
Effects of a Single Yoga Session on Cardiac Interoceptive Accuracy and Emotional Experience


Abstract
1. Introduction
1.1. Interoception
1.2. The Association between Cardiac Interoceptive Accuracy and Physical Activity
1.3. Approaches to Train Cardiac Interoceptive Accuracy
1.4. The Effect of Yoga Practice on Health-Related Parameters
1.5. The Effect of Yoga and Physical Exercises on Emotional Experience
1.6. Aims and Hypotheses of the Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedure and Materials
2.3. Emotional Experience
2.4. Physical Activity
2.5. Cardiac Interoceptive Accuracy (IAc)
2.6. Group: Yoga, Endurance, and Inactive Control Group
2.7. Data Analysis
3. Results
3.1. Descriptive Statistics
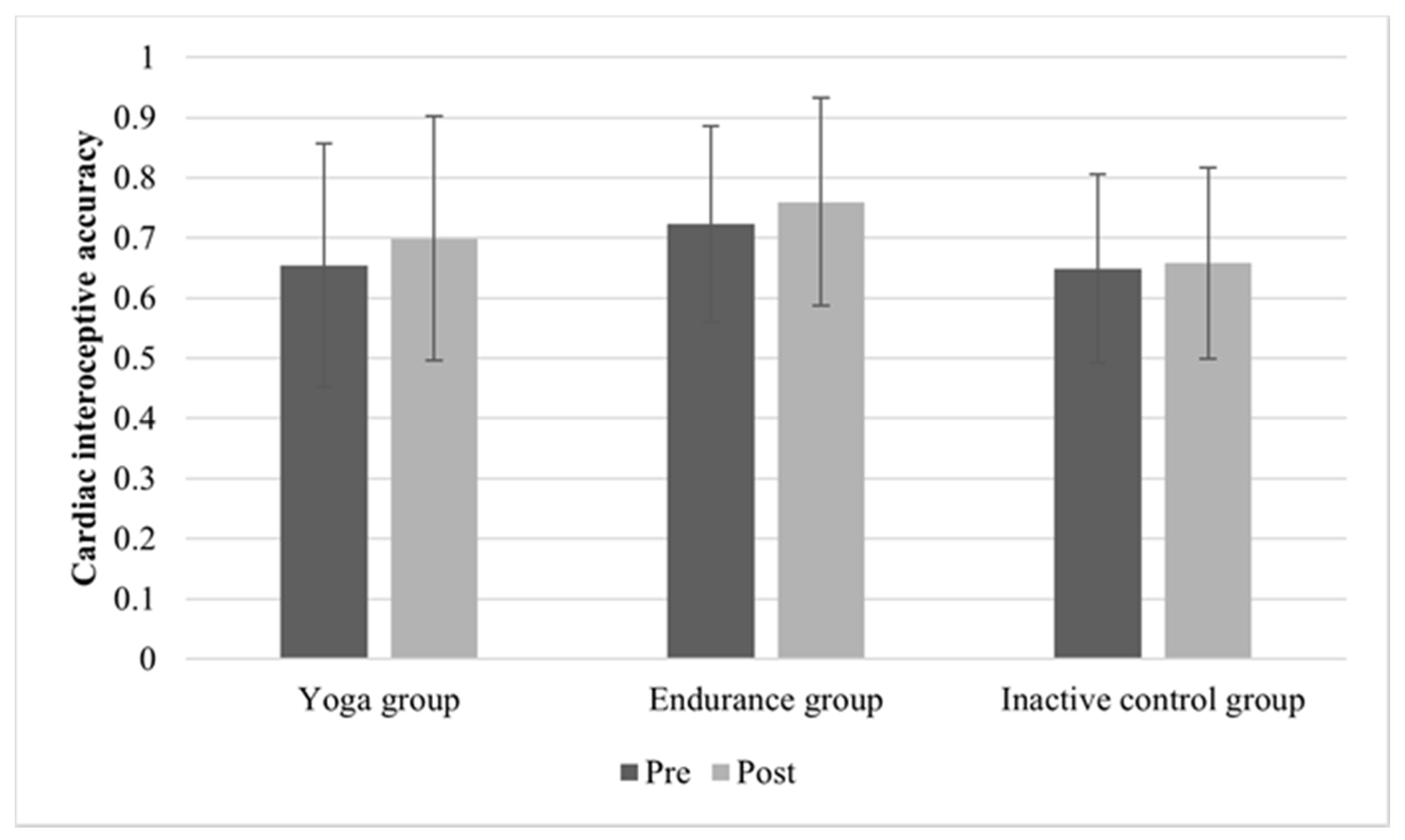
3.2. Changes in Cardiac Interoceptive Accuracy
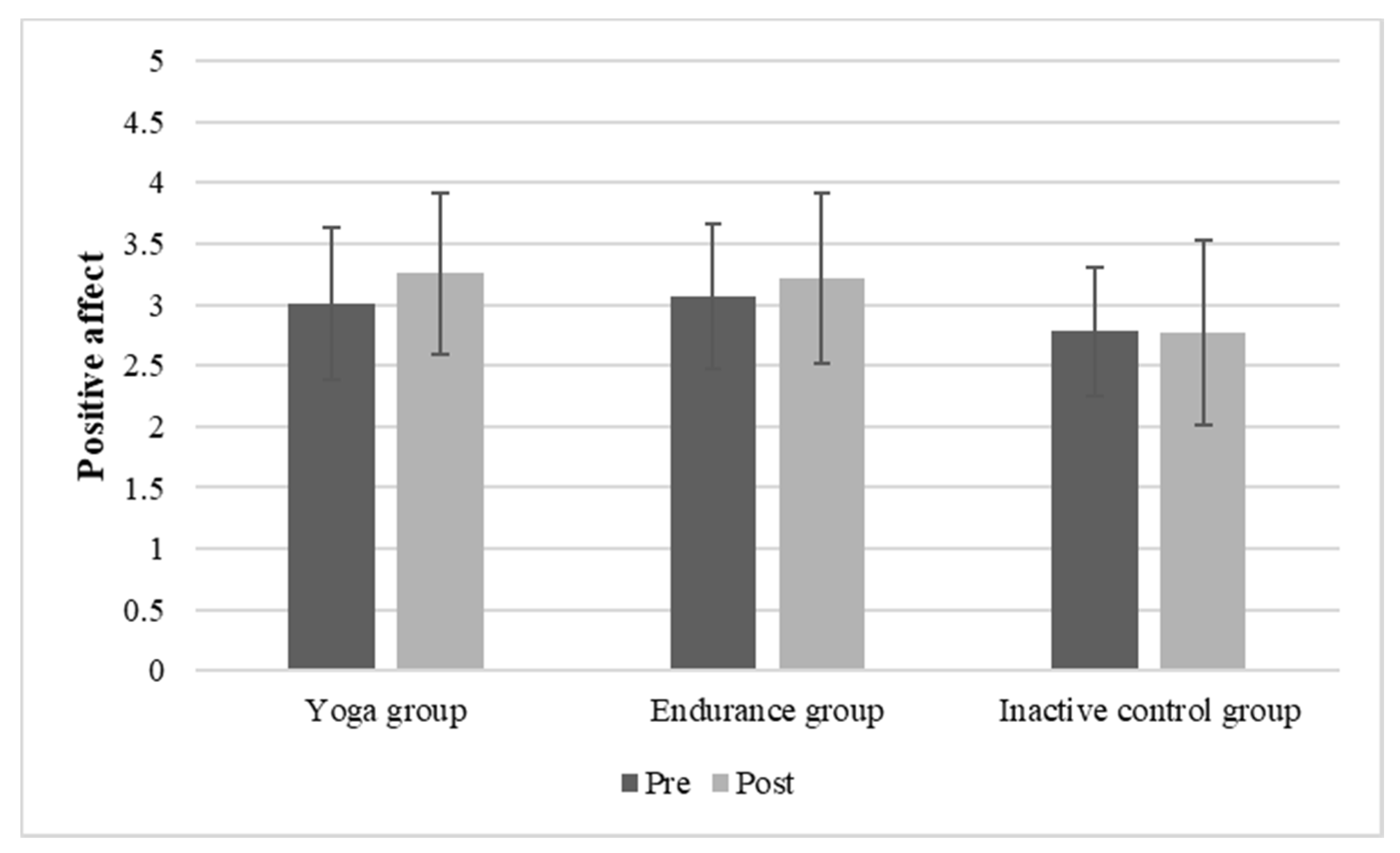
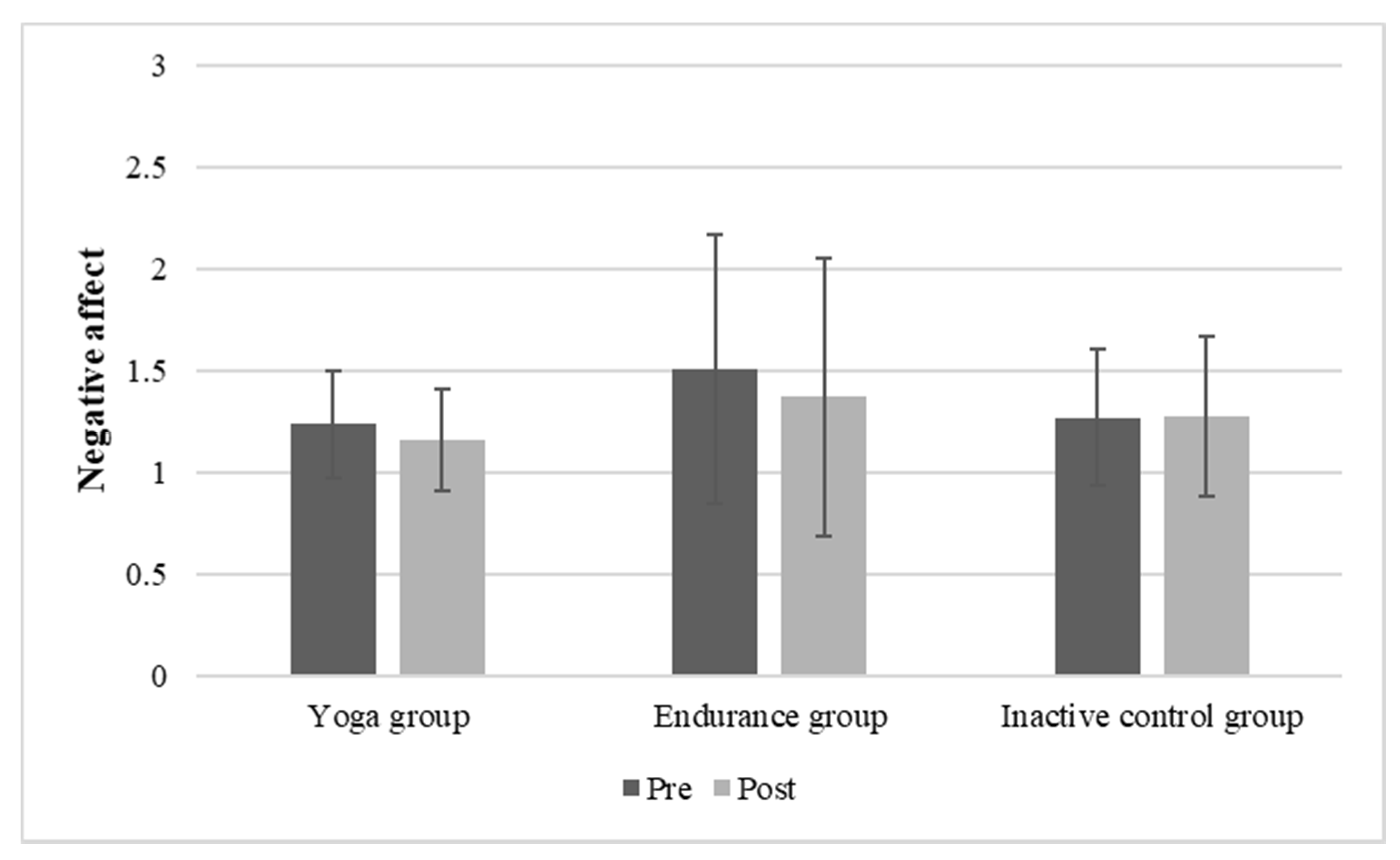
3.3. Changes in Emotional Experience
4. Discussion
4.1. Effect of Yoga on Cardiac Interoceptive Accuracy
4.2. Effect of Yoga vs. Endurance Exercise on Emotional Experience
4.3. Change in Positive Affect as a Predictor for IAc in the Yoga Group
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.D.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and Mental Health: A Roadmap. Biol. Psychiatry 2018, 3, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F.; Quigley, K.S.; Bliss-Moreau, E.; Aronson, K.R. Interoceptive sensitivity and self-reports of emotional experience. J. Pers. Soc. Psychol. 2004, 87, 684–697. [Google Scholar] [CrossRef] [PubMed]
- Bornemann, B.; Singer, T. Taking time to feel our body: Steady increases in heartbeat perception accuracy and decreases in alexithymia over 9 months of contemplative mental training. Psychophysiology 2017, 54, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.D. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef]
- Critchley, H.D.; Wiens, S.; Rotshtein, P.; Öhman, A.; Dolan, R.J. Neural systems supporting interoceptive awareness. Nat. Neurosci. 2004, 7, 189–195. [Google Scholar] [CrossRef]
- Critchley, H.D.; Garfinkel, S.N. Interoception and emotion. Curr. Opin. Psychol. 2017, 17, 7–14. [Google Scholar] [CrossRef]
- Dunn, B.D.; Galton, H.C.; Morgan, R.; Evans, D.; Oliver, C.; Meyer, M.; Cusack, R.; Lawrence, A.D.; Dalgleish, T. Listening to your heart. How interoception shapes emotion experience and intuitive decision making. Psychol. Sci. 2010, 21, 1835–1844. [Google Scholar] [CrossRef] [PubMed]
- Füstös, J.; Gramann, K.; Herbert, B.M.; Pollatos, O. On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Soc. Cogn. Affect. Neurosci. 2013, 8, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R. The Feeling of What Happens: Body, Emotion and the Making of Consciousness; Vintage: London, UK, 2000; ISBN 0099288761. [Google Scholar]
