
Is an Oral Health Status a Predictor of Functional Improvement in Ischemic Stroke Patients Undergoing Comprehensive Rehabilitation Treatment?


 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Material and Methods
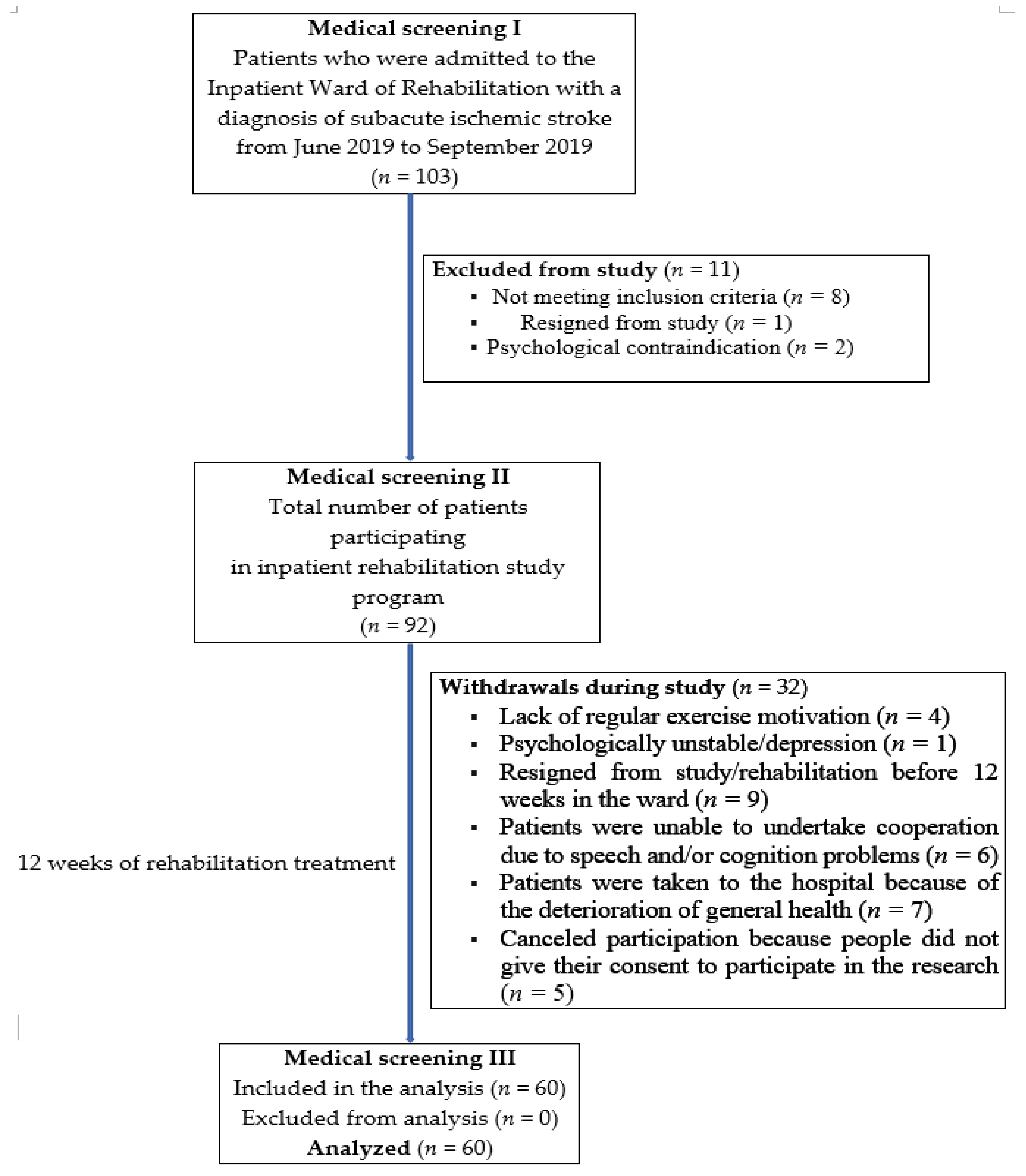
2.1. Study Design
2.2. Study Criteria
2.3. Assessment Schedule
2.4. Rehabilitation Intervention
2.5. Measurements
2.5.1. General Medical Information
2.5.2. Oral Examination
2.5.3. Functional Assessment
Activities of Daily Living
Balance Assessment
Assessment of Functional Independence
Cognitive Function Measurement
2.6. Statistical Analysis
3. Results
3.1. Study Patients
3.2. Analysis of Patient’s Oral Health Status during the Study Time
3.3. Analysis of Changes in Patient’s Functioning during the Study Time
3.4. Correlations between Functional Assessment and Oral Health Status
3.5. Multivariate Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sen, S.; Giamberardino, L.D.; Moss, K.; Morelli, T.; Rosamond, W.D.; Gottesman, R.F.; Beck, J.; Offenbacher, S. Periodontal Disease, Regular Dental Care Use, and Incident Ischemic Stroke. Stroke 2018, 49, 355–362. [Google Scholar] [CrossRef]
- Lee, H.J.; Choi, E.K.; Park, J.B.; Han, K.D.; Oh, S. Tooth Loss Predicts Myocardial Infarction, Heart Failure, Stroke, and Death. J. Dent. Res. 2019, 98, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Murakami, T.; Yoshimura, O.; Akagawa, Y. The evaluation of oral health in stroke patients. Gerodontology 2012, 29, e489–e493. [Google Scholar] [CrossRef] [PubMed]
- Meurman, J.H. A Role for Oral Health Personnel in Stroke Prevention. Compend. Contin. Educ. Dent. 2017, 38 (Suppl. 8), 26–28. [Google Scholar] [PubMed]
- Dietrich, T.; Webb, I.; Stenhouse, L.; Pattni, A.; Ready, D.; Wanyonyi, K.L.; White, S.; Gallagher, J.E. Evidence summary: The relationship between oral and cardiovascular disease. Br. Dent. J. 2017, 222, 381–385. [Google Scholar] [CrossRef]
- Daly, B.; Thompsell, A.; Sharpling, J.; Rooney, Y.M.; Hillman, L.; Wanyonyi, K.L.; White, S.; Gallagher, J.E. Evidence summary: The relationship between oral health and dementia. Br. Dent. J. 2018, 223, 846–853. [Google Scholar] [CrossRef]
- Zoellner, H. Dental infection and vascular disease. Semin. Thromb Hemost. 2011, 37, 181–192. [Google Scholar] [CrossRef]
- Lafon, A.; Pereira, B.; Dufour, T.; Rigouby, V.; Giroud, M.; Béjot, Y.; Tubert-Jeannin, S. Peridontal disease and stroke: A met-analysis of cohort studies. Eur. J. Neurol. 2014, 21, 1155–1161. [Google Scholar] [CrossRef]
- Fagundes, N.C.F.; Almeida, A.P.C.P.S.C.; Vilhena, K.F.B.; Magno, M.B.; Maia, L.C.; Lima, R.R. Periodontitis as a risk factor for stroke: A systematic review and meta-analysis. Vasc. Health Risk Manag. 2019, 15, 519–532. [Google Scholar] [CrossRef]
- Zeng, L.N.; Rao, W.W.; Luo, S.H.; Zhang, Q.E.; Hall, B.J.; Ungvari, G.S.; Chen, L.G.; Xiang, Y.T. Oral health in patients with stroke: A meta-analysis of comparative studies. Top Stroke Rehabil. 2020, 27, 75–80. [Google Scholar] [CrossRef]
