
Obesity and Gray Matter Volume Assessed by Neuroimaging: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Strategies
2.2. Eligibility Criteria
2.3. Obesity Measurements
2.4. Neuroimaging Technique and Analysis
3. Results
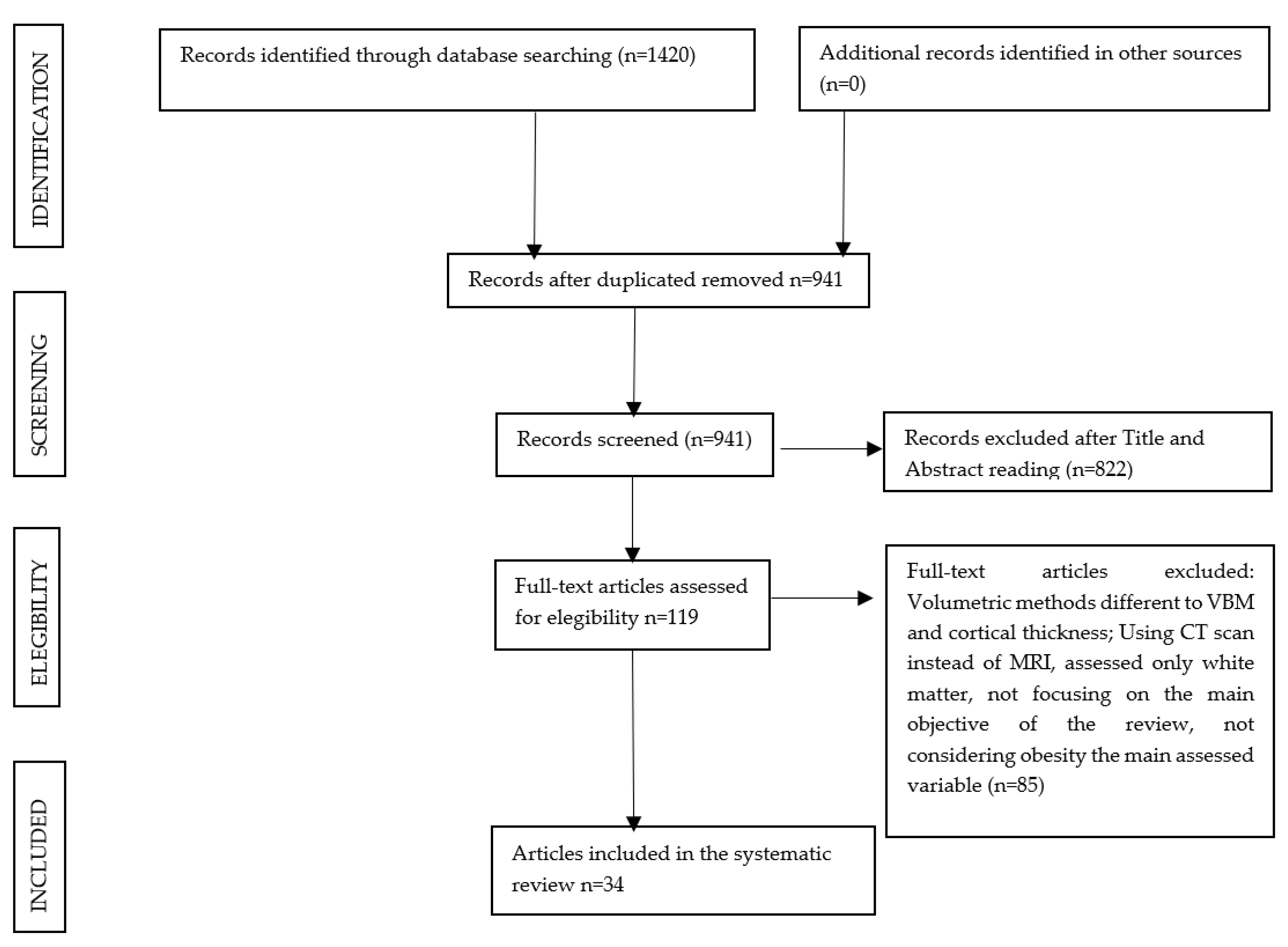
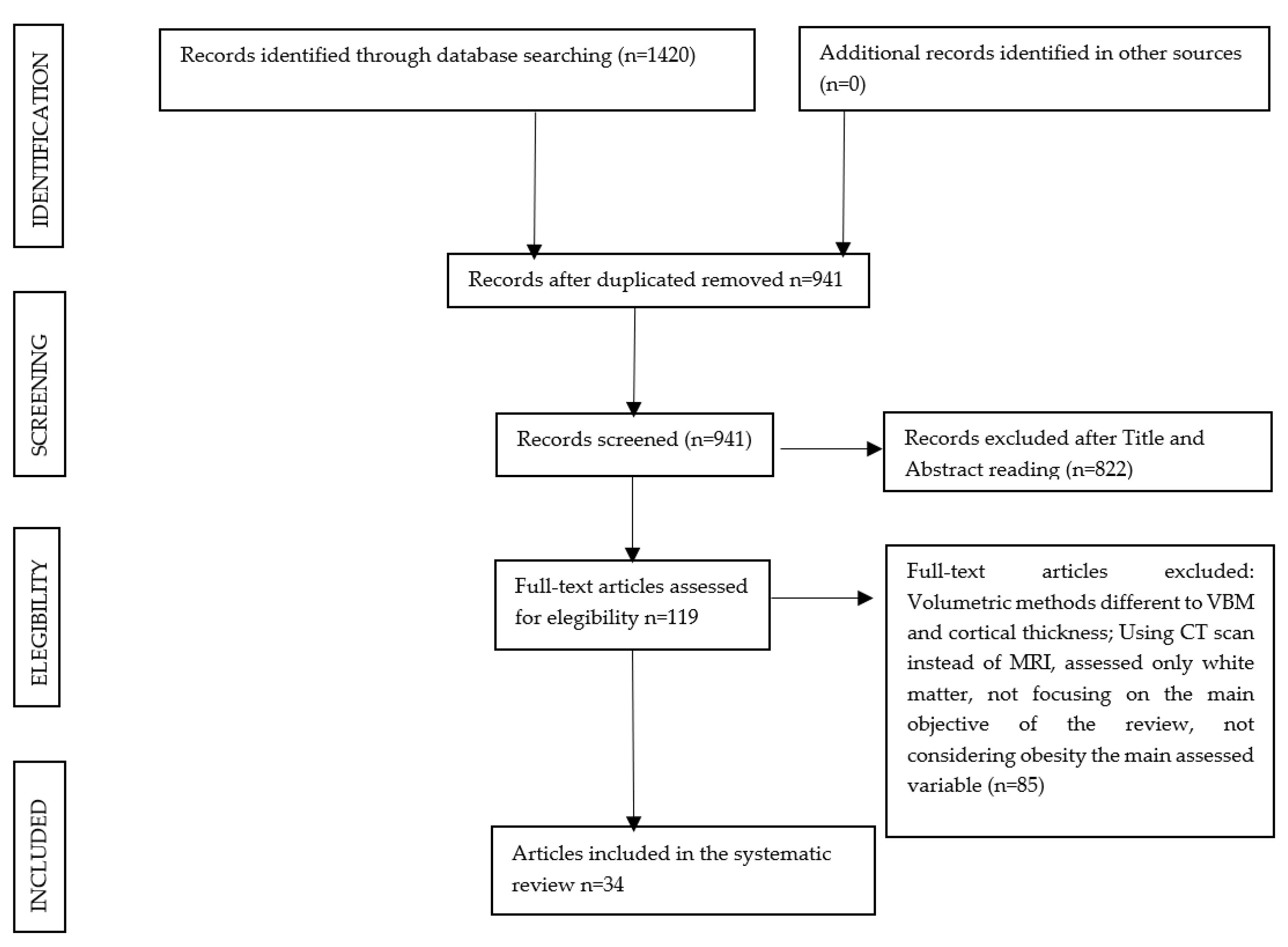
3.1. Study Selection
3.2. Study Characteristics
3.3. VBM Studies
3.3.1. Cross-Sectional Design
3.3.2. Prospective Longitudinal Design
3.3.3. Prospective Longitudinal Cross-Sectional Design
3.4. CT Studies
Cross-Sectional Design
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Media Centre: Obesity and Overweight [Aprox. 4 p.]; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Obesity and Overweight 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 February 2021).
