The Effect of Electrical Muscle Stimulation on Muscle Mass and Balance in Older Adults with Dementia

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design and Setting
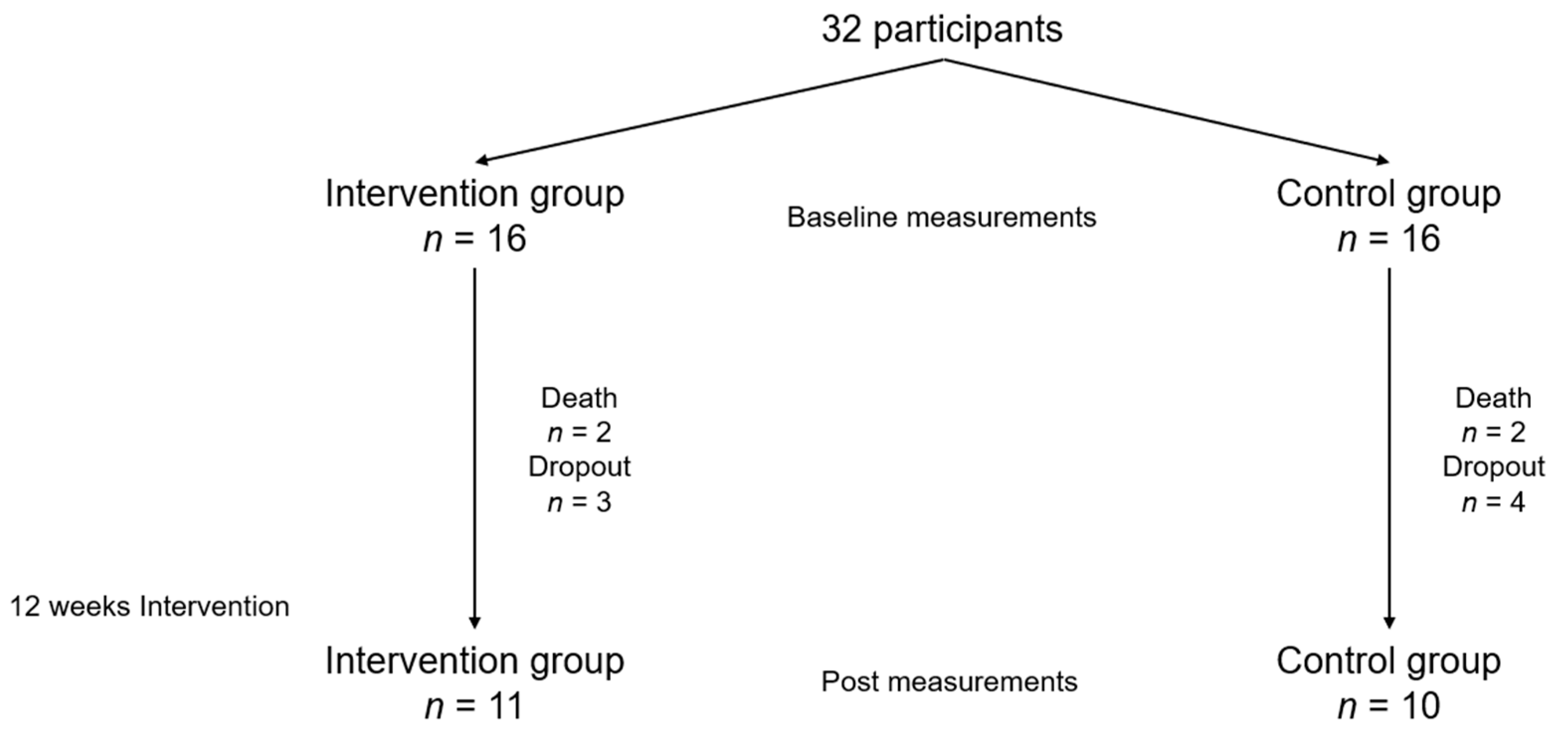
2.2. Participants
