
King-Devick Test Performance and Cognitive Dysfunction after Concussion: A Pilot Eye Movement Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials and Procedures
2.2.1. KD Test and Eye Tracking
2.2.2. Neuropsychological Assessment
2.3. Data Analyses
3. Results
3.1. KD Times and ISI Values
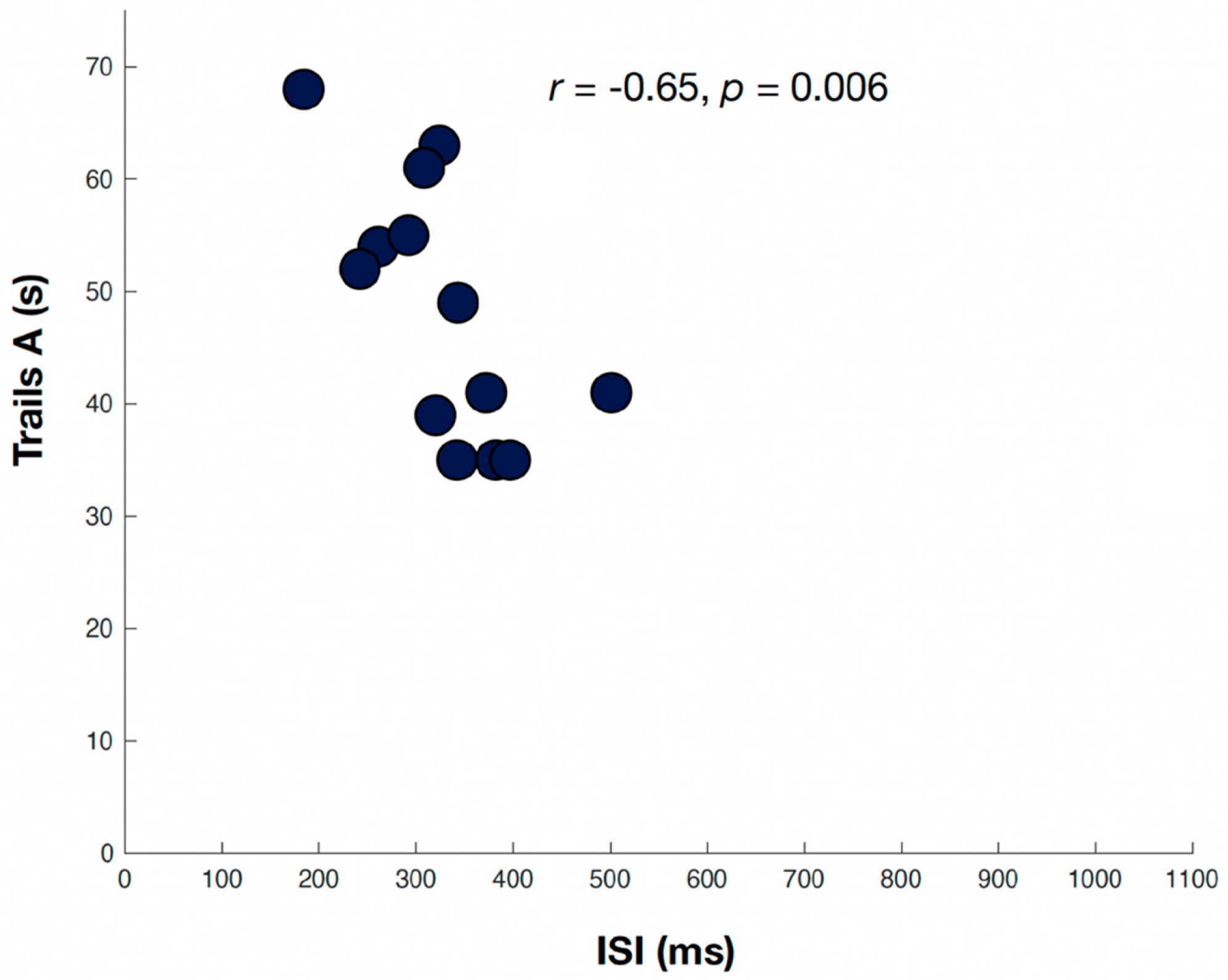
3.2. ISI and Neuropsychological Assessments
4. Discussion
4.1. Eye Tracking and Neuropsychological Assessment in Concussion
4.2. Interactions between KD Performance and Neuropsychological Assessments
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davis, G.A.; Ellenbogen, R.G.; Bailes, J.; Cantu, R.C.; Johnston, K.M.; Manley, G.T.; Nagahiro, S.; Sills, A.; Tator, C.H.; McCrory, P. The Berlin International Consensus Meeting on Concussion in Sport. Neurosurgery 2018, 82, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Hiploylee, C.; Dufort, P.A.; Davis, H.S.; Wennberg, R.A.; Tartaglia, M.C.; Mikulis, D.; Hazrati, L.N.; Tator, C.H. Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers. J. Neurotrauma 2017, 34, 1511–1523. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J.D.; Cancelliere, C.; Carroll, L.J.; Cote, P.; Hincapie, C.A.; Holm, L.W.; Hartvigsen, J.; Donovan, J.; Nygren-de Boussard, C.; Kristman, V.L.; et al. Systematic review of self-reported prognosis in adults after mild traumatic brain injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95, S132–S151. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaney, J.S.; Lamfookon, C.; Bloom, G.A.; Al-Kashmiri, A.; Correa, J.A. Why university athletes choose not to reveal their concussion symptoms during a practice or game. Clin. J. Sport Med. 2015, 25, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Kerr, Z.Y.; Register-Mihalik, J.K.; Kroshus, E.; Baugh, C.M.; Marshall, S.W. Motivations Associated With Nondisclosure of Self-Reported Concussions in Former Collegiate Athletes. Am. J. Sports Med. 2016, 44, 220–225. [Google Scholar] [CrossRef] [Green Version]
- Kerr, Z.Y.; Register-Mihalik, J.K.; Marshall, S.W.; Evenson, K.R.; Mihalik, J.P.; Guskiewicz, K.M. Disclosure and non-disclosure of concussion and concussion symptoms in athletes: Review and application of the socio-ecological framework. Brain Inj. 2014, 28, 1009–1021. [Google Scholar] [CrossRef]
- Conway, F.N.; Domingues, M.; Monaco, R.; Lesnewich, L.M.; Ray, A.E.; Alderman, B.L.; Todaro, S.M.; Buckman, J.F. Concussion Symptom Underreporting Among Incoming National Collegiate Athletic Association Division I College Athletes. Clin. J. Sport Med. 2020, 30, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Torres, D.M.; Galetta, K.M.; Phillips, H.W.; Dziemianowicz, E.M.; Wilson, J.A.; Dorman, E.S.; Laudano, E.; Galetta, S.L.; Balcer, L.J. Sports-related concussion: Anonymous survey of a collegiate cohort. Neurol. Clin. Pract. 2013, 3, 279–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, J.K.; Phelps, R.R.L.; Chandra, A.; Winkler, E.A.; Manley, G.T.; Berger, M.S. Sideline Concussion Assessment: The Current State of the Art. Neurosurgery 2020, 87, 466–475. [Google Scholar] [CrossRef] [PubMed]