- Dai, R.; Lam, O.L.; Lo, E.C.; Li, L.S.; Wen, Y.; McGrath, C. A systematic review and meta-analysis of clinical, microbiological, and behavioural aspects of oral health among patients with stroke. J. Dent. 2015, 43, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Ajwani, S.; Jayanti, S.; Burkolter, N.; Anderson, C.; Bhole, S.; Itaoui, R.; George, A. Integrated oral health care for stroke patients—A scoping review. J. Clin. Nurs. 2017, 26, 891–901. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y.; Shimazu, S.; Jeong, S. Impaired oral health status on admission is associated with poor clinical outcomes in post-acute inpatients: A prospective cohort study. Clin. Nutr. 2019, 38, 2677–2683. [Google Scholar] [CrossRef]
- Kim, H.T.; Park, J.B.; Lee, W.C.; Kim, Y.J.; Lee, Y. Differences in the oral health status and oral hygiene practices according to the extent of post-stroke sequelae. J. Oral Rehabil. 2018, 45, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Roman, N.; Miclaus, R.; Repanovici, A.; Nicolau, C. Equal Opportunities for Stroke Survivors’ Rehabilitation: A Study on the Validity of the Upper Extremity Fugl-Meyer Assessment Scale Translated and Adapted into Romanian. Medicina 2020, 56, 409. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Villani, E.R.; Grande, G.; Giovannini, S.; Cipriani, M.C.; Gravina, E.M.; Bernabei, R.; Onder, G. Association of Polypharmacy with 1-Year Trajectories of Cognitive and Physical Function in Nursing Home Residents: Results From a Multicenter European Study. J. Am. Med. Dir. Assoc. 2018, 19, 710–713. [Google Scholar] [CrossRef]
- Zhu, J.; Li, X.; Zhu, F.; Chen, L.; Zhang, C.; McGrath, C.; He, F.; Xiao, Y.; Jin, L. Multiple tooth loos is associated with vascular cognitive impairment in subjects with acute ischemic stroke. J. Periodontal. Res. 2015, 50, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Scholten, I. An oral hygiene protocol improves oral health for patients in inpatient stroke rehabilitation. Gerodontology 2018, 35, 18–24. [Google Scholar] [CrossRef]
- Giovannini, S.; Onder, G.; Leeuwenburgh, C.; Carter, C.; Marzetti, E.; Russo, A.; Capoluongo, E.; Pahor, M.; Bernabei, R.; Landi, F. Myeloperoxidase levels and mortality in frail community-living elderly individuals. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 369–376. [Google Scholar] [CrossRef]
- Giovannini, S.; Onder, G.; Lattanzio, F.; Bustacchini, S.; Di Stefano, G.; Moresi, R.; Russo, A.; Bernabei, R.; Landi, F. Selenium Concentrations and Mortality among Community-Dwelling Older Adults: Results from IlSIRENTE Study. J. Nutr. Health Aging 2018, 22, 608–612. [Google Scholar] [CrossRef]
- Padua, I.; Imbimbo, I.; Aprile, I.; Loreti, C.; Germanotta, M.; Coraci, D.; Piccinini, G.; Pazzaglia, C.; Santilli, C.; Cruciani, A.; et al. Cognitive reserve as a useful variable to address robotic or conventional upper limb rehabilitation treatment after stroke: A multicentre study of the Fondazione Don Carlo Gnocchi. Eur. J. Neurol. 2020, 27, 392–398. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Collamati, A.; Magnavita, N.; Sowa, A.; Topinkova, E.; Finne-Soveri, H.; van der Roest, H.G.; Tobiasz-Adamczyk, B.; Giovannini, S.; Ricciardi, W.; et al. Health determinants and survival in nursing home residents in Europe: Results from the SHELTER study. Maturitas 2018, 107, 19–25. [Google Scholar] [CrossRef]
- Biscetti, F.; Giovannini, S.; Straface, G.; Bertucci, F.; Angelini, F.; Porreca, C.; Landolfi, R.; Flex, A. RANK/RANKL/OPG pathway: Genetic association with history of ischemic stroke in Italian population. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 4574–4580. [Google Scholar] [PubMed]
