Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound with a 1.5 Tesla Scanner: A Prospective Intraindividual Comparison Study of Intraoperative Imaging

 ,
,  ,
, 

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Procedure Details
2.3. MRI Data Acquisition
2.4. MRI Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients
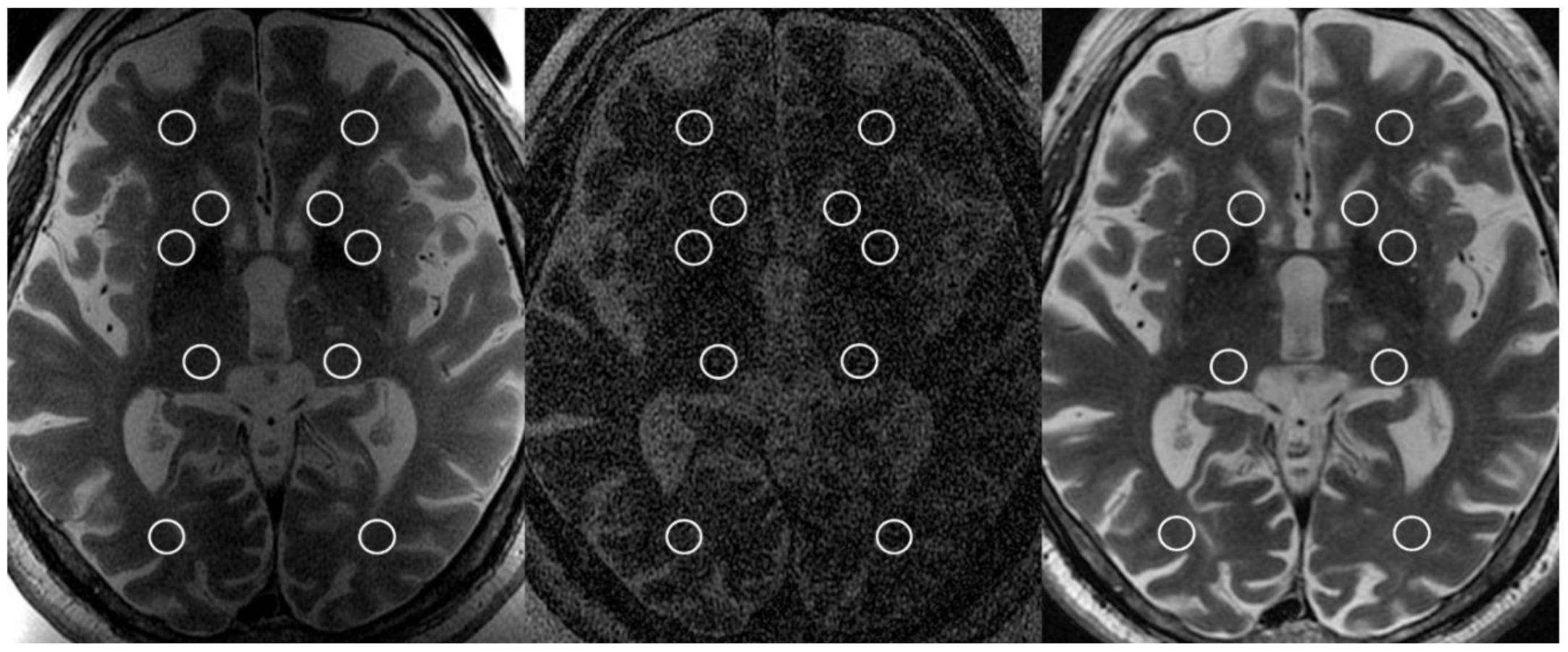
3.2. Signal-to-Noise Ratio
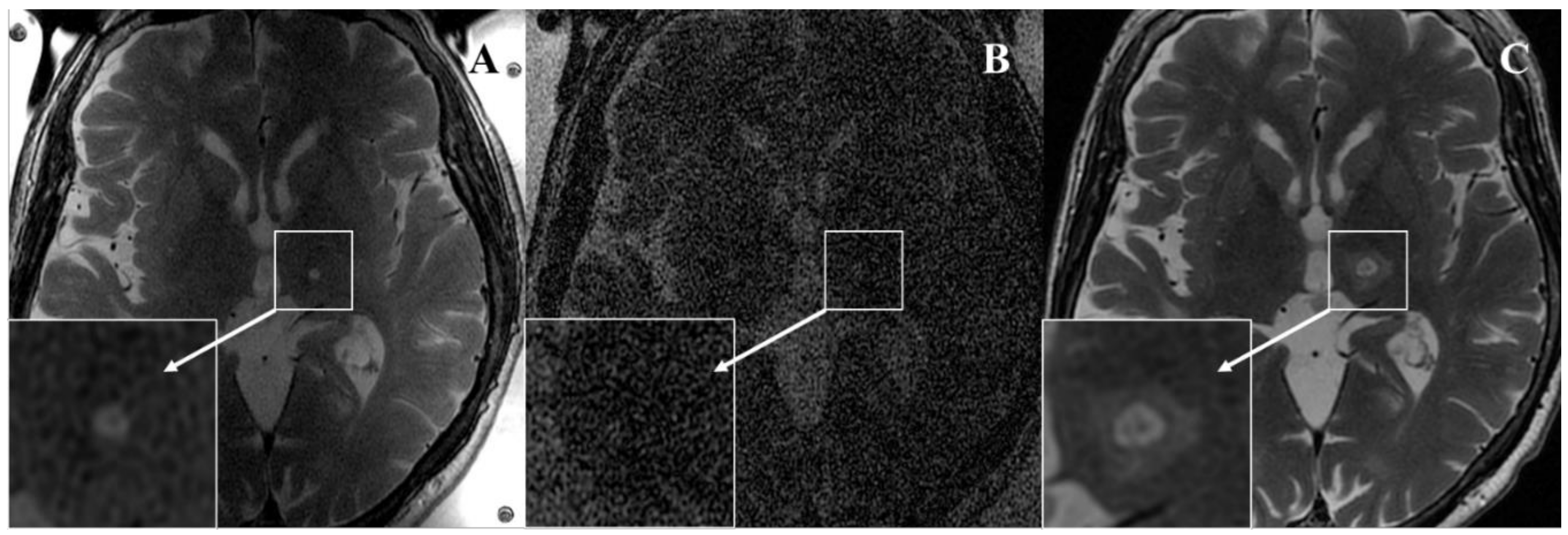
3.3. Qualitative Imaging Findings
4. Discussion and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elias, W.J.; Huss, D.; Voss, T.; Loomba, J.; Khaled, M.; Zadicario, E.; Frysinger, R.C.; Sperling, S.A.; Wylie, S.; Monteith, S.J.; et al. A pilot study of focused ultrasound thalamotomy for essential tremor. N. Engl. J. Med. 2013, 369, 640–648. [Google Scholar] [CrossRef]
- Elias, W.J.; Lipsman, N.; Ondo, W.G.; Ghanouni, P.; Kim, Y.G.; Lee, W.; Schwartz, M.; Hynynen, K.; Lozano, A.M.; Shah, B.B.; et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N. Engl. J. Med. 2016, 375, 730–739. [Google Scholar] [CrossRef]
- Chang, J.W.; Park, C.K.; Lipsman, N.; Schwartz, M.L.; Ghanouni, P.; Henderson, J.M.; Gwinn, R.; Witt, J.; Tierney, T.S.; Cosgrove, G.R.; et al. A prospective trial of magnetic resonance-guided focused ultrasound thalamotomy for essential tremor: Results at the 2-year follow-up. Ann. Neurol. 2018, 83, 107–114. [Google Scholar] [CrossRef]
- Magara, A.; Bühler, R.; Moser, D.; Kowalski, M.; Pourtehrani, P.; Jeanmonod, D. First experience with MR-guided focused ultrasound in the treatment of Parkinson’s disease. J. Ther. Ultrasound 2014, 2, 11. [Google Scholar] [CrossRef]
- Bond, A.E.; Shah, B.B.; Huss, D.S.; Dallapiazza, R.F.; Warren, A.; Harrison, M.B.; Sperling, S.A.; Wang, X.Q.; Gwinn, R.; Witt, J.; et al. Safety and Efficacy of Focused Ultrasound Thalamotomy for Patients with Medication-Refractory, Tremor-Dominant Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2017, 74, 1412–1418. [Google Scholar] [CrossRef]
- Jeanmonod, D.; Werner, B.; Morel, A.; Michels, L.; Zadicario, E.; Schiff, G.; Martin, E. Transcranial magnetic resonance imaging-guided focused ultrasound: Noninvasive central lateral thalamotomy for chronic neuropathic pain. Neurosurg. Focus 2012, 32, E1. [Google Scholar] [CrossRef]