- McCrory, P.; Johnston, K.; Meeuwisse, W.; Aubry, M.; Cantu, R.; Dvorak, J.; Graf-Baumann, T.; Kelly, J.; Lovell, M.; Schamasch, P. Summary and agreement statement of the 2nd International Conference on Concussion in Sport, Prague 2004. Br. J. Sports Med. 2005, 39, 196–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echemendia, R.J.; Meeuwisse, W.; McCrory, P.; Davis, G.A.; Putukian, M.; Leddy, J.; Makdissi, M.; Sullivan, S.J.; Broglio, S.P.; Raftery, M.; et al. The Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and rationale. Br. J. Sports Med. 2017, 51, 848–850. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Kelly, J.P.; Kluge, J.; Ackley, B.; Randolph, C. Standardized assessment of concussion in football players. Neurology 1997, 48, 586–588. [Google Scholar] [CrossRef] [Green Version]
- McCrory, P.; Meeuwisse, W.; Johnston, K.; Dvorak, J.; Aubry, M.; Molloy, M.; Cantu, R. Consensus Statement on Concussion in Sport: The 3rd International Conference on Concussion in Sport held in Zurich, November 2008. Br. J. Sports Med. 2009, 43 (Suppl. 1), i76–i90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucha, A.; Collins, M.W.; Elbin, R.J.; Furman, J.M.; Troutman-Enseki, C.; DeWolf, R.M.; Marchetti, G.; Kontos, A.P. A Brief Vestibular/Ocular Motor Screening (VOMS) assessment to evaluate concussions: Preliminary findings. Am. J. Sports Med. 2014, 42, 2479–2486. [Google Scholar] [CrossRef] [PubMed]
- Galetta, K.M.; Liu, M.; Leong, D.F.; Ventura, R.E.; Galetta, S.L.; Balcer, L.J. The King-Devick test of rapid number naming for concussion detection: Meta-analysis and systematic review of the literature. Concussion 2016, 1, CNC8. [Google Scholar] [CrossRef] [Green Version]
- Fallon, S.; Akhand, O.; Hernandez, C.; Galetta, M.S.; Hasanaj, L.; Martone, J.; Webb, N.; Drattell, J.; Amorapanth, P.; Rizzo, J.R.; et al. MULES on the sidelines: A vision-based assessment tool for sports-related concussion. J. Neurol. Sci. 2019, 402, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Thurman, D.J.; Alverson, C.; Dunn, K.A.; Guerrero, J.; Sniezek, J.E. Traumatic brain injury in the United States: A public health perspective. J. Head Trauma Rehabil. 1999, 14, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Kyle Harrold, G.; Hasanaj, L.; Moehringer, N.; Zhang, I.; Nolan, R.; Serrano, L.; Raynowska, J.; Rucker, J.C.; Flanagan, S.R.; Cardone, D.; et al. Rapid sideline performance meets outpatient clinic: Results from a multidisciplinary concussion center registry. J. Neurol. Sci. 2017, 379, 312–317. [Google Scholar] [CrossRef]