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected US state-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef]
- Ogden, C.L.; Yanovski, S.Z.; Carroll, M.D.; Flegal, K.M. The epidemiology of obesity. Gastroenterology 2007, 132, 2087–2102. [Google Scholar] [CrossRef]
- Xian, H.; Vasilopoulos, T.; Liu, W.; Hauger, R.L.; Jacobson, K.C.; Lyons, M.J.; Panizzon, M.; Reynolds, C.A.; Vuoksimaa, E.; Kremen, W.S.; et al. Steeper change in body mass across four decades predicts poorer cardiometabolic outcomes at midlife. Obesity 2017, 25, 773–780. [Google Scholar] [CrossRef] [Green Version]
- Masouleh, S.K.; Arélin, K.; Horstmann, A.; Lampe, L.; Kipping, J.A.; Luck, T.; Riedel-Heller, S.G.; Schroeter, M.L.; Stumvoll, M.; Villringer, A.; et al. Body Mass Index in older adults is associated with lower GMV: Implications for memory performance. Neurobiol. Aging 2016, 40, 1–10. [Google Scholar] [CrossRef]
- Yau, P.L.; Kang, E.H.; Javier, D.C.; Convit, A. Preliminary evidence of cognitive and brain abnormalities in uncomplicated adolescent obesity. Appetite 2014, 93, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.J.; Benedict, C.; Burgos, J.; Kempton, M.J.; Kullberg, J.; Nordenskjöld, R.; Kilander, L.; Nylander, R.; Larsson, E.M.; Johansson, L.; et al. Late-life obesity is associated with smaller global and regional GMVs: A voxel-based morphometric study. Int. J. Obes. 2013, 37, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walther, K.; Birdsill, A.C.; Glisky, E.L.; Ryan, L. Structural brain differences and cognitive functioning related to body mass index in older females. Hum. Brain Mapp. 2010, 31, 1052–1064. [Google Scholar] [CrossRef] [PubMed]
- Whitmer, R.A.; Gunderson, E.P.; Barrett-Connor, E.; Quesenberry, C.P.; Yaffe, K. Obesity in middle age and future risk of dementia: A 27 year longitudinal population based study. BMJ 2005, 330, 1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafson, D.; Rothenberg, E.; Blennow, K.; Steen, B.; Skoog, I. An 18-year follow-up of overweight and risk of Alzheimer disease. Arch. Intern. Med. 2003, 163, 1524–1528. [Google Scholar] [CrossRef] [Green Version]
- Singh-Manoux, A.; Dugravot, A.; Shipley, M.; Brunner, E.J.; Elbaz, A.; Sabia, S.; Kivimaki, M. Obesity trajectories and risk of dementia: 28 years of follow-up in the Whitehall II Study. Alzheimers Dement. 2018, 14, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Fox, N.C.; Jack, C.R.; Scheltens, P.; Thompson, P.M. The clinical use of structural MRI in Alzheimer disease. Nat. Rev. Neurol. 2010, 6, 67–77. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.R.; McEvoy, L.K.; Gharapetian, L.; Fennema-Notestine, C.; Hagler, D.J.; Holland, D.; Koyama, A.; Brewer, J.B.; Dale, A.M. Regional rates of neocortical atrophy from normal aging to early Alzheimer disease. Neurology 2009, 73, 457–465. [Google Scholar] [CrossRef]
- Whitmer, R.A.; Sidney, S.; Selby, J.; Johnston, S.C.; Yaffe, K. Midlife cardiovascular risk factors and risk of dementia in late life. Neurology 2005, 64, 277–281. [Google Scholar] [CrossRef]
- Yaffe, K.; Kanaya, A.; Lindquist, K.; Simonsick, E.M.; Harris, T.; Shorr, R.I.; Tylavsky, F.A.; Newman, A.B. The metabolic syndrome, inflammation, and risk of cognitive decline. JAMA 2004, 292, 2237–2242. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, R.M.; Saxby, B.K.; Burton, E.J.; Barber, R.; Ford, G.A.; O’Brien, J.T. Hippocampal atrophy, whole brain volume, and white matter lesions in older hypertensive subjects. Neurology 2004, 63, 1892–1897. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Casares, N.; Berthier, M.L.; Jorge, R.E.; Gonzalez-Alegre, P.; Gutierrez Cardo, A.; Rioja Villodres, J.; Acion, L.; Ariza Corbo, M.J.; Nabrozidis, A.; Garcia-Arnes, J.A.; et al. Structural and functional brain changes in middle-aged type 2 diabetic patients: A cross-sectional study. J. Alzheimers Dis. 2014, 40, 375–386. [Google Scholar] [CrossRef] [Green Version]
- Whalley, L.J.; Staff, R.T.; Murray, A.D.; Duthie, S.J.; Collins, A.R.; Lemmon, H.A.; Starr, J.M.; Deary, I.J. Plasma vitamin C, cholesterol and homocysteine are associated with GMV determined by MRI in non-demented old people. Neurosci. Lett. 2003, 341, 173–176. [Google Scholar] [CrossRef]
- Song, S.W.; Chung, J.H.; Rho, J.S.; Lee, Y.A.; Lim, H.K.; Kang, S.G.; Kim, H.N.; Kim, J.E.; Kim, S.H. Regional CT and subcortical volume changes in patients with metabolic syndrome. Brain Imaging Behav. 2015, 9, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Franz, C.E.; Xian, H.; Lew, D.; Hatton, S.N.; Puckett, O.; Whitsel, N.; Kremen, W.S. Body mass trajectories and CT in middle-aged men: A 42-year longitudinal study starting in young adulthood. Neurobiol. Aging 2019, 79, 11–21. [Google Scholar] [CrossRef]
- Pannacciulli, N.; Del Parigi, A.; Chen, K.; Le, D.S.; Reiman, E.M.; Tataranni, P.A. Brain abnormalities in human obesity: A voxel-based morphometric study. Neuroimage 2006, 31, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms linking obesity with cardiovascular disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef]
- Guillemot-Legris, O.; Muccioli, G.G. Obesity-induced neuroinflammation: Beyond the hypothalamus. Trends Neurosci. 2017, 40, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Bobb, J.F.; Schwartz, B.S.; Davatzikos, C.; Caffo, B. Cross-sectional and longitudinal association of body mass index and brain volume. Hum. Brain Mapp. 2014, 35, 75–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houben, K.; Nederkoorn, C.; Jansen, A. Eating on impulse: The relation between overweight and food-specific inhibitory control. Obesity 2014, 22, E6–E8. [Google Scholar] [CrossRef] [Green Version]
