
Caring for a Relative with Dementia: Determinants and Gender Differences of Caregiver Burden in the Rural Setting

 ,
,
Abstract
:1. Introduction
1.1. Family Caregiver and Caregiver Burden
1.2. Gender and Caregiver Burden
1.3. The Rural Setting
2. Materials and Methods
2.1. Sampling
2.2. Instruments
2.3. Analysis
3. Results
4. Discussion
4.1. Gender Aspects
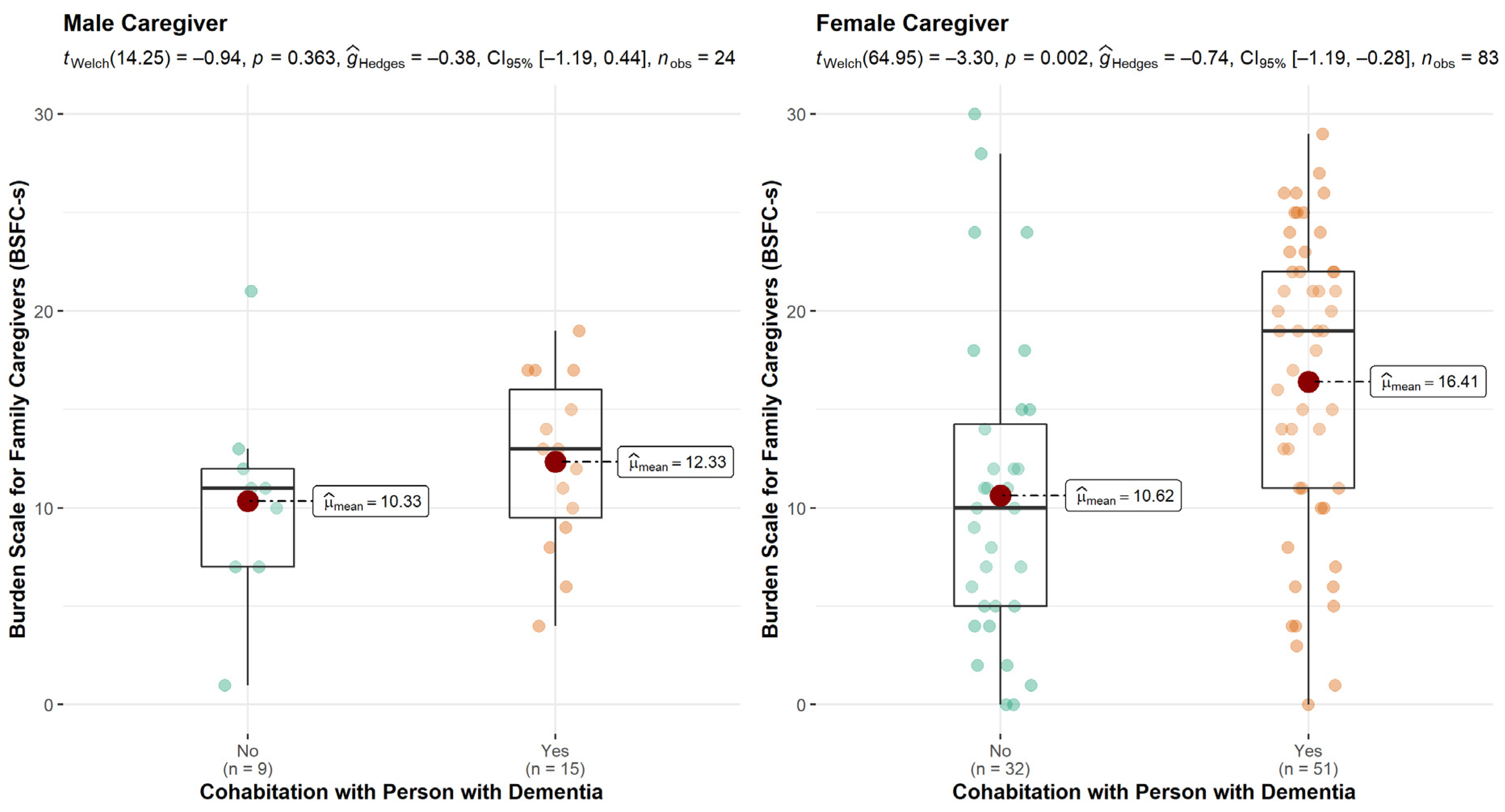
4.2. Effects of Kinship and Cohabititation
4.3. Employment
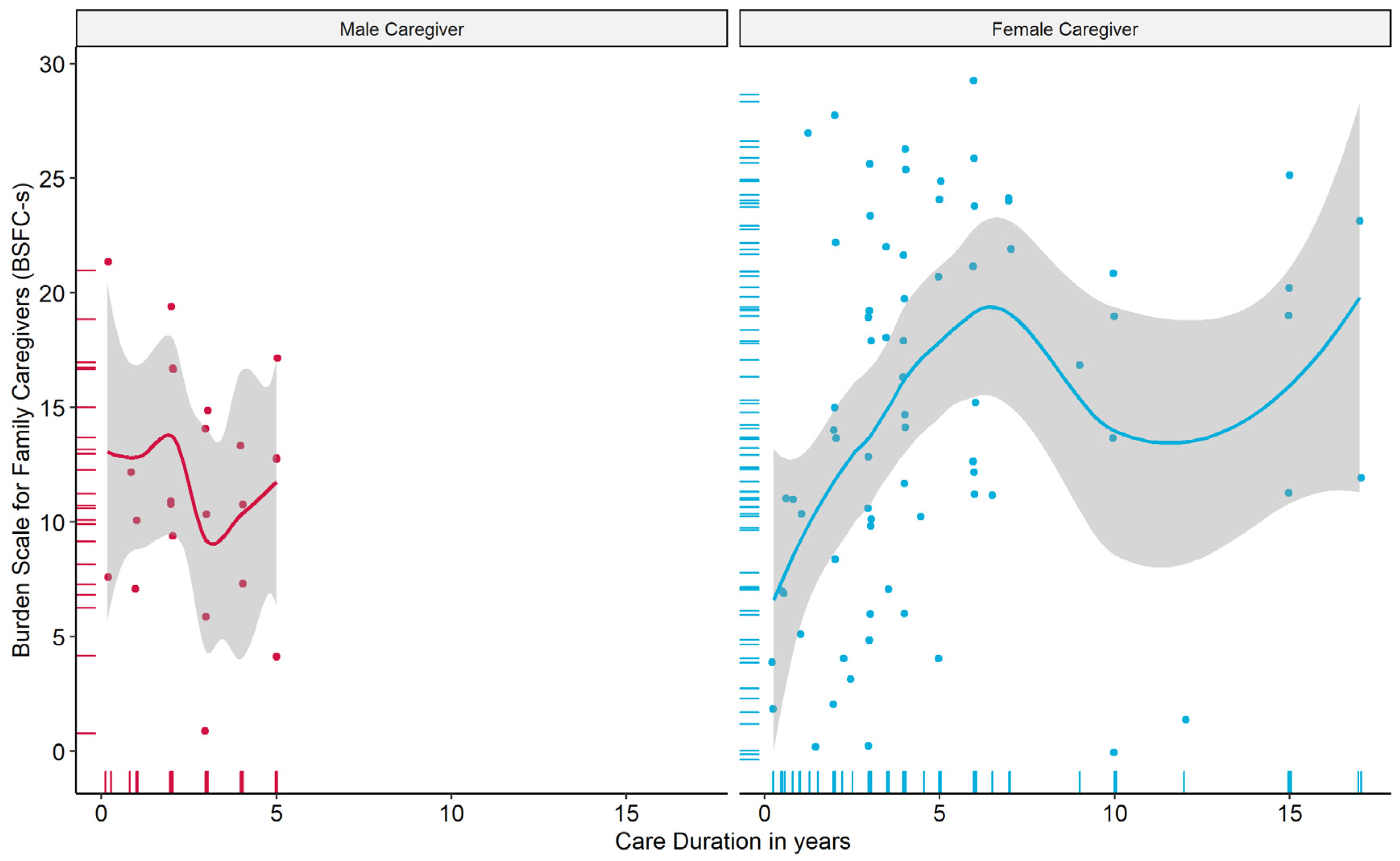
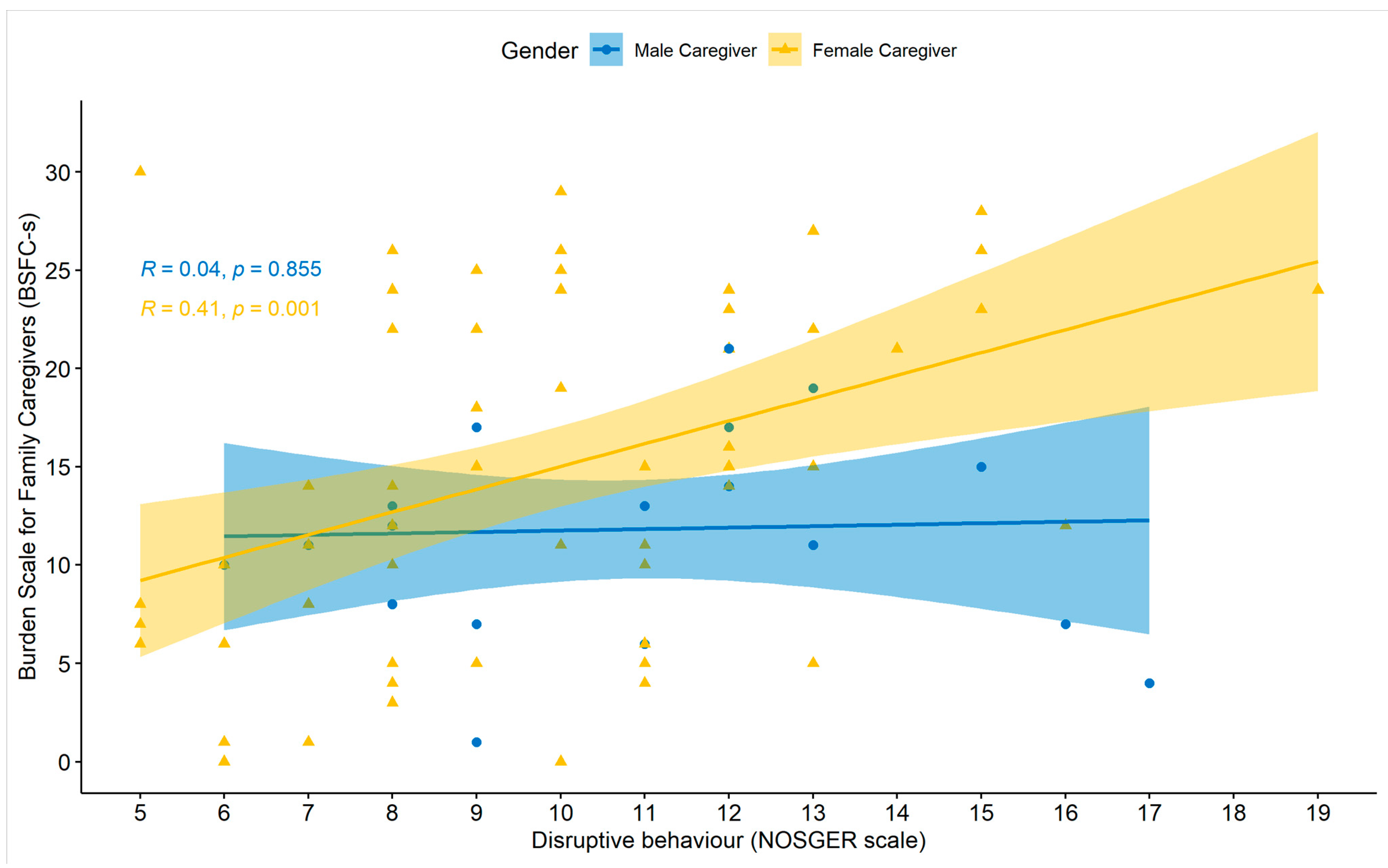
4.4. Care Duration and Dependency of the PwD
4.5. Service Utilisation
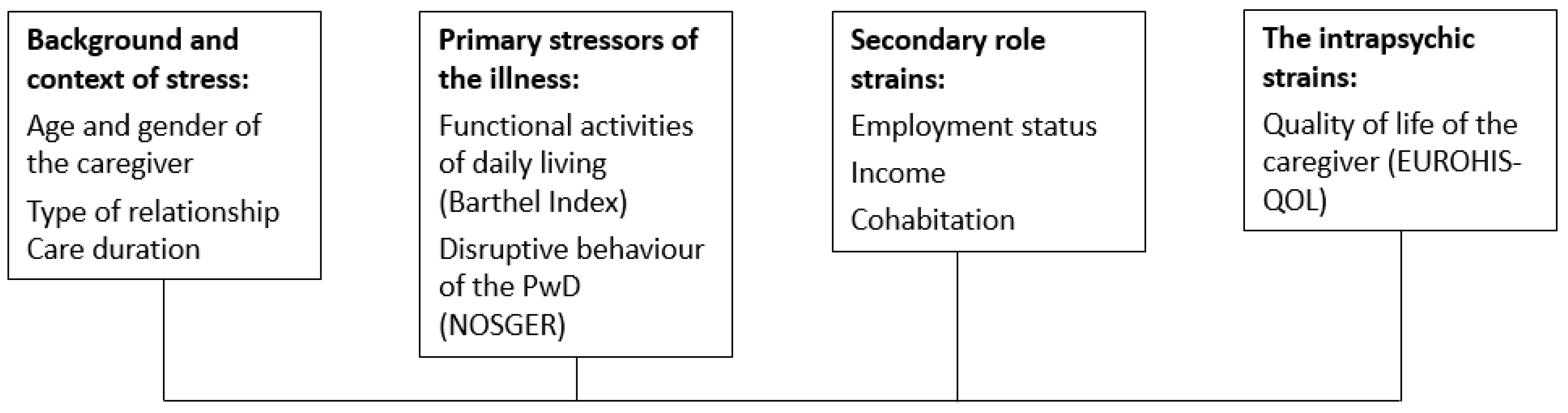
4.6. Path Model and Pearlin’s Four Dimensions Contributing to Caregiver Burden
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Maresovsa, P.; Javanmardi, E.; Barakovic, S.; Barakovic Husic, J.; Tomsone, S.; Krejcar, O.; Kuca, K. Consequences of chronic diseases and other limitations associated with old age—A scoping review. BMC Public Health 2019, 19, 1431. [Google Scholar] [CrossRef]
- Eurostat. Ageing Europe: Looking of Lives for Older People in the EU; European Union: Maastricht, The Netherlands, 2019. [Google Scholar]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. J. Alzheimers Assoc. 2013, 9, 63–75.e2. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016: Improving Healthcare for People Living with Dementia: Coverage, Quality and Costs Now and in the Future; Alzheimer’s Disease International (ADI): London, UK, 2016. [Google Scholar]
- Bökberg, C.; Ahlström, G.; Karlsson, S. Utilisation of formal and informal care and services at home among persons with dementia: A cross-sectional study. Scand. J. Caring Sci. 2018, 32, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Donkin, M. Family caregivers of people with dementia. Dialogues Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [PubMed]
- Schoenmakers, B.; Buntinx, F.; Delepeleire, J. Factors determining the impact of care-giving on caregivers of elderly patients with dementia. A systematic literature review. Maturitas 2010, 66, 191–200. [Google Scholar] [CrossRef]
- Farina, N.; Page, T.E.; Daley, S.; Brown, A.; Bowling, A.; Basset, T.; Livingston, G.; Knapp, M.; Murray, J.; Banerjee, S. Factors associated with the quality of life of family carers of people with dementia: A systematic review. Alzheimers Dement. J. Alzheimers Assoc. 2017, 13, 572–581. [Google Scholar] [CrossRef] [Green Version]
