; Vesterinen, H.M.; Laird, B.J.; Sena, E.S.; Colvin, L.A.; Chandran, S.; Macleod, M.R.; Fallon, M.T. Prevalence and natural history of pain in adults with multiple sclerosis: Systematic review and meta-analysis. Pain 2013, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, K.B.; Jensen, T.S.; Hansen, H.J.; Bach, F.W. Sensory function and quality of life in patients with multiple sclerosis and pain. Pain 2005, 114, 473–481. [Google Scholar] [CrossRef]
- Berger, T. Multiple sclerosis spasticity daily management: Retrospective data from Europe. Expert Rev. Neurother. 2013, 13 (Suppl. 1), 3–7. [Google Scholar] [CrossRef]
- Biering-Sørensen, F.; Biering-Sørensen, M. Sleep disturbances in the spinal cord injured: An epidemiological questionnaire investigation, including a normal population. Spinal Cord 2001, 39, 505–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, D.; Fullen, B.M.; Stokes, D.; Lennon, O. Neuropathic pain prevalence following spinal cord injury: A systematic review and meta-analysis. Eur. J. Pain 2017, 21, 29–44. [Google Scholar] [CrossRef] [Green Version]
- Andresen, S.R.; Hagen, E.M.; Biering-Sørensen, F.; Bach, F.W.; Finnerup, N.B.; Nielsen, J.F. Pain, spasticity and quality of life in individuals with traumatic spinal cord injury in Denmark. Spinal Cord 2016, 54, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Burns, A.S.; Lanig, I.; Grabljevec, K.; New, P.W.; Bensmail, D.; Ertzgaard, P.; Nene, A.V. Optimizing the Management of Disabling Spasticity Following Spinal Cord Damage: The Ability Network—An International Initiative. Arch. Phys. Med. Rehabil. 2016, 97, 2222–2228. [Google Scholar] [CrossRef]
- Otero-Romero, S.; Sastre-Garriga, J.; Comi, G.; Hartung, H.P.; Soelberg Sørensen, P.; Thompson, A.J.; Vermersch, P.; Gold, R.; Montalban, X. Pharmacological management of spasticity in multiple sclerosis: Systematic review and consensus paper. Mult. Scler. 2016, 22, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Pertwee, R.G. (Ed.) Handbook of Cannabis; Oxford University Press: Oxford, UK, 2014; ISBN 9780199662685. [Google Scholar]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for medical use: A systematic review and meta-analysis. JAMA-J. Am. Med. Assoc. 2015, 313, 2456–2473. [Google Scholar] [CrossRef]
- Torres-Moreno, M.C.; Papaseit, E.; Torrens, M.; Farré, M. Assessment of Efficacy and Tolerability of Medicinal Cannabinoids in Patients with Multiple Sclerosis. JAMA Netw. Open 2018, 1, e183485. [Google Scholar] [CrossRef] [Green Version]
- Koppel, B.S.; Brust, J.C.M.; Fife, T.; Bronstein, J.; Youssof, S.; Gronseth, G.; Gloss, D. Systematic Review: Efficacy and Safety of Medical Marijuana in Selected Neurologic Disorders. Neurology 2014, 82, 1556–1563. [Google Scholar] [CrossRef]
- Andresen, S.R.; Biering-Sørensen, F.; Hagen, E.M.; Nielsen, J.F.; Bach, F.W.; Finnerup, N.B. Cannabis use in persons with traumatic spinal cord injury in Denmark. J. Rehabil. Med. 2017, 49, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Scleroseforeningen. Cannabis Som Medicin Blandt Mennesker Med Sclerose—Holdninger, Erfaringer og Barrierer; Scleroseforeningen: Aarhus, Denmark, 2019. [Google Scholar]
- Gustavsen, S.; Søndergaard, H.B.; Andresen, S.R.; Magyari, M.; Sørensen, P.S.; Sellebjerg, F.; Oturai, A.B. Illegal cannabis use is common among Danes with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 33, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Banwell, E.; Pavisian, B.; Lee, L.; Anthony, F. Attitudes to cannabis and patterns of use among Canadians with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 10, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.J.; Ware, M.A.; Yazer, E.; Murray, T.J.; Lynch, M.E. Patterns of cannabis use among patients with multiple sclerosis. Neurology 2012, 62, 2098–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, P.; Hurst, D.P.; Reggio, R.H. Molecular Targes of the Phytocannabinoids—A Complex Picture. Prog. Chem. Org. Nat. Prod. 2017, 103, 103–131. [Google Scholar] [CrossRef] [Green Version]
