
Timing-Dependent Effects of Transcranial Direct Current Stimulation on Hand Motor Function in Healthy Individuals: A Randomized Controlled Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
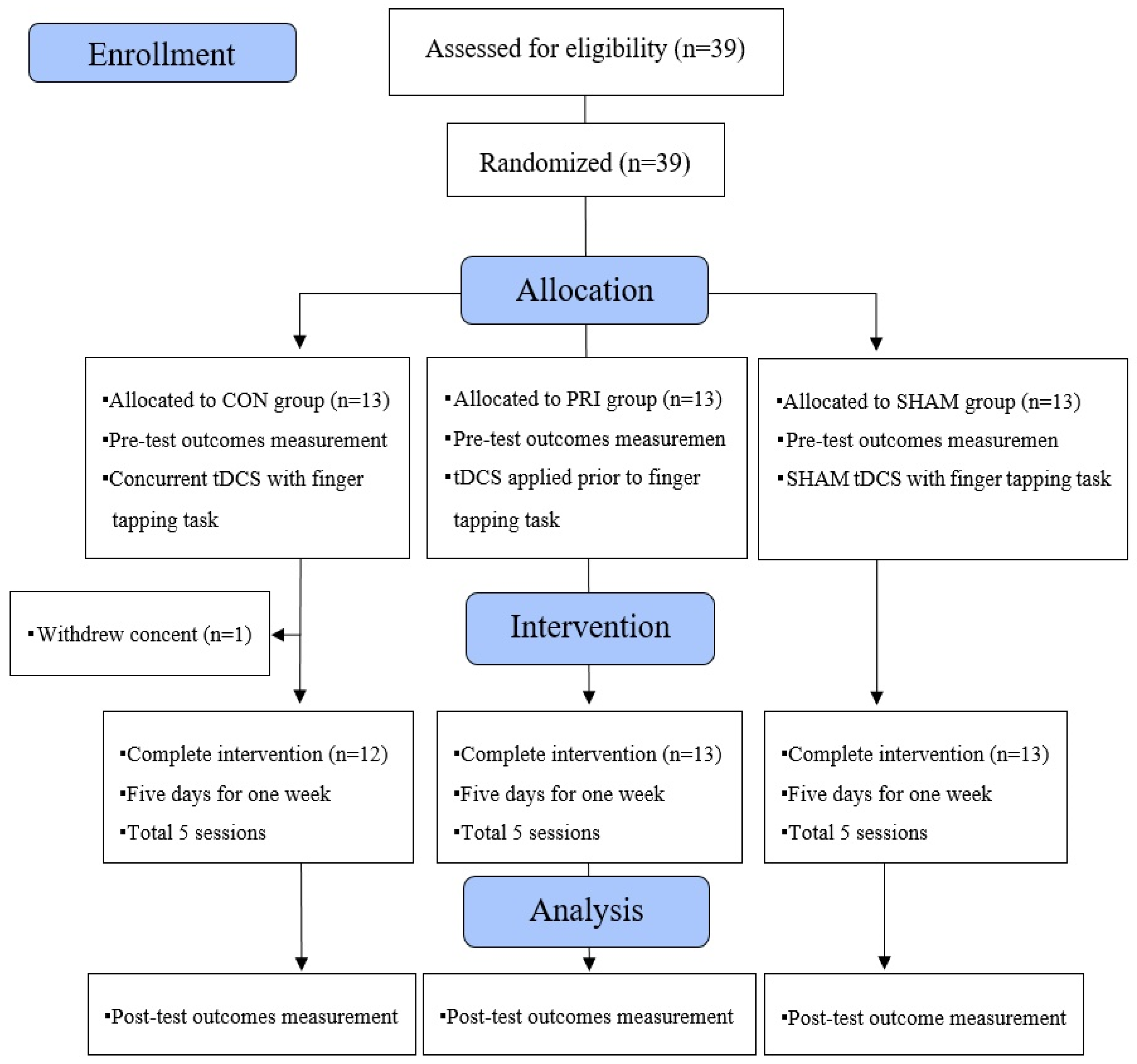
2.1. Participants
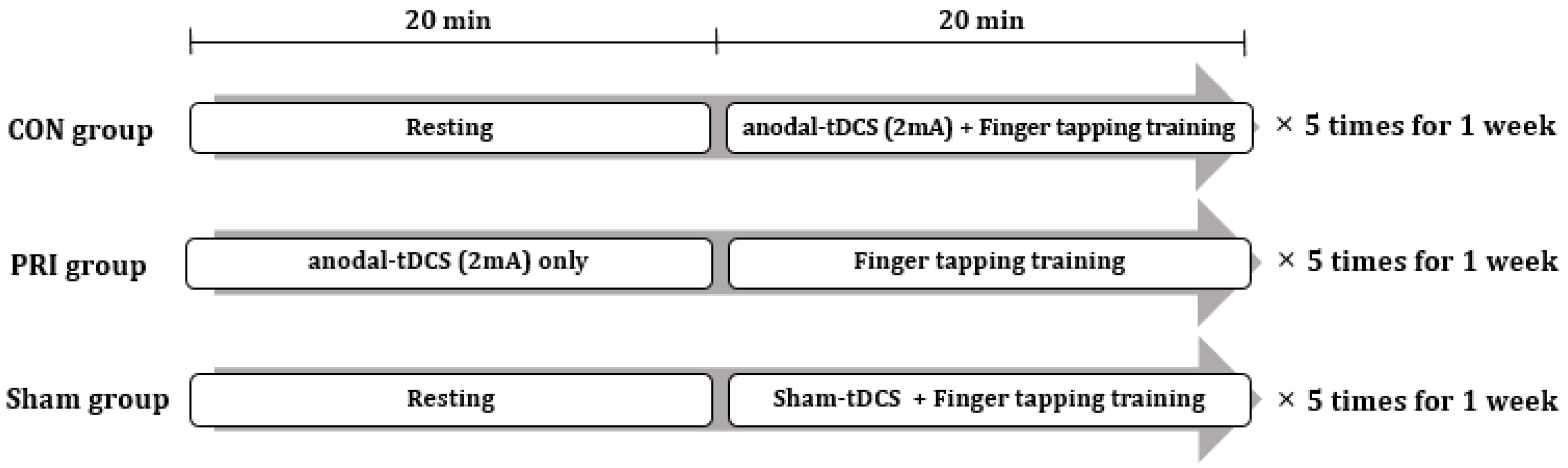
2.2. Trial Design
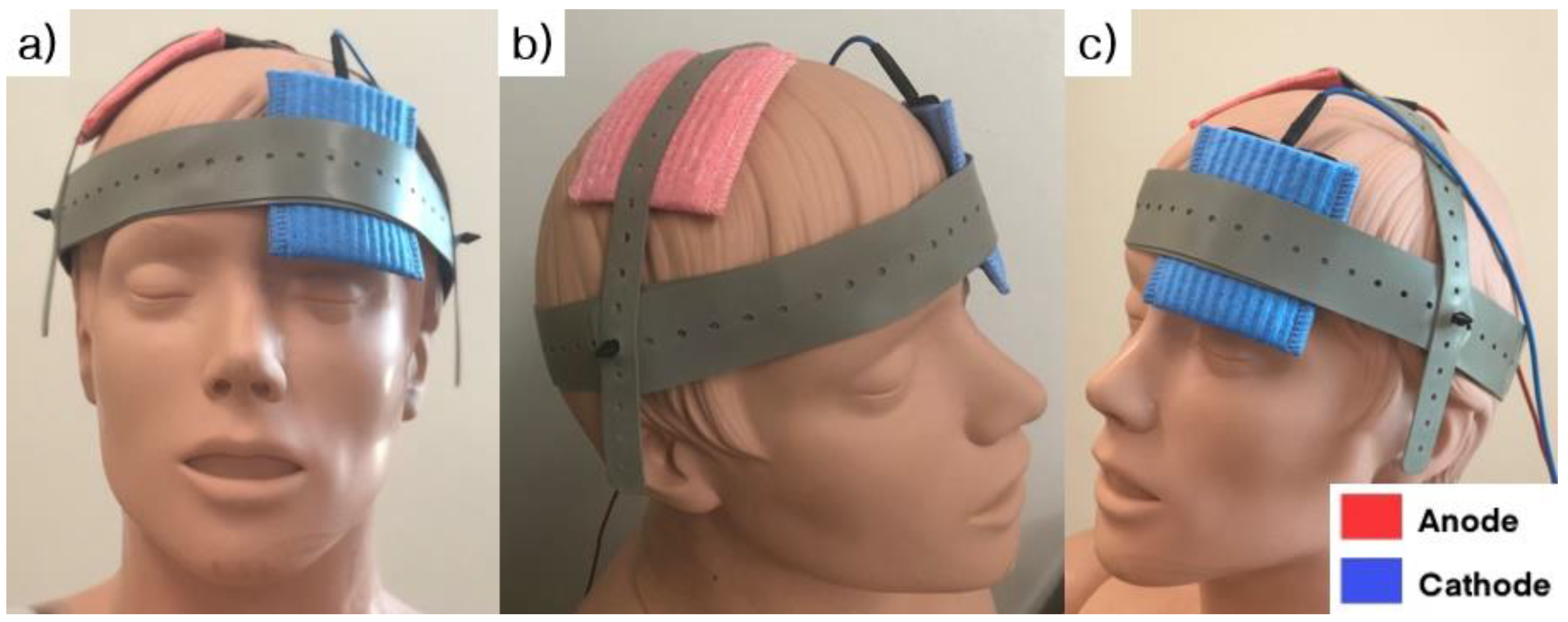
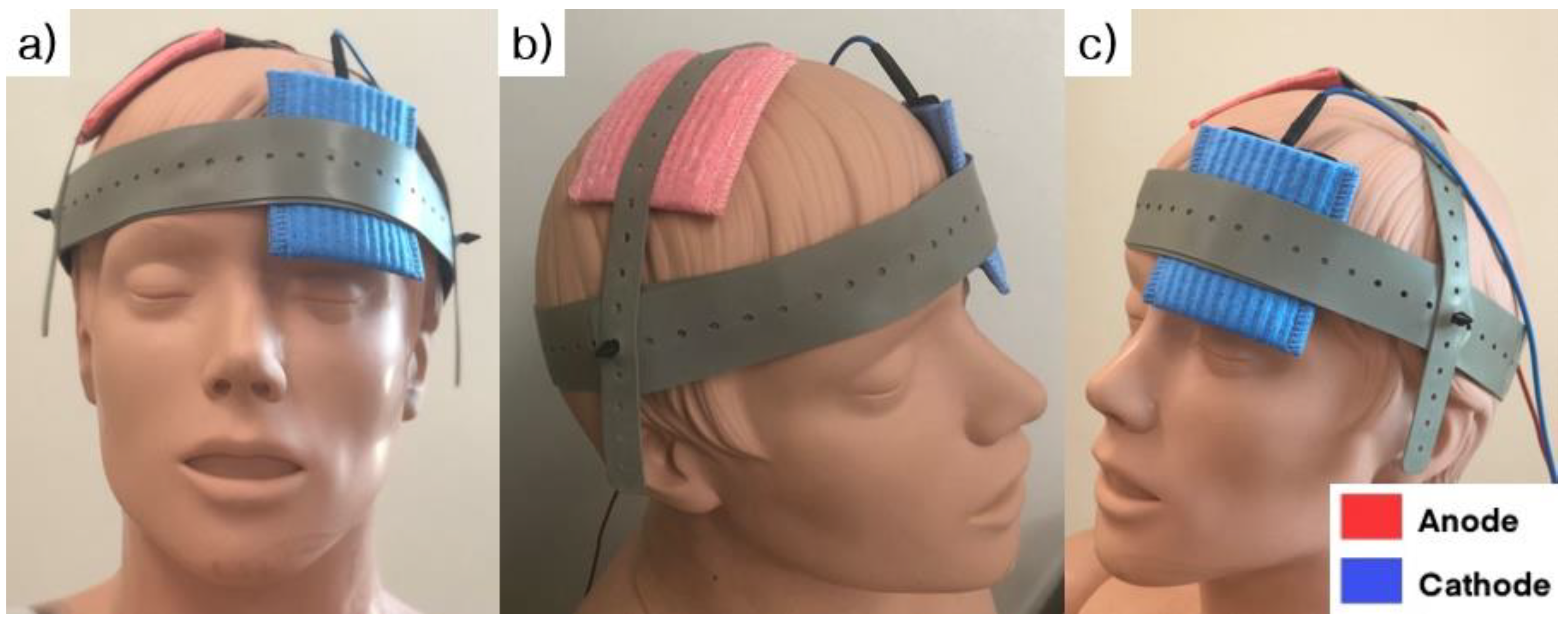
2.3. Experimental Setup
2.4. tDCS Protocol
2.5. Motor Performance Measurements
2.6. Statistical Analyses
3. Results
3.1. Baseline Measurement
3.2. Finger Tapping Task
3.3. Grooved Pegboard Test
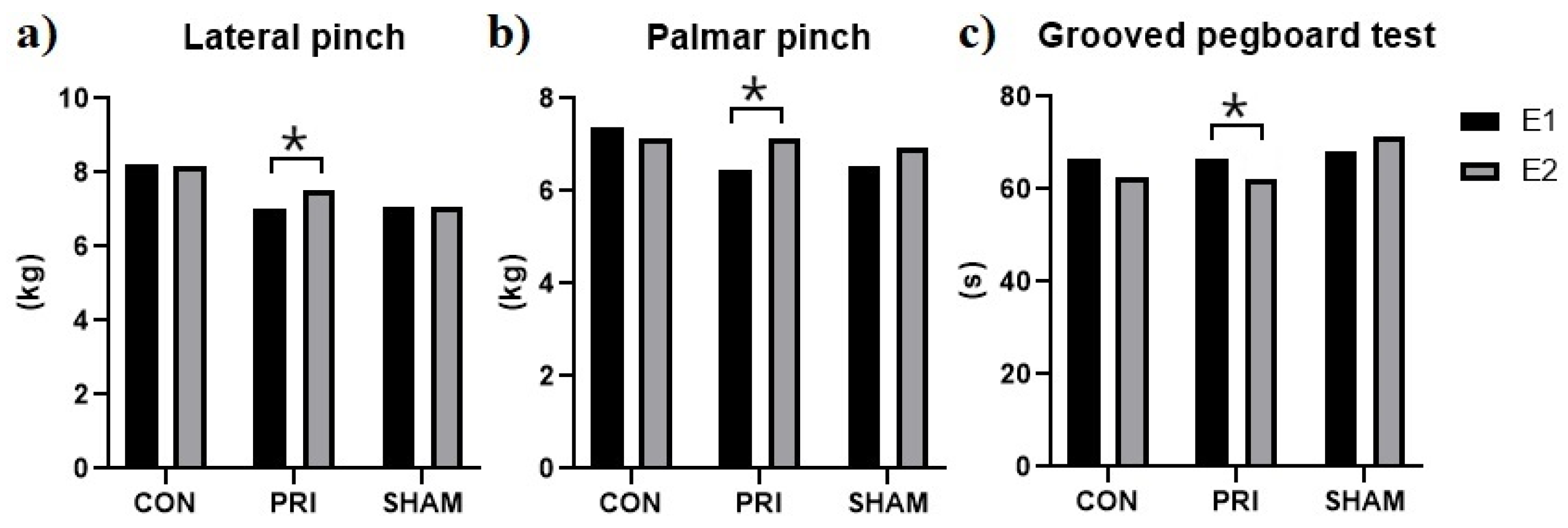
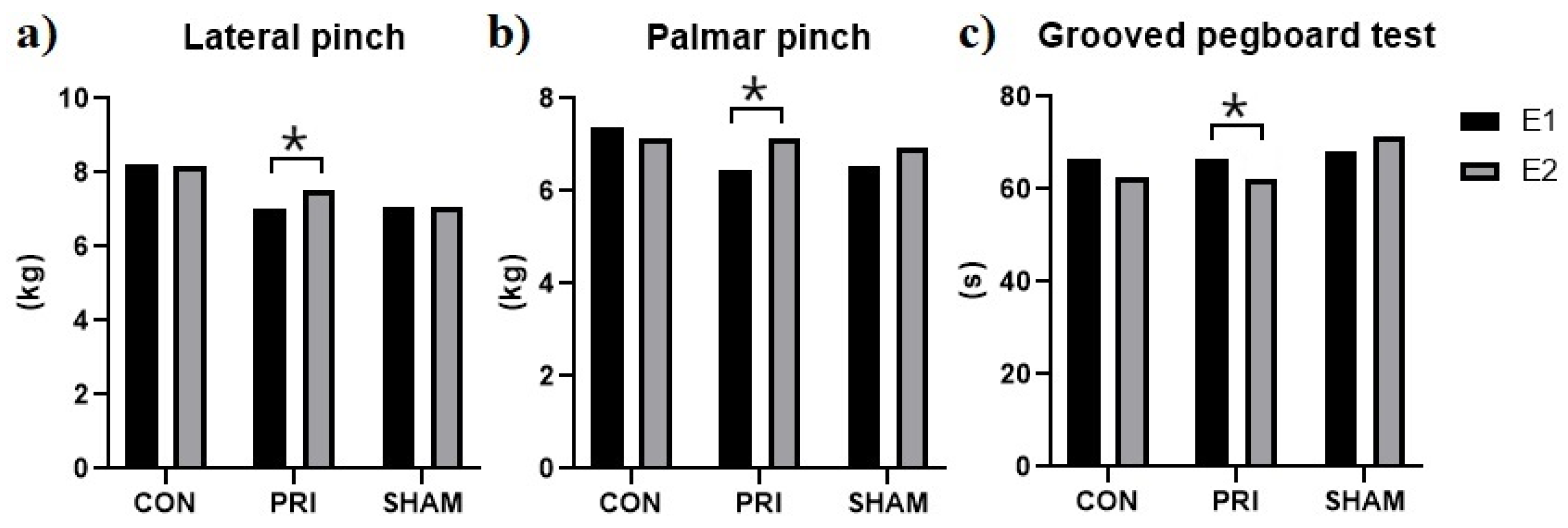
3.4. Hand Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W.J.N. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef] [PubMed]
- Liebetanz, D.; Nitsche, M.A.; Tergau, F.; Paulus, W.J.B. Pharmacological approach to the mechanisms of transcranial DC-stimulation-induced after-effects of human motor cortex excitability. Brain 2002, 125, 2238–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polania, R.; Nitsche, M.A.; Ruff, C.C. Studying and modifying brain function with non-invasive brain stimulation. Nat. Neurosci. 2018, 21, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Hummel, F.; Celnik, P.; Giraux, P.; Floel, A.; Wu, W.-H.; Gerloff, C.; Cohen, L.G. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005, 128, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Hummel, F.C.; Cohen, L.G. Non-invasive brain stimulation: A new strategy to improve neurorehabilitation after stroke? Lancet Neurol. 2006, 5, 708–712. [Google Scholar] [CrossRef]
- Garofalo, S.; Battaglia, S.; Starita, F.; di Pellegrino, G. Modulation of cue-guided choices by transcranial direct current stimulation. Cortex 2021, 137, 124–137. [Google Scholar] [CrossRef] [PubMed]
