
Using System Identification to Construct an Inherent Model of Pupillary Light Reflex to Explore Diabetic Neuropathy


Abstract
1. Introduction
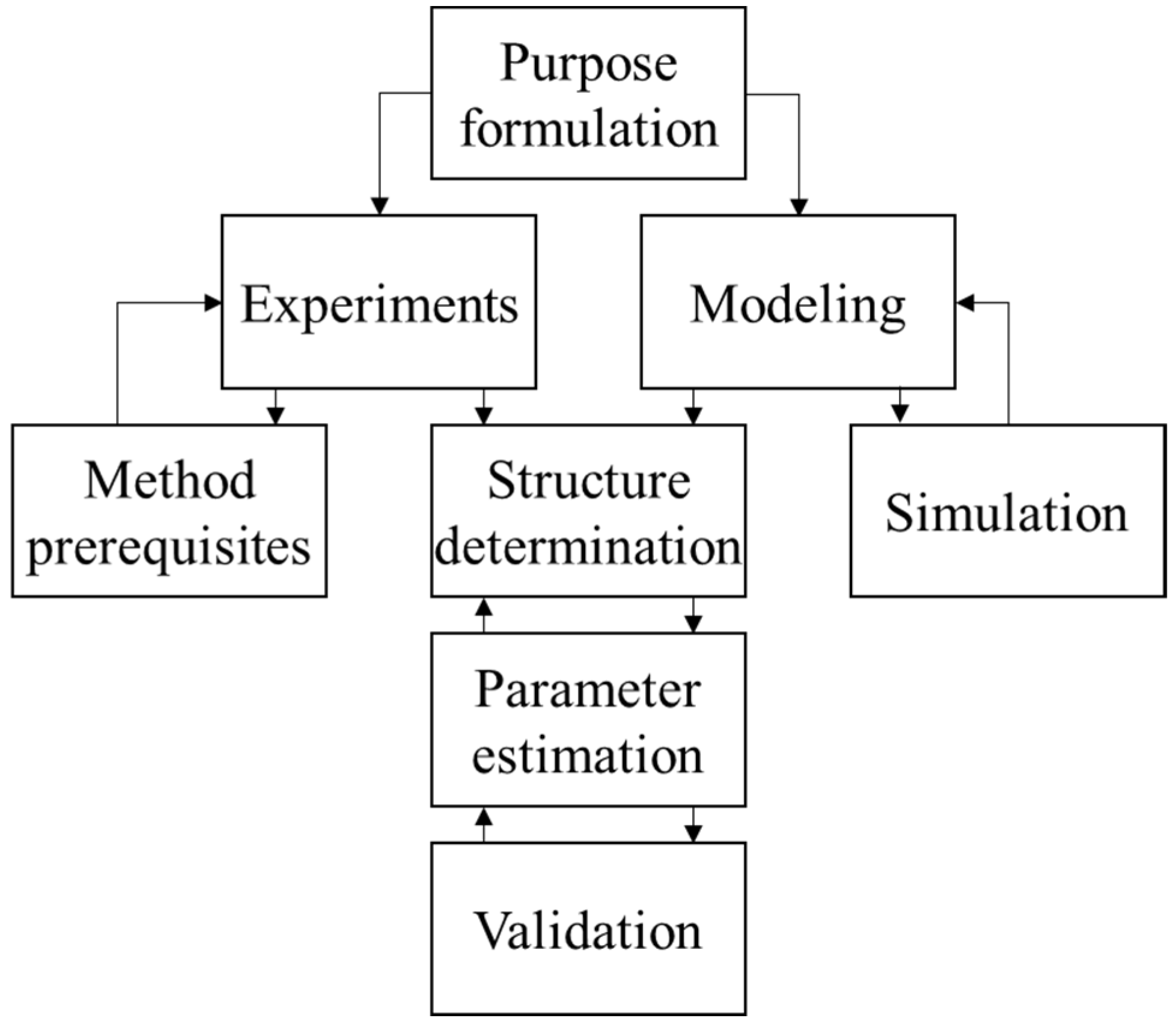
2. System Identification of Pupillary Light Reflex
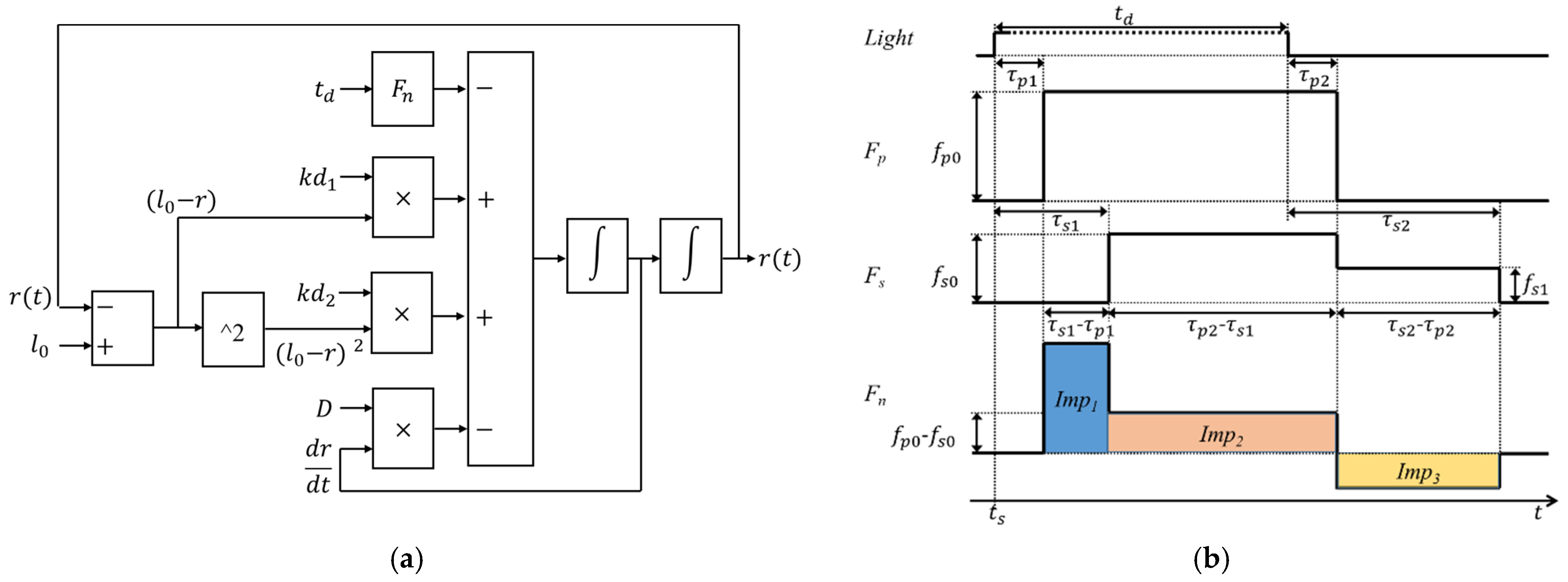
2.1. Pupillary Light Reflex Inherent Model Construction
2.2. Pupillary Light Reflex Response Experiment
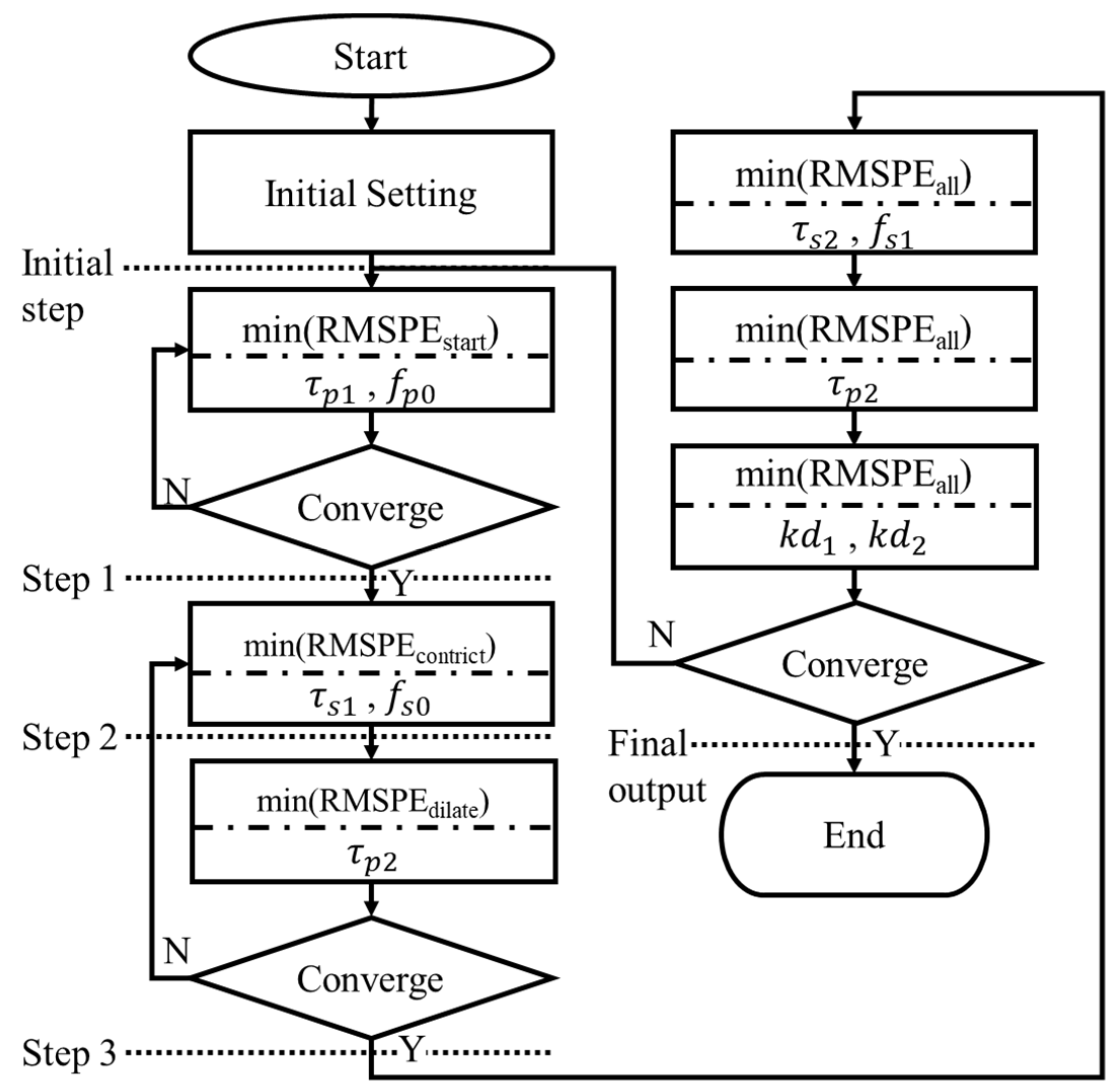
2.3. Structure Determination and Parameter Estimation of PLR Inherent Model
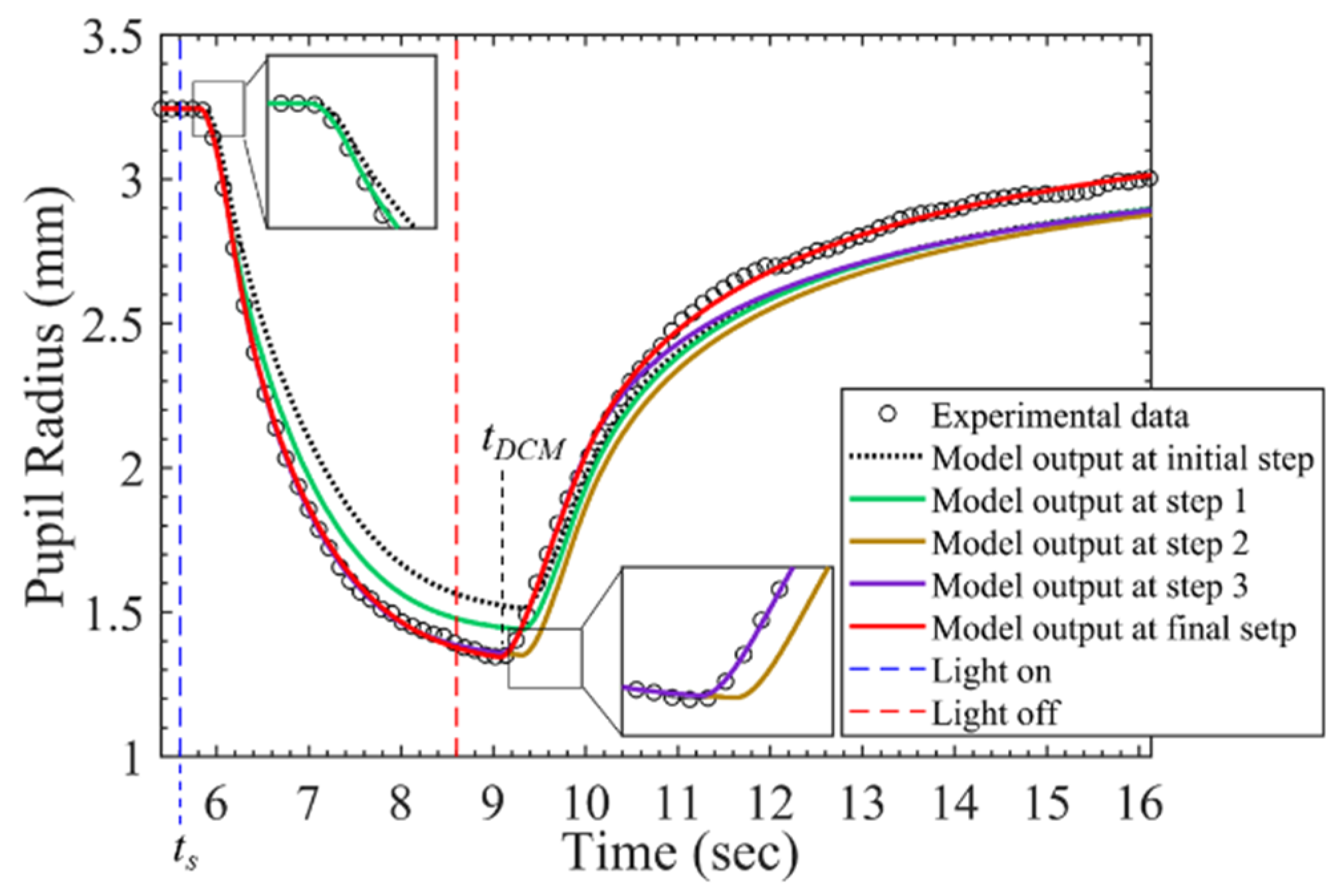
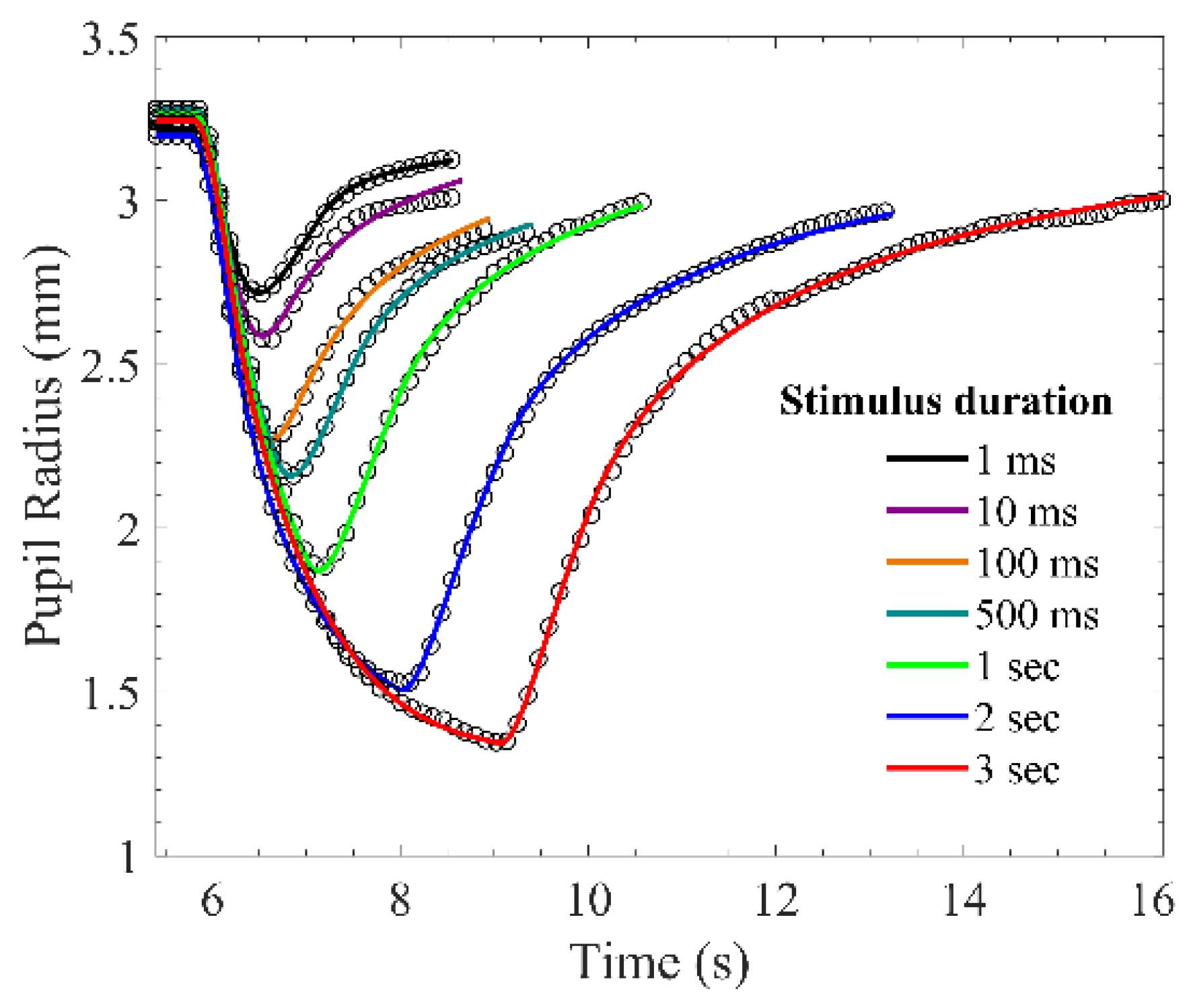
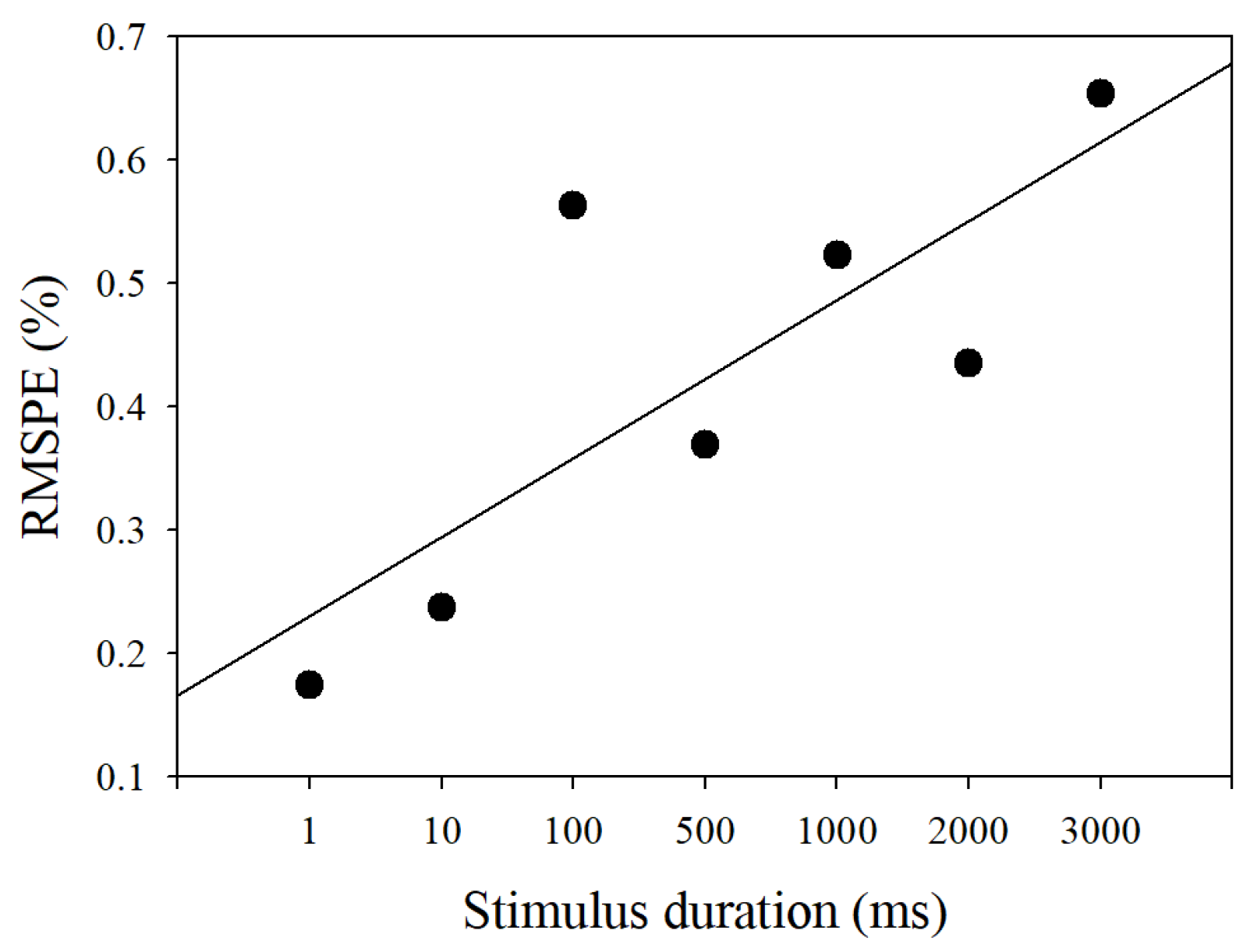
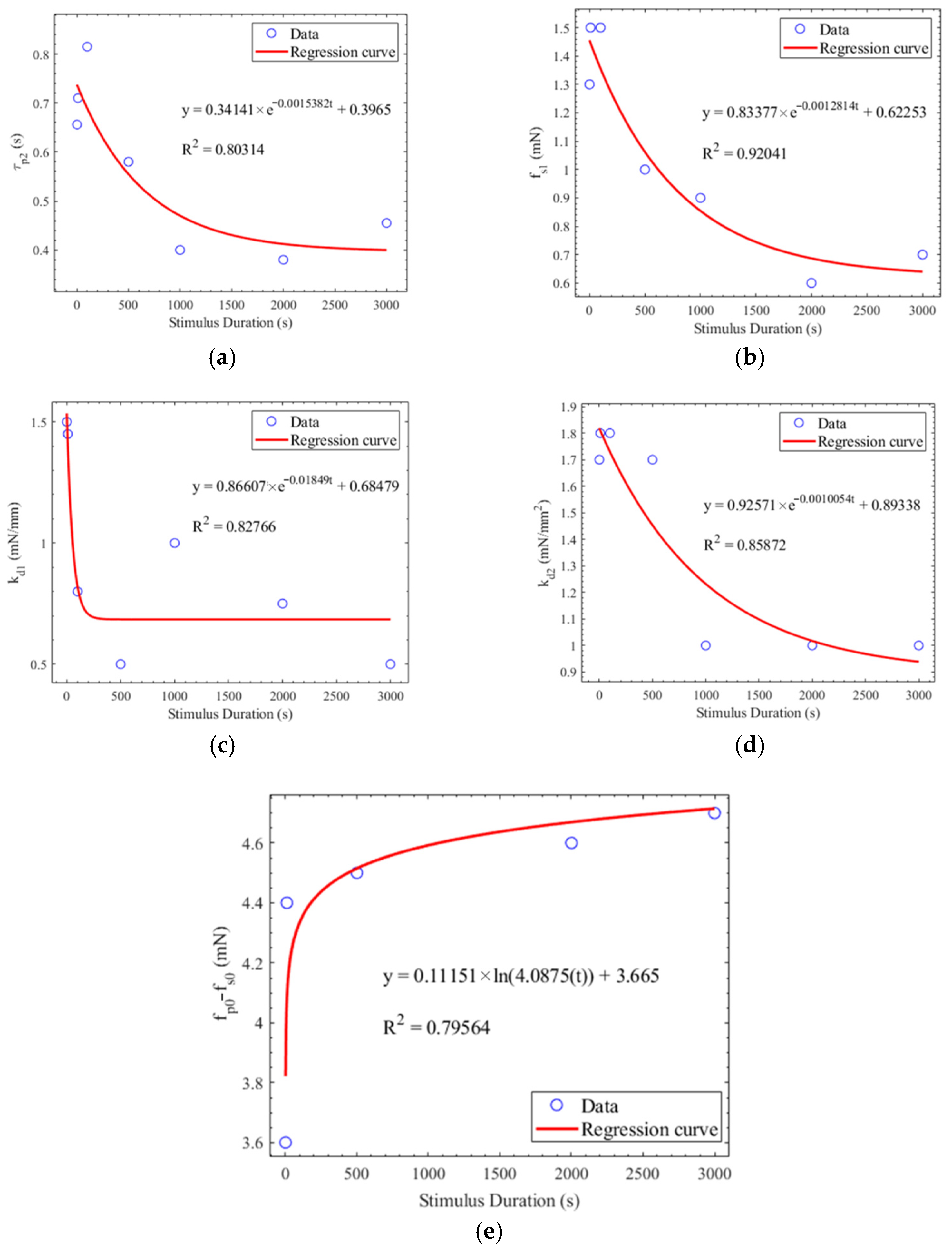
2.4. Validation of PLR Inherent Model
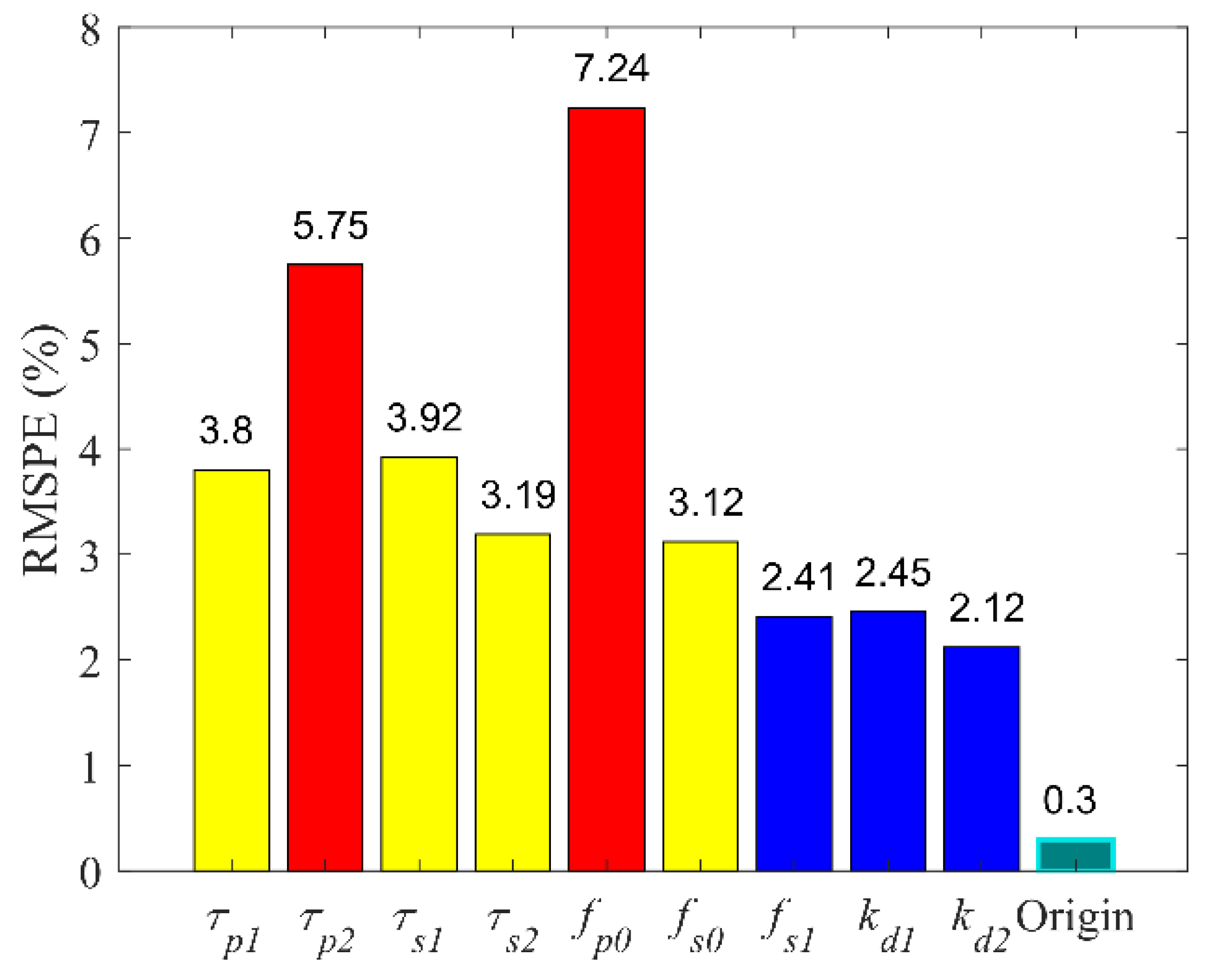
2.5. Sensitivity Analysis of PLR Inherent Model
3. Autonomic Neural Transmission Analysis
3.1. Material and Experiment
3.2. Coherence between Direct Response and the Consensual Response of Pupillary Light Reflex
3.3. The Coherence of Pupillary Light Reflex between Four Light Stimuli
3.4. PLR Comparison between Healthy People and Those with DM
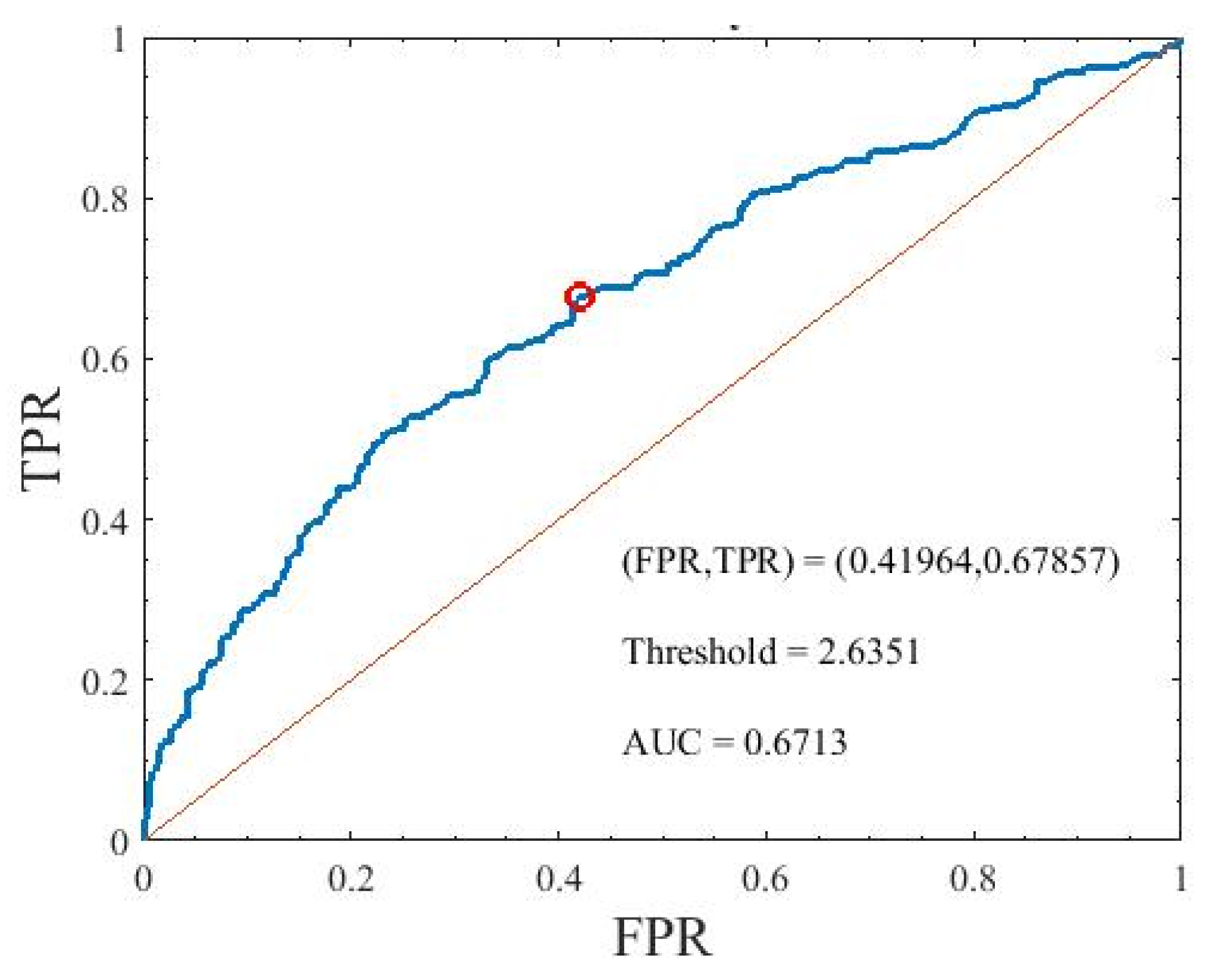
3.5. Receiver Operating Characteristic Analysis between Healthy People and Those with DM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vander, A.J.; Sherman, J.H.; Luciano, D.S. Human Physiology: The Mechanisms of Body Function; (no. 612 V228h); McGraw-Hill: New York, NY, USA, 1998. [Google Scholar]
- Zygmunt, A.; Stanczyk, J. Methods of evaluation of autonomic nervous system function. AMS 2010, 6, 11. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R.; Prineas, R.J.; Temprosa, M.; Zhang, Z.-M.; Uwaifo, G.; Molitch, M.E. The association among autonomic nervous system function, incident diabetes, and intervention arm in the Diabetes Prevention Program. Diabetes Care 2006, 29, 914–919. [Google Scholar] [CrossRef]