- Mackie, K. Cannabinoid receptors: Where they are and what they do. J. Neuroendocrinol. 2008, 20, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Lafaye, G.; Karila, L.; Blecha, L.; Benyamina, A. Cannabis, cannabinoids and health. Dialogues Clin. Neurosci. 2017, 19, 309–317. [Google Scholar]
- Iversen, L. Cannabis and the brain. Brain 2003, 126, 1252–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, D.; French, J.A.; Maccarrone, M. Safety, efficacy, and mechanisms of action of cannabinoids in neurological disorders. Lancet Neurol. 2019, 18, 504–512. [Google Scholar] [CrossRef]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 16, 1344–1354. [Google Scholar] [CrossRef] [PubMed]
- Pertwee, R.G. The diverse CB 1 and CB 2 receptor pharmacology of three plant cannabinoids: Δ 9-tetrahydrocannabinol, cannabidiol and Δ 9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, É.; Vlachou, S. A Critical Review of the Role of the Cannabinoid Compounds Δ9-Tetrahydrocannabinol (Δ9-THC) and Cannabidiol (CBD) and their Combination in Multiple Sclerosis Treatment. Molecules 2020, 25, 4930. [Google Scholar] [CrossRef]
- Bonn-Miller, M.O.; El Sohly, M.A.; Loflin, M.J.E.; Chandra, S.; Vandrey, R. Cannabis and cannabinoid drug development: Evaluating botanical versus single molecule approaches. Int. Rev. Psychiatry 2018, 30, 277–284. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [Green Version]
- Zajicek, J.; Fox, P.; Sanders, H.; Wright, D.; Vickery, J.; Nunn, A.; Thompson, A. Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): Multicentre randomised placebo-controlled trial. Lancet 2003, 362, 1517–1526. [Google Scholar] [CrossRef]
- Zajicek, J.P.; Hobart, J.C.; Slade, A.; Barnes, D.; Mattison, P.G. MUltiple Sclerosis and Extract of Cannabis: Results of the MUSEC trial. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1125–1132. [Google Scholar] [CrossRef] [Green Version]
- Corey-Bloom, J.; Wolfson, T.; Gamst, A.; Jin, S.; Marcotte, T.D.; Bentley, H.; Gouaux, B. Smoked cannabis for spasticity in multiple sclerosis: A randomized, placebo-controlled trial. CMAJ 2012, 184, 1143–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, D.T.; Collin, C.; Stott, C.; Duncombe, P. Meta-analysis of the efficacy and safety of Sativex (nabiximols), on spasticity in people with multiple sclerosis. Mult. Scler. 2010, 16, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Novotna; Mares, J.; Ratcliffe, S.; Novakova, I.; Vachova, M.; Gasperini, C.; Pozzilli, C.; Rossii, P.; Ambler, Z.; Stelmasiak, Z.; et al. A Randomized double-blind placebo-controlled, parallel-group enriched-design study of nabiximol (Sativex), as add-on therapy, in subject with refractory spasticity caused by multiple sclerosis. Eur. J. Neurol. 2011, 18. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Davies, P.; Mutiboko, I.K.; Ratcliffe, S. Randomized controlled trial of cannabis-based medicine in spasticity caused by multiple sclerosis. Eur. J. Neurol. 2007, 14, 290–296. [Google Scholar] [CrossRef]
- De Blasiis, P.; Siani, M.F.; Fullin, A.; Sansone, M.; Melone, M.A.B.; Sampaolo, S.; Signoriello, E.; Lus, G. Short and long term effects of Nabiximols on balance and walking assessed by 3D-gait analysis in people with Multiple Sclerosis and spasticity. Mult. Scler. Relat. Disord. 2021, 51, 102805. [Google Scholar] [CrossRef]
- Danish Health and Medicines Authority; Sativex Produktresumé. In Produktresumé for Sativex Mundhulespray. Available online: http://media.medicininstruktioner.se/Assets/Document/577/Sativex_pligttekst.pdf (accessed on 8 September 2021).