- King, D.; Clark, T.; Gissane, C. Use of a rapid visual screening tool for the assessment of concussion in amateur rugby league: A pilot study. J. Neurol. Sci. 2012, 320, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Galetta, K.M.; Barrett, J.; Allen, M.; Madda, F.; Delicata, D.; Tennant, A.T.; Branas, C.C.; Maguire, M.G.; Messner, L.V.; Devick, S.; et al. The King-Devick test as a determinant of head trauma and concussion in boxers and MMA fighters. Neurology 2011, 76, 1456–1462. [Google Scholar] [CrossRef] [Green Version]
- Galetta, K.M.; Brandes, L.E.; Maki, K.; Dziemianowicz, M.S.; Laudano, E.; Allen, M.; Lawler, K.; Sennett, B.; Wiebe, D.; Devick, S.; et al. The King-Devick test and sports-related concussion: Study of a rapid visual screening tool in a collegiate cohort. J. Neurol. Sci. 2011, 309, 34–39. [Google Scholar] [CrossRef]
- Galetta, M.S.; Galetta, K.M.; McCrossin, J.; Wilson, J.A.; Moster, S.; Galetta, S.L.; Balcer, L.J.; Dorshimer, G.W.; Master, C.L. Saccades and memory: Baseline associations of the King-Devick and SCAT2 SAC tests in professional ice hockey players. J. Neurol. Sci. 2013, 328, 28–31. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Gissane, C.; Hume, P.A.; Flaws, M. The King-Devick test was useful in management of concussion in amateur rugby union and rugby league in New Zealand. J. Neurol. Sci. 2015, 351, 58–64. [Google Scholar] [CrossRef]
- King, D.; Hume, P.; Gissane, C.; Clark, T. Use of the King-Devick test for sideline concussion screening in junior rugby league. J. Neurol. Sci. 2015, 357, 75–79. [Google Scholar] [CrossRef]
- Rizzo, J.-R.; Hudson, T.E.; Dai, W.; Birkemeier, J.; Pasculli, R.M.; Selesnick, I.; Balcer, L.J.; Galetta, S.L.; Rucker, J.C. Rapid number naming in chronic concussion: Eye movements in the King-Devick test. Ann. Clin. Transl. Neurol. 2016, 3, 801–811. [Google Scholar] [CrossRef]
- Denning, J.H. The efficiency and accuracy of the Test of Memory Malingering trial 1, errors on the first 10 items of the test of memory malingering, and five embedded measures in predicting invalid test performance. Arch. Clin. Neuropsychol. 2012, 27, 417–432. [Google Scholar] [CrossRef]
- Oride, M.K.; Marutani, J.K.; Rouse, M.W.; DeLand, P.N. Reliability study of the Pierce and King-Devick saccade tests. Am. J. Optom. Physiol. Opt. 1986, 63, 419–424. [Google Scholar] [CrossRef]