- Leal, G.; Neves, C.; Vieira, P.M. Pupillometry: Development of equipment for studies of autonomic nervous system. In Technological Innovation for Value Creation, International Federation for Information Processing Advances in Information and Communication Technology 2012; Springer: Berlin/Heidelberg, Germany, 2006; Volume 372, pp. 553–562. [Google Scholar]
- Barbur, J.L. Learning from the Pupil: Studies of Basic Mechanisms and Clinical Application; The Visual Neurosciences; Chalupa, L.M., Werner, J.S., Eds.; MIT Press: Cambridge, MA, USA, 2004; pp. 641–656. [Google Scholar]
- Surakka, J.; Ruutiainen, J.; Romberg, A.; Puukka, P.; Kronholm, E.; Karanko, H. Pupillary function in early multiple sclerosis. Clin. Auton. Res. 2008, 18, 150–154. [Google Scholar] [CrossRef]
- Mahmoudian, M.; Ebrahimi, S.A.; Kiani, Z. An image processing technique for diagnosis of Alzheimer’s disease. J. Res. Med. Sci. 2009, 14, 205–209. [Google Scholar] [PubMed]
- Chougule, P.S.; Najjar, R.P.; Finkelstein, M.T.; Kandiah, N.; Milea, D. Light-induced pupillary responses in Alzheimer’s disease. Front. Neurol. 2019, 10, 360. [Google Scholar] [CrossRef] [PubMed]
- Tatham, A.J.; Meira-Freitas, D.; Weinreb, R.N.; Zangwill, L.M.; Medeiros, F.A. Detecting glaucoma using automated pupillography. Ophthalmology 2014, 121, 1185–1193. [Google Scholar] [CrossRef]
- Chaidaroon, W.; Juwattanasomran, W. Colvard pupillometer measurement of scotopic pupil diameter in emmetropes and myopes. Jpn. J. Ophthalmol. 2002, 46, 640–644. [Google Scholar] [CrossRef]
- Zeng, T.; Shi, Y.T.; Peng, Y.T.; Chen, N.H.; Ma, Y.Y. Feature extraction and pupil size detection of pupillary light reflex in opiate addicts. Zool. Res. 2010, 31, 415–420. [Google Scholar]
- Narita, A.; Shirai, K.; Kubota, N.; Takayama, R.; Takahashi, Y.; Onuki, T.; Numakura, C.; Kato, M.; Hamada, Y.; Sakai, N.; et al. Abnormal pupillary light reflex with chromatic pupillometry in Gaucher disease. Ann. Clin. Transl. Neurol. 2014, 1, 135–140. [Google Scholar] [CrossRef]