- Hagenbach, U.; Luz, S.; Ghafoor, N.; Berger, J.M.; Grotenhermen, F.; Brenneisen, R.; Mäder, M. The treatment of spasticity with Δ9-tetrahydrocannabinol in persons with spinal cord injury. Spinal Cord 2007, 45, 551–562. [Google Scholar] [CrossRef]
- Pooyania, S.; Ethans, K.; Szturm, T.; Casey, A.; Perry, D. A Randomized, Double-Blinded, Crossover Pilot Study Assessing the Effect of Nabilone on Spasticity in Persons with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2010, 91, 703–707. [Google Scholar] [CrossRef]
- Rog, D.J.; Nurmikko, T.J.; Friede, T.; Young, C.A. Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology 2005, 65, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, K.B.; Jensen, T.S.; Bach, F.W. Does the cannabinoid dronabinol reduce central pain in multiple sclerosis? Randomised double blind placebo controlled crossover trial. BMJ 2004, 329, 253. [Google Scholar] [CrossRef] [Green Version]
- Schimrigk, S.; Marziniak, M.; Neubauer, C.; Kugler, E.M.; Werner, G.; Abramov-Sommariva, D. Dronabinol Is a Safe Long-Term Treatment Option for Neuropathic Pain Patients. Eur. Neurol. 2017, 78, 320–329. [Google Scholar] [CrossRef]
- Allan, G.M.; Finley, C.R.; Ton, J.; Perry, D.; Ramji, J.; Crawford, K.; Lindblad, A.J.; Korownyk, C.; Kolber, M.R. Systematic review of systematic reviews for medical cannabinoids. Can. Fam. Physician 2018, 64, e78–e94. [Google Scholar]
- Nielsen, S.; Germanos, R.; Weier, M.; Pollard, J.; Degenhardt, L.; Hall, W.; Buckley, N.; Farrell, M. The Use of Cannabis and Cannabinoids in Treating Symptoms of Multiple Sclerosis: A Systematic Review of Reviews. Curr. Neurol. Neurosci. Rep. 2018, 18, 8. [Google Scholar] [CrossRef]
- Fisher, E.; Moore, R.A.; Fogarty, A.E.; Finn, D.P.; Finnerup, N.B.; Gilron, I. Cannabinoids, cannabis, and cannabis-based medicine for pain management: A systematic review of randomised controlled trials. Pain 2021, 126, S45–S66. [Google Scholar] [CrossRef]
- IASP Presidential Task Force on Cannabis and Cannabinoid Analgesia. IASP International Association for the Study of Pain presidential task force on cannabis and cannabinoid analgesia position statement. Pain 2021, 162 (Suppl. 1), S1–S2. [Google Scholar] [CrossRef]
- Nugent, S.M.; Morasco, B.J.; O’Neil, M.E.; Freeman, M.; Low, A.; Kondo, K.; Elven, C.; Zakher, B.; Motu’apuaka, M.; Paynter, R.; et al. The effects of cannabis among adults with chronic painandan overview of general harms a systematic review. Ann. Intern. Med. 2017, 167, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Romero, K.; Pavisian, B.; Staines, W.R.; Feinstein, A. Multiple sclerosis, cannabis, and cognition: A structural MRI study. NeuroImage Clin. 2015, 8, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurmikko, T.J.; Serpell, M.G.; Hoggart, B.; Toomey, P.J.; Morlion, B.J.; Haines, D. Sativex successfully treats neuropathic pain characterised by allodynia: A randomised, double-blind, placebo-controlled clinical trial. Pain 2007, 133, 210–220. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies with Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, L.K.; Hasselstrøm, J.B. Sensitive determination of cannabinoids in whole blood by LC-MS-MS after rapid removal of phospholipids by filtration. J. Anal. Toxicol. 2017, 41, 382–391. [Google Scholar] [CrossRef]
- MacCallum, C.A.; Russo, E.B. Practical considerations in medical cannabis administration and dosing. Eur. J. Intern. Med. 2018, 49, 12–19. [Google Scholar] [CrossRef]
- Sørensen, J.; Gudex, C.; Davidsen, M.; Brønnum-Hansen, H.; Pedersen, K.M. Danish EQ-5D population norms. Scand. J. Public Health 2009, 37, 467–474. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef]