- Batterink, L.; Yokum, S.; Stice, E. Body mass correlates inversely with inhibitory control in response to food among adolescent girls: An fMRI study. Neuroimage 2010, 52, 1696–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasinska, A.J.; Yasuda, M.; Burant, C.F.; Gregor, N.; Khatri, S.; Sweet, M.; Falk, E.B. Impulsivity and inhibitory control deficits are associated with unhealthy eating in young adults. Appetite 2012, 59, 738–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokum, S.; Ng, J.; Stice, E. Relation of regional gray and white matter volumes to current BMI and future increases in BMI: A prospective MRI study. Int. J. Obes. 2012, 36, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Volkow, N.D.; Wang, G.J.; Tomasi, D.; Baler, R.D. Obesity and addiction: Neurobiological overlaps. Obes. Rev. 2013, 14, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.J.; Volkow, N.D.; Thanos, P.K.; Fowler, J.S. Similarity between obesity and drug addiction as assessed by neurofunctional imaging: A concept review. J. Addict. Dis. 2004, 23, 39–53. [Google Scholar] [CrossRef]
- Stice, E.; Burger, K. Neural vulnerability factors for obesity. Clin. Psychol. Rev. 2019, 68, 38–53. [Google Scholar] [CrossRef]
- Herrmann, M.J.; Tesar, A.K.; Beier, J.; Berg, M.; Warrings, B. Grey matter alterations in obesity: A meta-analysis of whole-brain studies. Obes. Rev. 2019, 20, 464–471. [Google Scholar] [CrossRef]
- García-García, I.; Michaud, A.; Dadar, M.; Zeighami, Y.; Neseliler, S.; Collins, D.L.; Evans, A.C.; Dagher, A. Neuroanatomical differences in obesity: Meta-analytic findings and their validation in an independent dataset. Int. J. Obes. 2019, 43, 943–951. [Google Scholar] [CrossRef]
- Favieri, F.; Forte, G.; Casagrande, M. The executive functions in overweight and obesity: A systematic review of neuropsychological cross-sectional and longitudinal studies. Front. Psychol. 2019, 10, 2126. [Google Scholar] [CrossRef]
- Takao, H.; Abe, O.; Ohtomo, K. Computational analysis of cerebral cortex. Neuroradiology 2010, 52, 691–698. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzla, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry—The methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.E.; Buchbinder, B.R.; Aharon, I. Three-dimensional mapping of CT using Laplace’s equation. Hum. Brain Mapp. 2000, 11, 12–32. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, D.; Kabani, N.; Avis, D.; Evans, A.C. Automated 3-D extraction of innerand outer surfaces of cerebral cortex from MRI. NeuroImage 2000, 12, 340–356. [Google Scholar] [CrossRef] [Green Version]
- Opel, N.; Redlich, R.; Kaehler, C.; Grotegerd, D.; Dohm, K.; Heindel, W.; Dannlowski, U. Prefrontal GMV mediates genetic risks for obesity. Mol. Psychiatry 2017, 22, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Medic, N.; Ziauddeen, H.; Ersche, K.D.; Farooqi, I.S.; Bullmore, E.T.; Nathan, P.J.; Ronan, L.; Fletcher, P.C. Increased body mass index is associated with specific regional alterations in brain structure. Int. J. Obes. 2016, 40, 1177–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veit, R.; Kullmann, S.; Heni, M.; Machann, J.; Häring, H.U.; Fritsche, A.; Preissl, H. Reduced CT associated with visceral fat and BMI. Neuroimage Clin. 2014, 6, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, B.; Chen, M.; Luo, X.; Dai, Y. Reduced right frontal fractional anisotropy correlated with early elevated plasma LDL levels in obese young adults. PLoS ONE 2014, 9, e108180. [Google Scholar] [CrossRef]
- Marqués-Iturria, I.; Pueyo, R.; Garolera, M.; Segura, B.; Junqué, C.; García-García, I.; Sender-Palacios, M.J.; Vernet-Vernet, M.; Narberhaus, A.; Ariza, M.; et al. Frontal cortical thinning and subcortical volume reductions in early adulthood obesity. Psychiatry Res. 2013, 214, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Kurth, F.; Levitt, J.G.; Phillips, O.R.; Luders, E.; Woods, R.P.; Mazziotta, J.C.; Toga, A.W.; Narr, K.L. Relationships between gray matter, body mass index, and waist circumference in healthy adults. Hum. Brain Mapp. 2013, 34, 1737–1746. [Google Scholar] [CrossRef]
- Weise, C.M.; Thiyyagura, P.; Reiman, E.M.; Chen, K.; Krakoff, J. Fat-free body mass but not fat mass is associated with reduced GMV of cortical brain regions implicated in autonomic and homeostatic regulation. Neuroimage 2013, 64, 712–721. [Google Scholar] [CrossRef] [Green Version]
- Pannacciulli, N.; Le, D.S.; Chen, K.; Reiman, E.M.; Krakoff, J. Relationships between plasma leptin concentrations and human brain structure: A voxel-based morphometric study. Neurosci. Lett. 2007, 412, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Westwater, M.L.; Vilar-López, R.; Ziauddeen, H.; Verdejo-García, A.; Fletcher, P.C. Combined effects of age and BMI are related to altered CT in adolescence and adulthood. Dev. Cogn. Neurosci. 2019, 40, 100728. [Google Scholar] [CrossRef]
