
Effects of Early Rehydration on Brain Perfusion and Infarct Core after Middle Cerebral Artery Occlusion in Rats

Abstract
1. Introduction
2. Materials and Methods
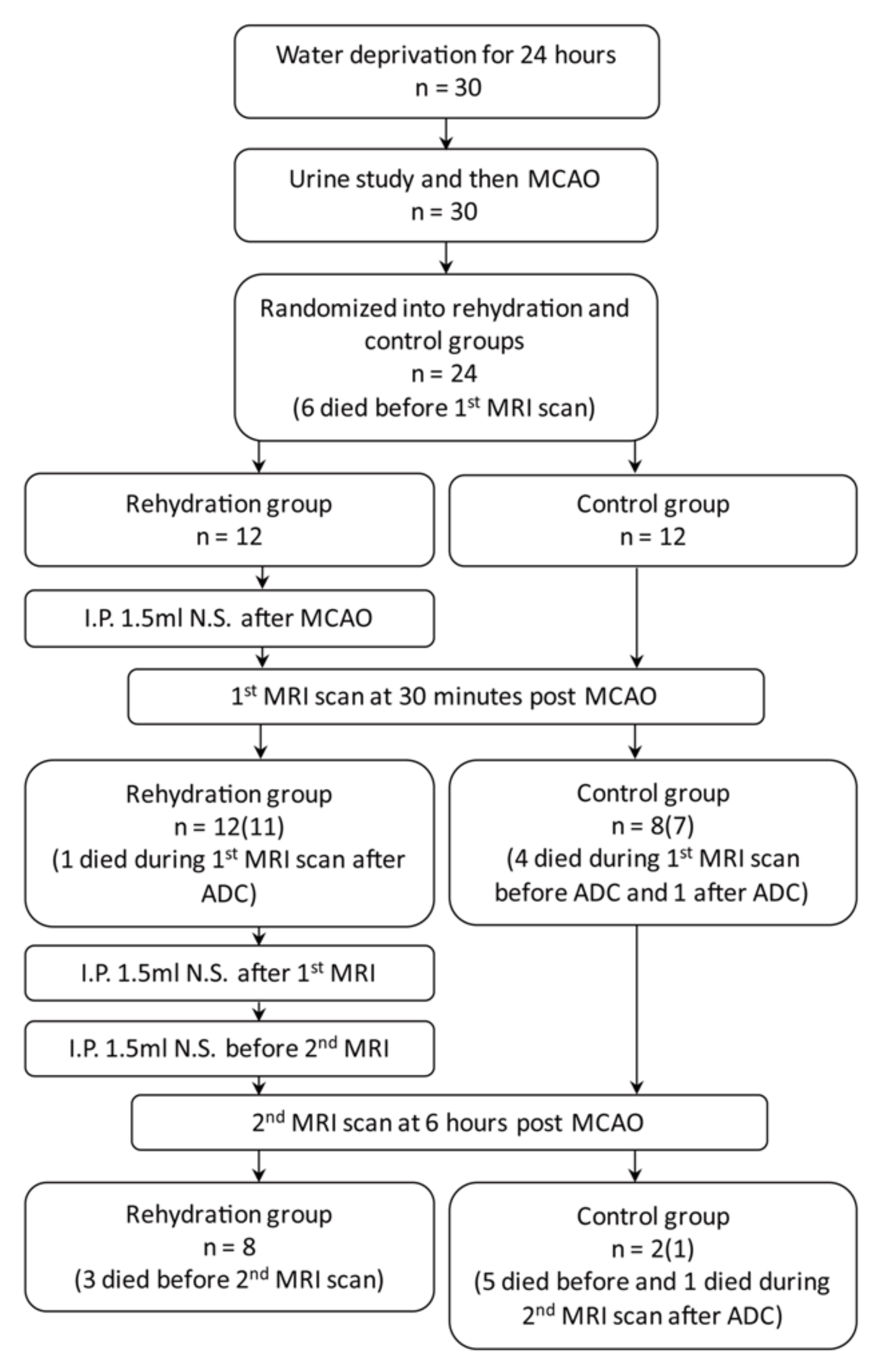
2.1. Dehydration and Ischemic Stroke Rat Model
2.2. MRI Acquisition and Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowat, A.; Graham, C.; Dennis, M. Dehydration in hospital-admitted stroke patients: Detection, frequency, and association. Stroke 2012, 43, 857–859. [Google Scholar] [CrossRef]
- Bahouth, M.N.; Gottesman, R.F.; Szanton, S.L. Primary ‘dehydration’ and acute stroke: A systematic research review. J. Neurol. 2018. [CrossRef]
- Bahouth, M.N.; Gaddis, A.; Hillis, A.E.; Gottesman, R.F. Pilot study of volume contracted state and hospital outcome after stroke. Neurol. Clin. Pract. 2018, 8, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Vicente, E.; Guisado-Alonso, D.; Delgado-Mederos, R.; Camps-Renom, P.; Prats-Sanchez, L.; Martinez-Domeno, A.; Marti-Fabregas, J. Frequency, Risk Factors, and Prognosis of Dehydration in Acute Stroke. Front. Neurol. 2019, 10, 305. [Google Scholar] [CrossRef] [PubMed]
- Hillis, A.E.; Ulatowski, J.A.; Barker, P.B.; Torbey, M.; Ziai, W.; Beauchamp, N.J.; Oh, S.; Wityk, R.J. A pilot randomized trial of induced blood pressure elevation: Effects on function and focal perfusion in acute and subacute stroke. Cerebrovasc. Dis. 2003. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.H.; Yang, J.L.; Lee, I.N.; Yang, J.T.; Lin, L.C.; Huang, Y.C.; Yeh, M.Y.; Weng, H.H.; Su, C.H. Effects of dehydration on brain perfusion and infarct core after acute middle cerebral artery occlusion in rats: Evidence from high-field magnetic resonance imaging. Front. Neurol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.W.; Huang, Y.C.; Lin, L.C.; Yang, J.T.; Weng, H.H.; Tsai, Y.H.; Lee, T.H. Effect of dehydration on the development of collaterals in acute middle cerebral artery occlusion. Eur. J. Neurol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Suwanwela, N.C.; Chutinet, A.; Mayotarn, S.; Thanapiyachaikul, R.; Chaisinanunkul, N.; Asawavichienjinda, T.; Muengtaweepongsa, S.; Nilanont, Y.; Samajarn, J.; Watcharasaksilp, K.; et al. A randomized controlled study of intravenous fluid in acute ischemic stroke. Clin. Neurol. Neurosurg. 