- Schwingshandl, J.; Simpson, J.M.; Donaghue, K.; Bonney, M.-A.; Howard, N.J.; Silink, M. Pupillary abnormalities in type I diabetes occurring during adolescence: Comparisons with cardiovascular reflexes. Diabetes Care 1993, 16, 630–633. [Google Scholar] [CrossRef]
- Pittasch, D.; Lobmann, R.; Behrens-Baumann, W.; Lehnert, H. Pupil signs of sympathetic autonomic neuropathy in patients with type 1 diabetes. Diabetes Care 2002, 25, 1545–1550. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, Y.; Yu, Y.; Yao, K. Pupillary dysfunction in type 2 diabetes mellitus to refine the early diagnosis of diabetic autonomic neuropathy. Neuro Ophthalmol. 2009, 30, 17–21. [Google Scholar] [CrossRef]
- Ferrari, G.L.; Marques, J.L.; Gandhi, R.A.; Emery, C.J.; Tesfaye, S.; Heller, S.R.; Gamba, H.R. An approach to the assessment of diabetic neuropathy based on dynamic pupillometry. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007; pp. 557–560. [Google Scholar]
- Ferrari, G.L.; Marques, J.L.; Gandhi, R.A.; Heller, S.R.; Schneider, F.K.; Tesfaye, S.; Gamba, H.R. Using dynamic pupilometry as a simple screening tool to detect autonomic neuropathy in patients with diabetes: A pilot study. Biomed. Eng. OnLine 2010, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Bernabé-Ortiz, A.; Ticse, R.; Hernandez, A.; Huaylinos, Y.; Pinto, M.E.; Málaga, G.; Checkley, W.; Gilman, R.H.; Miranda, J.J.; et al. Type 2 diabetes and cardiac autonomic neuropathy screening using dynamic pupillometry. Diabetic Med. 2015, 32, 1470–1478. [Google Scholar] [CrossRef]
- Park, J.C.; Chen, Y.F.; Blair, N.P.; Chau, F.Y.; Lim, J.I.; Leiderman, Y.I.; McAnany, J. Pupillary responses in non-proliferative diabetic retinopathy. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Devan, S.; Jaisankar, D.; Swaminathan, G.; Pardhan, S.; Raman, R. Pupillary abnormalities with varying severity of diabetic retinopathy. Sci. Rep. 2018, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.L.; Chen, Y.Y.; Ouyang, Y.; Huang, T.W.; Tsuen, B.S.; Jeng, W.D.; Ou-Yang, M. Design and analysis of wearable pupillometer for autonomic neuropathy of diabetic patients. Appl. Opt. 2014, 53, H27–H34. [Google Scholar] [CrossRef]