- Borgomaneri, S.; Battaglia, S.; Garofalo, S.; Tortora, F.; Avenanti, A.; di Pellegrino, G. State-dependent TMS over prefrontal cortex disrupts fear-memory reconsolidation and prevents the return of fear. Curr. Biol. 2020, 30, 3672–3679. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Vitale, F.; Battaglia, S.; Avenanti, A. Early Right Motor Cortex Response to Happy and Fearful Facial Expressions: A TMS Motor-Evoked Potential Study. Brain Sci. 2021, 11, 1203. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Battaglia, S.; Avenanti, A.; di Pellegrino, G. Don’t Hurt Me No More: State-dependent Transcranial Magnetic Stimulation for the treatment of specific phobia. J. Affect. Disord. 2021, 286, 78–79. [Google Scholar] [CrossRef]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving aphasia in adults with aphasia after stroke. Cochrane Libr. 2019, 5, CD009760. [Google Scholar] [CrossRef] [PubMed]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving activities of daily living, and physical and cognitive functioning, in people after stroke. Cochrane Libr. 2020, 3, CD009645. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Siebner, H.R.; Ward, N.S.; Lee, L.; Nitsche, M.A.; Paulus, W.; Rothwell, J.C.; Lemon, R.N.; Frackowiak, R. How does transcranial DC stimulation of the primary motor cortex alter regional neuronal activity in the human brain? Eur. J. Neurosci. 2005, 22, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neuroscientist 2011, 17, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Elsner, B.; Kwakkel, G.; Kugler, J.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving capacity in activities and arm function after stroke: A network meta-analysis of randomised controlled trials. J. Neuroeng. Rehabil. 2017, 14, 95. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.-F.; Paulus, W.; Nitsche, M.A. Therapeutic effects of non-invasive brain stimulation with direct currents (tDCS) in neuropsychiatric diseases. Neuroimage 2014, 85, 948–960. [Google Scholar] [CrossRef]
- Antal, A.; Nitsche, M.A.; Kincses, T.Z.; Kruse, W.; Hoffmann, K.P.; Paulus, W. Facilitation of visuo-motor learning by transcranial direct current stimulation of the motor and extrastriate visual areas in humans. Eur. J. Neurosci. 2004, 19, 2888–2892. [Google Scholar] [CrossRef]