2017, 161, 98–103. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P.; Bruno, A.; Connors, J.J.B.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Yang, J.T.; Huang, Y.C.; Tsai, Y.H.; Lee, M.H.; Lee, M.; Hsiao, C.T.; Hsiao, K.Y.; Lin, L.C. Favorable outcome of blood urea nitrogen/creatinine–based hydration therapy 3 months after acute ischemic stroke. Am. J. Emerg. Med. 2016. [Google Scholar] [CrossRef]
- Mücke, S.; Grotemeyer, K.H.; Stahlhut, L.; Husstedt, I.W.; Evers, S. The influence of fluid intake on stroke recurrence - A prospective study. J. Neurol. Sci. 2012. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.P.L.; Rowley, H. a Diffusion weighted magnetic resonance imaging in stroke. Eur. J. Radiol. 2003, 45, 185–194. [Google Scholar] [CrossRef]
- Wu, L.; Wu, W.; Tali, E.T.; Yuh, W.T. Oligemia, Penumbra, Infarction: Understanding Hypoperfusion with Neuroimaging. Neuroimaging Clin. N. Am. 2018, 28, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Bekkevold, C.M.; Robertson, K.L.; Reinhard, M.K.; Battles, A.H.; Rowland, N.E. Dehydration Parameters and Standards for Laboratory Mice. J. Am. Assoc. Lab. Anim. Sci. 2013, 52, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Morris, M. Neurohypophyseal response to dehydration in the spontaneously hypertensive rat. Hypertens 1982, 4, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Hsu, C.Y.; Hogan, E.L.; Maricq, H.; Balentine, J.D. A model of focal ischemic stroke in the rat: Reproducible extensive cortical infarction. Stroke 1986. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.C.; Der Lee, J.; Hung, Y.C.; Chang, C.H.; Yang, J.T. Bun/creatinine ratio-based hydration for preventing stroke-in-evolution after acute ischemic stroke. Am. J. Emerg. Med. 2014, 32, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.C.; Shih, H.M.; Lin, L.C. Preliminary Prospective Study to Assess the Effect of Early Blood Urea Nitrogen/Creatinine Ratio-Based Hydration Therapy on Poststroke Infection Rate and Length of Stay in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 2720–2727. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, A.; Sankaralingam, S.; Dundas, R.; Swaminathan, R.; Wolfe, C.D.; Rudd, A.G. Influence of raised plasma osmolality on clinical outcome after acute stroke. Stroke. 2000, 31, 2043–2048. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Tsai, Y.Y.; Hsiao, K.Y.; Tsai, Y.H.; Lee, M.H.; Huang, Y.C.; Lee, M.; Yang, J.T.; Hsiao, C.T.; Lin, L.C. Urine-Specific Gravity-Based Hydration Prevents Stroke in Evolution in Patients with Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 1885–1891. [Google Scholar] [CrossRef]
- Lourbopoulos, A.; Mamrak, U.; Roth, S.; Balbi, M.; Shrouder, J.; Liesz, A.; Hellal, F.; Plesnila, N. Inadequate food and water intake determine mortality following stroke in mice. J. Cereb. Blood Flow Metab. 2017, 37, 2084–2097. [Google Scholar] [CrossRef] [PubMed]
- González-Alonso, J.; Mora-Rodríguez, R.; Below, P.R.; Coyle, E.F. Dehydration reduces cardiac output and increases systemic and cutaneous vascular resistance during exercise. J. Appl. Physiol. 1995, 79, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Saikurai, M.; Hamada, K.; Matsumoto, K.; Yanagisawa, K.; Kikuchi, N.; Morimoto, T.; Greenleaf, J.E. Plasma volume and blood viscosity during 4 h sitting in a dry environment: Effect of prehydration. Aviat. Sp. Environ. Med. 2004, 75, 500–504. [Google Scholar]
- Kirkebo, A.; Tyssebotn, I. Effect of dehydration on renal blood flow in dog. Acta Physiol. Scand. 1977, 101, 257–263. [Google Scholar] [CrossRef]
- González-Alonso, J.; Calbet, J.A.; Nielsen, B. Muscle blood flow is reduced with dehydration during prolonged exercise in humans. J. Physiol. 1998, 513 (Pt 3), 895–905. [Google Scholar] [CrossRef]
- Baker, M.A. Cardiovascular and respiratory responses to heat in dehydrated dogs. Am. J. Physiol. 1984, 246, R369–R374. [Google Scholar] [CrossRef]
- Seker, F.; Potreck, A.; Möhlenbruch, M.; Bendszus, M.; Pham, M. Comparison of four different collateral scores in acute ischemic stroke by CT angiography. J. Neurointerv. Surg. 2015, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bivard, A.; Spratt, N.; Levi, C.; Parsons, M. Perfusion computer tomography: Imaging and clinical validation in acute ischaemic stroke. Brain 2011. [Google Scholar] [CrossRef]