- Janowitz, D.; Wittfeld, K.; Terock, J.; Freyberger, H.J.; Hegenscheid, K.; Völzke, H.; Habes, M.; Hosten, N.; Friedrich, N.; Nauck, M.; et al. Association between waist circumference and GMV in 2344 individuals from two adult community-based samples. Neuroimage 2015, 122, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Saute, R.L.; Soder, R.B.; Alves Filho, J.O.; Baldisserotto, M.; Franco, A.R. Increased brain CT associated with visceral fat in adolescents. Pediatric Obes. 2018, 13, 74–77. [Google Scholar] [CrossRef] [PubMed]
- De Groot, C.J.; van den Akker, E.L.; Rings, E.H.; Delemarre-van de Waal, H.A.; van der Grond, J. Brain structure, executive function and appetitive traits in adolescent obesity. Pediatric Obes. 2017, 12, e33–e36. [Google Scholar] [CrossRef] [PubMed]
- Hayakawa, Y.K.; Sasaki, H.; Takao, H.; Yoshikawa, T.; Hayashi, N.; Mori, H.; Ohtomo, K. The relationship of waist circumference and body mass index to grey matter volume in community dwelling adults with mild obesity. Obes. Sci. Pract. 2018, 4, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Tian, X.; Tian, D.; Wang, J.; Wang, Q.; Yu, C.; Wang, J. Altered regional GMV in obese men: A structural MRI study. Front. Psychol. 2017, 8, 125. [Google Scholar] [PubMed] [Green Version]
- Wang, H.; Wen, B.; Cheng, J.; Li, H. Brain structural differences between normal and obese adults and their links with lack of perseverance, negative urgency, and sensation seeking. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ronan, L.; Alexander-Bloch, A.F.; Wagstyl, K.; Farooqi, S.; Brayne, C.; Tyler, L.K.; Fletcher, P.C. Obesity associated with increased brain age from midlife. Neurobiol. Aging 2016, 47, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Kim, C.; Jeon, S.; Kang, M.; Kim, Y.J.; Lee, J.M.; Shin, H.Y.; Cho, H.; Ye, B.S.; Kim, J.H.; et al. Association of Body Fat Percentage and Waist-hip Ratio with Brain CT: A Study Among 1777 Cognitively Normal Subjects. Alzheimer Dis. Assoc. Disord. 2015, 29, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Gonzales, M.M.; Strasser, B.; Pasha, E.; McNeely, J.; Tanaka, H.; Haley, A.P. Central Adiposity and CT in Midlife. Psychosom. Med. 2015, 77, 671–678. [Google Scholar] [CrossRef]
- Shott, M.E.; Cornier, M.A.; Mittal, V.A.; Pryor, T.L.; Orr, J.M.; Brown, M.S.; Frank, G.K. Orbitofrontal cortex volume and brain reward response in obesity. Int. J. Obes. 2015, 39, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kim, C.; Seo, S.W.; Na, D.L.; Kim, H.J.; Kang, M.; Shin, H.Y.; Cho, S.K.; eon Park, S.; Lee, J.; et al. Association between body mass index and CT: Among elderly cognitively normal men and women. Int. Psychogeriatr. 2015, 27, 121–130. [Google Scholar] [CrossRef]
- Debette, S.; Wolf, C.; Lambert, J.C.; Crivello, F.; Soumaré, A.; Zhu, Y.C.; Schilling, S.; Dufouil, C.; Mazoyer, B.; Amouyel, P.; et al. Abdominal obesity and lower GMV: A Mendelian randomization study. Neurobiol. Aging 2014, 35, 378–386. [Google Scholar] [CrossRef]
- Mueller, K.; Sacher, J.; Arelin, K.; Holiga, Š.; Kratzsch, J.; Villringer, A.; Schroeter, M.L. Overweight and obesity are associated with neuronal injury in the human cerebellum and hippocampus in young adults: A combined MRI, serum marker and gene expression study. Transl. Psychiatry 2012, 2, e200. [Google Scholar] [CrossRef]
- Smucny, J.; Cornier, M.A.; Eichman, L.C.; Thomas, E.A.; Bechtell, J.L.; Tregellas, J.R. Brain structure predicts risk for obesity. Appetite 2012, 59, 859–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassenstab, J.J.; Sweet, L.H.; Del Parigi, A.; McCaffery, J.M.; Haley, A.P.; Demos, K.E.; Cohen, R.A.; Wing, R.R. CT of the cognitive control network in obesity and successful weight loss maintenance: A preliminary MRI study. Psychiatry Res. 2012, 202, 77–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narita, K.; Kosaka, H.; Okazawa, H.; Murata, T.; Wada, Y. Relationship between plasma leptin level and brain structure in elderly: A voxel-based morphometric study. Biol. Psychiatry 2009, 65, 992–994. [Google Scholar] [CrossRef] [PubMed]
- Taki, Y.; Kinomura, S.; Sato, K.; Inoue, K.; Goto, R.; Okada, K.; Uchida, S.; Kawashima, R.; Fukuda, H. Relationship between body mass index and GMV in 1,428 healthy individuals. Obesity 2008, 16, 119–124. [Google Scholar] [CrossRef]
- García-Casares, N.; Bernal-López, M.R.; Roé-Vellvé, N.; Gutiérrez-Bedmar, M.; Fernández-García, J.C.; García-Arnés, J.A.; Gómez-Huelgas, R. Brain functional connectivity is modified by a hypocaloric Mediterranean diet and physical activity in obese women. Nutrients 2017, 9, 685. [Google Scholar] [CrossRef] [Green Version]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The brain’s default network: Anatomy, function, and relevance to disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Lips, M.A.; Wijngaarden, M.A.; van der Grond, J.; van Buchem, M.A.; de Groot, G.H.; Rombouts, S.A.; Pijl, H.; Veer, I.M. Resting-state functional connectivity of brain regions involved in cognitive control, motivation, and reward is enhanced in obese females. Am. J. Clin. Nutr. 2014, 100, 524–531. [Google Scholar] [CrossRef] [Green Version]
- García-García, I.; Morys, F.; Dagher, A. Nucleus accumbens volume is related to obesity measures in an age-dependent fashion. J. Neuroendocrinol. 2020, 32, e12812. [Google Scholar] [CrossRef] [Green Version]
- Voets, N.L.; Hough, M.G.; Douaud, G.; Matthews, P.M.; James, A.; Winmill, L.; Webster, P.; Smith, S. Evidence for abnormalities of cortical development in adolescent-onset schizophrenia. NeuroImage 2008, 43, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Blankstein, U.; Chen, J.Y.; Mincic, A.M.; McGrath, P.A.; Davis, K.D. The complex minds of teenagers: Neuroanatomy of personality differs between sexes. Neuropsychologia 2009, 47, 599–603. [Google Scholar] [CrossRef]