- Molero-Chamizo, A.; Bailén, J.R.A.; Béjar, T.G.; López, M.G.; Rodríguez, I.J.; Lérida, C.G.; Panal, S.P.; Ángel, G.G.; Corchero, L.L.; Vega, M.J.R.; et al. Poststimulation time interval-dependent effects of motor cortex anodal tDCS on reaction-time task performance. Cogn. Affect. Behav. Neurosci. 2018, 18, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Summers, J.J.; Kang, N.; Cauraugh, J.H. Does transcranial direct current stimulation enhance cognitive and motor functions in the ageing brain? A systematic review and meta-analysis. Ageing Res. Rev. 2016, 25, 42–54. [Google Scholar] [CrossRef]
- Stagg, C.; Jayaram, G.; Pastor, D.; Kincses, Z.; Matthews, P.; Johansen-Berg, H.J.N. Polarity and timing-dependent effects of transcranial direct current stimulation in explicit motor learning. Neuropsychologia 2011, 49, 800–804. [Google Scholar] [CrossRef] [Green Version]
- Liao, W.-W.; Chiang, W.-C.; Lin, K.-C.; Wu, C.-Y.; Liu, C.-T.; Hsieh, Y.-W.; Lin, Y.-C.; Chen, C.-L. Timing-dependent effects of transcranial direct current stimulation with mirror therapy on daily function and motor control in chronic stroke: A randomized controlled pilot study. J. Neuroeng. Rehabil. 2020, 17, 101. [Google Scholar] [CrossRef]
- Cabral, M.E.; Baltar, A.; Borba, R.; Galvão, S.; Santos, L.; Fregni, F.; Monte-Silva, K.J.N. Transcranial direct current stimulation: Before, during, or after motor training? Neuroreport 2015, 26, 618–622. [Google Scholar] [CrossRef]
- Jin, M.; Zhang, Z.; Bai, Z.; Fong, K.N. Timing-Dependent interaction effects of tDCS with mirror therapy on upper extremity motor recovery in patients with chronic stroke: A randomized controlled pilot study. J. Neurol. Sci. 2019, 405, 116436. [Google Scholar] [CrossRef]
- Keele, S.W.; Ivry, R.; Mayr, U.; Hazeltine, E.; Heuer, H. The cognitive and neural architecture of sequence representation. Psychol. Rev. 2003, 110, 316–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyon, J.; Gabitov, E.; Vahdat, S.; Lungu, O.; Boutin, A. Current issues related to motor sequence learning in humans. Curr. Opin. Behav. Sci. 2018, 20, 89–97. [Google Scholar] [CrossRef]