- Damasio, A.R.; Grabowski, T.J.; Bechara, A.; Damasio, H.; Ponto, L.L.; Parvizi, J.; Hichwa, R.D. Subcortical and cortical brain activity during the feeling of self-generated emotions. Nat. Neurosci. 2000, 3, 1049–1056. [Google Scholar] [CrossRef]
- James, W. What is an emotion? Mind 1884, 9, 188–205. [Google Scholar] [CrossRef]
- Schachter, S.; Singer, J. Cognitive, social, and physiological determinants of emotional state. Psychol. Rev. 1962, 69, 379–399. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, S.N.; Seth, A.K.; Barrett, A.B.; Suzuki, K.; Critchley, H.D. Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 2015, 104, 65–74. [Google Scholar] [CrossRef]
- Schandry, R. Heart Beat Perception and Emotional Experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Eggart, M.; Lange, A.; Binser, M.J.; Queri, S.; Müller-Oerlinghausen, B. Major Depressive Disorder Is Associated with Impaired Interoceptive Accuracy: A Systematic Review. Brain Sci. 2019, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Traut-Mattausch, E.; Schandry, R. Differential effects of anxiety and depression on interoceptive accuracy. Depress. Anxiety 2009, 26, 167–173. [Google Scholar] [CrossRef]
- Fischer, D.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Weiss, S.; Pollatos, O. Interoceptive Processes in Anorexia Nervosa in the Time Course of Cognitive-Behavioral Therapy: A Pilot Study. Front. Psychiatry 2016, 7, 199. [Google Scholar] [CrossRef]
- Pollatos, O.; Kurz, A.-L.; Albrecht, J.; Schreder, T.; Kleemann, A.M.; Schöpf, V.; Kopietz, R.; Wiesmann, M.; Schandry, R. Reduced perception of bodily signals in anorexia nervosa. Eat. Behav. 2008, 9, 381–388. [Google Scholar] [CrossRef]
- Schultchen, D.; Zaudig, M.; Krauseneck, T.; Berberich, G.; Pollatos, O. Interoceptive deficits in patients with obsessive-compulsive disorder in the time course of cognitive-behavioral therapy. PLoS ONE 2019, 14, e0217237. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Herbert, C.; Pollatos, O. On the relationship between interoceptive awareness and alexithymia: Is interoceptive awareness related to emotional awareness? J. Pers. 2011, 79, 1149–1175. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Hall, R.; Catmur, C.; Bird, G. Alexithymia, not autism, is associated with impaired interoception. Cortex 2016, 81, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Köteles, F.; Éliás, I.; Szabolcs, Z.; Körmendi, J.; Ferentzi, E.; Szemerszky, R. Accuracy of reproduction of physical training load is not associated with resting heartbeat perception in healthy individuals. Biol. Psychol. 2020, 150, 107831. [Google Scholar] [CrossRef]