- Schulz, R.; Eden, J.; Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine. Families Caring for an Aging America; National Academies Press (US): Washington, DC, USA, 2016. [Google Scholar]
- Archbold, P.G. All-Consuming Activity: The Family as Caregiver. Gener. J. Am. Soc. Aging 1982, 7, 12–40. [Google Scholar]
- Kellett, U.M. Meaning-making for family carers in nursing homes. Int. J. Nurs. Pract. 1998, 4, 113–119. [Google Scholar] [CrossRef]
- Nolan, M.; Grant, G.; Keady, J. Understanding Family Care: A Multidimensional Model of Caring and Coping; Open University Press: Buckingham, UK, 1996. [Google Scholar]
- Lynch, S.H.; Shuster, G.; Lobo, M.L. The family caregiver experience—Examining the positive and negative aspects of compassion satisfaction and compassion fatigue as caregiving outcomes. Aging Ment. Health 2018, 22, 1424–1431. [Google Scholar] [CrossRef]
- Etters, L.; Goodall, D.; Harrison, B.E. Caregiver burden among dementia patient caregivers: A review of the literature. J. Am. Acad. Nurse Pract. 2008, 20, 423–428. [Google Scholar] [CrossRef]
- Gimeno, I.; Val, S.; Cardoso Moreno, M.J. Relation among Caregivers’ Burden, Abuse and Behavioural Disorder in People with Dementia. Int. J. Environ. Res. Public Health 2021, 18, 1263. [Google Scholar] [CrossRef] [PubMed]
- Chiao, C.Y.; Wu, H.S.; Hsiao, C.Y. Caregiver burden for informal caregivers of patients with dementia: A systematic review. Int. Nurs. Rev. 2015, 62, 340–350. [Google Scholar] [CrossRef]
- Campbell, P.; Wright, J.; Oyebode, J.; Job, D.; Crome, P.; Bentham, P.; Jones, L.; Lendon, C. Determinants of burden in those who care for someone with dementia. Int. J. Geriatr. Psychiatry 2008, 23, 1078–1085. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Joling, K.J.; Janssen, O.; Francke, A.L.; Verheij, R.A.; Lissenberg-Witte, B.I.; Visser, P.J.; van Hout, H.P.J. Time from diagnosis to institutionalization and death in people with dementia. Alzheimers Dement. 2020, 16, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Lautenschläger, S.; Meyer, G.; Stephan, A. Interventions to support people with dementia and their caregivers during the transition from home care to nursing home care: A systematic review. Int. J. Nurs. Stud. 2017, 71, 139–152. [Google Scholar] [CrossRef]