- Rioult-Pedotti, M.-S.; Friedman, D.; Donoghue, J.P. Learning-induced LTP in neocortex. Science 2000, 290, 533–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garofalo, S.; Battaglia, S.; di Pellegrino, G. Individual differences in working memory capacity and cue-guided behavior in humans. Sci. Rep. 2019, 9, 7327. [Google Scholar] [CrossRef] [PubMed]
- Borgomaneri, S.; Serio, G.; Battaglia, S.J.C. Please, don’t do it! Ten years of progress of non-invasive brain stimulation in action inhibition. Cortex 2020, 132, 404–422. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Serio, G.; Scarpazza, C.; D’Ausilio, A.; Borgomaneri, S. Frozen in (e) motion: How reactive motor inhibition is influenced by the emotional content of stimuli in healthy and psychiatric populations. Behav. Res. Ther. 2021, 146, 103963. [Google Scholar] [CrossRef] [PubMed]
- Classen, J.; Liepert, J.; Wise, S.P.; Hallett, M.; Cohen, L.G. Rapid plasticity of human cortical movement representation induced by practice. J. Neurophysiol. 1998, 79, 1117–1123. [Google Scholar] [CrossRef] [Green Version]
- Saucedo Marquez, C.M.; Zhang, X.; Swinnen, S.P.; Meesen, R.; Wenderoth, N. Task-specific effect of transcranial direct current stimulation on motor learning. Front. Hum. Neurosci. 2013, 7, 333. [Google Scholar] [CrossRef] [Green Version]
- Russo, C.; Souza Carneiro, M.I.; Bolognini, N.; Fregni, F. Safety review of transcranial direct current stimulation in stroke. Neuromodulation 2017, 20, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Hashemirad, F.; Zoghi, M.; Fitzgerald, P.B.; Jaberzadeh, S. The effect of anodal transcranial direct current stimulation on motor sequence learning in healthy individuals: A systematic review and meta-analysis. Brain Cogn. 2016, 102, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Turi, Z.; Csifcsák, G.; Boayue, N.M.; Aslaksen, P.; Antal, A.; Paulus, W.; Groot, J.; Hawkins, G.E.; Forstmann, B.; Opitz, A. Blinding is compromised for transcranial direct current stimulation at 1 mA for 20 min in young healthy adults. Eur. J. Neurosci. 