- Montgomery, W.A.; Jones, G.E.; Hollandsworth, J.G. The effects of physical fitness and exercise on cardiac awareness. Biol. Psychol. 1984, 18, 11–22. [Google Scholar] [CrossRef]
- Georgiou, E.; Matthias, E.; Kobel, S.; Kettner, S.; Dreyhaupt, J.; Steinacker, J.M.; Pollatos, O. Interaction of physical activity and interoception in children. Front. Psychol. 2015, 6, 502. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.E.; Hollandsworth, J.G. Heart Rate Discrimination Before and After Exercise-Induced Augmented Cardiac Activity. Psychophysiology 1981, 18, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Ulbrich, P.; Schandry, R. Interoceptive sensitivity and physical effort: Implications for the self-control of physical load in everyday life. Psychophysiology 2007, 44, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Ainley, V.; Tajadura-Jiménez, A.; Fotopoulou, A.; Tsakiris, M. Looking into myself: Changes in interoceptive sensitivity during mirror self-observation. Psychophysiology 2012, 49, 1504–1508. [Google Scholar] [CrossRef]
- Ainley, V.; Tsakiris, M. Body conscious? Interoceptive awareness, measured by heartbeat perception, is negatively correlated with self-objectification. PLoS ONE 2013, 8, e55568. [Google Scholar] [CrossRef]
- Pollatos, O.; Herbert, B.M.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Tsakiris, M. Atypical Self-Focus Effect on Interoceptive Accuracy in Anorexia Nervosa. Front. Hum. Neurosci. 2016, 10, 484. [Google Scholar] [CrossRef] [PubMed]
- Tsakiris, M.; Tajadura-Jiménez, A.; Costantini, M. Just a heartbeat away from one’s body: Interoceptive sensitivity predicts malleability of body-representations. Proc. Biol. Sci. 2011, 278, 2470–2476. [Google Scholar] [CrossRef] [PubMed]
- Weisz, J.; Bálazs, L.; Ádám, G. The Influence of Self-Focused Attention on Heartbeat Perception. Psychophysiology 1988, 25, 193–199. [Google Scholar] [CrossRef]
- Weineck, F.; Messner, M.; Hauke, G.; Pollatos, O. Improving interoceptive ability through the practice of power posing: A pilot study. PLoS ONE 2019, 14, e0211453. [Google Scholar] [CrossRef] [PubMed]
- Meyerholz, L.; Irzinger, J.; Witthöft, M.; Gerlach, A.L.; Pohl, A. Contingent biofeedback outperforms other methods to enhance the accuracy of cardiac interoception: A comparison of short interventions. J. Behav. Ther. Exp. Psychiatry 2019, 63, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.; Egloff, B.; Gerlach, A.L.; Witthöft, M. Improving heartbeat perception in patients with medically unexplained symptoms reduces symptom distress. Biol. Psychol. 