- Gregson, J.M.; Leathley, M.; Moore, A.P.; Sharma, A.K.; Smith, T.L.; Watkins, C.L. Reliability of the Tone Assessment Scale and the Modified Ashworth Scale as Clinical Tools for Assessing Poststroke Spasticity. Arch. Phys. Med. Rehabil. 1999, 80, 1013–1016. [Google Scholar] [CrossRef]
- Narayanaswami, P. The Spectrum of Functional Rating Scales in Neurology Clinical Trials. Neurotherapeutics 2017, 14, 161–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tombaugh, T.N. A comprehensive review of the Paced Auditory Serial Addition Test (PASAT). Arch. Clin. Neuropsychol. 2006, 21, 53–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleynhens, K.; D’hooghe, M.B.; D’hooge, M.; De Keyser, J.; Nagels, G.; Haelewyck, M.C.; Van Schependom, J. The Symbol Digit Modalities Test as sentinel test for cognitive impairment in multiple sclerosis. Eur. J. Neurol. 2014, 21, 1219–1225. [Google Scholar] [CrossRef]
- Goodkin, D.E.; Hertsgaard, D.; Seminary, J. Upper extremity Function in Multiple Sclerosis: Improving Assessment Sensitivity with Box -and-Block and Nine-Hole Peg Test. Arch. Phys. Med. Rehabil. 1988, 69, 59. [Google Scholar]
- Marrie, R.A.; Zhang, L.; Lix, L.M.; Graff, L.A.; Walker, J.R.; Fisk, J.D.; Patten, S.B.; Hitchon, C.A.; Bolton, J.M.; Sareen, J.; et al. The validity and reliability of screening measures for depression and anxiety disorders in multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 20, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Attal, N.; Bouhassira, D.; Baron, R.; Dostrovsky, J.; Dworkin, R.H.; Finnerup, N.; Gourlay, G.; Haanpaa, M.; Raja, S.; Rice, A.S.C.; et al. Assessing symptom profiles in neuropathic pain clinical trials: Can it improve outcome? Eur. J. Pain 2011, 15, 441–443. [Google Scholar] [CrossRef]
- Biering-Sørensen, B.; Finnderup, N.B.; Kasch, H.; Højsted, J.; Rotbøll, P.; Tollund, C.; Enggaard, T.; Handberg, G. National Behandlingsvejledning for Neuropatiske Smerter–Farmakologisk Behandling af Voksne. Available online: https://neuro.dk/wordpress/wp-content/uploads/2013/10/National-behandlingsvejledning-neuropatiske-smerter_version29.12.17.pdf (accessed on 8 September 2021).


{kind=link}
| Inclusion Criteria | |
|---|---|
| 1 | Definite or probable NP [1] for more than 3 months with mean pain intensity in baseline NRS > 3 and NRS ≤ 9 and/or presence of spasticity of more than 3 months with an intensity of >3 (NRS) |
| 2 | Stable disease (for pwMS; no relapse within the past month and no change in disease-modifying treatment during the previous three months). |
| 3 | Age ≥ 18 years |
| 4 | Informed consent is available. |
| Exclusion Criteria | |
| 1 | Competitive pain diseases (such as diabetic neuropathy) that cannot be distinguished from the patient’s pain due to SCI or MS |
| 2 | Opioid treatment that cannot be discontinued |
| 3 | Previous psychiatric disease in patient or nearest biological family, except well-treated depression |
| 4 | Previous risk of suicide assessed by the Columbia Suicide Severity Rating Scale [50] |
| 5 | Pregnancy and breast-feeding |
| 6 | Liver or renal insufficiency |
| 7 | Cardiovascular disease (except well-treated hypertension) |
| 8 | Previous convulsions/epilepsy |
| 9 | Active cancer disease |
| 10 | Previous or current addiction to alcohol/medication/drugs or positive urine screening |
| 11 | Current recreational cannabis use, or use within three months |
| 12 | Medical cannabis prescribed within 3 months |
| 13 | Allergy to cannabis products |
| 14 | Scheduled surgery during the study |
| 15 | Planned travels abroad during the study |