- Smith, S.A.; Dewhirst, R.R. A simple diagnostic test for pupillary abnormality in diabetic autonomic neuropathy. Diabetic Med. 1986, 3, 38–41. [Google Scholar] [CrossRef]
- Smith, S.A.; Smith, S.E. Reduced pupillary light reflexes in diabetic autonomic neuropathy. Diabetologia 1983, 24, 330–332. [Google Scholar] [CrossRef]
- Yan, Y.J.; Tsai, Y.C.; Ko, M.L.; Lee, N.C.; Chiou, J.C.; Ou-Yang, M. Quantitative examination of early diabetes by light-emitting diodes light-induced pupillary light reflex. Rev. Sci. Instrum. 2021, 92, 014101. [Google Scholar] [CrossRef] [PubMed]
- Muppidi, S.; Adams-Huet, B.; Tajzoy, E.; Scribner, M.; Blazek, P.; Spaeth, E.B.; Frohman, E.; Davis, S.; Vernino, S. Dynamic pupillometry as an autonomic testing tool. Clin. Auton. Res. 2013, 23, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Stark, L.; Sherman, P.M. A servoanalytic study of consensual pupil reflex to light. J. Neurophysiol. 1957, 20, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Stark, L.; Baker, F. Stability and oscillations in a neurological servomechanism. J. Neurophysiol. 1959, 22, 156–164. [Google Scholar] [CrossRef]
- Stark, L.; Campbell, F.W.; Atwood, J. Pupil unrest: An example of noise in a biological servomechanism. Nature 1958, 182, 857–858. [Google Scholar] [CrossRef]
- Sun, F.; Krenz, W.C.; Stark, L. A systems model for the pupil size effect: I. Transient data. Biol. Cybern. 1985, 48, 101–108. [Google Scholar] [CrossRef]
- Krenz, W.C.; Stark, L. Systems model for pupil size effect. II. Feedback model. Biol. Cybern. 1985, 51, 391–397. [Google Scholar] [CrossRef]
- Privitera, C.M.; Stark, L. A binocular pupil model for simulation of relative afferent pupil defects and the swinging flashlight test. Biol. Cybern. 2006, 94, 215–224. [Google Scholar] [CrossRef]