2.3. Randomization and Allocation Procedure
2.4. Experimental Design
2.5. Measurements of Muscle Mass
2.6. Statistical Analysis
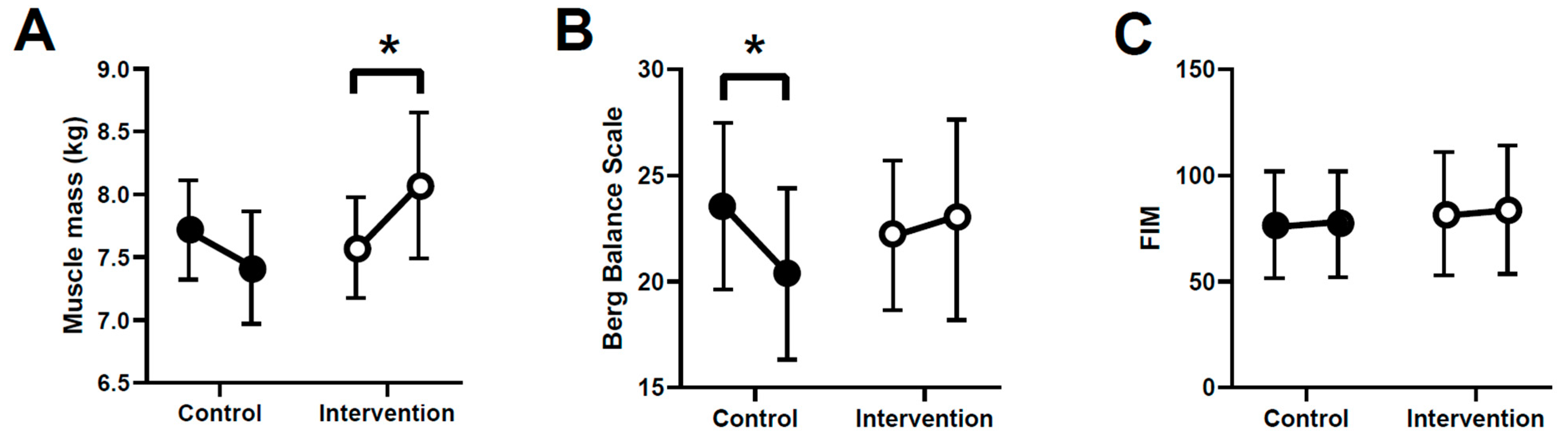
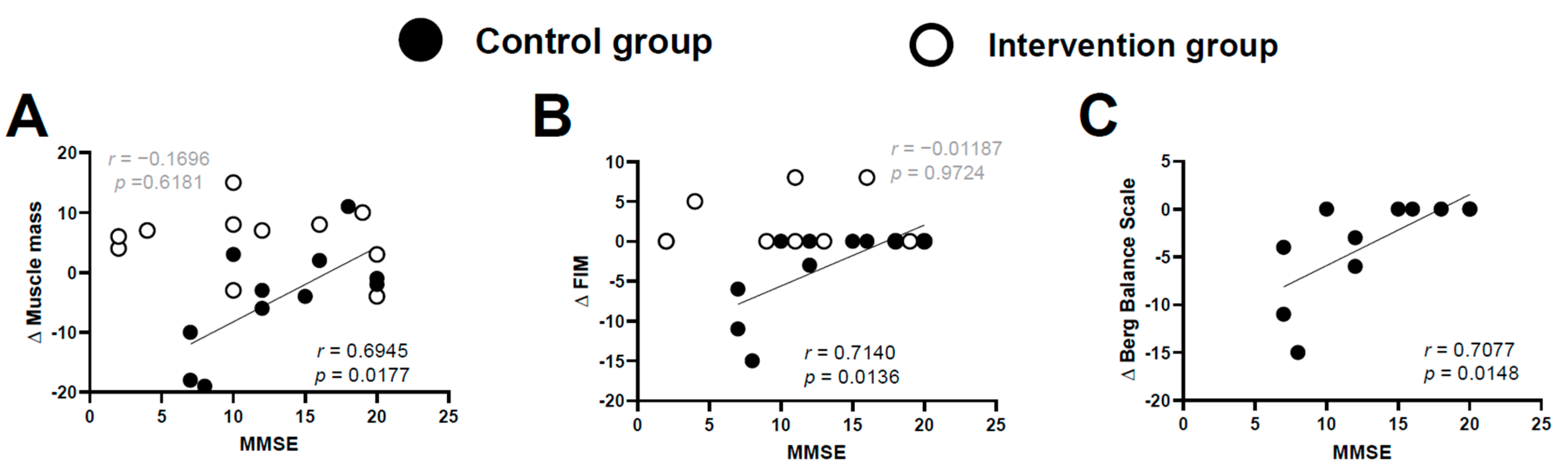