2019, 50, 3261–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.L.; Oliveira, R.M.; Rocha, F.o.R.; Abreu-Villaca, Y. Influences of handedness and gender on the grooved pegboard test. Brain Cogn. 2000, 44, 445–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W. Hand-grip dynamometry provides a valid indication of upper extremity strength impairment in home care patients. J. Hand Ther. 1998, 11, 258–260. [Google Scholar] [CrossRef]
- Kong, S.; Lee, K.S.; Kim, J.; Jang, S.H. The effect of two different hand exercises on grip strength, forearm circumference, and vascular maturation in patients who underwent arteriovenous fistula surgery. Ann. Rehabil. Med. 2014, 38, 648. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Reato, D.; Arlotti, M.; Gasca, F.; Datta, A.; Parra, L.C.; Bikson, M. Cellular effects of acute direct current stimulation: Somatic and synaptic terminal effects. J. Physiol. 2013, 591, 2563–2578. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, L.; Souza, I.C.; Vidor, L.; Souza, A.; Deitos, A.; Volz, M.S.; Fregni, F.; Caumo, W.; Torres, I.L. Neurobiological effects of transcranial direct current stimulation: A review. Front. Psychiatry 2012, 3, 110. [Google Scholar] [CrossRef] [Green Version]
- Nitsche, M.A.; Seeber, A.; Frommann, K.; Klein, C.C.; Rochford, C.; Nitsche, M.S.; Fricke, K.; Liebetanz, D.; Lang, N.; Antal, A. Modulating parameters of excitability during and after transcranial direct current stimulation of the human motor cortex. J. Physiol. 2005, 568, 291–303. [Google Scholar] [CrossRef]