- Pamplona, V.F.; Oliveira, M.M.; Baranoski, G.V.G. Photorealistic models for pupil light reflex and iridal pattern deformation. ACM Trans. Graph. 2009, 28, 1–12. [Google Scholar] [CrossRef]
- Moon, P.; Spencer, D.E. On the stiles-crawford effect. JOSA 1944, 34, 319–329. [Google Scholar] [CrossRef]
- Longtin, A.; Milton, J.G. Insight into the transfer function, gain, and oscillation onset for the pupil light reflex using nonlinear delay-differential equations. Biol. Cybern. 1989, 61, 51–58. [Google Scholar] [CrossRef]
- Longtin, A.; Milton, J.G. Modelling autonomous oscillations in the human pupil light reflex using nonlinear delay-differential equations. Bull. Math. Biol. 1989, 51, 605–624. [Google Scholar] [CrossRef] [PubMed]
- Usui, S.; Hirata, Y. Estimation of autonomic nervous activity using the inverse dynamic model of the pupil muscle plant. Ann. Biomed. Eng. 1995, 23, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Yao, G. Modeling transient pupillary light reflex induced by a short light flash. IEEE Transact. Biomed. Eng. 2011, 58, 36–42. [Google Scholar]
- Ljung, L. System Identification; Signal analysis and prediction; Springer: Berlin/Heidelberg, Germany, 1999; pp. 163–173. [Google Scholar]
- Ishikawa, S.; Bensaoula, T.; Uga, S.; Mukuno, K. Electron-microscopic study of iris nerves and muscles in diabetes. Ophthalmologica 1985, 191, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Güler, A.D.; Ecker, J.L.; Lall, G.S.; Haq, S.; Altimus, C.M.; Liao, H.W.; Barnard, A.R.; Cahill, H.; Badea, T.C.; Zhao, H.; et al. Melanopsin cells are the principal conduits for rod–cone input to non-image-forming vision. Nature 2008, 453, 102–105. [Google Scholar] [CrossRef]
- Berson, D.M. Strange vision: Ganglion cells as circadian photoreceptors. Trends Neurosci. 2003, 26, 314–320. [Google Scholar] [CrossRef]