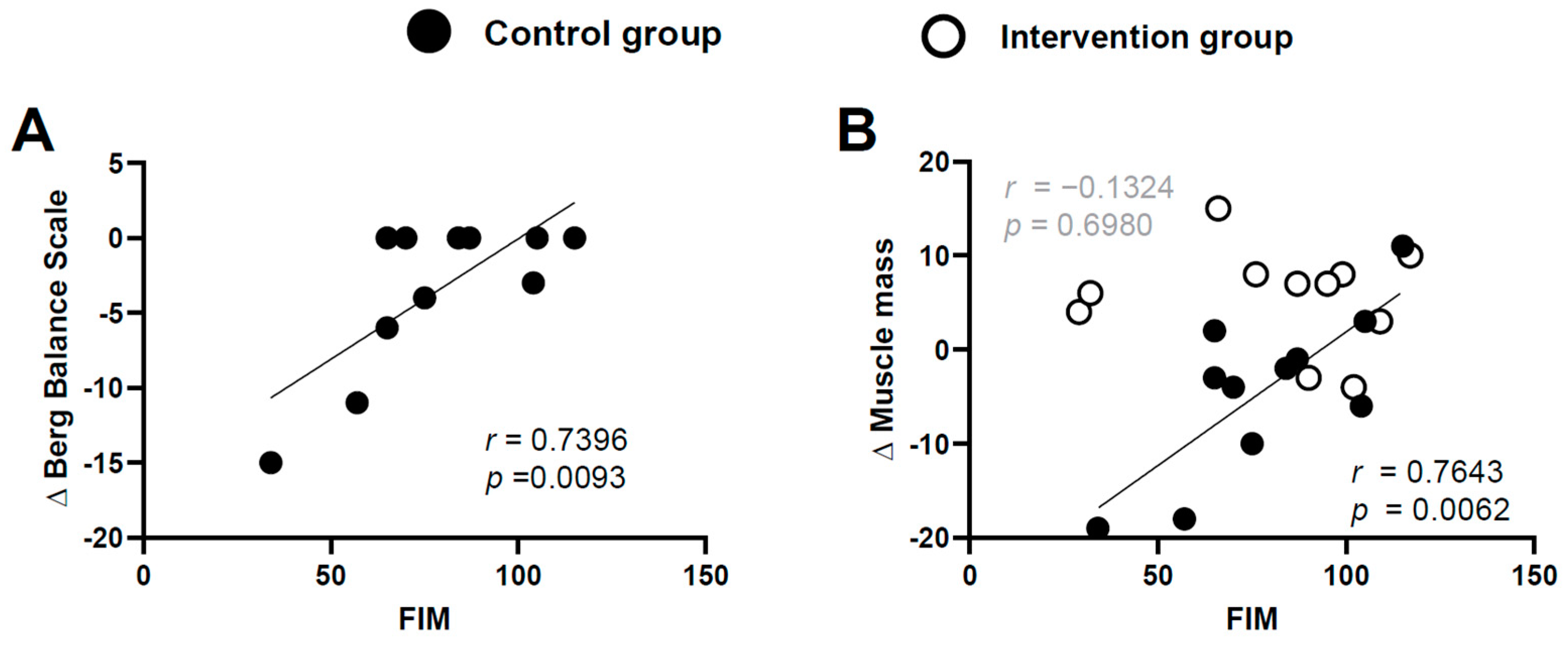
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office. Chapter 1. Situation on Aging. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2018/pdf/c1-1.pdf: (accessed on 2 September 2020).