- Rizzo, J.-R.; Hudson, T.E.; Dai, W.; Desai, N.; Yousefi, A.; Palsana, D.; Selesnick, I.; Balcer, L.J.; Galetta, S.L.; Rucker, J.C. Objectifying eye movements during rapid number naming: Methodology for assessment of normative data for the King-Devick test. J. Neurol. Sci. 2016, 362, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Donders, J.; Strong, C.A. Clinical utility of the Wechsler Adult Intelligence Scale-Fourth Edition after traumatic brain injury. Assessment 2015, 22, 17–22. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef]
- Dai, W.; Selesnick, I.; Rizzo, J.R.; Rucker, J.; Hudson, T. A nonlinear generalization of the Savitzky-Golay filter and the quantitative analysis of saccades. J. Vis. 2017, 17, 10. [Google Scholar] [CrossRef]
- Ventura, R.E.; Balcer, L.J.; Galetta, S.L.; Rucker, J.C. Ocular motor assessment in concussion: Current status and future directions. J. Neurol. Sci. 2016, 361, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhand, O.; Balcer, L.J.; Galetta, S.L. Assessment of vision in concussion. Curr. Opin. Neurol. 2019, 32, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Akhand, O.; Rizzo, J.R.; Rucker, J.C.; Hasanaj, L.; Galetta, S.L.; Balcer, L.J. History and Future Directions of Vision Testing in Head Trauma. J. Neuroophthalmol. 2019, 39, 68–81. [Google Scholar] [CrossRef]
- Barton, J.J.S.; Ranalli, P.J. Vision Therapy: Ocular Motor Training in Mild Traumatic Brain Injury. Ann. Neurol. 2020, 88, 453–461. [Google Scholar] [CrossRef]
- Rucker, J.C.; Rizzo, J.R.; Hudson, T.E.; Balcer, L.J.; Galetta, S.L. Concerning Vision Therapy and Ocular Motor Training in Mild Traumatic Brain Injury. Ann. Neurol. 2020, 88, 1053–1054. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.J.S.; Ranalli, P.J. Reply to “Concerning Vision Therapy and Ocular Motor Training in Mild TBI”. Ann. Neurol. 2020, 88, 1054–1055. [Google Scholar] [CrossRef]
- Leigh, R.J.; Zee, D.S. The Neurology of Eye Movements, 5th ed.; Oxford University Press: Oxford, UK; New York, NY, USA, 2015; 1109p. [Google Scholar]
- Heitger, M.H.; Anderson, T.J.; Jones, R.D.; Dalrymple-Alford, J.C.; Frampton, C.M.; Ardagh, M.W. Eye movement and visuomotor arm movement deficits following mild closed head injury. Brain 2004, 127, 575–590. [Google Scholar] [CrossRef]
- Kraus, M.F.; Little, D.M.; Donnell, A.J.; Reilly, J.L.; Simonian, N.; Sweeney, J.A. Oculomotor function in chronic traumatic brain injury. Cogn. Behav. Neurol. 2007, 20, 170–178. [Google Scholar] [CrossRef]
- Heitger, M.H.; Jones, R.D.; Macleod, A.D.; Snell, D.L.; Frampton, C.M.; Anderson, T.J. Impaired eye movements in post-concussion syndrome indicate suboptimal brain function beyond the influence of depression, malingering or intellectual ability. Brain 2009, 132, 2850–2870. [Google Scholar] [CrossRef] [PubMed]