- Good, C.D.; Johnsrude, I.S.; Ashburner, J.; Henson, R.N.; Friston, K.J.; Frackowiak, R.S. A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage 2001, 14, 21–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Year and First Author | Study Design | Sample Size, Type of Groups | Total Sample Mean Age (Unless Indicated): M ± SD (Range) | Obesity Measurement | MRI Analysis Description | Neuropsychological Assessment | Results |
|---|---|---|---|---|---|---|---|
| 2019, Franz CE [21] | Prospective longitudinal | n = 373 Obese (O) vs. Control (C) (171 vs. 202) | O= 61.7 ± 2.65 C= 62.0 ± 2.48 The reported data are given by the 2 groups separately | BMI (4 time measures according to normal/O trajectories) 32.6 ± 3.00 vs. 25.9 ± 2.48 The reported data are given by the 2 groups separately | 1T MRI CT ROI analysis | No | Obesity trajectory had thinner cortex compared with the normal trajectory in the superior, inferior, middle temporal gyri, temporal pole, fusiform gyrus, superior temporal sulcus, frontal pole, pars triangularis, caudal and rostral middle frontal gyri. |
| 2019, Westwater ML [49] | Cross-sectional | Adolescents = 70 O vs. Overweight vs. Healthy weight adolescents (18 vs. 17 vs. 35) Adults = 75 O vs. Overweight vs. Healthy weight adults (20 vs. 21 vs. 34) | Adolescents = Women (W): 35, 16.7 ± 1.4; Men (M): 35, 16.4 ± 1.5 Adults = 42W, 32.8 ± 6.3; 33M, 33.9 ± 6.4 The reported data are given by groups and genders separately (W/M). | BMI: Adolescents: 32.3 ± 2.4 vs. 26.7 ± 1.4 vs. 21.2 ± 2.1 Adults: 33.5 ± 2.6 vs. 27.6 ± 1.6 vs. 22.1 ±1.7 Body Fat (%) Adolescents: 31.5 ± 9.4 vs. 23.4 ± 10.2 vs. 16.1 ± 7.8 Adults: 34.6 ± 8.8 vs. 29.3 ±7.7 vs. 20.4 ± 6.1 The reported data are given by groups and genders separately (W/M) | 3T MRI CT ROI analysis | Impulsivity (delay discounting (DD)): monetary choice questionnaire | In adolescents, increasing age-adjusted BMI Z-score attenuated age-related CT reductions globally and in frontal, temporal and occipital regions. In adults, an increase in BMI increased age-related CT reductions both globally and in bilateral parietal cortex. Increased DD and adiposity were associated with a reduction in IFG thickness in adolescents and adults. |
| 2018, Saute RL [51] | Cross-sectional | n = 44 O vs. Lean (L) (18 vs. 26) | O: 16.22 ± 0.73 L: 16.81 ± 0.71 The reported data are given by the 2 groups separately | BMI: 31.11 ± 3.21 vs. 21.38 ± 1.70 VFR: 14.62 ± 7.15 vs. 5.10 ± 1.70 HRG: 14.44 ± 8.44 vs. 10.48 ± 7.72 The reported data are given by the 2 groups separately | 3T MRI CT whole-brain analysis | No | No relationship between BMI or HRG with brain cortical dimensions. Significant positive correlation between VFR and cortical areas in left paracentral, lateral occipital and right precentral, postcentral and superior temporal, among others. CT reductions were not different between groups, neither were they associated with BMI or HRG. |
| 2017, de Groot CJ [52] | Cross-sectional | n = 44 O vs. L (23 vs. 19) | Total sample age range: (12–16) | BMI: Significantly higher BMI in the obesity group (−0.08 vs. 3.54 standard deviation values) | 3T MRICT ROI analysis | Executive function: stop signal task and Choice Delay Task | O group had greater significant volumes of the pallidum when compared with C. A greater pallidum volume in O group was positively significant, associated with delay reward in the Choice Delay Task. |
| 2017, Opel N [41] | Cross-sectional | Healthy groups from two different studies: n = 330 (Münster Neuroimaging Cohort) and n = 347 (BiDirect study) | Münster Cohort = 39.2 ± 11.3 (20–59) BiDirectstudy = 51.6 ± 8.2 (35.3–65.6) The reported data are given by the 2 groups separately | BMI: 24.5 ± 3.9 vs. 26.3 ± 4.1 The reported data are given by the 2 groups separately | 3T MRI VBM whole-brain analysis | No | Higher BMI and PR for obesity (single-nucleotide polymorphisms (SNPs) selected from the genome-wide association study (GWAS)) were significantly associated with decreased medial prefrontal gray matter, and it was further demonstrated that prefrontal gray matter significantly mediated the effect of PR for O on the BMI in both samples. |
| 2017, Hayakawa YK [53] | Cross-sectional | n = 792 healthy sample (M = 523, W = 269) | M: 55.3 ± 9.7 (23–84) W: 55.2 ± 9.9 (24–81) The reported data are given by gender groups separately (W/M) | BMI 24.7 ± 3.1 vs. 22 ± 3.3 WC 88.5 ± 8.1 vs. 81.2 ± 9.8 The reported data is given by gender groups separately (W/M). | 3T MRI VBM whole-brain analysis | No | Negatively significant correlations were found between WC and BMI and gray matter volume. In W, the total area of the regions (left thalamus, precentral and inferior frontal gyrus) was significantly correlated with WC and was slightly larger than that of the regions significantly correlated with BMI. |
| 2017, Zhang B [54]4 | Cross-sectional | n = 40 O vs. L (20 vs. 20) Men adult sample | O: (20–28) L: (20–28) The reported data are given by the 2 groups separately | BMI: 33.56 ± 3.53 vs. 21.48 ± 1.43 The reported data is given by the 2 groups separately. | 3T MRI VBM whole-brain analysis | Hunger rating: visual analog scales | O group in comparison to C: increased GMV in the left putamen and it was positively correlated with BMI, plasma insulin and HOMA-IR. There was a negative correlation between OFC GMV and hunger score and no differences between groups. |