- Ghanouni, P.; Pauly, K.B.; Elias, W.J.; Henderson, J.; Sheehan, J.; Monteith, S.; Wintermark, M. Transcranial MRI-Guided Focused Ultrasound: A Review of the Technologic and Neurologic Applications. AJR Am. J. Roentgenol. 2015, 205, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Druzgal, J.; Huss, D.S.; Khaled, M.A.; Monteith, S.; Raghavan, P.; Huerta, T.; Schweickert, L.C.; Burkholder, B.; Loomba, J.J.; et al. Imaging findings in MR imaging-guided focused ultrasound treatment for patients with essential tremor. AJNR Am. J. Neuroradiol. 2014, 35, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Federau, C.; Goubran, M.; Rosenberg, J.; Henderson, J.; Halpern, C.H.; Santini, V.; Wintermark, M.; Butts Pauly, K.; Ghanouni, P. Transcranial MRI-guided high-intensity focused ultrasound for treatment of essential tremor: A pilot study on the correlation between lesion size, lesion location, thermal dose, and clinical outcome. J. Magn. Reson. Imaging 2018, 48, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Gagliardo, C.; Midiri, M.; Cannella, R.; Napoli, A.; Wragg, P.; Collura, G.; Marrale, M.; Bartolotta, T.V.; Catalano, C.; Lagalla, R. Transcranial magnetic resonance-guided focused ultrasound surgery at 1.5T: A technical note. Neuroradiol. J. 2019, 32, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Iacopino, D.G.; Gagliardo, C.; Giugno, A.; Giammalva, G.R.; Napoli, A.; Maugeri, R.; Graziano, F.; Valentino, F.; Cosentino, G.; D’Amelio, M.; et al. Preliminary experience with a transcranial magnetic resonance-guided focused ultrasound surgery system integrated with a 1.5-T MRI unit in a series of patients with essential tremor and Parkinson’s disease. Neurosurg. Focus 2018, 44, E7. [Google Scholar] [CrossRef]
- Gagliardo, C.; Cannella, R.; Quarrella, C.; D’Amelio, M.; Napoli, A.; Bartolotta, T.V.; Catalano, C.; Midiri, M.; Lagalla, R. Intraoperative imaging findings in transcranial MR imaging-guided focused ultrasound treatment at 1.5T may accurately detect typical lesional findings correlated with sonication parameters. Eur. Radiol. 2020, 30, 5059–5070. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.I.; Chaibainou, H.; Wang, S.; Hitti, F.L.; McShane, B.J.; Tilden, D.; Korn, M.; Blanke, A.; Dayan, M.; Wolf, R.L.; et al. Focused Ultrasound Thalamotomy for Essential Tremor in the Setting of a Ventricular Shunt: Technical Report. Oper. Neurosurg. 