- Kim, S.; Stephenson, M.C.; Morris, P.G.; Jackson, S.R.J.N. tDCS-induced alterations in GABA concentration within primary motor cortex predict motor learning and motor memory: A 7 T magnetic resonance spectroscopy study. Neuroimage 2014, 99, 237–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-H.; You, S.H.; Ko, M.-H.; Park, J.-W.; Lee, K.H.; Jang, S.H.; Yoo, W.-K.; Hallett, M.J.S. Repetitive transcranial magnetic stimulation–induced corticomotor excitability and associated motor skill acquisition in chronic stroke. Stroke 2006, 37, 1471–1476. [Google Scholar] [CrossRef] [Green Version]
- Ziemann, U.; Siebner, H.R. Modifying motor learning through gating and homeostatic metaplasticity. Brain Stimul. 2008, 1, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-W.; Ko, M.-H. Facilitation of corticospinal tract excitability by transcranial direct current stimulation combined with voluntary grip exercise. Neurosci. Lett. 2013, 548, 181–184. [Google Scholar] [CrossRef]
- Siebner, H.R.; Lang, N.; Rizzo, V.; Nitsche, M.A.; Paulus, W.; Lemon, R.N.; Rothwell, J. Preconditioning of low-frequency repetitive transcranial magnetic stimulation with transcranial direct current stimulation: Evidence for homeostatic plasticity in the human motor cortex. J. Neurosci. 2004, 24, 3379–3385. [Google Scholar] [CrossRef]
- Cooper, L.N.; Bear, M.F. The BCM theory of synapse modification at 30: Interaction of theory with experiment. Nat. Rev. Neurosci. 2012, 13, 798–810. [Google Scholar] [CrossRef]
- Bolognini, N.; Pascual-Leone, A.; Fregni, F. Using non-invasive brain stimulation to augment motor training-induced plasticity. J. Neuroeng. Rehabil. 2009, 6, 8. [Google Scholar] [CrossRef] [Green Version]
- Calderón, M.A.F.; Miralles, A.N.; Pimienta, M.J.; Estella, J.M.G.; Ledesma, M.J. Analysis of the factors related to the effectiveness of transcranial current stimulation in upper limb motor function recovery after stroke: A systematic review. J. Med. Syst. 2019, 43, 69. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, V.; Krebs, H.I.; Volpe, B.T.; Pascual-Leone, A.; Rykman, A.; Zeiarati, G.; Fregni, F.; Dipietro, L.; Thickbroom, G.; Edwards, D.J.N. Transcranial direct current stimulation (tDCS) and robotic practice in chronic stroke: The dimension of timing. NeuroRehabilitation 2013, 33, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Skogan, A.H.; Oerbeck, B.; Christiansen, C.; Lande, H.L.; Egeland, J. Updated developmental norms for fine motor functions as measured by finger tapping speed and the Grooved Pegboard Test. Dev. Neuropsychol. 