- Robinson, K.M.; Buckwalter, K.; Reed, D. Differences between Dementia Caregivers Who are Users and Nonusers of Community Services. Public Health Nurs. 2013, 30, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Bott, N.T.; Sheckter, C.C.; Milstein, A.S. Dementia Care, Women’s Health, and Gender Equity: The Value of Well-Timed Caregiver Support. JAMA Neurol. 2017, 74, 757–758. [Google Scholar] [CrossRef]
- Mott, J.; Schmidt, B.; MacWilliams, B. Male Caregivers: Shifting Roles among Family Caregivers. Clin. J. Oncol. Nurs. 2019, 23, E17–E24. [Google Scholar] [CrossRef]
- Fraser, C.; Warr, D.J. Challenging roles: Insights into issues for men caring for family members with mental illness. Am. J. Mens. Health 2009, 3, 36–49. [Google Scholar] [CrossRef]
- Robinson, C.A.; Bottorff, J.L.; Pesut, B.; Oliffe, J.L.; Tomlinson, J. The Male Face of Caregiving: A Scoping Review of Men Caring for a Person with Dementia. Am. J. Mens. Health 2014, 8, 409–426. [Google Scholar] [CrossRef] [Green Version]
- Mc Donnell, E.; Ryan, A.A. The experience of sons caring for a parent with dementia. Dementia 2014, 13, 788–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Donnell, E.; Ryan, A. Male caregiving in dementia: A review and commentary. Dementia 2013, 12, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Chappell, N.L.; Dujela, C.; Smith, A. Caregiver Well-Being: Intersections of Relationship and Gender. Res. Aging 2015, 37, 623–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family—Caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Klietz, M.; von Eichel, H.; Schnur, T.; Staege, S.; Höglinger, G.U.; Wegner, F.; Stiel, S. One Year Trajectory of Caregiver Burden in Parkinson’s Disease and Analysis of Gender-Specific Aspects. Brain Sci. 2021, 11, 295. [Google Scholar] [CrossRef]
- Pillemer, S.; Davis, J.; Tremont, G. Gender effects on components of burden and depression among dementia caregivers. Aging Ment. Health 2018, 22, 1156–1161. [Google Scholar] [CrossRef]
- Gilmore-Bykovskyi, A.; Johnson, R.; Walljasper, L.; Block, L.; Werner, N. Underreporting of Gender and Race/Ethnicity Differences in NIH-Funded Dementia Caregiver Support Interventions. Am. J. Alzheimers Dis. Demen. 2018, 33, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Baker, K.L.; Robertson, N.; Connelly, D. Men caring for wives or partners with dementia: Masculinity, strain and gain. Aging Ment. Health 2010, 14, 319–327. [Google Scholar] [CrossRef]