- Clough, M.; Mutimer, S.; Wright, D.K.; Tsang, A.; Costello, D.M.; Gardner, A.J.; Stanwell, P.; Mychasiuk, R.; Sun, M.; Brady, R.D.; et al. Oculomotor Cognitive Control Abnormalities in Australian Rules Football Players with a History of Concussion. J. Neurotrauma 2018, 35, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Wetzel, P.A.; Lindblad, A.S.; Raizada, H.; James, N.; Mulatya, C.; Kannan, M.A.; Villamar, Z.; Gitchel, G.T.; Weaver, L.K. Eye Tracking Results in Postconcussive Syndrome Versus Normative Participants. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4011–4019. [Google Scholar] [CrossRef]
- Webb, B.; Humphreys, D.; Heath, M. Oculomotor Executive Dysfunction during the Early and Later Stages of Sport-Related Concussion Recovery. J. Neurotrauma 2018, 35, 1874–1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matuseviciene, G.; Johansson, J.; Moller, M.; Godbolt, A.K.; Pansell, T.; Deboussard, C.N. Longitudinal changes in oculomotor function in young adults with mild traumatic brain injury in Sweden: An exploratory prospective observational study. BMJ Open 2018, 8, e018734. [Google Scholar] [CrossRef] [Green Version]
- Pearson, B.C.; Armitage, K.R.; Horner, C.W.; Carpenter, R.H. Saccadometry: The possible application of latency distribution measurement for monitoring concussion. Br. J. Sports Med. 2007, 41, 610–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane, G.D.; Christy, J.B.; Almutairi, A.; Busettini, C.; Swanson, M.W.; Weise, K.K. Visuo-oculomotor Function and Reaction Times in Athletes with and without Concussion. Optom. Vis. Sci. 2019, 96, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Levin, H.S.; Williams, D.H.; Eisenberg, H.M.; High, W.M., Jr.; Guinto, F.C., Jr. Serial MRI and neurobehavioural findings after mild to moderate closed head injury. J. Neurol. Neurosurg. Psychiatry 1992, 55, 255–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crevits, L.; Hanse, M.C.; Tummers, P.; Van Maele, G. Antisaccades and remembered saccades in mild traumatic brain injury. J. Neurol. 2000, 247, 179–182. [Google Scholar] [CrossRef]
- Heitger, M.H.; Anderson, T.J.; Jones, R.D. Saccade sequences as markers for cerebral dysfunction following mild closed head injury. Prog. Brain Res. 2002, 140, 433–448. [Google Scholar] [CrossRef] [PubMed]
- Heitger, M.H.; Jones, R.D.; Dalrymple-Alford, J.C.; Frampton, C.M.; Ardagh, M.W.; Anderson, T.J. Motor deficits and recovery during the first year following mild closed head injury. Brain Inj. 2006, 20, 807–824. [Google Scholar] [CrossRef]
- Johnson, B.; Hallett, M.; Slobounov, S. Follow-up evaluation of oculomotor performance with fMRI in the subacute phase of concussion. Neurology 2015, 85, 1163–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, W.K.; Schweizer, T.A.; Topolovec-Vranic, J.; Cusimano, M.D. Antisaccadic Eye Movements Are Correlated with Corpus Callosum White Matter Mean Diffusivity, Stroop Performance, and Symptom Burden in Mild Traumatic Brain Injury and Concussion. Front. Neurol. 2015, 6, 271. [Google Scholar] [CrossRef] [Green Version]