2018, 43, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Derakhshanfar, M.; Raji, P.; Bagheri, H.; Jalili, M.; Tarhsaz, H. The effect of extroceptive and proprioceptive sensory stimulation on ADL and motor function of upper limb in stroke patients. Razi. J. Med. Sci. 2018, 25, 55–61. [Google Scholar]
- Cho, H.-S.; Cha, H.G. Effect of mirror therapy with tDCS on functional recovery of the upper extremity of stroke patients. J. Phys. Ther. Sci. 2015, 27, 1045–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CON (n = 12) | PRI (n = 13) | SHAM (n = 13) | p-Value | |
|---|---|---|---|---|
| Age (years) | 27.58 (9.12) | 25.69 (4.13) | 28.23 (12.54) | 0.820 2 |
| Sex | ||||
| Male | 9 (23.7%) | 7 (18.4%) | 7 (18.4%) | 0.464 3 |
| Female | 3 (7.9%) | 6 (15.8%) | 6 (15.8%) | |
| Non-dominant hand | ||||
| Right | 0 (0.0%) | 1 (2.6%) | 3 (7.9%) | 0.157 3 |
| Left | 12 (31.6%) | 12 (31.6%) | 10 (26.3%) | |
| Finger tapping task | ||||
| Skill | 0.15 (0.02) | 0.16 (0.01) | 0.15 (0.03) | 0.339 1 |
| Grooved pegboard test | ||||
| Time (s) | 66.61 (7.10) | 66.78 (7.83) | 68.11 (13.13) | 1.000 2 |
| Hand strength (Kg) | ||||
| Grip power | 37.28 (10.34) | 30.52 (11.00) | 27.37 (9.97) | 0.068 1 |
| Lateral pinch | 8.24 (1.97) | 7.01 (1.83) | 7.05 (2.07) | 0.220 1 |
| Palmar pinch | 7.39 (1.93) | 6.44 (1.04) | 6.56 (1.95) | 0.323 1 |
| Tip pinch | 5.26 (1.63) | 5.03 (1.00) | 5.42 (1.89) | 0.812 1 |
| Variables | Group | E1 | E2 | Intra-Group p-Value | Inter-Group p-Value |
|---|---|---|---|---|---|
| Finger tapping task (Skill) | CON | 0.15 (0.02) | 0.20 (0.03) | <0.001 1 | 0.498 3 |
| PRI | 0.16 (0.01) | 0.22 (0.02) | <0.001 1 | ||
| SHAM | 0.15 (0.03) | 0.20 (0.04) | 0.001 2 | ||
| Grooved pegboard test (s) | CON | 66.61 (7.10) | 62.71 (4.85) | 0.059 1 | 0.002 3 |