- Ikezoe, T.; Nakamura, M.; Shima, H.; Asakawa, Y.; Ichihashi, N. Association between walking ability and trunk and lower-limb muscle atrophy in institutionalized elderly women: A longitudinal pilot study. J. Physiol. Anthropol. 2015, 34, 31. [Google Scholar] [CrossRef]
- Pisciottano, M.V.C.; Pinto, S.S.; Szejnfeld, V.L.; Castro, C.H.M. The relationship between lean mass, muscle strength and physical ability in independent healthy elderly women from the community. J. Nutr. Health Aging 2014, 18, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Hinkka, K.; Karppi, S.-L.; Pohjolainen, T.; Rantanen, T.; Puukka, P.; Tilvis, R. Network-based geriatric rehabilitation for frail elderly people: Feasibility and effects on subjective health and pain at one year. J. Rehabil. Med. 2007, 39, 473–478. [Google Scholar] [CrossRef][Green Version]
- Imanishi, M.; Tomohisa, H.; Higaki, K. Impact of continuous in-home rehabilitation on quality of life and activities of daily living in elderly clients over 1 year. Geriatr. Gerontol. Int. 2017, 17, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Dirks, M.L.; Wall, B.T.; Snijders, T.; Ottenbros, C.L.; Verdijk, L.B.; Van Loon, L.J. Neuromuscular electrical stimulation prevents muscle disuse atrophy during leg immobilization in humans. Acta Physiol. 2014, 210, 628–641. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Maffiuletti, N.A. Neural adaptations to electrical stimulation strength training. Eur. J. Appl. Physiol. 2011, 111, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Man, W.D.; Gao, W.; Higginson, I.J.; Wilcock, A.; Maddocks, M. Neuromuscular electrical stimulation for muscle weakness in adults with advanced disease. Cochrane Database Syst. Rev. 2016, 10, Cd009419. [Google Scholar] [CrossRef]
- Gerovasili, V.; Stefanidis, K.; Vitzilaios, K.; Karatzanos, E.; Politis, P.; Koroneos, A.; Chatzimichail, A.; Routsi, C.; Roussos, C.; Nanas, S. Electrical muscle stimulation preserves the muscle mass of critically ill patients: A randomized study. Crit. Care 2009, 13, R161. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, Y.; Watanabe, K.; Kawade, S.; Takahashi, T.; Kimura, H.; Maruyama, H.; Hyngstrom, A. The effect of a portable electrical muscle stimulation device at home on muscle strength and activation patterns in locomotive syndrome patients: A randomized control trial. J. Electromyogr. Kinesiol. 2019, 45, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, E.P.; Cook, P.G. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Man. Ther. 2013, 18, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Kuitunen, S.; Racinais, S.; Cresswell, A.G. Recruitment of the plantar intrinsic foot muscles with increasing postural demand. Clin. Biomech. (Bristol Avon) 2012, 27, 46–51. [Google Scholar] [CrossRef]
- Bosaeus, I.; Wilcox, G.; Rothenberg, E.; Strauss, B.J. Skeletal muscle mass in hospitalized elderly patients: Comparison of measurements by single-frequency BIA and DXA. Clin. Nutr. 2014, 33, 426–431. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Nishikawa, Y.; Watanabe, K.; Takahashi, T.; Kimura, H.; Maruyama, H. The effect of medication on vastus lateralis muscle activation patterns in Parkinson’s disease patients. J. Electromyogr. Kinesiol. 2018, 42, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Maki, Y.; Sakurai, T.; Okochi, J.; Yamaguchi, H.; Toba, K. Rehabilitation to live better with dementia. Geriatr. Gerontol. Int. 2018, 18, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Sondell, A.; Rosendahl, E.; Sommar, J.N.; Littbrand, H.; Lundin-Olsson, L.; Lindelöf, N. Motivation to Participate in High-Intensity Functional Exercise Compared With a Social Activity in Older People With Dementia in Nursing Homes. PLoS ONE 2018, 13, 0206899. [Google Scholar] [CrossRef]
- Kowalska, J.; Mazurek, J.; Kubasik, N.; Rymaszewska, J. Effectiveness of physiotherapy in elderly patients with dementia: A prospective, comparative analysis. Disabil. Rehabil. 2019, 41, 815–819. [Google Scholar] [CrossRef]