- Baker, K.L.; Robertson, N. Coping with caring for someone with dementia: Reviewing the literature about men. Aging Ment. Health 2008, 12, 413–422. [Google Scholar] [CrossRef]
- Bai, X.; Liu, C.; Baladon, L.; Rubio-Valera, M. Multidimensional determinants of the caregiving burden among Chinese male caregivers of older family members in Hong Kong. Aging Ment. Health 2018, 22, 980–989. [Google Scholar] [CrossRef]
- Bartlett, R.; Gjernes, T.; Lotherington, A.T.; Obstefelder, A. Gender, citizenship and dementia care: A scoping review of studies to inform policy and future research. Health Soc. Care Community 2018, 26, 14–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, N.J.; Morgan, D.G.; Karunanayake, C.P.; Wickenhauser, J.P.; Cammer, A.; Minish, D.; O’Connell, M.E.; Hayduk, L.A. Rural Caregivers for a Family Member With Dementia. J. Appl. Gerontol. 2016, 35, 150–178. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Fetherstonhaugh, D.; Blackberry, I.; Farmer, J.; Wilding, C. Identifying support needs to improve rural dementia services for people with dementia and their carers: A consultation study in Victoria, Australia. Aust. J. Rural. Health 2019, 27, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Bedard, M.; Koivuranta, A.; Stuckey, A. Health impact on caregivers of providing informal care to a cognitively impaired older adult: Rural versus urban settings. Can. J. Rural. Med. Off. J. Soc. Rural. Physicians Can. 2004, 9, 15–23. [Google Scholar]
- O’Connell, M.E.; Germaine, N.; Burton, R.; Stewart, N.; Morgan, D.G. Degree of rurality is not related to dementia caregiver distress, burden, and coping in a predominantly rural sample. J. Appl. Gerontol. Off. J. South Gerontol. Soc. 2013, 32, 1015–1029. [Google Scholar] [CrossRef]
- Krutter, S.; Schaffler-Schaden, D.; Eßl-Maurer, R.; Seymer, A.; Osterbrink, J.; Flamm, M. Home care nursing for persons with dementia from a family caregivers’ point of view: Predictors of utilisation in a rural setting in Austria. Health Soc. Care Community 2021, 1–11. [Google Scholar] [CrossRef]