2014, 101, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Rudrauf, D.; Damasio, A.R.; Davidson, R.J.; Lutz, A.; Tranel, D. Interoceptive awareness in experienced meditators. Psychophysiology 2008, 45, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Mirams, L.; Poliakoff, E.; Brown, R.J.; Lloyd, D.M. Brief body-scan meditation practice improves somatosensory perceptual decision making. Conscious. Cogn. 2013, 22, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.; Messner, M.; Pollatos, O. Improvement of Interoceptive Processes after an 8-Week Body Scan Intervention. Front. Hum. Neurosci. 2017, 11, 452. [Google Scholar] [CrossRef] [PubMed]
- Parkin, L.; Morgan, R.; Rosselli, A.; Howard, M.; Sheppard, A.; Evans, D.; Hawkins, A.; Martinelli, M.; Golden, A.-M.; Dalgleish, T.; et al. Exploring the Relationship Between Mindfulness and Cardiac Perception. Mindfulness 2014, 5, 298–313. [Google Scholar] [CrossRef]
- Fairclough, S.H.; Goodwin, L. The effect of psychological stress and relaxation on interoceptive accuracy: Implications for symptom perception. J. Psychosom. Res. 2007, 62, 289–295. [Google Scholar] [CrossRef]
- Melloni, M.; Sedeño, L.; Couto, B.; Reynoso, M.; Gelormini, C.; Favaloro, R.; Canales-Johnson, A.; Sigman, M.; Manes, F.; Ibanez, A. Preliminary evidence about the effects of meditation on interoceptive sensitivity and social cognition. Behav. Brain Funct. 2013, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Daubenmier, J.; Sze, J.; Kerr, C.E.; Kemeny, M.E.; Mehling, W. Follow your breath: Respiratory interoceptive accuracy in experienced meditators. Psychophysiology 2013, 50, 777–789. [Google Scholar] [CrossRef]
- Demartini, B.; Goeta, D.; Marchetti, M.; Bertelli, S.; Anselmetti, S.; Cocchi, A.; Ischia, M.; Gambini, O. The effect of a single yoga class on interoceptive accuracy in patients affected by anorexia nervosa and in healthy controls: A pilot study. Eat. Weight Disord. 2021, 26, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Finkelstein-Fox, L.; Groessl, E.J.; Elwy, A.R.; Lee, S.Y. Exploring how different types of yoga change psychological resources and emotional well-being across a single session. Complementary Ther. Med. 2020, 49, 102354. [Google Scholar] [CrossRef]
- Hendriks, T.; de Jong, J.; Cramer, H. The Effects of Yoga on Positive Mental Health Among Healthy Adults: A Systematic Review and Meta-Analysis. J. Altern. Complement. Med. 2017, 23, 505–517. [Google Scholar] [CrossRef] [PubMed]
- Hartfiel, N.; Havenhand, J.; Khalsa, S.B.; Clarke, G.; Krayer, A. The effectiveness of yoga for the improvement of well-being and resilience to stress in the workplace. Scand. J. Work Environ. Health 2011, 37, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Butzer, B.; Ahmed, K.; Khalsa, S.B.S. Yoga Enhances Positive Psychological States in Young Adult Musicians. Appl. Psychophysiol. Biofeedback 2016, 41, 191–202. [Google Scholar] [CrossRef]