- Lyons, M.; Smith, C.; Boaden, E.; Brady, M.C.; Brocklehurst, P.; Dickinson, H.; Hamdy, S.; Higham, S.; Langhorne, P.; Lightbody, C.; et al. Oral care after stroke: Where are we now? Eur. Stroke J. 2018, 3, 347–354. [Google Scholar] [CrossRef]
- Cieplik, F.; Wiedenhofer, A.M.; Pietsch, V.; Hiller, K.A.; Hiergeist, A.; Wagner, A.; Baldaranov, D.; Linker, R.A.; Jantsch, J.; Buchalla, W. Oral Health, Oral Microbiota, and Incidence of Stroke-Associated Pneumonia-A Prospective Observational Study. Front Neurol. 2020, 11, 528056. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013; ISBN 9789241548649. [Google Scholar]
- Loe, H.; Silness, J. Periodontal Disease In Pregnancy. I. Prevalence And Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Silness, J.; Loe, H. Periodontal Disease In Pregnancy. II. Correlation Between Oral Hygiene And Periodontal Condition. Acta Odontol. Scand 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; Di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief 2020, 6, 105419. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Ohura, T.; Hase, K.; Nakajima, Y.; Nakayama, T. Validity and reliability of a performance evaluation tool based on the modified Barthel Index for stroke patients. BMC Med. Res. Methodol. 2017, 17, 131. [Google Scholar] [CrossRef]
- Louie, D.R.; Eng, J.J. Berg Balance Scale score at admission can predict walking suitable for community ambulation at discharge from inpatient stroke rehabilitation. J. Rehabil. Med. 2018, 50, 37–44. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale has high intra- and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef]
- Chumney, D.; Nollinger, K.; Shesko, K.; Skop, K.; Spencer, M.; Newton, R.A. Independence Measure to accurately predict functional outcome of stroke specific population: Systematic review. J. Rehabil. Res. Dev. 2010, 47, 17–29. [Google Scholar] [CrossRef]
- Lin, C.; Katkar, M.; Lee, J.; Roth, E.; Harvey, R.L.; Prabhakaran, S. Functional Measures Upon Admission to Acute Inpatient Rehabilitation Predict Quality of Life After Ischemic Stroke. Arch. Phys. Med. Rehabil. 2019, 100, 481–487.e2. [Google Scholar] [CrossRef]
- Lees, R.A.; Hendry, B.K.; Broomfield, N.; Stott, D.; Larner, A.J.; Quinn, T.J. Cognitive assessment in stroke: Feasibility and test properties using differing approaches to scoring of incomplete items. Int. J. Geriatr. Psychiatry 2017, 32, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Hodges, J.R.; Larner, A.J. Addenbrooke’s Cognitive Examinations: ACE, ACE-R, ACE-III, ACEapp, and M-ACE. In Cognitive Screening Instruments; Springer: Cham, Switzerland, 2017; pp. 109–137. [Google Scholar]
- Matias-Guiu, J.A.; Cortés-Martínez, A.; Valles-Salgado, M.; Rognoni, T.; Fernández-Matarrubia, M.; Moreno-Ramos, T.; Matías-Guiu, J. Addenbrooke’s cognitive examination III: Diagnostic utility for mild cognitive impairment and dementia and correlation with standardized neuropsychological tests. Int. Psychogeriatr. 2017, 29, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Obana, M.; Furuya, J.; Matsubara, C.; Tohara, H.; Inaji, M.; Miki, K.; Numasawa, Y.; Minakuchi, S.; Maehara, T. Effect of a collaborative transdisciplinary team approach on oral health status in acute stroke patients. J. Oral. Rehabil. 2019, 46, 1170–1176. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Gerreth, P.; Zalewska, A.; Hojan, K.; Gerreth, K. Salivary Gland Dysfunction in Stroke Patients Is Associated with Increased Protein Glycoxidation and Nitrosative Stress. Oxid. Med. Cell. Longev. 2020, 2020, 6619439. [Google Scholar] [CrossRef]