- Ehrlich, K.; Bostrom, A.M.; Mazaheri, M.; Heikkila, K.; Emami, A. Family caregivers’ assessments of caring for a relative with dementia: A comparison of urban and rural areas. Int. J. Older People Nurs. 2015, 10, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tommis, Y.; Seddon, D.; Woods, B.; Robinson, C.A.; Reeves, C.; Russell, I.T. Rural-urban differences in the effects on mental well-being of caring for people with stroke or dementia. Aging Ment. Health 2007, 11, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Krutter, S.; Schaffler-Schaden, D.; Essl-Maurer, R.; Wurm, L.; Seymer, A.; Kriechmayr, C.; Mann, E.; Osterbrink, J.; Flamm, M. Comparing perspectives of family caregivers and healthcare professionals regarding caregiver burden in dementia care: Results of a mixed methods study in a rural setting. Age Ageing 2019, 49, 199–207. [Google Scholar] [CrossRef]
- Dijkstra, L.; Poelman, H. A Harmonised Definition of Cities and rural Areas: The New Degree of Urbanisation; Working Paper 01/2014 of the European Commission; European Commission: Belgium, Luxembourg, 2014. [Google Scholar]
- Sinoff, G.; Ore, L. The Barthel activities of daily living index: Self-reporting versus actual performance in the old-old (> or =75 years). J. Am. Geriatr. Soc. 1997, 45, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, R.; Brunner, C.; Ermini-Fünfschilling, D.; Monsch, A.; Notter, M.; Puxty, J.; Tremmel, L. A new behavioral assessment scale for geriatric out- and in-patients: The NOSGER (Nurses’ Observation Scale for Geriatric Patients). J. Am. Geriatr. Soc. 1991, 39, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Brähler, E.; Mühlan, H.; Albani, C.; Schmidt, S. Teststatistische Prüfung und Normierung der deutschen Versionen des EUROHIS-QOL Lebensqualität-Index und des WHO-5 Wohlbefindens-Index. Diagnostica 2007, 53, 83–96. [Google Scholar] [CrossRef]
- Graessel, E.; Berth, H.; Lichte, T.; Grau, H. Subjective caregiver burden: Validity of the 10-item short version of the Burden Scale for Family Caregivers BSFC-s. BMC Geriatr. 2014, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Pendergrass, A.; Malnis, C.; Graf, U.; Engel, S.; Graessel, E. Screening for caregivers at risk: Extended validation of the short version of the Burden Scale for Family Caregivers (BSFC-s) with a valid classification system for caregivers caring for an older person at home. BMC Health Serv. Res. 2018, 18, 229. [Google Scholar] [CrossRef] [Green Version]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.R-project.org/ (accessed on 19 July 2021).