- Gothe, N.P.; Khan, I.; Hayes, J.; Erlenbach, E.; Damoiseaux, J.S. Yoga Effects on Brain Health: A Systematic Review of the Current Literature. Brain Plast. 2019, 5, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Yogendra, J.; Yogendra, H.J.; Ambardekar, S.; Lele, R.D.; Shetty, S.; Dave, M.; Husein, N. Beneficial effects of yoga lifestyle on reversibility of ischaemic heart disease: Caring heart project of International Board of Yoga. J. Assoc. Physicians India 2004, 52, 283–289. [Google Scholar] [PubMed]
- Damodaran, A.; Malathi, A.; Patil, N.; Shah, N.; Suryavansihi; Marathe, S. Therapeutic potential of yoga practices in modifying cardiovascular risk profile in middle aged men and women. J. Assoc. Physicians India 2002, 50, 633–640. [Google Scholar]
- Cade, W.T.; Reeds, D.N.; Mondy, K.E.; Overton, E.T.; Grassino, J.; Tucker, S.; Bopp, C.; Laciny, E.; Hubert, S.; Lassa-Claxton, S.; et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. 2010, 11, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Michalak, J.; Steinhaus, K.; Heidenreich, T. (How) Do Therapists Use Mindfulness in Their Clinical Work? A Study on the Implementation of Mindfulness Interventions. Mindfulness 2020, 11, 401–410. [Google Scholar] [CrossRef]
- Harkess, K.N.; Delfabbro, P.; Mortimer, J.; Hannaford, Z.; Cohen-Woods, S. Brief Report on the Psychophysiological Effects of a Yoga Intervention for Chronic Stress. J. Psychophysiol. 2017, 31, 38–48. [Google Scholar] [CrossRef]
- Telles, S.; Gaur, V.; Balkrishna, A. Effect of a yoga practice session and a yoga theory session on state anxiety. Percept. Mot. Skills 2009, 109, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Yoga clinical research review. Complementary Ther. Clin. Pract. 2011, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Uebelacker, L.A.; Tremont, G.; Epstein-Lubow, G.; Gaudiano, B.A.; Gillette, T.; Kalibatseva, Z.; Miller, I.W. Open trial of Vinyasa yoga for persistently depressed individuals: Evidence of feasibility and acceptability. Behav. Modif. 2010, 34, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, D.E.; Cook, I.A.; Davydov, D.M.; Ottaviani, C.; Leuchter, A.F.; Abrams, M. Yoga as a complementary treatment of depression: Effects of traits and moods on treatment outcome. Evid. Based Complement. Alternat. Med. 2007, 4, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Sherman, K.J.; Cullum-Dugan, D.; Davis, R.B.; Phillips, R.S.; Culpepper, L. Yoga for chronic low back pain in a predominantly minority population: A pilot randomized controlled trial. Altern. Ther. Health Med. 2009, 15, 18–27. [Google Scholar] [PubMed]
- Büssing, A. German Translation of Cohen´s 10 Item Perceived Stress Scale (PSS). Available online: http://www.psy.cmu.edu/~scohen/scales.html (accessed on 27 August 2021).