- Lamb, S.E.; Sheehan, B.; Atherton, N.; Nichols, V.; Collins, H.; Mistry, D.; Dosanjh, S.; Slowther, A.M.; Khan, I.; Petrou, S.; et al. Dementia And Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: Randomised controlled trial. BMJ 2018, 361, k1675. [Google Scholar] [CrossRef] [PubMed]
- Hirose, T.; Shiozaki, T.; Shimizu, K.; Mouri, T.; Noguchi, K.; Ohnishi, M.; Shimazu, T. The effect of electrical muscle stimulation on the prevention of disuse muscle atrophy in patients with consciousness disturbance in the intensive care unit. J. Crit. Care 2013, 28, 536.e1–536.e7. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A.; Minetto, M.A.; Farina, D.; Bottinelli, R. Electrical stimulation for neuromuscular testing and training: State-of-the art and unresolved issues. Eur. J. Appl. Physiol. 2011, 111, 2391–2397. [Google Scholar] [CrossRef]
- Stevens, J.E.; Mizner, R.L.; Snyder-Mackler, L. Neuromuscular electrical stimulation for quadriceps muscle strengthening after bilateral total knee arthroplasty: A case series. J. Orthop. Sports Phys. Ther. 2004, 34, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.B.; Chong, S.L.; James, K.B.; Kido, A.; Bell, G.J.; Tubman, L.A.; Belanger, M. Electrical stimulation for therapy and mobility after spinal cord injury. Prog. Brain Res. 2002, 137, 27–34. [Google Scholar]
- Belanger, M.; Stein, R.B.; Wheeler, G.D.; Gordon, T.; Leduc, B. Electrical stimulation: Can it increase muscle strength and reverse osteopenia in spinal cord injured individuals? Arch. Phys. Med. Rehabil. 2000, 81, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, Y.; Watanabe, K.; Takahashi, T.; Maeda, N.; Maruyama, H.; Kimura, H. The effect of electrical muscle stimulation on quadriceps muscle strength and activation patterns in healthy young adults. Eur. J. Sport. Sci. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, D.; Smith, B.; Malone, T.R. A strength study utilizing the electro-stim 180. J. Orthop. Sports Phys. Ther. 1985, 7, 50–53. [Google Scholar] [CrossRef]
- Broekmans, T.; Roelants, M.; Feys, P.; Alders, G.; Gijbels, D.; Hanssen, I.; Stinissen, P.; Eijnde, B.O. Effects of long-term resistance training and simultaneous electro-stimulation on muscle strength and functional mobility in multiple sclerosis. Mult. Scler. J. 2011, 17, 468–477. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention Group | Control Group | p Value |
|---|---|---|---|
| Age, years | 89.4 ± 4.8 | 88.1 ± 5.2 | p = 0.4949 |
| Height, cm | 145.2 ± 6.9 | 147.3 ± 5.8 | p = 0.3577 |
| Body mass, kg | 45.9 ± 5.5 | 46.9 ± 4.9 | p = 0.5803 |
| MMSE | 12.4 ± 7.2 (5–20) | 13.4 ± 5.1 (6–20) | p = 0.6381 |
| FIM | 83.8 ± 29.0 (29–117) | 76.8 ± 25.1 (25–115) | p = 0.5884 |
| Berg Balance Score | 22.5 ± 14.1 | 21.8 ± 11.5 | p = 0.8892 |
| Lower limb muscle mass, kg | 7.6 ± 1.6 | 8.0 ± 1.3 | p = 0.3698 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, Y.; Takahashi, T.; Kawade, S.; Maeda, N.; Maruyama, H.; Hyngstrom, A. The Effect of Electrical Muscle Stimulation on Muscle Mass and Balance in Older Adults with Dementia. Brain Sci. 2021, 11, 339. https://doi.org/10.3390/brainsci11030339
Nishikawa Y, Takahashi T, Kawade S, Maeda N, Maruyama H, Hyngstrom A. The Effect of Electrical Muscle Stimulation on Muscle Mass and Balance in Older Adults with Dementia. Brain Sciences. 2021; 11(3):339. https://doi.org/10.3390/brainsci11030339
Chicago/Turabian StyleNishikawa, Yuichi, Tetsuya Takahashi, Shuhei Kawade, Noriaki Maeda, Hirofumi Maruyama, and Allison Hyngstrom. 2021. "The Effect of Electrical Muscle Stimulation on Muscle Mass and Balance in Older Adults with Dementia" Brain Sciences 11, no. 3: 339. https://doi.org/10.3390/brainsci11030339
APA StyleNishikawa, Y., Takahashi, T., Kawade, S., Maeda, N., Maruyama, H., & Hyngstrom, A. (2021). The Effect of Electrical Muscle Stimulation on Muscle Mass and Balance in Older Adults with Dementia. Brain Sciences, 11(3), 339. https://doi.org/10.3390/brainsci11030339