- Kumar, S.; Zhuo, L. Quantitative analysis of pupillary light reflex by real-time autofluorescent imaging in a diabetic mouse model. Exp. Eye Res. 2011, 92, 164–172. [Google Scholar] [CrossRef]
- Adhikari, P.; Zele, A.J.; Feigl, B. The post-illumination pupil response (PIPR). Investig. Ophthalmol. Vis. Sci. 2015, 56, 3838–3849. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Initial Value | Unit | Lower Bound | Upper Bound | Step |
|---|---|---|---|---|---|
| 0.250 | s | 0.150 | 0.300 | 0.005 | |
| 1.250 | s | 0.200 | 1.250 | 0.005 | |
| 0.500 | s | 0.270 | 0.650 | 0.005 | |
| 1.300 | s | 1.200 | 2.000 | 0.005 | |
| 11.00 | mN | 8.000 | 14.000 | 0.100 | |
| 7.000 | mN | 4.000 | 15.000 | 0.100 | |
| 1.000 | mN | 0.100 | 1.500 | 0.100 | |
| 4.300 | g/s | … | … | … | |
| 1.000 | mN/mm | 0.500 | 1.500 | 0.050 | |
| 1.600 | mN/mm2 | 1.000 | 1.800 | 0.050 |
| Parameter | 1 ms | 10 ms | 100 ms | 500 ms | 1 s | 2 s | 3 s |
|---|---|---|---|---|---|---|---|
| (s) | 0.235 | 0.205 | 0.175 | 0.220 | 0.215 | 0.165 | 0.210 |
| (s) | 0.656 | 0.710 | 0.815 | 0.580 | 0.400 | 0.380 | 0.455 |
| (s) | 0.415 | 0.425 | 0.545 | 0.565 | 0.555 | 0.570 | 0.570 |
| (s) | 1.520 | 1.205 | 1.215 | 1.365 | 1.395 | 1.545 | 1.370 |
| (mN) | 10.900 | 11.1000 | 12.20 | 11.300 | 11.100 | 10.800 | 11.300 |
| (mN) | 7.300 | 6.700 | 9.700 | 6.800 | 5.800 | 6.200 | 6.600 |
| (mN) | 1.300 | 1.500 | 1.500 | 1.000 | 0.900 | 0.600 | 0.700 |
| () | 1.500 | 1.450 | 0.800 | 0.500 | 1.000 | 0.750 | 0.500 |
| () | 1.700 | 1.800 | 1.800 | 1.700 | 1.000 | 1.000 | 1.000 |
| (g/s) | 4.300 | 4.300 | 4.300 | 4.300 | 4.300 | 4.300 | 4.300 |
| Parameter | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0.204 | 0.571 | 0.521 | 1.374 | 11.243 | 7.014 | 1.071 | 0.929 | 1.429 | 3.245 | |
| 0.025 | 0.166 | 0.069 | 0.132 | 0.461 | 1.275 | 0.368 | 0.412 | 0.403 | 0.029 | |
| 0.123 | 0.291 | 0.133 | 0.096 | 0.041 | 0.182 | 0.344 | 0.444 | 0.282 | 0.009 |
| Healthy Participants | Participants with DM | |