- Impett, E.A.; Daubenmier, J.J.; Hirschman, A.L. Minding the body: Yoga, embodiment, and well-being. Sex. Res. Soc. Policy 2006, 3, 39–48. [Google Scholar] [CrossRef]
- Gard, T.; Noggle, J.J.; Park, C.L.; Vago, D.R.; Wilson, A. Potential self-regulatory mechanisms of yoga for psychological health. Front. Hum. Neurosci. 2014, 8, 770. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.S.; Hansen, J.S. Positive affect, negative affect, and social interaction. J. Pers. Soc. Psychol. 1996, 71, 796–809. [Google Scholar] [CrossRef]
- Narasimhan, L.; Nagarathna, R.; Nagendra, H.R. Effect of integrated yogic practices on positive and negative emotions in healthy adults. Int. J. Yoga 2011, 4, 13–19. [Google Scholar] [CrossRef]
- Vadiraja, H.S.; Rao, M.R.; Nagarathna, R.; Nagendra, H.R.; Rekha, M.; Vanitha, N.; Gopinath, K.S.; Srinath, B.S.; Vishweshwara, M.S.; Madhavi, Y.S.; et al. Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy: A randomized controlled trial. Complementary Ther. Med. 2009, 17, 274–280. [Google Scholar] [CrossRef]
- Felver, J.C.; Butzer, B.; Olson, K.J.; Smith, I.M.; Khalsa, S.B.S. Yoga in Public School Improves Adolescent Mood and Affect. Contemp. School Psychol. 2015, 19, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.; Carberry, A.; Evans, E.S.; Hall, E.E.; Nepocatych, S. The effects of power and stretch yoga on affect and salivary cortisol in women. J. Health Psychol. 2019, 24, 1658–1667. [Google Scholar] [CrossRef]
- Bershadsky, S.; Trumpfheller, L.; Kimble, H.B.; Pipaloff, D.; Yim, I.S. The effect of prenatal Hatha yoga on affect, cortisol and depressive symptoms. Complementary Ther. Clin. Pract. 2014, 20, 106–113. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Otte, C.; Geher, K.; Johnson, J.; Mohr, D.C. Effects of Hatha yoga and African dance on perceived stress, affect, and salivary cortisol. Ann. Behav. Med. 2004, 28, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Csala, B.; Ferentzi, E.; Tihanyi, B.T.; Drew, R.; Köteles, F. Verbal Cuing Is Not the Path to Enlightenment. Psychological Effects of a 10-Session Hatha Yoga Practice. Front. Psychol. 2020, 11, 1375. [Google Scholar] [CrossRef] [PubMed]
- Reed, J.; Ones, D.S. The effect of acute aerobic exercise on positive activated affect: A meta-analysis. Psychol. Sport Exerc. 2006, 7, 477–514. [Google Scholar] [CrossRef]
- Yeung, R.R. The acute effects of exercise on mood state. J. Psychosom. Res. 1996, 40, 123–141. [Google Scholar] [CrossRef]
- Liao, Y.; Shonkoff, E.T.; Dunton, G.F. The Acute Relationships Between Affect, Physical Feeling States, and Physical Activity in Daily Life: A Review of Current Evidence. Front. Psychol. 2015, 6, 1975. [Google Scholar] [CrossRef]
- Ludwick-Rosenthal, R.; Neufeld, R.W. Heart beat interoception: A study of individual differences. Int. J. Psychophysiol. 1985, 3, 57–65. [Google Scholar] [CrossRef]
- Murphy, J.; Millgate, E.; Geary, H.; Ichijo, E.; Coll, M.-P.; Brewer, R.; Catmur, C.; Bird, G. Knowledge of resting heart rate mediates the relationship between intelligence and the heartbeat counting task. Biol. Psychol. 2018, 133, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Grabauskaitė, A.; Baranauskas, M.; Griškova-Bulanova, I. Interoception and gender: What aspects should we pay attention to? Conscious. Cogn. 2017, 48, 129–137. [Google Scholar] [CrossRef]
- Koch, A.; Pollatos, O. Interoceptive sensitivity, body weight and eating behavior in children: A prospective study. Front. Psychol. 2014, 5, 1003. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Pollatos, O. Attenuated interoceptive sensitivity in overweight and obese individuals. Eat. Behav. 2014, 15, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Schandry, R.; Bestler, M.; Montoya, P. On the relation between cardiodynamics and heartbeat perception. Psychophysiology 1993, 30, 467–474. [Google Scholar] [CrossRef]
- G* Power 3.1.9 [App]; Heinrich-Heine-Universität Düsseldorf: Düsseldorf, Germany, 2014.