| PRI | 66.78 (7.83) | 62.36 (7.69) | 0.006 1 | ||
| SHAM | 68.11 (13.13) | 71.59 (11.79) | 0.050 1 | ||
| Grip power (Kg) | CON | 37.28 (10.34) | 35.96 (11.17) | 0.173 1 | 0.511 3 |
| PRI | 30.52 (11.00) | 30.50 (11.78) | 0.970 1 | ||
| SHAM | 27.37 (9.97) | 27.03 (10.22) | 0.708 1 | ||
| Lateral pinch (Kg) | CON | 8.24 (1.97) | 8.20 (2.04) | 0.839 1 | 0.156 3 |
| PRI | 7.01 (1.83) | 7.54 (1.77) | 0.027 1 | ||
| SHAM | 7.05 (2.07) | 7.09 (1.72) | 0.854 1 | ||
| Palmar pinch (Kg) | CON | 7.39 (1.93) | 7.13 (2.43) | 0.306 2 | 0.059 3 |
| PRI | 6.44 (1.04) | 7.14 (1.36) | 0.003 1 | ||
| SHAM | 6.56 (1.95) | 6.95 (2.07) | 0.166 1 | ||
| Tip pinch (Kg) | CON | 5.26 (1.63) | 5.49 (1.94) | 0.341 1 | 0.222 3 |
| PRI | 5.03 (1.00) | 5.60 (1.35) | 0.093 1 | ||
| SHAM | 5.42 (1.89) | 5.28 (1.53) | 0.641 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, N.-G.; Kim, G.-W.; Won, Y.H.; Park, S.-H.; Seo, J.-H.; Ko, M.-H. Timing-Dependent Effects of Transcranial Direct Current Stimulation on Hand Motor Function in Healthy Individuals: A Randomized Controlled Study. Brain Sci. 2021, 11, 1325. https://doi.org/10.3390/brainsci11101325
Jo N-G, Kim G-W, Won YH, Park S-H, Seo J-H, Ko M-H. Timing-Dependent Effects of Transcranial Direct Current Stimulation on Hand Motor Function in Healthy Individuals: A Randomized Controlled Study. Brain Sciences. 2021; 11(10):1325. https://doi.org/10.3390/brainsci11101325
Chicago/Turabian StyleJo, Nam-Gyu, Gi-Wook Kim, Yu Hui Won, Sung-Hee Park, Jeong-Hwan Seo, and Myoung-Hwan Ko. 2021. "Timing-Dependent Effects of Transcranial Direct Current Stimulation on Hand Motor Function in Healthy Individuals: A Randomized Controlled Study" Brain Sciences 11, no. 10: 1325. https://doi.org/10.3390/brainsci11101325
APA StyleJo, N.-G., Kim, G.-W., Won, Y. H., Park, S.-H., Seo, J.-H., & Ko, M.-H. (2021). Timing-Dependent Effects of Transcranial Direct Current Stimulation on Hand Motor Function in Healthy Individuals: A Randomized Controlled Study. Brain Sciences, 11(10), 1325. https://doi.org/10.3390/brainsci11101325