1. Introduction
Despite the decline of incidence and mortality rates [
1], stroke remains a leading cause of morbidity worldwide [
2]. Most studies addressing the health impact of stroke are based on short, long-term mortality and functional neurological outcome. However, even in patients without significant neurological disability, stroke can be associated with poor Quality of Life (QoL) [
3,
4,
5,
6]. QoL measurements are potentially more relevant and informative to patients than the evaluation of functional outcomes [
7]. QoL evaluation may uncover insufficiently managed chronic health problems or facilitate a much broader description of stroke impact on survivors [
8]. Worldwide, there are few studies addressing QoL among stroke survivors. These studies have identified factors such as functional status, depression, low socioeconomic status, or pain as the main determinants of QoL in stroke survivors [
5,
6,
8,
9,
10,
11]. Despite the extreme importance for patients and community, there are no community based published studies describing the QoL of stroke survivors in Portugal. Therefore, we sought to investigate which factors determine QoL of stroke survivors in a community representative population of Algarve, the southernmost part of Portugal.
3. Results
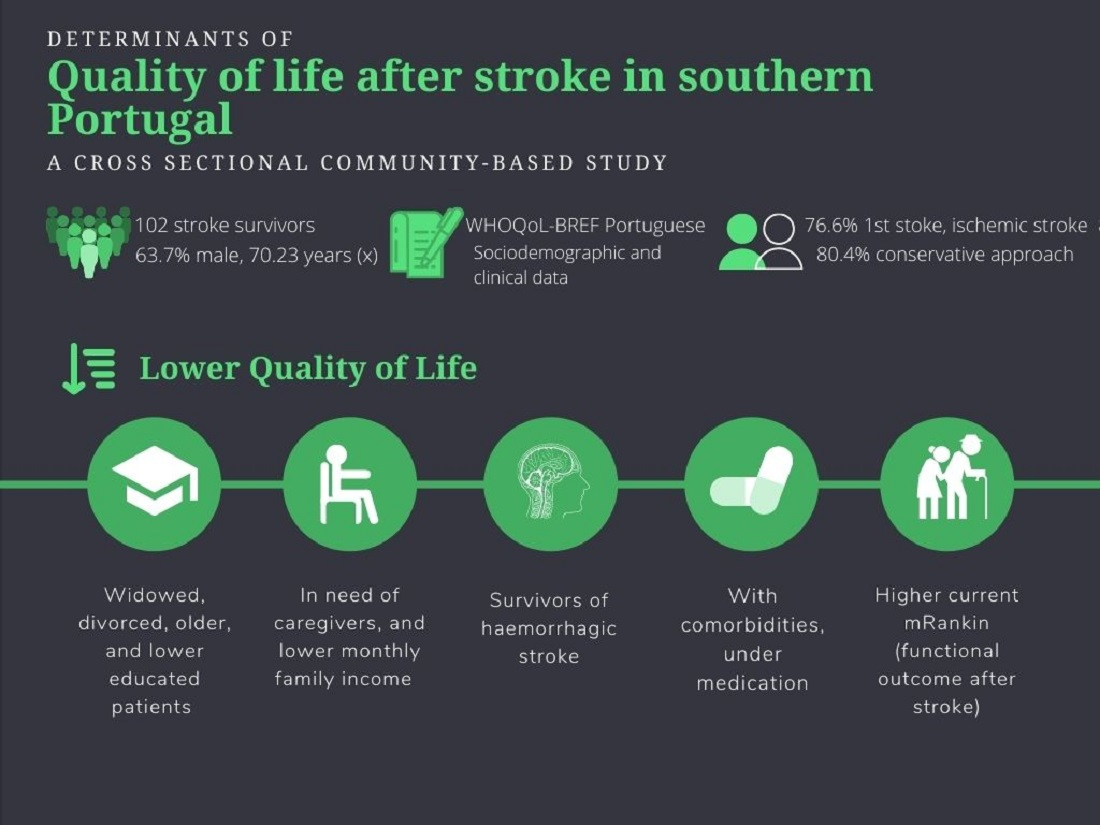
Of the 120 persons who met the inclusion criteria and could be located, 102 (85.8%) agreed to participate and completed the questionnaire.
Table 1 and
Table 2 resume, respectively, the sociodemographic and clinical characteristics of the patients included in the study.
Table 1 shows that the majority (65/63.7%) were men and the mean age at the diagnosis of stroke was 67.7 years old (SD: 12.3). The mean time between the stroke event and the questionnaire was 29.52 months (SD: 32). Most of the patients were married (65/63.7%), had four years of schooling (55/53.9%), were retired (69/67.6%) and had an income lower than 580 euros (47/46.1%).
Ischemic stroke was the most common type (87/86.4%). The most prevalent risk factors at the time of the vascular event were hypertension (85/82.5%), dyslipidemia (61/59.2%) and sedentary lifestyle (51/49.5%). The proportion of stroke survivors with any functional neurological dependency was 10 (9.9%), 72 (69.5%) and 63 (61.6%), before stroke, immediately after stroke and at the time of the questionnaire (from December 2018 to June 2019), respectively (
Table 2). The majority of patients had a single stroke (78/76.6%); 82 patients (80.4%) did not receive any acute reperfusion treatment; only 29 patients had a positive clinical evolution without neurological sequelae.