2019, 17, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.S.; Jung, H.H.; Zadicario, E.; Rachmilevitch, I.; Tlusty, T.; Vitek, S.; Chang, J.W. Factors associated with successful magnetic resonance-guided focused ultrasound treatment: Efficiency of acoustic energy delivery through the skull. J. Neurosurg. 2016, 124, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.R.; Bond, A.E.; Dallapiazza, R.F.; Blanke, A.; Tilden, D.; Huerta, T.E.; Moosa, S.; Prada, F.U.; Elias, W.J. Transcranial magnetic resonance imaging-guided focused ultrasound thalamotomy for tremor: Technical note. Neurosurg. Focus 2018, 44, E3. [Google Scholar] [CrossRef]
- National Electrical Manufacturers Association (NEMA). Determination of Signal-to-Noise Ratio (SNR) in Diagnostic Magnetic Resonance Imaging. MS 1-2001; NEMA Standards Publication: Rosslyn, WV, USA, 2001. [Google Scholar]
- Werner, B.; Martin, E.; Bauer, R.; O’Gorman, R. Optimizing MR imaging-guided navigation for focused ultrasound interventions in the brain. AIP Conf. Proc. 2017, 1821, 120001. [Google Scholar]
- Harary, M.; Essayed, W.I.; Valdes, P.A.; McDannold, N.; Cosgrove, G.R. Volumetric analysis of magnetic resonance-guided focused ultrasound thalamotomy lesions. Neurosurg. Focus 2018, 44, E6. [Google Scholar] [CrossRef]
- Jung, H.H.; Chang, W.S.; Rachmilevitch, I.; Tlusty, T.; Zadicario, E.; Chang, J.W. Different magnetic resonance imaging patterns after transcranial magnetic resonance-guided focused ultrasound of the ventral intermediate nucleus of the thalamus and anterior limb of the internal capsule in patients with essential tremor or obsessive-compulsive disorder. J. Neurosurg. 2015, 122, 162–168. [Google Scholar]
- Coluccia, D.; Fandino, J.; Schwyzer, L.; O’Gorman, R.; Remonda, L.; Anon, J.; Martin, E.; Werner, B. First noninvasive thermal ablation of a brain tumor with MR-guided focused ultrasound. J. Ther. Ultrasound 2014, 2, 17. [Google Scholar] [CrossRef]
- Grasso, G.; Midiri, M.; Catalano, C.; Gagliardo, C. Transcranial Magnetic Resonance-Guided Focused Ultrasound Surgery for Brain Tumor Ablation: Are We Ready for This Challenging Treatment? World Neurosurg. 2018, 119, 438–440. [Google Scholar] [CrossRef]