- Muizelaar, J.P.; Wei, E.P.; Kontos, H.A.; Becker, D.P. Cerebral blood flow is regulated by changes in blood pressure and in blood viscosity alike. Stroke 1986, 17, 44–48. [Google Scholar] [CrossRef]
- Moralez, G.; Romero, S.A.; Rickards, C.A.; Ryan, K.L.; Convertino, V.A.; Cooke, W.H. Effects of dehydration on cerebrovascular control during standing after heavy resistance exercise. J. Appl. Physiol. 2012, 112, 1875–1883. [Google Scholar] [CrossRef]
- Perry, B.G.; Bear, T.L.K.; Lucas, S.J.E.; Mündel, T. Mild dehydration modifies the cerebrovascular response to the cold pressor test. Exp. Physiol. 2016, 101, 135–142. [Google Scholar] [CrossRef]
- Johnson, J.M.; Lev, M.H. Computed tomography in acute stroke. In The Stroke Book, 2nd ed.; Selim, M.H., Torbey, M.T., Eds.; Cambridge University Press: Cambridge, UK, 2013; pp. 93–123. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALL | Control Group | Rehydration Group | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Urine sodium (mg/dL) | 303.35 | 58.91 | 308.13 | 44.01 | 300.17 | 68.81 | 0.678 |
| Urine osmolarity (mosm/KgH2O) | 2776.15 | 513.24 | 2493.75 | 291.47 | 2964.42 | 551.60 | 0.016 * |
| Urine specific gravity | 1.07 | 0.02 | 1.07 | 0.01 | 1.07 | 0.02 | 0.025 * |
| MRI results at 30 min post MCAO | |||||||
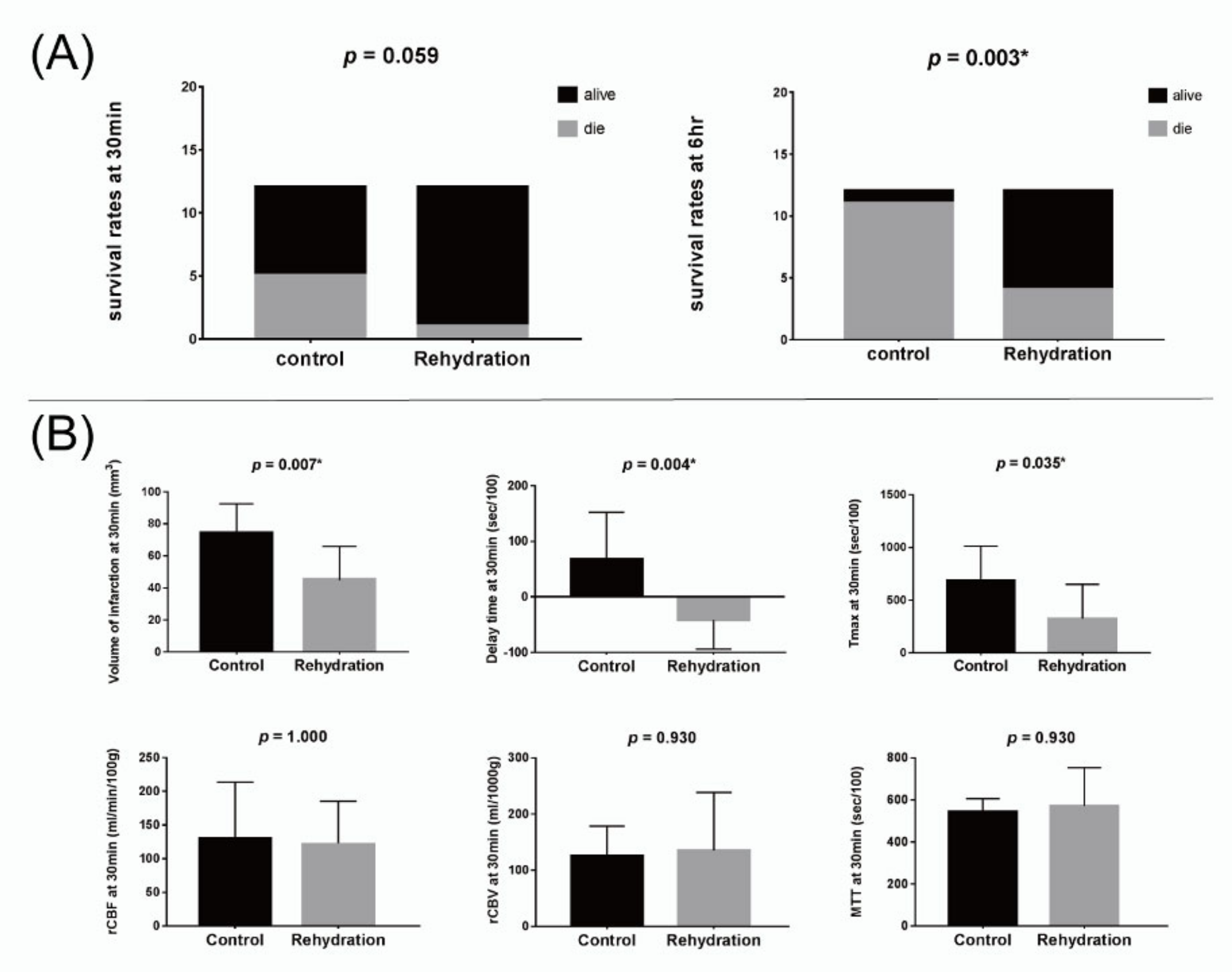
| Volume of infarction (mL) | 56.37 | 24.48 | 73.72 | 18.73 | 44.80 | 21.15 | 0.007 * |
| Infarct side | |||||||
| rCBF (mL/min/100 g) | 126.51 | 68.25 | 131.82 | 81.84 | 123.14 | 62.19 | 1.000 |
| rCBV (mL/1000 g) | 131.62 | 85.37 | 125.52 | 53.12 | 135.50 | 103.21 | 0.930 |
| Mean transit time (MTT) (sec/100) | 560.61 | 145.11 | 543.50 | 63.05 | 571.49 | 181.88 | 0.930 |
| Delay time (sec/100) | 0.99 | 84.60 | 68.39 | 84.28 | −41.90 | 51.98 | 0.004 * |
| Tmax (sec/100) | 464.95 | 365.18 | 685.72 | 329.14 | 324.46 | 325.39 | 0.035 * |
| Normal side | |||||||
| rCBF (mL/min/100 g) | 190.57 | 141.81 | 244.69 | 173.47 | 156.13 | 113.04 | 0.211 |
| rCBV (mL/1000 g) | 192.36 | 137.98 | 211.10 | 94.10 | 180.44 | 163.25 | 0.151 |
| MTT (sec/100) | 645.80 | 144.83 | 602.72 | 178.69 | 673.22 | 119.90 | 0.479 |
| Delay time (sec/100) | −59.56 | 88.72 | −21.55 | 117.01 | −83.74 | 59.25 | 0.425 |