Table 3 and
Table 4 resume the analysis of the association between specific domains of the HRQoL with different sociodemographic and clinical variables, respectively.
Higher age at the time of stroke onset was negatively correlated with the physical (
p < 0.01) and social (
p < 0.05) dimensions of the HRQoL. Divorced survivors had higher average scores on physical, psychological, social, and general dimensions than married (
p < 0.05) or widowed survivors (
p < 0.01). Survivors with more years of school (
p < 0.01) and higher family income (
p < 0.05) had higher perception in all dimensions of the HRQoL. On the contrary, retired survivors (
p < 0.05) and those with current need of caregivers (
p < 0.01) had worse perception in multidomain of the HRQoL (
Table 3).
Survivors who were taking medication or with comorbidities had worse perception of HRQoL in the physical, psychological, social, and general domains (
p < 0.01) (
Table 4). In comparison to ischemic stroke survivors, patients who suffered a hemorrhagic stroke had worse perception in almost all dimensions of the HRQoL (
p < 0.01).
On multivariate analysis (
Table 5,
Table 6,
Table 7 and
Table 8) chronic mRS was the only predictor found for the physical domain (R
2 = 0.406; F = 8.757;
p < 0.001), the psychological domain (R
2 = 0.286; F = 5.536;
p < 0.001) and the general domain (R
2 = 0.357; F = 7.287;
p < 0.001). Chronic mRS explained 40.6%, 28.6% and 35.7% of the variance, respectively. For the environmental domain, monthly family income emerged as a predictor, explaining 6% of the variance (R
2 = 0.160; F = 3.156;
p < 0.005).
4. Discussion
This is the first community-based study describing the QoL of stroke survivors in our country. The study demonstrated that in stroke survivors, several sociodemographic factors (being older, widow, less educated), economic factors (lower monthly family income) and clinical factors (hemorrhagic stroke type, comorbidities, high chronic mRankin score) are associated with reduced perception of QoL in different dimensions. These findings are similar to those reported in previous studies [
5,
6,
8,
9,
10,
11]. A large proportion of stroke survivors have poor perception of their QoL and probably face unmet long-term needs [
6]. Sociodemographic, economic and health factors have been shown to influence the QoL of stroke survivors [
18,
19,
20]. The relatively young age at the time of stroke, as well at the time of QoL evaluation, further emphasizes the potential for long-term impact and great repercussions to the survivors and consequently for the society [
19,
20]. QoL is very complex and dependent on several factors. For instance, in our study we have demonstrated that widowed survivors have poor QoL. However, widowed patients are generally older, at greater risk of functional decline and poor social support. In addition, the grieving process, per se, negatively impacts various aspects of physical and mental health that can lead to a decrease in the perception of QoL [
19,
20,
21].
Indeed, among older patients and in patients with lower education, reduced HRQoL has been shown to be multifactorial [
6,
11]. Compliance with post-stroke management including rehabilitation, control of vascular risk factors; access to supporting networks within or outside the family helps improve the perception of QoL [
8]. Low education and income influence the ability to control cardiovascular risk factors and the treatment of stroke, due to the difficulty in implementing preventive measures and problems in accessing information, treatment, and rehabilitation services [
11]. Patients may encounter financial barriers to accessing high cost treatments, resulting in a cycle of health degradation and worse perception of QoL [
6]. Additionally, the effort to put in place specific prevention strategies, including restrictive diets, adoption of healthy behaviors, and chronic use of medications—which are sometimes very expensive—can further cause low perception of QoL [
6,
8].
In our study, only chronic mRankin and income emerged as a predictor of poorer QoL. The mRankin scale is used to evaluate the functional neurological outcome after stroke and is one of the most widely used scales [
11,
22]. Therefore, it is expected that a higher mRankin score or higher dependency would be associated with a lower perception of QoL. Others have also demonstrated that patients with worse functional outcomes or more severe strokes have poor perception on some specific domains of HRQoL such as physical, psychological, and general health. These domains are highly associated with autonomy or dependence on their caregivers [
8,
22]. Improvement of post-stroke QoL demands an integrated view of each patient. Management of specific social or health problems, for instance, spasticity, can have a large impact in multiple domains of QoL [
23].
The percentage of ischemic stroke versus haemorrhagic stroke is similar to that described in the medical literature, where it is reported that around 85–90% of all strokes are ischemic and the remaining are haemorrhagic strokes [
24]. Despite that, haemorrhagic stroke is often more deadly than ischemic stroke. The justification may be related to the pathophysiology of the stroke itself, which may lead to a lower response of deficits to rehabilitation, more sequelae, greater dependence, and dysfunction, and consequently a worse perception of QoL [
8,
9,
24].
There are several limitations to be considered. Depression, a major contributor for HQoL [
3,
16,
18] was not specifically evaluated. The inclusion of mental health in the HRQoL partially attenuates this limitation. There is no consensus on when to evaluate the QoL of post-stroke patients. We evaluated patients with different post-stroke follow-up durations, which may have reduced the possibility of identifying meaningful differences. Nevertheless, in some studies, on the long-term follow-up no significant changes occurred in perception of QoL in stroke survivors [
9,
21]. Finally, the number of participants was small, preventing a more detailed and robust statistical analysis.



 ,
, 


{kind=link}