- Iverson, G.L.; Lange, R.T.; Brooks, B.L.; Rennison, V.L. “Good old days” bias following mild traumatic brain injury. Clin. Neuropsychol. 2010, 24, 17–37. [Google Scholar] [CrossRef] [PubMed]
- Rohling, M.L.; Binder, L.M.; Demakis, G.J.; Larrabee, G.J.; Ploetz, D.M.; Langhinrichsen-Rohling, J. A meta-analysis of neuropsychological outcome after mild traumatic brain injury: Re-analyses and reconsiderations of Binder et al., (1997), Frencham et al., (2005), and Pertab et al., (2009). Clin. Neuropsychol. 2011, 25, 608–623. [Google Scholar] [CrossRef]
- Schretlen, D.J.; Shapiro, A.M. A quantitative review of the effects of traumatic brain injury on cognitive functioning. Int. Rev. Psychiatry 2003, 15, 341–349. [Google Scholar] [CrossRef]
- Carney, N.; Ghajar, J.; Jagoda, A.; Bedrick, S.; Davis-O’Reilly, C.; du Coudray, H.; Hack, D.; Helfand, N.; Huddleston, A.; Nettleton, T.; et al. Concussion guidelines step 1: Systematic review of prevalent indicators. Neurosurgery 2014, 75 (Suppl. 1), S3–S15. [Google Scholar] [CrossRef] [Green Version]
- Pierrot-Deseilligny, C.; Muri, R.M.; Ploner, C.J.; Gaymard, B.; Demeret, S.; Rivaud-Pechoux, S. Decisional role of the dorsolateral prefrontal cortex in ocular motor behaviour. Brain 2003, 126, 1460–1473. [Google Scholar] [CrossRef] [Green Version]
- Bari, S.; Svaldi, D.O.; Jang, I.; Shenk, T.E.; Poole, V.N.; Lee, T.; Dydak, U.; Rispoli, J.V.; Nauman, E.A.; Talavage, T.M. Dependence on subconcussive impacts of brain metabolism in collision sport athletes: An MR spectroscopic study. Brain Imaging Behav. 2018, 13, 735–749. [Google Scholar] [CrossRef]
- Subotic, A.; Ting, W.K.; Cusimano, M.D. Characteristics of the King-Devick test in the assessment of concussed patients in the subacute and later stages after injury. PLoS ONE 2017, 12, e0183092. [Google Scholar] [CrossRef] [Green Version]
- Drew, A.S.; Langan, J.; Halterman, C.; Osternig, L.R.; Chou, L.S.; van Donkelaar, P. Attentional disengagement dysfunction following mTBI assessed with the gap saccade task. Neurosci. Lett. 2007, 417, 61–65. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Participant | Age (at Eye Movement Visit) | Sex * | Neuropsychological Testing (Relative to Most Recent Concussion) | Eye Movement Recording (Relative to Most Recent Concussion) |
|---|---|---|---|---|
| 1 | 28 | M | 7 months | 6 months |
| 2 | 28 | M | >24 months (2013—11/2015) | >24 months (2013—9/2015) |
| 3 | 50 | F | 3 months | 4 months |
| 4 | 61 | M | 29 months | 30 months |
| 5 | 47 | M | 4 months | 7 months |
| 6 | 32 | F | 18 months | 17 months |
| 7 | 47 | F | 1 month | 19 months |
