
Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
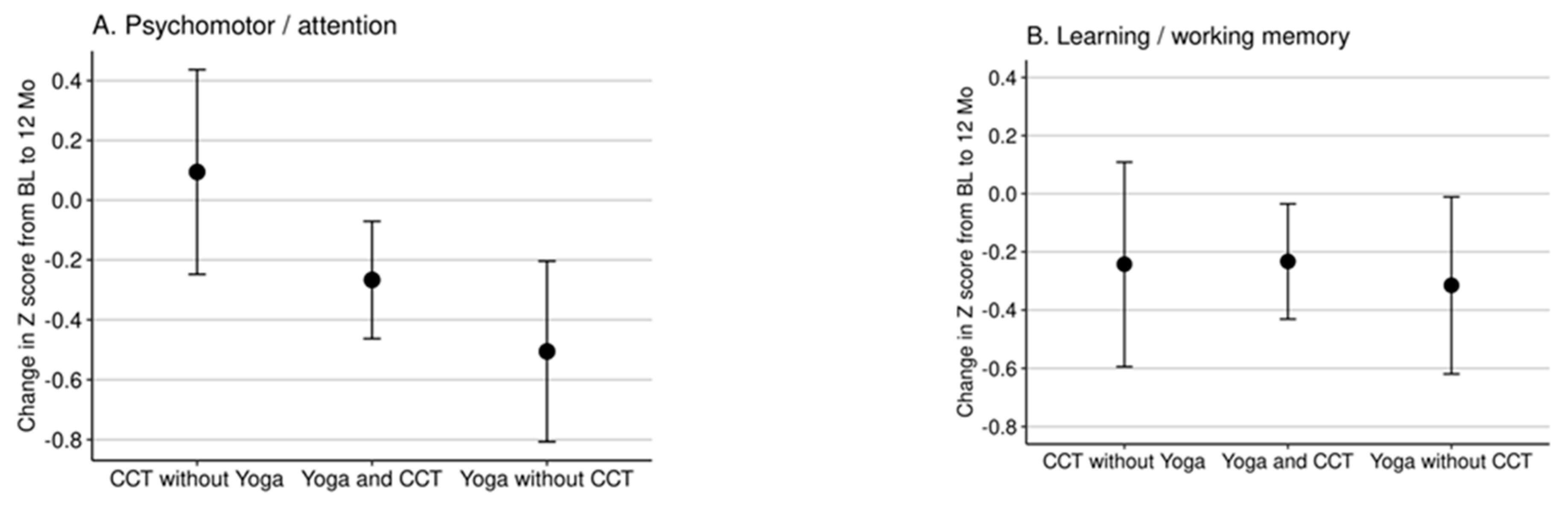
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Census Bureau. An Aging World: 2015 International Population Reports. Available online: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf (accessed on 7 June 2021).
- Alzheimer’s Disease International. World Alzheimer Report 2015. In The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Stern, C.; Munn, Z. Cognitive leisure activities and their role in preventing dementia: A systematic review. Int. J. Evid. Based Healthc. 2010, 8, 2–17. [Google Scholar] [CrossRef]
- Hughes, T.F.; Chang, C.C.; Vander Bilt, J.; Ganguli, M. Engagement in reading and hobbies and risk of incident dementia: The MoVIES project. Am. J. Alzheimers Dis. Other Dement. 2010, 25, 432–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basak, C.; Qin, S.; O’Connell, M.A. Differential effects of cognitive training modules in healthy aging and mild cognitive impairment: A comprehensive meta-analysis of randomized controlled trials. Psychol. Aging 2020, 35, 220–249. [Google Scholar] [CrossRef] [PubMed]
- Borella, E.; Carretti, B.; Riboldi, F.; De Beni, R. Working memory training in older adults: Evidence of transfer and maintenance effects. Psychol. Aging 2010, 25, 767–778. [Google Scholar] [CrossRef] [Green Version]
- Zinke, K.; Zeintl, M.; Rose, N.S.; Putzmann, J.; Pydde, A.; Kliegel, M. Working memory training and transfer in older adults: Effects of age, baseline performance, and training gains. Dev. Psychol. 2014, 50, 304–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richmond, L.L.; Morrison, A.B.; Chein, J.M.; Olson, I.R. Working memory training and transfer in older adults. Psychol. Aging 2011, 26, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Anguera, J.A.; Boccanfuso, J.; Rintoul, J.L.; Al-Hashimi, O.; Faraji, F.; Janowich, J.; Gazzaley, A. Video game training enhances cognitive control in older adults. Nature 2013, 501, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebok, G.W.; Ball, K.; Guey, L.T.; Jones, R.N.; Kim, H.Y.; King, J.W.; Group, A.S. Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J. Am. Geriatr. Soc. 2014, 62, 16–24. [Google Scholar] [CrossRef]
- Wolinsky, F.D.; Vander Weg, M.W.; Howren, M.B.; Jones, M.P.; Dotson, M.M. A randomized controlled trial of cognitive training using a visual speed of processing intervention in middle aged and older adults. PLoS ONE 2013, 8, e61624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.E.; Housen, P.; Yaffe, K.; Ruff, R.; Kennison, R.F.; Mahncke, H.W.; Zelinski, E.M. A cognitive training program based on principles of brain plasticity: Results from the Improvement in Memory with Plasticity-based Adaptive Cognitive Training (IMPACT) study. J. Am. Geriatr. Soc. 2009, 57, 594–603. [Google Scholar] [CrossRef] [Green Version]
- Barnes, D.E.; Yaffe, K.; Belfor, N.; Jagust, W.J.; DeCarli, C.; Reed, B.R.; Kramer, J.H. Computer-based cognitive training for mild cognitive impairment: Results from a pilot randomized, controlled trial. Alzheimer Dis. Assoc. Disord. 2009, 23, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Gates, N.J.; Vernooij, R.W.; Di Nisio, M.; Karim, S.; March, E.; Martinez, G.; Rutjes, A.W. Computerised cognitive training for preventing dementia in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2019, 3, CD012279. [Google Scholar] [CrossRef]
- Jia, R.X.; Liang, J.H.; Xu, Y.; Wang, Y.Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef]
- Gates, N.; Fiatarone Singh, M.A.; Sachdev, P.S.; Valenzuela, M. The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am. J. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef]
- Song, D.; Yu, D.S.F.; Li, P.W.C.; Lei, Y. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2018, 79, 155–164. [Google Scholar] [CrossRef]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef]
- Bhattacharyya, K.K.; Andel, R.; Small, B.J. Effects of yoga-related mind-body therapies on cognitive function in older adults: A systematic review with meta-analysis. Arch. Gerontol. Geriatr. 2020. [Google Scholar] [CrossRef]
- Maffei, L.; Picano, E.; Andreassi, M.; Angelucci, A.; Baldacci, F.; Baroncelli, L.; Biagi, L. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef]
- Sr, P.A.A.; DeFeis, B.; De Wit, L.; O’Shea, D.; Mejia, A.; Chandler, M.; Smith, G. Functional ability is associated with higher adherence to behavioral interventions in mild cognitive impairment. Clin. Neuropsychol. 2020, 34, 937–955. [Google Scholar] [CrossRef] [Green Version]
- Chandler, M.J.; Locke, D.E.; Crook, J.E.; Fields, J.A.; Ball, C.T.; Phatak, V.S.; Smith, G.E. Comparative Effectiveness of Behavioral Interventions on Quality of Life for Older Adults with Mild Cognitive Impairment: A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e193016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amofa, P.A.; Locke, D.E.C.; Chandler, M.; Crook, J.E.; Ball, C.T.; Phatak, V.; Smith, G.E. Comparative effectiveness of behavioral interventions to prevent or delay dementia: One year partner outcomes. J. Prev. Alzheimers Dis. 2021, 8, 33–40. [Google Scholar]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Smith, G.; Chandler, M.; Locke, D.E.; Fields, J.; Phatak, V.; Crook, J.; Cochran, D. Behavioral Interventions to Prevent or Delay Dementia: Protocol for a Randomized Comparative Effectiveness Study. JMIR Res. Protoc. 2017, 6, e223. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, J.; Maruff, P.; Woodward, M.; Moore, L.; Fredrickson, A.; Sach, J.; Darby, D. Evaluation of the usability of a brief computerized cognitive screening test in older people for epidemiological studies. Neuroepidemiology 2010, 34, 65–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darby, D.; Maruff, P.; Collie, A.; McStephen, M. Mild cognitive impairment can be detected by multiple assessments in a single day. Neurology 2002, 59, 1042–1046. [Google Scholar] [CrossRef]
- Maruff, P.; Lim, Y.Y.; Darby, D.; Ellis, K.A.; Pietrzak, R.H.; Snyder, P.J.; Group, A.R. Clinical utility of the cogstate brief battery in identifying cognitive impairment in mild cognitive impairment and Alzheimer’s disease. BMC Psychol. 2013, 1, 30. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N.; Sherwood, A. Aerobic Exercise and Neurocognitive Performance: A Meta-Analytic Review of Randomized Controlled Trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef]
- Shandera-Ochsner, A.L.; Chandler, M.J.; Locke, D.L.; Ball, C.T.; Crook, J.E.; Phatak, V.S.; Smith, G.E. Comparative effects of physical exercise and other behavioral interventions on functional status outcomes in mild cognitive impairment. J. Int. Neuropsychol. Soc. 2021. accepted. [Google Scholar]


{kind=link}
| Composite Score | No Yoga (N = 31) | No CCT (N = 43) | No Wellness Education (N = 40) | No Support Groups (N = 35) | No MSS-Calendar (N = 34) |
|---|---|---|---|---|---|
| Age, mean (SD) | 75.4 (7.5) | 75.7 (8.6) | 77.1 (7.0) | 74.5 (8.4) | 74.2 (7.9) |
| Male % | 64.5 | 60.5 | 60.0 | 68.6 | 52.9 |
| Composite Score | No Yoga | No CCT | No Wellness Education | No Support Groups | No MSS−Calendar | Baseline p Value |
|---|---|---|---|---|---|---|
| Psychomotor/attention | ||||||
| Baseline, mean (SD) | −0.073 (0.905) | 0.036 (0.868) | −0.196 (0.969) | 0.072 (0.910) | 0.174 (0.797) | 0.32 |
| 12 months, mean (SD) | −0.008 (1.010) | −0.446 (1.033) | −0.640 (1.243) | −0.263 (0.924) | −0.066 (1.058) | |
| Learning/working memory | ||||||
| Baseline, mean (SD) | 0.133 (1.027) | 0.068 (0.823) | −0.200 (0.807) | 0.157 (0.749) | −0.130 (0.848) | 0.32 |
| 12 months, mean (SD) | −0.145 (1.004) | −0.197 (1.199) | −0.174 (0.867) | −0.258 (0.942) | −0.002 (0.909) |
| Composite | Contrasts | Difference at 12 mo (95% CI) | Original p Value | Adjusted p Value |
|---|---|---|---|---|
| Primary outcome | ||||
| Psychomotor/Attention | CCT vs. Yoga | 0.54 (0.15 to 0.92) | 0.007 | 0.021 |
| CCT without Yoga vs. CCT with Yoga | 0.32 (−0.00 to 0.65) | 0.053 | 0.11 | |
| Yoga without CCT vs. Yoga with CCT | −0.21 (−0.51 to 0.09) | 0.17 | 0.17 | |
| Secondary outcome | ||||
| Learning/ Working memory | CCT vs. Yoga | 0.06 (−0.31 to 0.44) | 0.75 | 1.00 |
| CCT without Yoga vs. CCT with Yoga | −0.01 (−0.33 to 0.31) | 0.96 | 1.00 | |
| Yoga without CCT vs. Yoga with CCT | −0.07 (−0.36 to 0.22) | 0.64 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phatak, V.S.; Smith, G.E.; Locke, D.; Shandera-Ochsner, A.; Dean, P.M.; Ball, C.; Gutierrez, G.; Chandler, M.J. Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment. Brain Sci. 2021, 11, 988. https://doi.org/10.3390/brainsci11080988
Phatak VS, Smith GE, Locke D, Shandera-Ochsner A, Dean PM, Ball C, Gutierrez G, Chandler MJ. Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment. Brain Sciences. 2021; 11(8):988. https://doi.org/10.3390/brainsci11080988
Chicago/Turabian StylePhatak, Vaishali S., Glenn E. Smith, Dona Locke, Anne Shandera-Ochsner, Pamela M. Dean, Colleen Ball, Gianna Gutierrez, and Melanie J. Chandler. 2021. "Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment" Brain Sciences 11, no. 8: 988. https://doi.org/10.3390/brainsci11080988
APA StylePhatak, V. S., Smith, G. E., Locke, D., Shandera-Ochsner, A., Dean, P. M., Ball, C., Gutierrez, G., & Chandler, M. J. (2021). Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment. Brain Sciences, 11(8), 988. https://doi.org/10.3390/brainsci11080988