| Tmax (sec/100) | 226.89 | 152.15 | 279.86 | 177.59 | 193.18 | 131.21 | 0.211 |
| MRI results at 6 h post MCAO | |||||||
| Volume of infarction (mm3) | 82.83 | 48.83 | 147.12 | 35.74 | 66.76 | 37.52 | 0.089 |
| Infarct side | |||||||
| rCBF (mL/min/100 g) | 117.66 | 92.29 | 40.78 | 127.26 | 93.72 | 0.444 | |
| rCBV (mL/1000 g) | 129.92 | 117.08 | 36.12 | 141.65 | 119.38 | 0.444 | |
| MTT (sec/100) | 515.75 | 117.84 | 392.44 | 531.16 | 115.87 | 0.444 | |
| Delay time (sec/100) | 6.80 | 47.99 | −1.82 | 7.88 | 51.19 | 1.000 | |
| Tmax (sec/100) | 500.85 | 318.88 | 295.21 | 526.55 | 330.77 | 0.444 | |
| Normal side | |||||||
| rCBF (mL/min/100 g) | 139.78 | 47.13 | 116.11 | 142.74 | 49.48 | 0.667 | |
| rCBV (ML/1000 g) | 148.81 | 61.39 | 92.61 | 155.83 | 61.64 | 0.444 | |
| MTT (sec/100) | 598.91 | 110.14 | 540.36 | 606.23 | 115.38 | 0.444 | |
| Delay time (sec/100) | −41.03 | 64.50 | −95.24 | −34.25 | 65.44 | 0.667 | |
| Tmax (sec/100) | 341.72 | 168.36 | 130.54 | 368.12 | 158.83 | 0.222 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-H.; Su, C.-H.; Lee, I.-N.; Yang, J.-T.; Lin, L.-C.; Huang, Y.-C.; Yang, J.-L. Effects of Early Rehydration on Brain Perfusion and Infarct Core after Middle Cerebral Artery Occlusion in Rats. Brain Sci. 2021, 11, 439. https://doi.org/10.3390/brainsci11040439
Tsai Y-H, Su C-H, Lee I-N, Yang J-T, Lin L-C, Huang Y-C, Yang J-L. Effects of Early Rehydration on Brain Perfusion and Infarct Core after Middle Cerebral Artery Occlusion in Rats. Brain Sciences. 2021; 11(4):439. https://doi.org/10.3390/brainsci11040439
Chicago/Turabian StyleTsai, Yuan-Hsiung, Chia-Hao Su, I-Neng Lee, Jen-Tsung Yang, Leng-Chieh Lin, Yen-Chu Huang, and Jenq-Lin Yang. 2021. "Effects of Early Rehydration on Brain Perfusion and Infarct Core after Middle Cerebral Artery Occlusion in Rats" Brain Sciences 11, no. 4: 439. https://doi.org/10.3390/brainsci11040439
APA StyleTsai, Y.-H., Su, C.-H., Lee, I.-N., Yang, J.-T., Lin, L.-C., Huang, Y.-C., & Yang, J.-L. (2021). Effects of Early Rehydration on Brain Perfusion and Infarct Core after Middle Cerebral Artery Occlusion in Rats. Brain Sciences, 11(4), 439. https://doi.org/10.3390/brainsci11040439