- Frey, I.; Berg, A.; Grathwohl, D.; Keul, J. Freiburger Fragebogen zur körperlichen Aktivität--Entwicklung, Prüfung und Anwendung. Soz. Praventivmed. 1999, 44, 55–64. [Google Scholar] [CrossRef]
- Krohne, H.W.; Egloff, B.; Kohlmann, C.-W.; Tausch, A. Untersuchungen mit einer deutschen Version der “Positive and Negative Affect Schedule” (PANAS). Diagnostica 1996, 42, 139–156. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed]
- Frey, I.; Berg, A. Physical activity counseling: Assessment of physical activity by questionnaire. Eur. J. Sport Sci. 2002, 2, 1–6. [Google Scholar] [CrossRef]
- Desmedt, O.; Corneille, O.; Luminet, O.; Murphy, J.; Bird, G.; Maurage, P. Contribution of Time Estimation and Knowledge to Heartbeat Counting Task Performance under Original and Adapted Instructions. Biol. Psychol. 2020, 154, 107904. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Jakovljevic, D.G.; Donovan, G.; Hodges, L.D.; Sandercock, G.R.H.; Brodie, D.A. Levels of agreement for RR intervals and short-term heart rate variability obtained from the Polar S810 and an alternative system. Eur. J. Appl. Physiol. 2008, 103, 529–537. [Google Scholar] [CrossRef]
- Kingsley, M.; Lewis, M.J.; Marson, R.E. Comparison of Polar 810s and an ambulatory ECG system for RR interval measurement during progressive exercise. Int. J. Sports Med. 2005, 26, 39–44. [Google Scholar] [CrossRef]
- Herbert, B.M.; Pollatos, O. Interozeptive Sensitivität, Gefühle und Verhaltensregulation [Interoceptive sensitivity, feelings and behavorial control]. Z. Für Neuropsychol. 2008, 19, 125–137. [Google Scholar] [CrossRef]
- Cameron, O.G. Interoception: The Inside Story—A Model for Psychosomatic Processes. Psychosom. Med. 2001, 63, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Zaki, J.; Davis, J.I.; Ochsner, K.N. Overlapping activity in anterior insula during interoception and emotional experience. Neuroimage 2012, 62, 493–499. [Google Scholar] [CrossRef]
- Pollatos, O.; Schandry, R. Accuracy of heartbeat perception is reflected in the amplitude of the heartbeat-evoked brain potential. Psychophysiology 2004, 41, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action From a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Farb, N.A.S.; Segal, Z.V.; Anderson, A.K. Mindfulness meditation training alters cortical representations of interoceptive attention. Soc. Cogn. Affect. Neurosci. 2013, 8, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Werner, N.S.; Kerschreiter, R.; Kindermann, N.K.; Duschek, S. Interoceptive Awareness as a Moderator of Affective Responses to Social Exclusion. J. Psychophysiol. 2013, 27, 39–50. [Google Scholar] [CrossRef]
- Weiss, S.; Sack, M.; Henningsen, P.; Pollatos, O. On the interaction of self-regulation, interoception and pain perception. Psychopathology 2014, 47, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Schultchen, D.; Bayer, J.; Kühnel, J.; Melchers, K.G.; Pollatos, O. Interoceptive accuracy is related to long-term stress via self-regulation. Psychophysiology 2019, 56, e13429. [Google Scholar] [CrossRef]
- Pollatos, O.; Matthias, E.; Keller, J. When interoception helps to overcome negative feelings caused by social exclusion. Front. Psychol. 2015, 6, 786. [Google Scholar] [CrossRef] [PubMed]
- Short, M.M.; Mazmanian, D.; Oinonen, K.; Mushquash, C.J. Executive function and self-regulation mediate dispositional mindfulness and well-being. Personal. Individ. Differ. 2016, 93, 97–103. [Google Scholar] [CrossRef]
- Walsh, K.M.; Saab, B.J.; Farb, N.A.S. Effects of a Mindfulness Meditation App on Subjective Well-Being: Active Randomized Controlled Trial and Experience Sampling Study. JMIR Ment. Health 2019, 6, e10844. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Herbert, B.M.; Mai, S.; Kammer, T. Changes in interoceptive processes following brain stimulation. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20160016. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.; van Staeyen, K.; Vögele, C.; von Leupoldt, A.; van den Bergh, O. Interoception and symptom reporting: Disentangling accuracy and bias. Front. Psychol. 2015, 6, 732. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, S.N.; Tiley, C.; O’Keeffe, S.; Harrison, N.A.; Seth, A.K.; Critchley, H.D. Discrepancies between dimensions of interoception in autism: Implications for emotion and anxiety. Biol. Psychol. 2016, 114, 117–126. [Google Scholar] [CrossRef]
- Wittkamp, M.F.; Bertsch, K.; Vögele, C.; Schulz, A. A latent state-trait analysis of interoceptive accuracy. Psychophysiol. 2018, 55, e13055. [Google Scholar] [CrossRef]
- Murphy, J.; Brewer, R.; Plans, D.; Khalsa, S.S.; Catmur, C.; Bird, G. Validation of the Interoceptive Accuracy scale (IAS) Supports Distinction between Self-Reported Interoceptive Accuracy and Awareness, 2018, Preprint. Available online: https://osf.io/fgjuw/download/?version=2&displayName=IAS%20MS%20Final-2018-10-07T15%3A01%3A00.739Z.pdf (accessed on 22 October 2021).