- Schimmel, M.; Ono, T.; Lam, O.L.; Muller, F. Oro-facial impairment in stroke patients. J. Oral. Rehabil. 2017, 44, 313–326. [Google Scholar] [CrossRef]
- Kim, E.K.; Park, E.Y.; Sa Gong, J.W.; Jang, S.H.; Choi, Y.H.; Lee, H.K. Lasting effect of an oral hygiene care program for patients with stroke during in-hospital rehabilitation: A randomized single-center clinical trial. Disabil. Rehabil. 2017, 39, 2324–2329. [Google Scholar] [CrossRef]
- Ab Malik, N.M.; Yatim, S.; Lam, O.L.T.; Jin, L.; McGrath, C. Oral Health Care Guidelines, Training, and Resources among Stroke Care Providers. JDR Clin. Trans. Res. 2017, 2, 312–319. [Google Scholar] [CrossRef]
- Giebel, C.M.; Challis, D. Sensitivity of the Mini-Mental State Examination, Montreal Cognitive Assessment and the Addenbrooke’s Cognitive Examination III to everyday activity impairments in dementia: An exploratory study. Int. J. Geriatr. Psyschiatry 2017, 32, 1085–1093. [Google Scholar] [CrossRef]
- Jacova, C.; Pearce, L.A.; Costello, R.; McClure, L.A.; Holliday, S.L.; Hart, R.G.; Benavente, O.R. Cognitive impairment in lacunar strokes: The SPS3 trial. Ann. Neurol. 2012, 72, 351–362. [Google Scholar] [CrossRef]
- ‘Senda, M.; Terada, S.; Takenoshita, S.; Hayashi, S.; Yabe, M.; Imai, N.; Horiuchi, M.; Yamada, N. Diagnostic utility of the Addenbrooke’s Cognitive Examination-III (ACE-III), Mini-ACE, Mini-Mental State Examination, Montreal Cognitive Assessment, and Hasegawa Dementia Scale-Revised for detecting mild cognitive impairment and dementia. Psychogeriatrics 2020, 20, 156–162. [Google Scholar] [CrossRef]
- Wagner, C.; Marchina, S.; Deveau, J.A.; Frayne, C.; Sulmonte, K.; Kumar, S. Risk of Stroke-Associated Pneumonia and Oral Hygiene. Cerebrovasc. Dis. 2016, 41, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Kumar, G.; Jalaluddin, M.; Singh, D.K. Tooth Brush and Brushing Technique. J. Adv. Med. 2013, 2, 65–76. [Google Scholar]
- Chen, H.J.; Chen, J.L.; Chen, C.Y.; Lee, M.; Chang, W.H.; Huang, T.T. Effect of an Oral Health Programme on Oral Health, Oral Intake, and Nutrition in Patients with Stroke and Dysphagia in Taiwan: A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 2228. [Google Scholar] [CrossRef] [PubMed]
- Woon, C. Improving oral hygiene for stroke patients. Australas. J. Neurosci. 2017, 27, 11–13. [Google Scholar]
- Murie-Fernández, M.; Marzo, M.M. Predictors of Neurological and Functional Recovery in Patients with Moderate to Severe Ischemic Stroke: The EPICA Study. Stroke Res. Treat. 2020, 2020, 1419720. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, D.; Fitzgerald, S.; Rumrill, P. Multiple regression in rehabilitation research. Work 2000, 15, 209–215. [Google Scholar] [PubMed]
- Kaye, E.K.; Valencia, A.; Baba, N.; Spiro, A., 3rd; Dietrich, T.; Garcia, R.I. Tooth loss and periodontal disease predict poor cognitive function in older men. J. Am. Geriatr. Soc. 2010, 58, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Suk, S.H.; Cheong, J.S.; Lee, H.S.; Chang, H.; Do, S.Y.; Kang, J.S. Tooth loss may predict poor cognitive function in community-dwelling adults without dementia or stroke: The PRESENT project. J. Korean Med. Sci. 2013, 28, 1518–1521. [Google Scholar] [CrossRef] [PubMed]