|---|---|---|
| Male: Female | 26/16 | 29/13 |
| Age (years old) | 37 ± 17 | 47 ± 14 |
| Original HbA1c (years old) | <6 | 8.9 ± 2.9 |
| Current HbA1c (years old) | <6 | 7.6 ± 2.1 |
| Duration (years old) | … | 7.1 ± 7 |
| Diabetic type | … | Type I and 2 |
| Parameters | Healthy Participant 1 | Healthy Participant 2 | ||||
|---|---|---|---|---|---|---|
| Right | Left | PE (%) | Right | Left | PE (%) | |
| τp1 * | 0.19 | 0.200 | 5.263 | 0.230 | 0.245 | 6.522 |
| τp2 * | 0.475 | 0.500 | 5.263 | 0.595 | 0.630 | 5.882 |
| τs1 * | 0.360 | 0.375 | 4.167 | 0.395 | 0.420 | 6.329 |
| τs2 | 1.215 | 1.210 | −0.412 | 1.195 | 1.195 | 0.000 |
| fp0 | 11.400 | 11.300 | −0.877 | 10.800 | 10.700 | −0.926 |
| fs0 * | 5.000 | 5.300 | 6.000 | 6.600 | 7.100 | 7.576 |
| fs1 | 1.500 | 1.500 | 0.000 | 1.500 | 1.500 | 0.000 |
| kd1 | 1.500 | 1.500 | 0.000 | 1.500 | 1.500 | 0.000 |
| kd2 | 1.800 | 1.800 | 0.000 | 1.800 | 1.800 | 0.000 |
| l0 | 2.534 | 2.681 | 5.773 | 2.706 | 2.784 | 2.89 |
| Parameter | W | R | G | B | Mean | Std | Cv |
|---|---|---|---|---|---|---|---|
| τp1 | 0.224 | 0.201 | 0.197 | 0.190 | 0.203 | 0.015 | 0.0725 |
| τp2 | 0.716 | 0.787 | 0.795 | 0.807 | 0.776 | 0.041 | 0.0528 |
| τs1 | 0.416 | 0.418 | 0.428 | 0.423 | 0.421 | 0.005 | 0.0128 |
| τs2 | 1.375 | 1.420 | 1.358 | 1.403 | 1.389 | 0.028 | 0.0200 |
| fp0 | 10.036 | 10.564 | 10.671 | 10.707 | 10.495 | 0.312 | 0.0297 |
| fs0 | 7.536 | 7.876 | 7.831 | 7.598 | 7.71 | 0.168 | 0.0218 |
| fs1 | 1.319 | 1.224 | 1.281 | 1.226 | 1.263 | 0.046 | 0.0364 |
| kd1 | 1.277 | 1.292 | 1.260 | 1.224 | 1.263 | 0.029 | 0.0232 |
| kd2 | 1.657 | 1.635 | 1.690 | 1.664 | 1.662 | 0.023 | 0.0136 |
| l0 | 3.098 | 3.070 | 3.038 | 2.991 | 3.049 | 0.046 | 0.0151 |
| Parameters | Healthy Participants (336 Samples) | Participants with DM (336 Samples) | p-Value | |||
|---|---|---|---|---|---|---|
| Mean | STD | Mean | STD | |||
| τp1 | 0.205 | 0.035 | 0.208 | 0.038 | 0.2842 | |