| 8 | 57 | F | 10 months | 13 months |
| 9 | 32 | M | >24 months (2009—8/2016) | >24 months (2009—6/2016) |
| 10 | 38 | F | 2 months | 5 months |
| 11 | 34 | M | 1 month | 2 weeks |
| 12 | 34 | F | 8 months | 6 months |
| 13 | 30 | M | 8 months | 8 months |
| 14 | 24 | M | 4 months | 4 months |
| Cognitive Domain | Test * |
|---|---|
| Processing Speed | SCWT Word; SCWT Color; WAIS-IV Coding |
| Attention/Working Memory | WAIS-IV (Digit Span Forward; Digit Span Backward; Digit Span Sequencing; Digit Span Total); TMTA |
| Perceptual Reasoning | WASI-II Matrix Reasoning |
| Executive Functioning | SCWT Interference; TMTB |
| Emotional Functioning | BAI; BDI-II |
| Subject | Trail Making Test A (T-Score) | Digit Span Forward (SS) | Digit Span Backward (SS) | Digit Span Total (SS) | SCWT Interference (T-Score) | WAIS-IV Coding (SS) |
|---|---|---|---|---|---|---|
| 1 | 76 | 9 | 8 | 9 | 51 | 15 |
| 2 | 68 | 11 | 14 | 12 | 60 | 10 |
| 3 | 35 | 10 | 13 | 11 | 51 | 6 |
| 4 | 35 | 5 | 7 | 5 | 42 | 5 |
| 5 | 54 | 10 | 14 | 12 | 46 | 15 |
| 6 | 63 | 12 | 10 | 10 | 56 | 9 |
| 7 | 55 | 11 | 8 | 12 | 50 | 12 |
| 8 | 41 | 11 | 8 | 9 | 50 | 8 |
| 9 | 52 | 12 | 14 | 13 | 67 | 16 |
| 10 | 35 | 8 | 10 | 8 | 57 | 11 |
| 11 | 61 | 12 | 12 | 14 | 52 | 11 |
| 12 | 41 | 8 | 10 | 9 | 59 | 6 |
| 13 | 39 | 12 | 12 | 12 | 54 | 10 |
| 14 | 49 | 9 | 10 | 11 | 49 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gold, D.M.; Rizzo, J.-R.; Lee, Y.S.C.; Childs, A.; Hudson, T.E.; Martone, J.; Matsuzawa, Y.K.; Fraser, F.; Ricker, J.H.; Dai, W.; et al. King-Devick Test Performance and Cognitive Dysfunction after Concussion: A Pilot Eye Movement Study. Brain Sci. 2021, 11, 1571. https://doi.org/10.3390/brainsci11121571
Gold DM, Rizzo J-R, Lee YSC, Childs A, Hudson TE, Martone J, Matsuzawa YK, Fraser F, Ricker JH, Dai W, et al. King-Devick Test Performance and Cognitive Dysfunction after Concussion: A Pilot Eye Movement Study. Brain Sciences. 2021; 11(12):1571. https://doi.org/10.3390/brainsci11121571
Chicago/Turabian StyleGold, Doria M., John-Ross Rizzo, Yuen Shan Christine Lee, Amanda Childs, Todd E. Hudson, John Martone, Yuka K. Matsuzawa, Felicia Fraser, Joseph H. Ricker, Weiwei Dai, and et al. 2021. "King-Devick Test Performance and Cognitive Dysfunction after Concussion: A Pilot Eye Movement Study" Brain Sciences 11, no. 12: 1571. https://doi.org/10.3390/brainsci11121571
APA StyleGold, D. M., Rizzo, J.-R., Lee, Y. S. C., Childs, A., Hudson, T. E., Martone, J., Matsuzawa, Y. K., Fraser, F., Ricker, J. H., Dai, W., Selesnick, I., Balcer, L. J., Galetta, S. L., & Rucker, J. C. (2021). King-Devick Test Performance and Cognitive Dysfunction after Concussion: A Pilot Eye Movement Study. Brain Sciences, 11(12), 1571. https://doi.org/10.3390/brainsci11121571