| 2017, Wang H [55] | Cross-sectional | n = 80 O vs. C (31 vs. 49) | O: 39.58 ± 1.93 vs. C: 29.55 ± 1.41 The reported data are given by the 2 groups separately | BMI: 34.38 ± 0.69 vs. 21.87 ± 0.29 The reported data is given by the 2 groups separately. | 3T MRI VBM ROI analysis | Impulsivity: UPPS-P Impulsive Behavior Scale, eating behavior: Three-Factor Eating Questionnaire and depression (Beck Depression Inventory-II) | O group in comparison to C: reduced GMV in the frontal and limbic regions. In the O group: sensation seeking was negatively correlated with GMV in the left amygdala and right pallidum. |
| 2016, Ronan L [56] | Cross-sectional | n = 473 O/Overweight vs. Normal weight (77/150 vs. 246) | 54 (20–87) | BMI: O: 33.5 ± 3.8 vs. Overweight: 27.1 ± 1.6 vs. Normal weight: 22.7 ± 1.7 | 3T MRI CT whole-brain analysis | Cognitive performance: Cattell Culture Fair | No relation between BMI with cortical area surface, regional CT and cognitive performance. Overweight and O groups in comparison to C: increased mean CT. |
| 2016, Medic N [42]4 | Cross-sectional | n = 202 O vs. Overweight vs. C Healthy sample 19 smokers | 32.3 ± 7.7 (18–50) | BMI: 28.5 ± 6.3 (18.5–46.4) | 3T MRI CT whole-brain analysis | No | BMI with global CT: not significant association. BMI with regional CT: negatively correlated within left LOC and right vmPFC. |
| 2016, Masouleh SK [6] | Cross-sectional | n = 617 No C group | 68.7 ± 4.6 (60–79) | BMI: 27.5 ± 4 (18.5–45.5) | 3T MRI VBM whole-brain analysis | Alzheimer diagnosis (CERAD plus): TMTA and B, semantic and phonemic verbal fluency and verbal memory | BMI with GMV: negatively correlated within the prefrontal, temporal, insular and occipital cortex, thalamus, putamen, amygdala and cerebellum. BMI memory performance: negatively associated within the prefrontal cortex, thalamus, orbitofrontal cortex and insula and paracingulate gyrus due to its effect in the GMV. BMIs with processing speed were negatively correlated after the adjustment for almost all confounders within the bilateral temporal and insula and intracalcarine cortex. |
| 2015, Kim HJ [57] | Cross-sectional | n = 1777 O vs. C (M = 312, W = 174) Gender-stratified analysis Reported data are for the groups and gender, separately (F/M) | M: 64.9 ± 7.0 (45–91) W: 62.6 ± 7.5 (45–85) Reported data are for the groups and genders separately (F/M) | Body fat % and WHR: M: 24.0 ± 5.4 and 0.937 ± 0.036, W: 32.0 ± 6.0 and 0.913 ± 0.057 Reported data is for the groups and gender, separately (F/M) | 3T MRI CT whole-brain analysis | Cognitive performance and dementia diagnosis: MMSE and MoCA | M: body fat % with CT: positively correlated in all brain lobes; WHR and CT: negatively correlated in total and in the frontal lobe. Low fat % and central obesity related to decreased CT in men but not to MMSE or MoCA. W: no relation between CT and body fat % or WHR. No relation between body fat % and WHR and the MMSE or MoCA. |
| 2015, Janowitz D [50] | Cross-sectional | Study of Health in Pomerania (SHIP-2) = 758 and SHIP-TREND = 1586 Healthy group from SHIP-2 and SHIP-TREND (n = 435) | SHIP-2: 49.8 ± 9.3 SHIP-TREND: 46.3 ± 11.3(20–79) The reported data are given by the 2 groups separately | WC and BMI: SHIP-2: 88.7 ± 12.8 and 27.4 ± 4.5 SHIP-TREND: 87.9 ± 12.6 and 27.2 ± 4.4 The reported data is given by the 2 groups separately | 1.5T MRI VBM whole-brain analysis | No | WC with GMV: negatively correlated, especially within the frontal lobe and thalamus. BMI and gray matter: negatively associated. In the healthy subsample, WC with GMV: negatively associated within right gyrus rectus, bilateral frontal lobes, left insula, temporal and cerebellum. |
| 2015, Kaur S [58] | Cross-sectional | n = 103 No C group | 49.63 ± 6.47 (40–60) | VFM and VFV: 1276.33 ± 1021.17 1206.93 ± 961.73 | 3T MRI CT whole-brain analysis | Global cognition (MMSE, Vocabulary and Matrix WASI II subtests and full-scale IQ), Memory (CVLT-II), executive function (TMTA and B, COWA, WAIS III Digit Span and Stroop color–word subtest) | VFM and VFV with CT: positively correlated within the right posterior cingulate gyrus. VFM and VFV with cognitive assessment: no significant association. |
| 2015, Shott ME [59] | Cross-sectional | n = 42 O vs. C (18 vs. 24) W sample (neuroimaging carried out during the first 10 days of the follicular menstrual phase) | O: 28.7.4 ± 8.3 C: 27.4 ± 6.3 The reported data are given by the 2 groups separately | BMI: 34.78 ± 4.44 vs. 21.64 ± 1.26 | 3T MRI VBM whole-brain analysis | Neuropsychiatric assessment: depression (Beck Depression Inventory (BDI)]; novelty seeking, reward dependence and harm avoidance, (Temperament and Character Inventory (TCI)); drive for thinness, body dissatisfaction, bulimia, (Eating Disorder Inventory-3 (EDI-3)); punishment sensitivity, reward sensitivity (Revised Sensitivity to Punishment and Reward Questionnaire (SPSRQ)) and state and trait anxiety (Spielberger State and Trait Anxiety Inventory (STAI)) | O group in comparison to C: lower GMV within the OFC, striatum and insula. In C group, GMV of the gyrus rectus at the medial edge of the OFC predicted functional taste reward-learning response in frontal cortex, insula, basal ganglia, amygdala, hypothalamus and anterior cingulate cortex, but not in the O group. |