- Bindawas, S.M.; Vennu, V.; Moftah, E. Improved functions and reduced length of stay after inpatient rehabilitation programs in older adults with stroke: A systematic review and meta-analysis of randomized controlled trials. NeuroRehabilitation 2017, 40, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Gunning, E.; Uszynski, M.K. Effectiveness of the Proprioceptive Neuromuscular Facilitation Method on Gait Parameters in Patients With Stroke: A Systematic Review. Arch. Phys. Med. Rehabil. 2019, 100, 980–986. [Google Scholar] [CrossRef]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, E.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.E.H.; Wolf, S.L.; et al. Standardized Measurement of Sensorimotor Recovery in Stroke Trials: Consensus-Based Core Recommendations from the Stroke Recovery and Rehabilitation Roundtable. Neurorehabil. Neural. Repair. 2017, 31, 784–792. [Google Scholar] [CrossRef]
- Suzuki, R.; Nagano, A.; Wakabayashi, H.; Maeda, K.; Nishioka, S.; Takahashi, M.; Momosaki, R. Assignment of Dental Hygienists Improves Outcomes in Japanese Rehabilitation Wards: A Retrospective Cohort Study. J. Nutr. Health Aging 2020, 24, 28–36. [Google Scholar] [CrossRef]
- Chen, H.M.; Lee, H.L.; Yang, F.C.; Chiu, Y.W.; Chao, S.Y. Effectiveness of Motivational Interviewing in Regard to Activities of Daily Living and Motivation for Rehabilitation among Stroke Patients. Int. J. Environ. Res. Public Health 2020, 17, 2755. [Google Scholar] [CrossRef]
- Prodinger, B.; O’Connor, R.J.; Stucki, G.; Tennant, A. Establishing score equivalence of the Functional Independence Measure motor scale and the Barthel Index, utilising the International Classification of Functioning, Disability and Health and Rasch measurement theory. J. Rehabil. Med. 2017, 49, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Gerreth, P.; Maciejczyk, M.; Zalewska, A.; Gerreth, K.; Hojan, K. Comprehensive Evaluation of the Oral Health Status, Salivary Gland Function, and Oxidative Stress in the Saliva of Patients with Subacute Phase of Stroke: A Case-Control Study. J. Clin. Med. 2020, 9, 2252. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients Demographic and Clinical Characteristics | Study Group N (%) | |
|---|---|---|
| Sex | Male | 34 (56.66) |
| Female | 26 (43.33) | |
| Formal education | Primary | 8 (13.33) |
| Vocational | 17 (28.33) | |
| Secondary | 19 (31.66) | |
| University | 16 (26.66) | |
| Location of daily life | Urban center (over 150.000 inhabitants) | 27 (45.00) |
| Small town (10.000–150.000 inhabitants) | 17 (28.33) | |
| Rural area or small village (less than 10.000 inhabitants) | 16 (26.66) | |
| Housing status | Living home with family member | 41 (68.66) |
| Living alone | 19 (31.66) | |
| Brain lesion side | Left | 27 (45.00) |
| Right | 33 (55.00) | |
| Comorbidities | BMI >30 | 28 (46.66) |
| Hypertension | 42 (70.00) | |
| Diabetes | 28 (46.66) | |
| Epilepsy | 6 (10.00) | |
| Arteriosclerosis | 37 (61.66) | |
| Limb thrombosis in the past | 4 (6.66) | |
| Glucose intolerance | 10 (16.66) | |
| Myocardial infarction | 6 (10.00) | |
| Atrial fibrillation | 18 (30.00) | |
| Angina pectoris | 4 (6.66) | |
| Chronic renal failure | 6 (10.00) | |