| Inclusion | Baseline | Randomization | Titration | Stable Phase (Maximum Dose) | Phase Out | Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Week | −4–0 | 0 | Week 1 Day 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 11 | ||
| VISIT | 1 | 2 | 3 | 4 | 5 | ||||||||
| Medical Examination | x | x | x | ||||||||||
| Medical history | x | ||||||||||||
| Neurological exam. | x | x | |||||||||||
| EDSS/ISNCSCI | x | ||||||||||||
| Heart and lung stethoscopy | x | ||||||||||||
| MAS | x | x | |||||||||||
| Clinical tests | |||||||||||||
| 9-hole peg test | x | x | |||||||||||
| PASAT | x | x | |||||||||||
| NPSI | x | x | |||||||||||
| SDMT | x | x | |||||||||||
| Trail making test | x | x | |||||||||||
| EQ5D5L | x | x | |||||||||||
| PGIC | x | ||||||||||||
| Others | x | x | x | ||||||||||
| Pregnancy test | x | x | |||||||||||
| Biochemistry * | x | x | x | ||||||||||
| U-stix (Drug/THC) | x | ||||||||||||
| Electrocardiogram | x | x | x | ||||||||||
| Blood pressure | x | x | x | x | |||||||||
| Expectation of relief | x | ||||||||||||
| Blinding ** | x | x | |||||||||||
| Dispensing of medicine | x | x | |||||||||||
| Returning packaging | x | x | x | ||||||||||
| Counting of capsules | x | x | x | ||||||||||
| Admission *** | x | ||||||||||||
| Telephone | x | x | x | x | |||||||||
| eDiary | x | x | x | x | x | x | x | x | |||||
| Pain (NRS) | x | x | x | x | x | x | x | ||||||
| Spasticity (NRS) | x | x | x | x | x | x | x | ||||||
| Relief pain (NRS) | x | x | |||||||||||
| Relief spasticity NRS | x | x | |||||||||||
| Sleep (NRS) | x | x | x | x | x | x | x | ||||||
| PROMIS sleep | x | x | x | ||||||||||
| PROMIS anxiety/depression | x | x | x | ||||||||||
| Influence of pain/spasticity (NRS) -activity, mood and sleep | x | x | x | ||||||||||
| Escape medicine | x | x | x | x | x | x | x | x | |||||
| Side effects/AE | x | x | x | x | x | x | x | x | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, J.S.; Hansen, R.M.; Petersen, T.; Gustavsen, S.; Oturai, A.B.; Sellebjerg, F.; Sædder, E.A.; Kasch, H.; Rasmussen, P.V.; Finnerup, N.B.; et al. The Effect of Cannabis-Based Medicine on Neuropathic Pain and Spasticity in Patients with Multiple Sclerosis and Spinal Cord Injury: Study Protocol of a National Multicenter Double-Blinded, Placebo-Controlled Trial. Brain Sci. 2021, 11, 1212. https://doi.org/10.3390/brainsci11091212
Hansen JS, Hansen RM, Petersen T, Gustavsen S, Oturai AB, Sellebjerg F, Sædder EA, Kasch H, Rasmussen PV, Finnerup NB, et al. The Effect of Cannabis-Based Medicine on Neuropathic Pain and Spasticity in Patients with Multiple Sclerosis and Spinal Cord Injury: Study Protocol of a National Multicenter Double-Blinded, Placebo-Controlled Trial. Brain Sciences. 2021; 11(9):1212. https://doi.org/10.3390/brainsci11091212
Chicago/Turabian StyleHansen, Julie Schjødtz, Rikke Middelhede Hansen, Thor Petersen, Stefan Gustavsen, Annette Bang Oturai, Finn Sellebjerg, Eva Aggerholm Sædder, Helge Kasch, Peter Vestergaard Rasmussen, Nanna Brix Finnerup, and et al. 2021. "The Effect of Cannabis-Based Medicine on Neuropathic Pain and Spasticity in Patients with Multiple Sclerosis and Spinal Cord Injury: Study Protocol of a National Multicenter Double-Blinded, Placebo-Controlled Trial" Brain Sciences 11, no. 9: 1212. https://doi.org/10.3390/brainsci11091212
APA StyleHansen, J. S., Hansen, R. M., Petersen, T., Gustavsen, S., Oturai, A. B., Sellebjerg, F., Sædder, E. A., Kasch, H., Rasmussen, P. V., Finnerup, N. B., & Svendsen, K. B. (2021). The Effect of Cannabis-Based Medicine on Neuropathic Pain and Spasticity in Patients with Multiple Sclerosis and Spinal Cord Injury: Study Protocol of a National Multicenter Double-Blinded, Placebo-Controlled Trial. Brain Sciences, 11(9), 1212. https://doi.org/10.3390/brainsci11091212