| 2015, Kim H [60] | Cross-sectional | n = 1111 O mild/moderate–severe vs. Overweight vs. C vs. Underweight (260/114 vs. 313 vs. 406 vs. 18) Gender-stratified analysis Reported data are for the groups and gender, separately (F/M) | M: 64.7 ± 7.0 W: 62.1 ± 7.3 (≥45) | BMI for Asian population: moderate to severe obesity ≥27.5 vs. 25–27.4 mild obesity vs. 23–24.9 overweight vs. 18.5–22.9 normal weight vs. <18.5 underweight | 3T MRI CT whole-brain analysis | No | M, underweight: lower CT in the frontal and temporal regions; overweight: greater CT in the frontal cortex; mildly O: greater CT in the frontal, temporal and occipital. No significant difference in moderate–severe obesity. W: BMI and CT: no significant association. |
| 2014, Veit R [43] | Cross-sectional | n = 72 O/Overweight vs. Normal weight (13/17 vs. 42) Healthy sample | 29.65 ± 8.15 (19–50) | BMI and VAT: 25.49 ± 5.18 (17.70–46.49) and 2.39 ± 1.56 (0.31–7.58) | 3T MRI CT whole-brain analysis | No | BMI and VAT with CT: negatively correlated within left occipital area, inferior temporal cortex and precentral and inferior parietal areas. VAT with CT: negatively correlated in the right insula, the left fusiform gyrus and the right inferior temporal. |
| 2014, Yau PL [7] | Cross-sectional | n = 53 O vs. C (26 vs. 27) Healthy sample (adolescents) | O: 17.64 ± 1.62 (14.89–20.76) C: 17.22 ± 1.55 (14.28–20.21) The reported data are given by the 2 groups separately | BMI: 35.47 ± 5.88 vs. 21.12 ± 2.18 | 1.5T MRI CT whole-brain analysis | Intellectual functioning and academic achievement (Vocabulary and Matrix Reasoning WASI subtests and WRAT), memory (WRAML), executive function (TMTB, Tower of London Test (TOL), Wisconsin Card Sorting Test (WCST), Stroop Test and COWAT), attention and psychomotor speed (WRAML, TMTA, Digit Vigilance Test (DVT) and Digit Symbol Substitution Test (DSST)) | O group in comparison with C: lower academic achievement (arithmetic and spelling), working memory, attention, psychomotor efficiency and mental flexibility, CT within the OFC and ACC. |
| 2014, Debette S [61] | Cross-sectional | n = 1779 Obesity tertiles (T1: control)Gender-stratified analysis | 72.8 ± 4.1 (≥65) | WHR, BMI and WC: 0.87 ± 0.09 and 25.4 ± 3.8 and 86.4 ± 12.2 | 1.5T MRI VBM whole-brain analysis | No | M and W, WHR with TBV and GMV: negatively correlated; WC and GMV: negatively correlated. More extensive correlations in W. BMI with brain volumes (TVB and GMV): no significant association. Women, WHR with HV: no association after confounder’s adjustment. |
| 2014, Bobb JF [25] | Cross-sectional Prospective longitudinal (5 years) | n = 347 O/Overweight vs. C (142/158 vs. 47) L workers + healthy = Single group | O: 59.8 ± 7.3–64.7 ± 7.4 | BMI: O: 33.1 ± 2.9 vs. Overweight: 27.7 ± 1.4 vs. C: 23.5 ± 1.2 (21.0–43.3) | 1.5T–3T MRI VBM whole-brain and ROI analysis | No | Cross-sectional, BMI with GMV: negatively correlated in ROI and VBM. Longitudinal, BMI with GMV: negatively correlated within the temporal and occipital cortex in ROI. |
| 2014, Lou B [44] | Cross-sectional | n = 49 O/Overweight vs. C (22 vs. 27) Healthy sample (Chinese young adults) | O/Overweight: 31.72 ± 8.04C: 29.04 ± 7.32 The reported data are given by the 2 groups separately | BMI and WC: 31.44 ± 3.34 vs. 21.54 ± 2.06 and 100.25 ± 9.97 vs. 76.91 ± 7.70 | 3T MRI VBM whole-brain analysis | No | O/Overweight group in comparison with C group: lower GMV within the left prefrontal cortex, bilateral cingulate gyrus and the right temporal lobe and greater GMV within the bilateral putamen. BMI and WC with GMV: positively associated within bilateral putamen. |
| 2013, Marqués-Iturria I [45] | Cross-sectional | n = 37 O vs. C (19 vs. 18) Healthy sample | O: 33.7 ± 5.7 C: 32.3 ± 5.9 (20–40) The reported data are given by the 2 groups separately | BMI: 36.08 ± 5.92 vs. 22.54 ± 1.94 (30.1–49.69 vs. 19.53–24.97) | 3T MRI CT whole-brain analysis | No | O group in comparison with controls: reduced CT within left superior frontal and right medial OFC; ventral diencephalon and brainstem volumes. |
| 2013, Kurth F [46] | Cross-sectional | n = 115 O (n = 11) vs. Overweight (n = 11) vs. Normal vs. Underweight Gender-stratified analysisHealthy Caucasian sample | 45.17 ± 15.45 (18–80) | BMI and WC: 25.02 ± 4.13 (18.18–42.37) and 0.87 ± 0.12 (0.67–1.32) | 1.5T MRI VBM whole-brain analysis | No | BMI and WC with GMV: negatively correlated within hypothalamus, prefrontal, anterior temporal and inferior parietal cortex and cerebellum (more widespread and pronounced for WC). W: more extensive correlations for WC than M. |
| 2013, Brooks SJ [8] | Prospective longitudinal (5 years) | n = 292 O vs. C (59 vs. 97) | 75 (70–75) | BMI: 33.0 ± 0.3 vs. 22.5 ± 0.2 | 1.5T MRI VBM whole brain-analysis | Executive function: Trail Making Test | O group in comparison with C: lower global GMV and GMV within bilateral supplementary motor area, bilateral DLPFC, left inferior frontal gyrus and postcentral gyrus and lower executive function (related with DLPFC). |
| 2013, Weise CM [47] | Cross-sectional | n = 76 O vs. Overweight vs. C (36 vs. 8 vs. 36) Healthy sample | 32.1 ± 8.8 | FFMI and adiposity (Body fat % and FMI): 8.4 ± 5.6 and (25.5 ± 10.9 and 21.4 ± 3.8) | 1.5T MRI VBM whole-brain analysis | No | FFMI with GMV: negatively correlated within bilateral temporal regions, the bilateral medial and caudolateral OFC and the left insula independent of adiposity. Adiposity with GMV: no significant association when adjusted for FFM. |