| Chronic obstructive pulmonary disease | 3 (5.00) | |
| Hyperlipidemia | 39 (65.00) | |
| Bronchial asthma | 4 (6.66) | |
| Parameter | Assessment I | Assessment II | p-Value | ||
|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) (95% CI) | Median (IQR) | Mean (SD) (95% CI) | ||
| Number of teeth present in oral cavity | 14 (2–24) | 14 (11) (10–18) | 14 (2–24) | 14(11) (10–18) | 1.0 |
| DT | 1 (0–4) | 2.6 (3.6) (1.7–3.5) | 1 (0–4) | 2.6 (3.6) (1.7–3.5) | 1.0 |
| MT | 20 (8–28) | 18 (10) (15–20) | 20 (8–28) | 18 (10) (15–20) | 1.0 |
| FT | 0 (0–3) | 2.4 (4.5) (1.2–3.6) | 0 (0–3) | 2.4 (4.5) (1.2–3.6) | 1.0 |
| DMFT | 25 (17–28) | 23 (7) (21–25) | 25 (17–28) | 23 (7) (21–25) | 1.0 |
| DS | 2 (0–9) | 7.4 (12) (4.3–10) | 2 (0–9) | 7.4 (12) (4.3–10) | 1.0 |
| MS | 92 (40–147) | 86 (51) (73–100) | 92 (40–147) | 86 (51) (73–100) | 1.0 |
| FS | 0 (0–5.5) | 5.8 (13) (2.4–9.1) | 0 (0–5.5) | 5.8 (13) (2.4–9.1) | 1.0 |
| DMFS | 113 (57–147) | 100 (43) (88–111) | 113 (57–147) | 100 (43) (88–111) | 1.0 |
| GI | 1.2 (0.5–2) | 1.2 (0.87) (0.98–1.5) | 0.83 (0–1.8) | 0.99 (0.9) (0.71–1.3) | <0.001 |
| PlI | 2 (1–3) | 1.9 (0.93) (1.6–2.2) | 1.5 (0.5–2.5) | 1.6 (1) (1.2–1.9) | <0.001 |
| Parameter | Assessment I | Assessment II | p-Value | ||
|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) (95% CI) | Median (IQR) | Mean (SD) (95% CI) | ||
| BI | 12 (7–13) | 11 (3.9) (9.5–12) | 19 (15–20) | 16 (5.1) (15–18) | <0.001 |
| FIM | 89 (60–109) | 82 (32) (74–80) | 115 (96–126) | 104 (31) (96–112) | <0.001 |
| BBS | 36 (17–42) | 30 (16) (26–31) | 50 (37–54) | 43 (15) (39–47) | <0.001 |
| ACE III total scale | 72 (57–82) | 66 (23) (60–72) | 81 (68–90) | 76 (22) (70–82) | <0.001 |
| ACE memory | 18 (13–22) | 17 (6.8) (15–18) | 21 (18–24) | 19 (6.3) (18–21) | <0.001 |
| ACE attention and orientation | 14 (12–17) | 13 (4.3) (12–15) | 16 (14–18) | 15 (3.5) (14–16) | <0.001 |
| ACE verbal fluency | 8 (5–11) | 7.5 (3.9) (6.5–8.5) | 10 (7–12) | 9.1 (3.6) (8.1–10) | <0.001 |
| ACE language function | 21 (18–24) | 19 (7.3) (17–21) | 24 (20–25) | 21 (6.1) (20–23) | <0.001 |
| ACE visual-spatial functions | 11 (8–16) | 11 (4.5) (9.7–12) | 13 (11–15) | 13 (3.6) (12–13) | <0.001 |
| Study Time | Number of Teeth Present in Oral Cavity | DT | MT | FT | DMFT | DS | MS | FS | DMFS | GI 1 | GI 2 | PlI 1 | PlI 2 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BI | I | −0.203 | −0.118 | 0.013 | 0.019 | −0.071 | −0.14 | 0.021 | 0.019 | −0.043 | −0.4 ** | −0.42 ** | −0.363 * | −0.344 * |
| II | 0.281 | 0.048 | −0.208 | 0.238 | −0.248 | 0.019 | −0.203 | 0.231 | −0.212 | −0.293 | −0.232 | −0.338 * | −0.215 | |
| FIM | I | −0.001 | −0.134 | −0.078 | 0.066 | −0.2 | −0.166 | −0.062 | 0.069 | −0.134 | −0.394 ** | −0.433 ** | −0.408 ** | −0.399 ** |
| II | 0.126 | −0.087 | −0.137 | 0.155 | −0.223 | −0.114 | −0.121 | 0.15 | −0.184 | −0.403 ** | −0.407 ** | −0.424 ** | −0.381 * | |
| BBS | I | 0.018 | −0.124 | −0.082 | 0.038 | −0.195 | −0.138 | −0.066 | 0.045 | −0.122 | −0.33 * | −0.423 ** | −0.363 * | −0.4 ** |
| II | 0.217 | −0.045 | −0.218 | 0.182 | −0.299 | −0.082 | −0.199 | 0.183 | −0.238 | −0.389 ** | −0.386 * | −0.465 ** | −0.407 ** | |
| ACE III | I | 0.179 | 0.006 | −0.19 | 0.161 | −0.286 * | −0.023 | −0.183 | 0.156 | −0.212 | −0.154 | −0.121 | −0.211 | −0.117 |