- Ring, C.; Brener, J. Heartbeat counting is unrelated to heartbeat detection: A comparison of methods to quantify interoception. Psychophysiology 2018, 55, e13084. [Google Scholar] [CrossRef] [PubMed]
- Zamariola, G.; Maurage, P.; Luminet, O.; Corneille, O. Interoceptive accuracy scores from the heartbeat counting task are problematic: Evidence from simple bivariate correlations. Biol. Psychol. 2018, 137, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Desmedt, O.; Luminet, O.; Corneille, O. The heartbeat counting task largely involves non-interoceptive processes: Evidence from both the original and an adapted counting task. Biol. Psychol. 2018, 138, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Zimprich, D.; Nusser, L.; Pollatos, O. Are interoceptive accuracy scores from the heartbeat counting task problematic? A comment on Zamariola et al. (2018). Biol. Psychol. 2020, 152, 107868. [Google Scholar] [CrossRef] [PubMed]
- Ainley, V.; Tsakiris, M.; Pollatos, O.; Schulz, A.; Herbert, B.M. Comment on “Zamariola et al. (2018), Interoceptive Accuracy Scores are Problematic: Evidence from Simple Bivariate Correlations”-The empirical data base, the conceptual reasoning and the analysis behind this statement are misconceived and do not support the authors’ conclusions. Biol. Psychol. 2020, 152, 107870. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Vögele, C. Interoception and stress. Front. Psychol. 2015, 6, 993. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Catmur, C.; Bird, G. Classifying individual differences in interoception: Implications for the measurement of interoceptive awareness. Psychon. Bull. Rev. 2019, 26, 1467–1471. [Google Scholar] [CrossRef]
- Schultchen, D.; Reichenberger, J.; Mittl, T.; Weh, T.R.M.; Smyth, J.M.; Blechert, J.; Pollatos, O. Bidirectional relationship of stress and affect with physical activity and healthy eating. Br. J. Health Psychol. 2019, 24, 315–333. [Google Scholar] [CrossRef] [PubMed]
- Reichenberger, J.; Richard, A.; Smyth, J.M.; Fischer, D.; Pollatos, O.; Blechert, J. It’s craving time: Time of day effects on momentary hunger and food craving in daily life. Nutrition 2018, 55–56, 15–20. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Yoga Group | Endurance Group | Control Group | |||
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | F (2, 134) | p | |
| Age | 24.11 (4.44) | 23.89 (4.02) | 23.09 (3.33) | 0.82 | 0.443 |
| BMI | 22.65 (3.12) | 22.69 (4.23) | 23.55 (5.06) | 0.67 | 0.516 |
| Positive Affect | 3.01 (0.63) | 3.07 (0.59) | 2.78 (0.52) | 3.05 | 0.051 |
| Negative Affect | 1.24 (0.27) | 1.51 (0.66) | 1.28 (0.33) | 4.7 | 0.011 |
| Cardiac IAc | 0.65 (.20) | 0.72 (0.16) | 0.65 (0.16) | 2.48 | 0.089 |
| Yoga Group | Endurance Group | Control Group | df | Χ2 | p | |
|---|---|---|---|---|---|---|
| Sex | 2 | 2.63 | 0.269 | |||
| Male | 17 | 17 | 10 | |||
| Female | 30 | 29 | 34 | |||
| Physical Activity level | 4 | 5.16 | 0.272 | |||
| Low | 12 | 16 | 14 | |||
| Moderate | 13 | 17 | 18 | |||
| High | 22 | 13 | 12 |
| R | R2 | Corr. R2 | SE |
|---|---|---|---|
| 0.827 | 0.684 | 0.669 | 0.118 |
| Independent Variable | Standardized Beta | SE | t | p | 95% CI Lower Limit | 95% CI Upper Limit |
|---|---|---|---|---|---|---|
| Cardiac | 0.797 | 0.086 | 9.287 | <0.001 | 0.626 | 0.973 |
| IAc (baseline) | ||||||
| Change in positive affect | 0.186 | 0.034 | 2.173 | 0.035 | 0.005 | 0.143 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schillings, C.; Schultchen, D.; Pollatos, O. Effects of a Single Yoga Session on Cardiac Interoceptive Accuracy and Emotional Experience. Brain Sci. 2021, 11, 1572. https://doi.org/10.3390/brainsci11121572
Schillings C, Schultchen D, Pollatos O. Effects of a Single Yoga Session on Cardiac Interoceptive Accuracy and Emotional Experience. Brain Sciences. 2021; 11(12):1572. https://doi.org/10.3390/brainsci11121572
Chicago/Turabian StyleSchillings, Christine, Dana Schultchen, and Olga Pollatos. 2021. "Effects of a Single Yoga Session on Cardiac Interoceptive Accuracy and Emotional Experience" Brain Sciences 11, no. 12: 1572. https://doi.org/10.3390/brainsci11121572
APA StyleSchillings, C., Schultchen, D., & Pollatos, O. (2021). Effects of a Single Yoga Session on Cardiac Interoceptive Accuracy and Emotional Experience. Brain Sciences, 11(12), 1572. https://doi.org/10.3390/brainsci11121572