- Jung, H.H.; Kim, S.J.; Roh, D.; Chang, J.G.; Chang, W.S.; Kweon, E.J.; Kim, C.H.; Chang, J.W. Bilateral thermal capsulotomy with MR-guided focused ultrasound for patients with treatment-refractory obsessive-compulsive disorder: A proof-of-concept study. Mol. Psychiatry 2015, 20, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Roh, D.; Jung, H.H.; Chang, W.S.; Kim, C.H.; Chang, J.W. A study of novel bilateral thermal capsulotomy with focused ultrasound for treatment-refractory obsessive-compulsive disorder: 2-year follow-up. J. Psychiatry Neurosci. 2018, 43, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.; Hamani, C.; Rabin, J.S.; Goubran, M.; Meng, Y.; Huang, Y.; Baskaran, A.; Sharma, S.; Ozzoude, M.; Richter, M.A.; et al. Magnetic resonance-guided focused ultrasound capsulotomy for refractory obsessive compulsive disorder and major depressive disorder: Clinical and imaging results from two phase I trials. Mol. Psychiatry 2020, 25, 1946–1957. [Google Scholar] [CrossRef] [PubMed]
- Kinfe, T.; Stadlbauer, A.; Winder, K.; Hurlemann, R.; Buchfelder, M. Incisionless MR-guided focused ultrasound: Technical considerations and current therapeutic approaches in psychiatric disorders. Expert Rev. Neurother. 2020, 20, 687–696. [Google Scholar] [CrossRef]
- Kinfe, T.; Stadlbauer, A.; Winder, K.; Hurlemann, R.; Buchfelder, M. Intracranial Applications of MR Imaging-Guided Focused Ultrasound. AJNR Am. J. Neuroradiol. 2017, 38, 426–431. [Google Scholar]
- Lipsman, N.; Meng, Y.; Bethune, A.J.; Huang, Y.; Lam, B.; Masellis, M.; Herrmann, N.; Heyn, C.; Aubert, I.; Boutet, A.; et al. Blood-brain barrier opening in Alzheimer’s disease using MR-guided focused ultrasound. Nat. Commun. 2018, 9, 2336. [Google Scholar] [CrossRef]
- Abrahao, A.; Meng, Y.; Llinas, M.; Huang, Y.; Hamani, C.; Mainprize, T.; Aubert, I.; Heyn, C.; Black, S.E.; Hynynen, K.; et al. First-in-human trial of blood-brain barrier opening in amyotrophic lateral sclerosis using MR-guided focused ultrasound. Nat. Commun. 2019, 10, 4373. [Google Scholar] [CrossRef]
- Mainprize, T.; Lipsman, N.; Huang, Y.; Meng, Y.; Bethune, A.; Ironside, S.; Heyn, C.; Alkins, R.; Trudeau, M.; Sahgal, A.; et al. Blood-Brain Barrier Opening in Primary Brain Tumors with Non-invasive MR-Guided Focused Ultrasound: A Clinical Safety and Feasibility Study. Sci. Rep. 2019, 9, 321. [Google Scholar] [CrossRef]
- Lee, E.J.; Fomenko, A.; Lozano, A.M. Magnetic Resonance-Guided Focused Ultrasound: Current Status and Future Perspectives in Thermal Ablation and Blood-Brain Barrier Opening. J. Korean Neurosurg. Soc. 2019, 62, 10–26. [Google Scholar] [CrossRef]
- Huang, Y.; Lipsman, N.; