
Modulated Neuroprotection in Unresponsive Wakefulness Syndrome after Severe Traumatic Brain Injury

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
- Actovegin, a deproteinized hemoderivative obtained by ultrafiltration from calf blood, in order to increase the cellular energy metabolism, the respiratory capacity of mitochondria, and the oxygen and the glucose uptake [12];
- pyritinolum (Encephabol), facilitates the passing of glucose across the blood–brain barrier and increases its metabolism in the neuronal tissue; it also shows antioxidant properties [13];
- cyanocobalamin improves nerve repair and functional recovery after TBI [16];
- alpha-lipoic acid is neuroprotective by preserving blood–brain barrier permeability and by reducing brain edema probably via its anti-inflammatory and antioxidant properties in the TBI model [17];
- carotene (pro A vitamin), coenzyme Q-10, L-carnitine, DL-α-tocopherol acetate (E vitamin), and ascorbic acid are antioxidants, protecting neuronal cells from oxidative stress. DL-α-tocopherol acetate is an antioxidant with anti-inflammatory properties and also exhibits modulatory activities of autophagy [18,19,20];
- pyridoxine has been chosen for its neuroprotection properties and behavioral function improvement in experimental studies [23].
2. Materials and Methods
2.1. Inclusion Criteria
- Patients over 18 years old;
- diagnosed with severe TBI (Glasgow Coma Scale (GCS) of 3–8 points at admission) [24];
- TBI followed by coma and then UWS;
- personal history of severe TBI not older than 3 months;
- association of different comorbidities in the context of polytrauma.
2.2. Exclusion Criteria
- Patients with UWS induced by any pathology other than TBI;
- patients with UWS after medium (CGS of 9–12 points) or mild TBI (GCS of 13–15 points) [24] associated or not with other factors which may induce UWS;
- personal history of severe TBI older than 3 months;
- patients with any modified conscience state after severe TBI other than UWS.
2.3. Study Design
2.4. Patients’ Rehabilitation Management
2.5. Neuroprotective Treatment
- Actovegin, 400 mg/day, every day for the first year; in the second year, 400 mg/day, 21 days each month for 6 months, then 400 mg/day, 14 days each month for another 6 months;
- Cerebrolysin, starting from the second year, 10 mL/day, a set of 10 days every three months, for one year;
- pyritinol (Encephabol) 100 mg, once a day for the first 6 months, then every other two months;
- L-phosphothreonine: 20 mg/day, L-glutamine 75 mg/day, and hydroxocobalamin 500 µg/day, daily for the first two months, then 10 days per month; during the second year, 10 days every 3 months;
- alpha-lipoic acid, 600 mg/daily for the first 3 months, then daily for a month every 3 months;
- carotene 10 mg/day, DL-α-tocopherol acetate 40 mg/day, ascorbic acid 100 mg/day, for the first 3 months;
- thiamine 100 mg/day, pyridoxine 100 mg/day, and cyanocobalamin 50 µg/day, 10 days per month for the first three months;
- coenzyme Q-10, 30 mg daily for a month, every 3 months;
- L-carnitine 100 mg, daily the first month, then 10 days per month, every 3 months.
2.6. Evaluated Parameters
2.7. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Clinical and Paraclinical Features
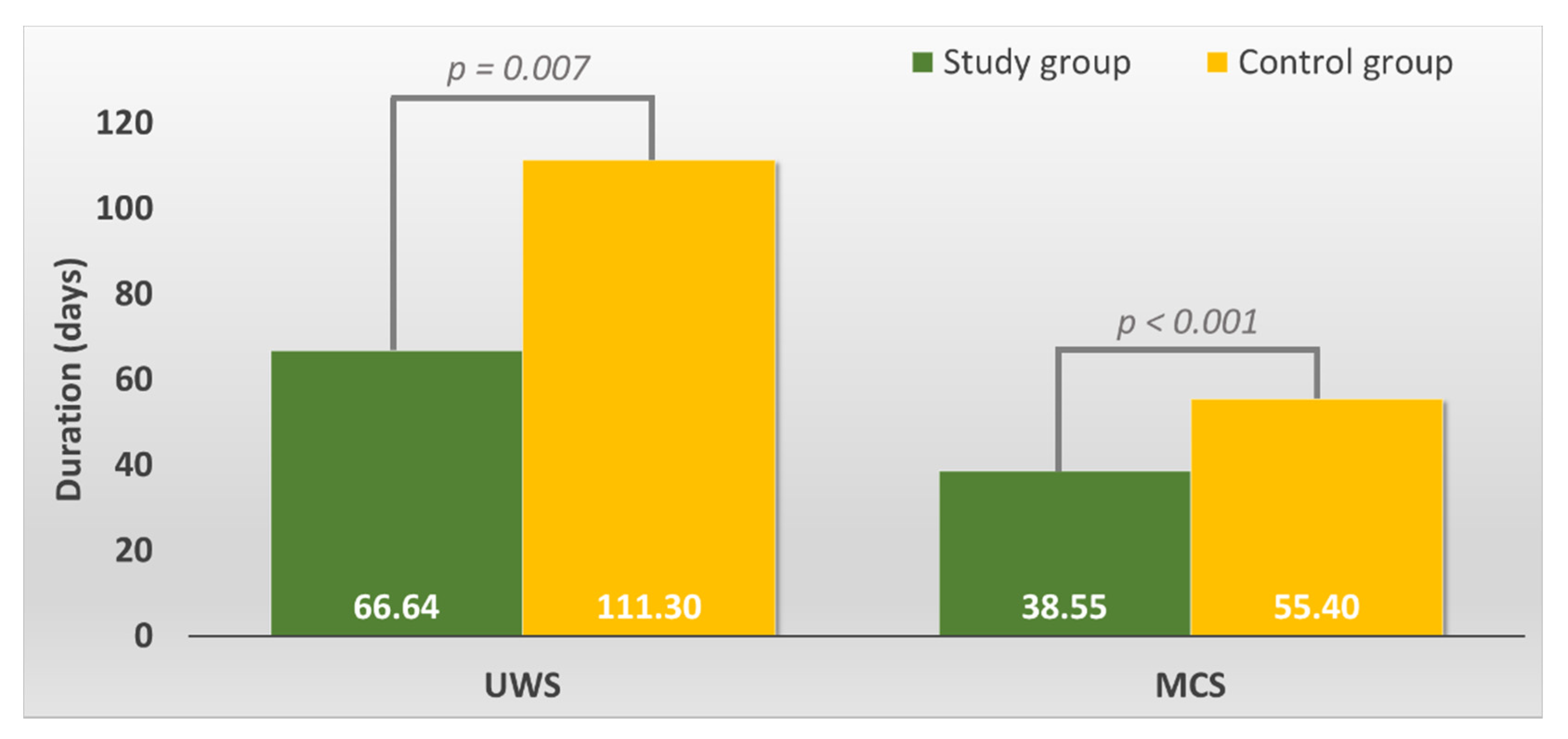
3.3. Cognitive Evolution
- Unresponsive Wakefulness Syndrome (UWS)
- 2.
- Minimally Conscious State (MCS)
- 3.
- Moderate Conscious State (MoCS)
- 4.
- Psycho-Cognitive state (PCS)
3.4. Functional Level
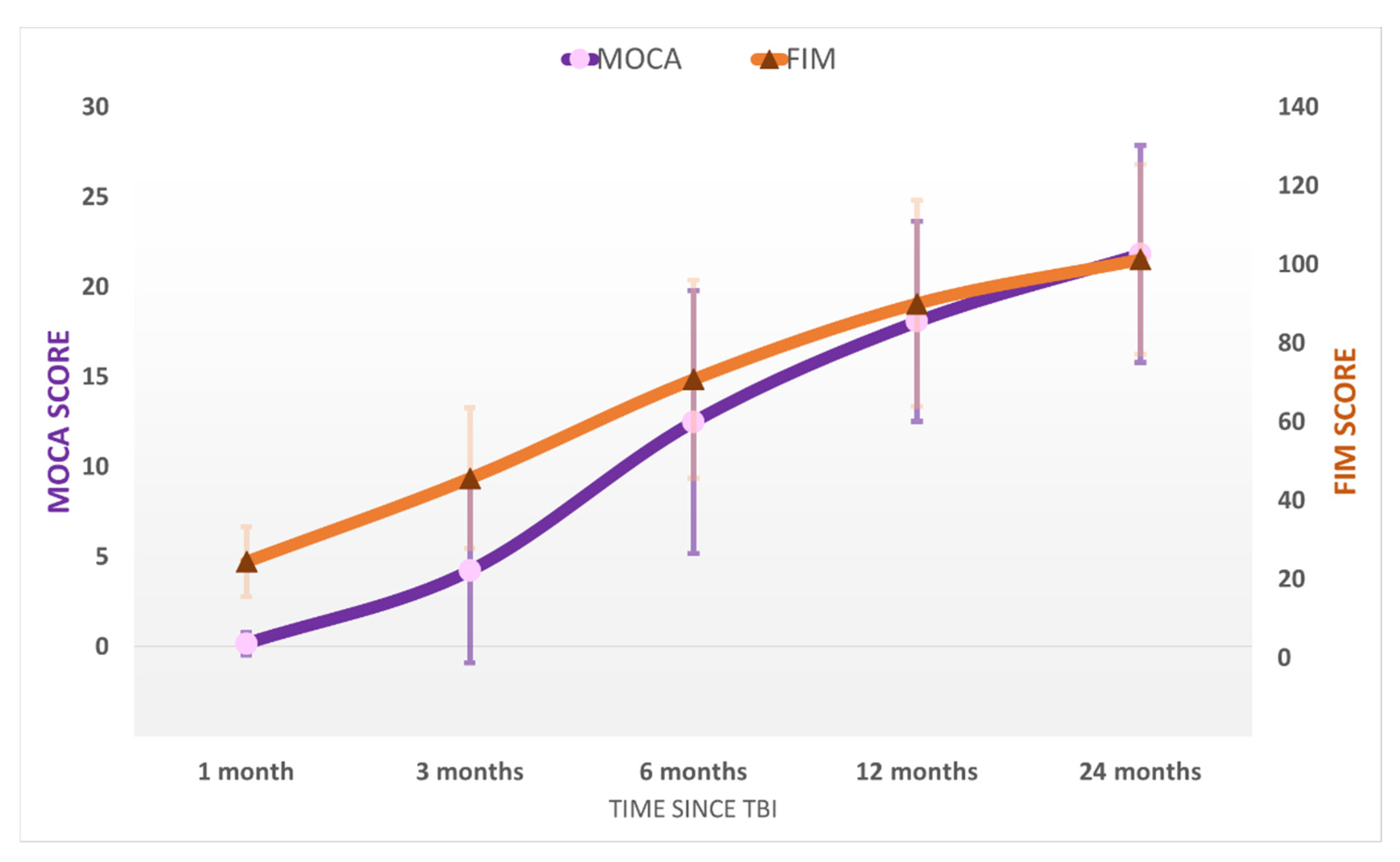
- In the UWS period, the average FIM level was 19 ± 3 in the control group and 24 ± 9 in the study group, which functionally means the patient is bedridden in both groups.
- In the MCS state, in the control group the average FIM was 29 ± 4 (bedridden), while in the study group, FIM = 46 ± 18, functionally meaning the patient was mobilized in the specially adapted wheelchair.
- Only patients in the study group achieved the MoCS state. The average FIM was 71 ± 26 meaning, in general, that the patients maintained the sitting position in the normal wheelchair and were elevated using a tilt table for the orthostatic position.
- In the PCS the average FIM in the study group at evaluation 12 was 90 ± 27, which equivalated to patients walking with the high rolled frame assisted by the kinesiotherapist. At the final evaluation, 24 months after the TBI, the average FIM was 101 ± 25, which corresponded to assisted gait (eventually only with surveillance for those patients with higher scores).
3.5. Cognitive and Functional Statistical Analysis in the Study Group
4. Discussions
4.1. Limitations of the Study
4.2. Neuroprotection Treatment
4.3. Lesions of the Brain
4.4. Death of Patients in UWS after Severe TBI
4.5. Cognitive Evolution
4.6. Functional Level
4.7. Rehabilitation Program
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuller, G.W.; Ransom, J.; Mandrekar, J.; Brown, A.W. Long-Term Survival Following Traumatic Brain Injury: A Population-Based Parametric Survival Analysis. Neuroepidemiology 2016, 47, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Huff, J.S.; Tadi, P. Coma. [Updated 8 July 2021]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430722/ (accessed on 8 July 2021).
- Firsching, R. Coma After Acute Head Injury. Dtsch. Arztebl. Int. 2017, 114, 313–320. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Kavusipur, S.; Rojhani Shirazi, Z.; Ardekani, Z.; Omidi, S. Prediction of Consciousness Recovery in Coma after Traumatic Brain Injury by Disorder of Consciousness Scale (DOCS). Bull. Emerg. Trauma 2013, 1, 86–89. [Google Scholar]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice guideline update recommendations summary: Disorders of consciousness. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology 2018, 91, 450–460. [Google Scholar] [CrossRef]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef]
- Muresanu, D.; Birle, C.; Muresanu, I.; Costin, C.; Vester, J.; Rafila, A.; Verisezan Rosu, O.; Slavoaca, D. Neuroprotection in TBI. In Neurotrauma: A Comprehensive Textbook on Traumatic Brain Injury and Spinal Cord Injury; Wang, K.K.W., Ed.; Oxford University Press: Oxford, UK, 2018; pp. 333–346. [Google Scholar] [CrossRef]
- Onose, G.; Daia-Chendreanu, C.; Haras, M.; Ciurea, A.; Anghelescu, A. Traumatic brain injury: Current endeavours and trends for neuroprotection and related recovery. Rom. Neurosurg. 2011, 18, 11–30. [Google Scholar]
- Muresanu, D.F.; Florian, S.; Hömberg, V.; Matula, C.; von Steinbüchel, N.; Vos, P.E.; von Wild, K.; Birle, C.; Muresanu, I.; Slavoaca, D.; et al. Efficacy and safety of cerebrolysin in neurorecovery after moderate-severe traumatic brain injury: Results from the CAPTAIN II trial. Neurol. Sci. 2020, 41, 1171–1181. [Google Scholar] [CrossRef]
- Bornstein, N.M.; Guekht, A.; Vester, J.; Heiss, W.D.; Gusev, E.; Hömberg, V.; Rahlfs, V.W.; Bajenaru, O.; Popescu, B.O.; Muresanu, D. Safety and efficacy of Cerebrolysin in early post-stroke recovery: A meta-analysis of nine randomized clinical trials. Neurol. Sci. 2018, 39, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Onose, G.; Mureşanu, D.F.; Ciurea, A.V.; Daia Chendreanu, C.; Mihaescu, A.S.; Mardare, D.C.; Andone, I.; Spânu, A.; Popescu, C.; Dumitrescu, A.; et al. Neuroprotective and consequent neurorehabilitative clinical outcomes, in patients treated with the pleiotropic drug cerebrolysin. J. Med. Life 2009, 2, 350–360. [Google Scholar]
- Passler, M.A.; Riggs, R.V. Positive outcomes in traumatic brain injury-vegetative state: Patients treated with bromocriptine. Arch. Phys. Med. Rehabil. 2001, 82, 311–315. [Google Scholar] [CrossRef]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau-Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74, 1063–1072. [Google Scholar] [CrossRef]
- Berg, A.; Bellander, B.M.; Wanecek, M.; Gamrin, L.; Elving, A.; Rooyackers, O.; Ungerstedt, U.; Wernerman, J. Intravenous glutamine supplementation to head trauma patients leaves cerebral glutamate concentration unaffected. Intensive Care Med. 2006, 32, 1741–1746. [Google Scholar] [CrossRef]
- Wu, F.; Xu, K.; Liu, L.; Zhang, K.; Xia, L.; Zhang, M.; Teng, C.; Tong, H.; He, Y.; Xue, Y.; et al. Vitamin B(12) Enhances Nerve Repair and Improves Functional Recovery After Traumatic Brain Injury by Inhibiting ER Stress-Induced Neuron Injury. Front. Pharmacol. 2019, 10, 406. [Google Scholar] [CrossRef]
- Toklu, H.Z.; Hakan, T.; Biber, N.; Solakoğlu, S.; Oğünç, A.V.; Sener, G. The protective effect of alpha lipoic acid against traumatic brain injury in rats. Free Radic. Res. 2009, 43, 658–667. [Google Scholar] [CrossRef]
- Di Pietro, V.; Yakoub, K.M.; Caruso, G.; Lazzarino, G.; Signoretti, S.; Barbey, A.K.; Tavazzi, B.; Lazzarino, G.; Belli, A.; Amorini, A.M. Antioxidant Therapies in Traumatic Brain Injury. Antioxidants 2020, 9, 260. [Google Scholar] [CrossRef]
- Allan, K.; Hayes, K.; Thomas, M.; Barnard, K. Coenzyme Q10 supplementation in traumatic brain injury: A scoping review protocol. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 1901–1908. [Google Scholar] [CrossRef]
- Chen, H.; Chan, Y.L.; Linnane, C.; Mao, Y.; Anwer, A.G.; Sapkota, A.; Annissa, T.F.; Herok, G.; Vissel, B.; Oliver, B.G.; et al. L-Carnitine and extendin-4 improve outcomes following moderate brain contusion injury. Sci. Rep. 2018, 8, 11201. [Google Scholar] [CrossRef] [PubMed]
- Mkrtchyan, G.V.; Üçal, M.; Müllebner, A.; Dumitrescu, S.; Kames, M.; Moldzio, R.; Molcanyi, M.; Schaefer, S.; Weidinger, A.; Schaefer, U.; et al. Thiamine preserves mitochondrial function in a rat model of traumatic brain injury, preventing inactivation of the 2-oxoglutarate dehydrogenase complex. Biochim. Biophys. Acta (BBA) Bioenerg. 2018, 1859, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Jhala, S.S.; Hazell, A.S. Modeling neurodegenerative disease pathophysiology in thiamine deficiency: Consequences of impaired oxidative metabolism. Neurochem. Int. 2011, 58, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, N.J.; Hoane, M.R. Pyridoxine administration improves behavioral and anatomical outcome after unilateral contusion injury in the rat. J. Neurotrauma 2010, 27, 1275–1282. [Google Scholar] [CrossRef]
- Jain, S.; Iverson, L.M. Glasgow coma scale. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/nbk513298/ (accessed on 3 August 2021).
- Mena, J.H.; Sanchez, A.I.; Rubiano, A.M.; Peitzman, A.B.; Sperry, J.L.; Gutierrez, M.I.; Puyana, J.C. Effect of the modified Glasgow Coma Scale score criteria for mild traumatic brain injury on mortality prediction: Comparing classic and modified Glasgow Coma Scale score model scores of 13. J. Trauma 2011, 71, 1185–1192, discussion 1193. [Google Scholar] [CrossRef]
- Lu, J.; Marmarou, A.; Lapane, K.; Turf, E.; Wilson, L.; Group, I.; American Brain Injury Consortium Study Participation Centers. A method for reducing misclassification in the extended Glasgow Outcome Score. J. Neurotrauma 2010, 27, 843–852. [Google Scholar] [CrossRef]
- Rappaport, M.; Hall, K.M.; Hopkins, K.; Belleza, T.; Cope, D.N. Disability rating scale for severe head trauma: Coma to community. Arch. Phys. Med. Rehabil. 1982, 63, 118–123. [Google Scholar]
- de Guise, E.; Alturki, A.Y.; LeBlanc, J.; Champoux, M.C.; Couturier, C.; Lamoureux, J.; Desjardins, M.; Marcoux, J.; Maleki, M.; Feyz, M. The Montreal Cognitive Assessment in persons with traumatic brain injury. Appl. Neuropsychol. Adult 2014, 21, 128–135. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Shukla, D.; Devi, B.I.; Agrawal, A. Outcome measures for traumatic brain injury. Clin. Neurol. Neurosurg. 2011, 113, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Olaya, J.; Noé, E.; Navarro, M.D.; O’Valle, M.; Colomer, C.; Moliner, B.; Ippoliti, C.; Ferri, J.; Maza, A.; Llorens, R. When, How, and to What Extent Are Individuals with Unresponsive Wakefulness Syndrome Able to Progress? Functional Independence. Brain Sci. 2020, 10, 990. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J. The prognostic factors related to traumatic brain stem injury. J. Korean Neurosurg. Soc. 2012, 51, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, M.; Katsakiori, P.; Kefalopoulou, Z.; Ellul, J.; Chroni, E.; Constantoyannis, C. Vegetative state and minimally conscious state: A review of the therapeutic interventions. Stereotact. Funct. Neurosurg. 2010, 88, 199–207. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lesions Identified on Brain Imaging | Study Group (n = 33) | Control Group (n = 27) |
|---|---|---|
| Intracerebral hemorrhage | 15 (45.5%) | 11 (40.7%) |
| Subarachnoid hemorrhage | 16 (48.5%) | 8 (29.6%) |
| Subdural hemorrhage | 4 (12.1%) | 2 (7.4%) |
| Diffuse axonal injury | 8 (24.2%) | 9 (33.3%) |
| Traumatic subdural hygroma | 2 (6.1%) | 2 (7.4%) |
| Internal capsule/thalamic contusion | 4 (12.1%) | 1 (3.7%) |
| Brainstem contusion | 1 (3.0%) | 5 (18.5%) |
| Hemispheric contusion | - | - |
| Frontal | 18 (54.5%) | 14 (51.9%) |
| Temporal | 18 (54.5%) | 12 (44.4%) |
| Parietal | 12 (36.4) | 10 (37.0%) |
| Occipital | 1 (3.0%) | 1 (3.7%) |
| Bilateral | 6 (18.1%) | 7 (25.9%) |
| Hemispheric laceration | 3 (9.1%) | 6 (22.2%) |
| Parameter | Study Group (n = 33) | Control Group (n = 27) |
|---|---|---|
| Cause leading to TBI | - | - |
| car accident | 24 (72.73%) | 18 (66.67%) |
| aggression | 5 (15.15%) | 5 (18.52%) |
| work accident | 1 (3.03%) | 1 (3.70%) |
| domestic accident | 1 (3.03%) | 2 (7.41%) |
| train accident | 2 (6.06%) | 1 (3.70%) |
| Associated traumatic injuries | - | - |
| thoraco-abdominal contusion | 33 (100%) | 27 (100%) |
| articular contusion (hip, knee, shoulder, elbow) | 12 (36.36%) | 10 (37.04%) |
| internal organ rupture (spleen, liver, kidney, lung) | 10 (30.30%) | 7 (25.93%) |
| calvaria or facial bones fracture | 12 (36.36%) | 7 (25.93%) |
| limbs or pelvic fracture | 18 (54.55%) | 15 (55.56%) |
| rib cage fracture | 21 (63.64%) | 14 (51.85%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daia, C.; Scheau, C.; Spinu, A.; Andone, I.; Popescu, C.; Toader, C.; Bumbea, A.M.; Verenca, M.C.; Onose, G. Modulated Neuroprotection in Unresponsive Wakefulness Syndrome after Severe Traumatic Brain Injury. Brain Sci. 2021, 11, 1044. https://doi.org/10.3390/brainsci11081044
Daia C, Scheau C, Spinu A, Andone I, Popescu C, Toader C, Bumbea AM, Verenca MC, Onose G. Modulated Neuroprotection in Unresponsive Wakefulness Syndrome after Severe Traumatic Brain Injury. Brain Sciences. 2021; 11(8):1044. https://doi.org/10.3390/brainsci11081044
Chicago/Turabian StyleDaia, Cristina, Cristian Scheau, Aura Spinu, Ioana Andone, Cristina Popescu, Corneliu Toader, Ana Maria Bumbea, Madalina Codruta Verenca, and Gelu Onose. 2021. "Modulated Neuroprotection in Unresponsive Wakefulness Syndrome after Severe Traumatic Brain Injury" Brain Sciences 11, no. 8: 1044. https://doi.org/10.3390/brainsci11081044
APA StyleDaia, C., Scheau, C., Spinu, A., Andone, I., Popescu, C., Toader, C., Bumbea, A. M., Verenca, M. C., & Onose, G. (2021). Modulated Neuroprotection in Unresponsive Wakefulness Syndrome after Severe Traumatic Brain Injury. Brain Sciences, 11(8), 1044. https://doi.org/10.3390/brainsci11081044