| 2012, Mueller K [62] | Cross-sectional | n = 43 O/Overweight vs. C (27 vs. 16) NSE levels (neuronal injury marker) Young adults | O/Overweight: 26.4 ± 5.4 (20–41) | BMI O/Overweight: 33.0 ± 6.4 (25.3–50.7) | 3T MRI VBM whole-brain analysis | No | O/overweight group in comparison with C: lower GMV and elevated serum NSE levels within the hippocampal cortex and the cerebellum. |
| 2012, Smucny J [63] | Cross-sectional | n = 53 O-prone (overweight) vs. O resistant (lean C) (28 vs. 25) | O-prone (overweight): 30.29 ± 3.81 O resistant: 31.32 ± 3.45 (25–40) | BMI and plasma leptin level: O-prone (overweight): 26.2 ± 2.0 vs. O resistant: 21 ± 2 and O-prone (overweight): 11.42 ± 7.27 vs. O resistant: 3.91 ± 2.89 | 3T MRI VBM whole-brain and ROI analysis | No | O-prone group in comparison with C: lower GMV within the insula, medial OFC and cerebellum. Leptin level and measures of hunger with GMV: negatively correlated within the insula. |
| 2012, Yokum S [29] | Prospective longitudinal (1 year) | n = 83 O vs. Overweight vs. Normal (17 vs. 31 vs. 36) W-adolescent sample | O: 18.4 ± 2.8 | BMI: 17.3–38.9 | 3T MRI VBM whole-brain and ROI analysis | No | 1-year-change BMI with GMV: negatively correlated within bilateral superior frontal and left middle frontal cortex. |
| 2012, Hassenstab JJ [64] | Cross-sectional | n = 53 O vs. Successful weight loss maintainers vs. Never-O lean (C) (17 vs. 17 vs. 19) | O: 47.8 ± 7.6 (27–65) | BMI: 34.0 ± 3.6 vs. 23.7 ± 1.5 vs. 21.7 ± 1.9 | 3T MRI CT ROI analysis | No | O group in comparison with the never-O lean group: lower CT within DACC, PPC and AIC. Successful weight loss maintainers: intermediate results between both O and never-O lean groups, with lower CT within the PPC compared to the never-O lean group. |
| 2010, Walther K [9] | Cross-sectional | n = 95 O vs. Overweight vs. Normal weight (20 vs. 22 vs. 53) Older-W sample | O: 66.9 ± 9.9 (52–92) | BMI: 34.9 ± 3.3 vs. 27.6 ± 1.4 vs. 22.3 ± 1.6 | 3T MRI VBM whole-brain and ROI analysis | MMSE, vocabulary test from WASI, memory (WMS-III, WMS-R and CVLT); executive function (WCST; WAIS-R; verbal fluency task, WMS-III and processing speed (TMTA)) | BMI with GMV: negatively correlated within the left orbitofrontal, right inferior frontal, precentral gyri, parahippocampal, fusiform and lingual gyri and cerebellar regions. O group: lower executive function. |
| 2009, Narita K [65] | Cross-sectional | n = 34 Asian population BMI > 27 excluded Gender-stratified analysis | M: 64.8 ± 5.1 (57–76) W: 64.3 ± 4.4 (56–74) | Plasma leptin level (ng/mL): M: 3.1 ± 1.7 W: 4.9 ± 1.9 | 3T MRI VBM whole-brain analysis | No | Leptin level with total GMV: no significant association. Leptin level with GMV: positively correlated within the right hippocampus and bilateral cerebellum (leptin acts as a neuroprotective hormone in those regions). M and W separately: no significant associations. |
| 2008, Taki Y [66] | Cross-sectional | n = 1428 O (n = 27) vs. Overweight (n = 273) vs. Normal vs. Underweight Gender-stratified analysis Japanese sample Reported data is for the groups and gender, separately (F/M) | M: 44.5 ± 16.1 W: 46.4 ± 14.1 (12–81) | BMI: M: 23.41 ± 3.00 (13.2–40.1) W: 22.23 ± 2.97 (15.2–33.3) | 0.5T MRI VBM whole-brain analysis | No | M, BMI with GMR (GMV/ICV): negatively correlated; with GMV: negatively correlated within all lobes, anterior cerebellum and midbrain and positively correlated within frontal and temporal lobes, cerebellum, thalami and caudate. W, BMI with GMR and GMV: no significant association. |
| 2007, Pannacciulli N [48] | Cross-sectional | n = 32 O vs. C (16 vs. 16) Caucasian participants Healthy sample | 32 ± 9 (18–49) | Plasma leptin level (ng/mL): 16 ± 20 (0.5–65) | 1.5T MRI VBM whole-brain analysis | No | Plasma leptin levels and GMV: positively correlated within the left cerebellum and inferior temporal gyrus and negatively correlated within the left inferior frontal operculum, postcentral gyrus and right putamen. |
| 2006, Pannacciulli N [22] | Cross-sectional | n = 60 O vs. C (24 vs. 36) Non-diabetic Caucasian participants Healthy sample | O: 32 ± 8 L:33 ± 9 | BMI: 39.4 ± 4.7 vs. 22.7 ± 2.2 | 1.5T MRI VBM whole-brain analysis | No | O group in comparison with C: lower GM density within the post-gyrus, frontal operculum, putamen and middle frontal gyrus. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Andújar, M.; Morales-García, E.; García-Casares, N. Obesity and Gray Matter Volume Assessed by Neuroimaging: A Systematic Review. Brain Sci. 2021, 11, 999. https://doi.org/10.3390/brainsci11080999
Fernández-Andújar M, Morales-García E, García-Casares N. Obesity and Gray Matter Volume Assessed by Neuroimaging: A Systematic Review. Brain Sciences. 2021; 11(8):999. https://doi.org/10.3390/brainsci11080999
Chicago/Turabian StyleFernández-Andújar, Marina, Ester Morales-García, and Natalia García-Casares. 2021. "Obesity and Gray Matter Volume Assessed by Neuroimaging: A Systematic Review" Brain Sciences 11, no. 8: 999. https://doi.org/10.3390/brainsci11080999
APA StyleFernández-Andújar, M., Morales-García, E., & García-Casares, N. (2021). Obesity and Gray Matter Volume Assessed by Neuroimaging: A Systematic Review. Brain Sciences, 11(8), 999. https://doi.org/10.3390/brainsci11080999