- Hu, L.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Schreiber, J.B. Core reporting practices in structural equation modeling. Res. Soc. Adm. Pharm. 2008, 4, 83–97. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Papastavrou, E.; Kalokerinou, A.; Papacostas, S.S.; Tsangari, H.; Sourtzi, P. Caring for a relative with dementia: Family caregiver burden. J. Adv. Nurs. 2007, 58, 446–457. [Google Scholar] [CrossRef] [Green Version]
- Croog, S.H.; Burleson, J.A.; Sudilovsky, A.; Baume, R.M. Spouse caregivers of Alzheimer patients: Problem responses to caregiver burden. Aging Ment. Health 2006, 10, 87–100. [Google Scholar] [CrossRef]
- Connors, M.H.; Seeher, K.; Teixeira-Pinto, A.; Woodward, M.; Ames, D.; Brodaty, H. Dementia and caregiver burden: A three-year longitudinal study. Int. J. Geriatr. Psychiatry 2020, 35, 250–258. [Google Scholar] [CrossRef]
- Swinkels, J.; Tilburg, T.V.; Verbakel, E.; van Groenou, M.B. Explaining the Gender Gap in the Caregiving Burden of Partner Caregivers. J. Gerontol. B Psychol. Sci. Soc. Sci. 2019, 74, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Connell, C.M.; Janevic, M.R.; Gallant, M.P. The costs of caring: Impact of dementia on family caregivers. J. Geriatr. Psychiatry Neurol. 2001, 14, 179–187. [Google Scholar] [CrossRef]
- Raccichini, A.; Spazzafumo, L.; Castellani, S.; Civerchia, P.; Pelliccioni, G.; Scarpino, O. Living with mild to moderate Alzheimer patients increases the caregiver’s burden at 6 months. Am. J. Alzheimers Dis. Demen. 2015, 30, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef]
- Aneshensel, C.S.; Pearlin, L.I.; Schuler, R.H. Stress, role captivity, and the cessation of caregiving. J. Health Soc. Behav. 1993, 34, 54–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietzel, N.; Karrer, L.; Wolff, F.; Kratzer, A.; Hess, M.; Gräßel, E.; Kolominsky-Rabas, P. Predictors of Caregiver Burden in Dementia: Results of the Bavarian Dementia Survey (BayDem). Gesundheitswesen 2020, 82, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vatter, S.; McDonald, K.R.; Stanmore, E.; Clare, L.; McCormick, S.A.; Leroi, I. A qualitative study of female caregiving spouses’ experiences of intimate relationships as cognition declines in Parkinson’s disease. Age Ageing 2018, 47, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Penning, M.J.; Wu, Z. Caregiver Stress and Mental Health: Impact of Caregiving Relationship and Gender. Gerontologist 2016, 56, 1102–1113. [Google Scholar] [CrossRef]
- Viñas-Diez, V.; Turró-Garriga, O.; Portellano-Ortiz, C.; Gascón-Bayarri, J.; Reñé-Ramírez, R.; Garre-Olmo, J.; Conde-Sala, J.L. Kinship and cohabitation in relation to caregiver burden in the context of Alzheimer’s disease: A 24-month longitudinal study. Int. J. Geriatr. Psychiatry 2017, 32, e72–e82. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.; Slagsvold, B. Feeling the squeeze? The effects of combining work and informal caregiving on psychological well-being. Eur. J. Ageing 2015, 12, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaugler, J.E.; Pestka, D.L.; Davila, H.; Sales, R.; Owen, G.; Baumgartner, S.A.; Shook, R.; Cunningham, J.; Kenney, M. The Complexities of Family Caregiving at Work: A Mixed-Methods Study. Int. J. Aging Hum. Dev. 2018, 87, 347–376. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dokos, M.; Fauth, E.B.; Lee, Y.G.; Zarit, S.H. Financial Strain, Employment, and Role Captivity and Overload Over Time Among Dementia Family Caregivers. Gerontologist 2019, 59, e512–e520. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, N.; Smith, R. Barriers and facilitators for male carers in accessing formal and informal support: A systematic review. Maturitas 2015, 82, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.C.; Coogle, C.L. Spousal Caregiving for Partners With Dementia: A Deductive Literature Review Testing Calasanti’s Gendered View of Care Work. J. Appl. Gerontol. 2016, 35, 759–787. [Google Scholar] [CrossRef]