| II | 0.395 * | −0.03 | −0.312 * | 0.346 ** | −0.339 ** | −0.054 | −0.325* | 0.336 ** | −0.329* | −0.257 | −0.189 | −0.319* | −0.208 | |
| ACE—attention and orientation | I | 0.084 | 0.002 | −0.11 | 0.09 | −0.204 | −0.046 | −0.107 | 0.092 | −0.15 | −0.244 | −0.221 | −0.3* | −0.243 |
| II | 0.143 | −0.061 | −0.18 | 0.242 | −0.221 | −0.109 | −0.223 | 0.233 | −0.245 | −0.16 | −0.121 | −0.293 | −0.236 | |
| ACE—memory | I | 0.349 | −0.03 | −0.233 | 0.16 | −0.28* | −0.057 | −0.215 | 0.149 | −0.23 | −0.069 | 0.027 | −0.1 | 0.045 |
| II | 0.309 | −0.03 | −0.235 | 0.222 | −0.273* | −0.062 | −0.234 | 0.211 | −0.237 | −0.023 | 0.043 | −0.113 | 0.023 | |
| ACE—verbal fluency | I | 0.102 | 0.006 | −0.094 | 0.035 | −0.123 | −0.02 | −0.079 | 0.034 | −0.088 | −0.079 | −0.085 | −0.174 | −0.134 |
| II | 0.333 | 0.067 | −0.244 | 0.225 | −0.221 | 0.046 | −0.221 | 0.225 | −0.206 | −0.175 | −0.18 | −0.28 | −0.224 | |
| ACE—language function | I | 0.24 | −0.085 | −0.161 | 0.191 | −0.202 | −0.129 | −0.158 | 0.192 | −0.17 | −0.185 | −0.187 | −0.239 | −0.197 |
| II | 0.411 | −0.113 | −0.274 * | 0.35 ** | −0.344 ** | −0.142 | −0.298* | 0.352 ** | −0.322* | −0.22 | −0.193 | −0.275 | −0.224 | |
| ACE—visual−spatial function | I | −0.155 | −0.068 | −0.121 | 0.18 | −0.18 | −0.132 | −0.138 | 0.187 | −0.182 | −0.203 | −0.194 | −0.235 | −0.174 |
| II | 0.207 | −0.051 | −0.241 | 0.311 | −0.209 | −0.105 | −0.256 | 0.318* | −0.227 | −0.225 | −0.224 | −0.238 | −0.192 |
| Dependent Variable | Independent Variable | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Sex | Tobacco Smoking | Number of Strokes | ACE III | BI | FIM | BBS | ||
| Number of teeth present in oral cavity | EE | −0.266 | −1.545 | 1 | −1.021 | 0.0594 | −0.957 | 0.04787 | 0.1623 |
| 95% CI | −0.5506 to 0.01865 | −7.676 to 4.586 | −6.576 to 8.576 | −3.678 to 1.636 | −0.1215 to 0.2403 | −1.980 to 0.06632 | −0.2245 to 0.3203 | −0.2490 to 0.5736 | |
| p-value | 0.0664 | 0.6156 | 0.7924 | 0.4445 | 0.5133 | 0.0662 | 0.726 | 0.4324 | |
| DT | EE | −0.1042 | −0.2103 | 0.2715 | −0.3998 | 0.008942 | 0.03388 | −0.03951 | 0.04047 |
| 95% CI | −0.1714 to −0.03701 | −1.578 to 1.158 | −1.320 to 1.863 | −1.169 to 0.3694 | −0.02735 to 0.04523 | −0.2210 to 0.2888 | −0.1020 to 0.02296 | −0.05794 to 0.1389 | |
| p-value | 0.0027 ** | 0.7611 | 0.7358 | 0.3051 | 0.6262 | 0.7926 | 0.2126 | 0.4167 | |
| MT | EE | 0.004214 | 0.319 | 0.118 | 0.279 | −0.004451 | 0.0358 | −0.0002452 | −0.02673 |
| 95% CI | −0.01347 to 0.02191 | −0.06859 to 0.7065 | −0.3337 to 0.5697 | 0.08872 to 0.4692 | −0.01607 to 0.007167 | −0.03703 to 0.1086 | −0.01714 to 0.01665 | −0.05525 to 0.001799 | |
| p-value | 0.6367 | 0.1053 | 0.6046 | 0.0046 ** | 0.4479 | 0.3307 | 0.977 | 0.0659 | |
| FT | EE | −0.1083 | −0.6938 | −1.465 | −0.5722 | 0.02142 | −0.0005962 | −0.03311 | 0.06244 |
| 95% CI | −0.1886 to −0.0280 | −2.329 to 0.9411 | −3.367 to 0.4371 | −1.492 to 0.3471 | −0.02195 to 0.06479 | −0.3040 to 0.3052 | −0.1078 to 0.04154 | −0.05516 to 0.1801 | |
| p-value | 0.0087 ** | 0.402 | 0.1297 | 0.2199 | 0.3297 | 0.9969 | 0.3811 | 0.2949 | |
| DMFT | EE | 0.1841 | −1.815 | −1.513 | −0.5752 | −0.06282 | 0.4849 | −0.0427 | −0.1218 |
| 95% CI | 0.0593 to 0.3089 | −4.359 to 0.7212 | −4.469 to 1.442 | −2.004 to 0.8533 | −0.1302 to 0.00457 | 0.01156 to 0.9582 | −0.1587 to 0.07329 | −0.3045 to 0.06098 | |
| p-value | 0.0042 ** | 0.1586 | 0.3124 | 0.4264 | 0.0497 * | 0.0448 * | 0.467 | 0.1893 | |