| τp2 | 0.779 | 0.142 | 0.772 | 0.14 | 0.5357 | |
| τs1 | 0.423 | 0.045 | 0.439 | 0.05 | ** | |
| τs2 | 1.391 | 0.228 | 1.397 | 0.24 | 0.7035 | |
| fp0 | 10.573 | 1.193 | 10.549 | 1.189 | 0.7881 | |
| fs0 | 7.745 | 1.547 | 7.991 | 1.525 | 0.0384 | * |
| fs1 | 1.264 | 0.304 | 1.279 | 0.282 | 0.4946 | |
| kd1 | 1.251 | 0.257 | 1.195 | 0.286 | 0.0081 | * |
| kd2 | 1.656 | 0.217 | 1.676 | 0.208 | 0.2276 | |
| l0′ | 3.051 | 0.392 | 2.783 | 0.381 | ** | |
| τp2-τs1 | 0.356 | 0.131 | 0.333 | 0.129 | 0.0240 | * |
| fp0-fs0 | 2.828 | 1.21 | 2.558 | 1.258 | 0.0046 | * |
| τs1-τp1 | 0.219 | 0.053 | 0.232 | 0.066 | 0.0051 | * |
| τs2-τp2 | 0.611 | 0.231 | 0.625 | 0.229 | 0.4436 | |
| Imp1 | 2.333 | 0.723 | 2.481 | 0.844 | 0.0150 | * |
| Imp2 | 0.964 | 0.481 | 0.79 | 0.401 | ** | |
| Imp3 | 0.749 | 0.266 | 0.766 | 0.247 | 0.3904 | |
| l0′ * kd1 | 3.799 | 0.846 | 3.305 | 0.835 | ** | |
| τp1 | 0.205 | 0.035 | 0.208 | 0.038 | 0.2842 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, Y.-J.; Chen, C.-N.; Ou-Yang, M. Using System Identification to Construct an Inherent Model of Pupillary Light Reflex to Explore Diabetic Neuropathy. Brain Sci. 2021, 11, 852. https://doi.org/10.3390/brainsci11070852
Yan Y-J, Chen C-N, Ou-Yang M. Using System Identification to Construct an Inherent Model of Pupillary Light Reflex to Explore Diabetic Neuropathy. Brain Sciences. 2021; 11(7):852. https://doi.org/10.3390/brainsci11070852
Chicago/Turabian StyleYan, Yung-Jhe, Chien-Nan Chen, and Mang Ou-Yang. 2021. "Using System Identification to Construct an Inherent Model of Pupillary Light Reflex to Explore Diabetic Neuropathy" Brain Sciences 11, no. 7: 852. https://doi.org/10.3390/brainsci11070852
APA StyleYan, Y.-J., Chen, C.-N., & Ou-Yang, M. (2021). Using System Identification to Construct an Inherent Model of Pupillary Light Reflex to Explore Diabetic Neuropathy. Brain Sciences, 11(7), 852. https://doi.org/10.3390/brainsci11070852