- Xiong, C.; Biscardi, M.; Astell, A.; Nalder, E.; Cameron, J.I.; Mihailidis, A.; Colantonio, A. Sex and gender differences in caregiving burden experienced by family caregivers of persons with dementia: A systematic review. PLoS ONE 2020, 15, e0231848. [Google Scholar] [CrossRef] [Green Version]
- Cepoiu-Martin, M.; Tam-Tham, H.; Patten, S.; Maxwell, C.J.; Hogan, D.B. Predictors of long-term care placement in persons with dementia: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2016, 31, 1151–1171. [Google Scholar] [CrossRef] [PubMed]
- Thyrian, J.R.; Winter, P.; Eichler, T.; Reimann, M.; Wucherer, D.; Dreier, A.; Michalowsky, B.; Zarm, K.; Hoffmann, W. Relatives’ burden of caring for people screened positive for dementia in primary care: Results of the DelpHi study. Z. Gerontol. Geriatr. 2017, 50, 4–13. [Google Scholar] [CrossRef]
- Thyrian, J.R.; Eichler, T.; Hertel, J.; Wucherer, D.; Dreier, A.; Michalowsky, B.; Killimann, I.; Teipel, S.; Hoffmann, W. Burden of Behavioral and Psychiatric Symptoms in People Screened Positive for Dementia in Primary Care: Results of the DelpHi-Study. J. Alzheimers Dis. 2015, 46, 451–459. [Google Scholar] [CrossRef]
- Bédard, M.; Kuzik, R.; Chambers, L.; Molloy, D.W.; Dubois, S.; Lever, J.A. Understanding burden differences between men and women caregivers: The contribution of care-recipient problem behaviors. Int. Psychogeriatr. 2005, 17, 99–118. [Google Scholar] [CrossRef]
- Van den Kieboom, R.; Snaphaan, L.; Mark, R.; Bongers, I. The Trajectory of Caregiver Burden and Risk Factors in Dementia Progression: A Systematic Review. J. Alzheimers Dis. JAD 2020, 77, 1107–1115. [Google Scholar] [CrossRef]
- Srivastava, G.; Tripathi, R.K.; Tiwari, S.C.; Singh, B.; Tripathi, S.M. Caregiver Burden and Quality of Life of Key Caregivers of Patients with Dementia. Indian J. Psychol. Med. 2016, 38, 133–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male Caregiver (n = 27) | Female Caregiver (n = 86) | Overall (n = 113) | p-Value | |
|---|---|---|---|---|
| Age (years) | ||||
| Mean (SD) | 61.4 (18.4) | 60.5 (13.8) | 60.7 (14.9) | 0.830 1 |
| Relationship with PwD | ||||
| Spouse or partner | 10 (37.0%) | 25 (29.8%) | 35 (31.5%) | 0.803 2 |
| Mother/father | 14 (51.9%) | 37 (44.0%) | 51 (45.9%) | |
| Sister/brother | 0 (0.0%) | 2 (2.4%) | 2 (1.8%) | |
| Daughter/son | 1 (3.7%) | 6 (7.1%) | 7 (6.3%) | |
| Daughter/son in law | 0 (0.0%) | 2 (2.4%) | 2 (1.8%) | |
| Grandmother/grandfather | 1 (3.7%) | 6 (7.1%) | 7 (6.3%) | |
| Friend | 1 (3.7%) | 6 (7.1%) | 7 (6.3%) | |
| Marital status | ||||
| Married/cohabitation | 22 (81.5%) | 62 (72.1%) | 84 (74.3%) | 0.218 2 |
| Separated/divorced | 2 (7.4%) | 17 (19.8%) | 19 (16.8%) | |
| Widowed | 0 (0.0%) | 3 (3.5%) | 3 (2.7%) | |
| Single | 3 (11.1%) | 4 (4.7%) | 7 (6.2%) | |
| Education | ||||
| Compulsory school | 4 (16.0%) | 11 (13.3%) | 15 (13.9%) | 0.875 2 |
| Apprenticeship | 8 (32.0%) | 28 (33.7%) | 36 (33.3%) | |
| Technical or commercial school | 4 (16.0%) | 20 (24.1%) | 24 (22.2%) | |