| DS | EE | −0.3086 | −0.1191 | 1.227 | −1.054 | 0.02 | 0.1998 | −0.2207 | 0.2313 |
| 95% CI | −0.5359 to −0.08117 | −4.748 to 4.510 | −4.159 to 6.612 | −3.657 to 1.549 | −0.1028 to 0.1427 | −0.6627 to 1.1062 | −0.4321 to −0.009355 | −0.1017 to 0.5643 | |
| p-value | 0.0083 ** | 0.9594 | 0.6525 | 0.4238 | 0.7474 | 0.647 | 0.0409 * | 0.1714 | |
| MS | EE | 1.998 | −6.178 | −3.742 | −1.757 | −0.425 | 1.931 | 0.1456 | −1.031 |
| 95% CI | 1.133 to 2.863 | −23.75 to 11.48 | −24.24 to 16.75 | −11.66 to 8.148 | −0.8928 to 0.04226 | −1.351 to 5.213 | −0.6587 to 0.9498 | −2.298 to 0.2367 | |
| p-value | <0.0001 ** | 0.4883 | 0.718 | 0.7258 | 0.0742 | 0.245 | 0.7204 | 0.1097 | |
| FS | EE | −0.1404 | −0.8427 | −3.474 | −1.908 | 0.05655 | −0.02189 | −0.1204 | 0.2435 |
| 95% CI | −0.3936 to 0.1128 | −5.997 to 4.312 | −9.470 to 2.523 | −4.806 to 0.9901 | −0.08018 to 0.1933 | −0.9384 to 0.8822 | −0.3558 to 0.1149 | −0.1273 to 0.6142 | |
| p-value | 0.2741 | 0.7464 | 0.2533 | 0.1946 | 0.4141 | 0.964 | 0.3126 | 0.1958 | |
| DMFS | EE | 1.549 | −7.14 | −5.99 | −4.719 | −0.3485 | 2.152 | −0.1956 | −0.5561 |
| 95% CI | 0.8175 to 2.280 | −22.03 to 7.749 | −23.310 to 11.33 | −13.09 to 3.654 | −0.7435 to 0.04654 | −0.6218 to 4.927 | −0.8755 to 0.4843 | −1.627 to 0.5150 | |
| p-value | <0.0001 ** | 0.3439 | 0.4945 | 0.2663 | 0.0832 | 0.127 | 0.5696 | 0.3056 | |
| PlI | EE | −0.00303 | 0.4128 | 0.2507 | 0.305 | −0.006446 | 0.01106 | −0.000569 | −0.02626 |
| 95% CI | −0.0216 to 0.0156 | 0.00127 to 0.8244 | −0.2395 to 0.7408 | 0.1037 to 0.5063 | −0.01923 to 0.00634 | −0.0656 to 0.08773 | −0.01759 to 0.01873 | −0.05651 to 0.00398 | |
| p-value | 0.7469 | 0.0493 * | 0.3115 | 0.0035 ** | 0.3185 | 0.7745 | 0.9504 | 0.0878 | |
| GI | EE | −0.01068 | 0.1511 | −0.04456 | 0.2454 | −0.000729 | −0.004064 | −0.003209 | −0.01496 |
| 95% CI | −0.02783 to 0.006461 | −0.2277 to 0.5299 | −0.4957 to 0.4066 | 0.06012 to 0.4306 | −0.0125 to 0.01104 | −0.07462 to 0.0665 | −0.01993 to 0.01351 | −0.0428 to 0.01288 | |
| p-value | 0.186 | 0.4541 | 0.7842 | 0.0101 * | 0.9021 | 0.909 | 0.7032 | 0.288 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerreth, P.; Gerreth, K.; Maciejczyk, M.; Zalewska, A.; Hojan, K. Is an Oral Health Status a Predictor of Functional Improvement in Ischemic Stroke Patients Undergoing Comprehensive Rehabilitation Treatment? Brain Sci. 2021, 11, 338. https://doi.org/10.3390/brainsci11030338
Gerreth P, Gerreth K, Maciejczyk M, Zalewska A, Hojan K. Is an Oral Health Status a Predictor of Functional Improvement in Ischemic Stroke Patients Undergoing Comprehensive Rehabilitation Treatment? Brain Sciences. 2021; 11(3):338. https://doi.org/10.3390/brainsci11030338
Chicago/Turabian StyleGerreth, Piotr, Karolina Gerreth, Mateusz Maciejczyk, Anna Zalewska, and Katarzyna Hojan. 2021. "Is an Oral Health Status a Predictor of Functional Improvement in Ischemic Stroke Patients Undergoing Comprehensive Rehabilitation Treatment?" Brain Sciences 11, no. 3: 338. https://doi.org/10.3390/brainsci11030338
APA StyleGerreth, P., Gerreth, K., Maciejczyk, M., Zalewska, A., & Hojan, K. (2021). Is an Oral Health Status a Predictor of Functional Improvement in Ischemic Stroke Patients Undergoing Comprehensive Rehabilitation Treatment? Brain Sciences, 11(3), 338. https://doi.org/10.3390/brainsci11030338