| High school degree | 6 (24.0%) | 14 (16.9%) | 20 (18.5%) | |
| (Technical) college/university | 3 (12.0%) | 10 (12.0%) | 13 (12.0%) | |
| Monthly net household income (€) | ||||
| Less than 1000 | 1 (4.17%) | 28 (40.0%) | 29 (30.9%) | 0.001 2 |
| 1001 to 1500 | 4 (16.7%) | 20 (28.6%) | 24 (25.5%) | |
| 1501 to 2000 | 10 (41.7%) | 12 (17.1%) | 22 (23.4%) | |
| 2001 to 2500 | 6 (25.0%) | 7 (10.0%) | 13 (13.8%) | |
| 2501 to 4000 | 3 (12.5%) | 3 (4.3%) | 6 (6.4%) | |
| Population at place of residence | ||||
| Less than 2000 | 4 (15.4%) | 3 (3.7%) | 7 (6.5%) | 0.187 2 |
| 2001 to 5000 | 7 (26.9%) | 36 (44.4%) | 43 (40.2%) | |
| 5001 to 10,000 | 3 (11.5%) | 14 (17.3%) | 17 (15.9%) | |
| 10,001 to 15,000 | 5 (19.2%) | 13 (16.0%) | 18 (16.8%) | |
| 15,001 to 20,000 | 3 (11.5%) | 4 (4.94%) | 7 (6.5%) | |
| 20,001 or more | 4 (15.4%) | 11 (13.6%) | 15 (14.0%) | |
| Employment | ||||
| Full time | 13 (50.0%) | 10 (11.9%) | 23 (20.9%) | <0.001 2 |
| Part time | 0 (0%) | 22 (26.2%) | 22 (20.0%) | |
| Retired | 12 (46.2%) | 42 (50.0%) | 54 (49.1%) | |
| Not working | 1 (3.85%) | 10 (11.9%) | 11 (10.0%) | |
| Cohabitation with PwD | ||||
| No | 10 (37.0%) | 34 (39.5%) | 44 (38.9%) | 0.995 2 |
| Yes | 17 (63.0%) | 52 (60.5%) | 69 (61.1%) | |
| Burden level (BSFC-s) | ||||
| Mean (SD) | 11.6 (4.77) | 14.2 (8.20) | 13.6 (7.63) | 0.055 1 |
| Disruptive behaviour (NOSGER scale) | ||||
| Mean (SD) | 10.9 (2.99) | 9.97 (3.05) | 10.2 (3.04) | 0.249 1 |
| Barthel Index | ||||
| Mean (SD) | 76.0 (19.9) | 63.5 (26.5) | 66.5 (25.5) | 0.026 1 |
| Median [Min, Max] | 75.0 [40.0, 100] | 65.0 [0, 100] | 70.0 [0, 100] | |
| Quality of Life (EUROHIS-QOL) | ||||
| Mean (SD) | 3.73 (0.555) | 3.69 (0.661) | 3.70 (0.637) | 0.779 1 |
| Median [Min, Max] | 3.63 [2.75, 4.75] | 3.75 [2.13, 5.00] | 3.75 [2.13, 5.00] | |
| Caregiving duration (years) | ||||
| Mean (SD) | 2.72 (1.53) | 5.30 (4.38) | 4.67 (4.03) | <0.001 1 |
| Weekly caregiving (days) | ||||
| Mean (SD) | 6.13 (1.78) | 5.56 (2.10) | 5.69 (2.04) | 0.196 1 |
| Daily caregiving (hours) | ||||
| Mean (SD) | 4.88 (5.25) | 8.39 (8.43) | 7.54 (7.91) | 0.016 1 |
| Home nursing service usage | ||||
| No | 6 (22.2%) | 35 (44.9%) | 41 (39.0%) | 0.064 2 |
| Yes | 21 (77.8%) | 43 (55.1%) | 64 (61.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schaffler-Schaden, D.; Krutter, S.; Seymer, A.; Eßl-Maurer, R.; Flamm, M.; Osterbrink, J. Caring for a Relative with Dementia: Determinants and Gender Differences of Caregiver Burden in the Rural Setting. Brain Sci. 2021, 11, 1511. https://doi.org/10.3390/brainsci11111511
Schaffler-Schaden D, Krutter S, Seymer A, Eßl-Maurer R, Flamm M, Osterbrink J. Caring for a Relative with Dementia: Determinants and Gender Differences of Caregiver Burden in the Rural Setting. Brain Sciences. 2021; 11(11):1511. https://doi.org/10.3390/brainsci11111511
Chicago/Turabian StyleSchaffler-Schaden, Dagmar, Simon Krutter, Alexander Seymer, Roland Eßl-Maurer, Maria Flamm, and Jürgen Osterbrink. 2021. "Caring for a Relative with Dementia: Determinants and Gender Differences of Caregiver Burden in the Rural Setting" Brain Sciences 11, no. 11: 1511. https://doi.org/10.3390/brainsci11111511
APA StyleSchaffler-Schaden, D., Krutter, S., Seymer, A., Eßl-Maurer, R., Flamm, M., & Osterbrink, J. (2021). Caring for a Relative with Dementia: Determinants and Gender Differences of Caregiver Burden in the Rural Setting. Brain Sciences, 11(11), 1511. https://doi.org/10.3390/brainsci11111511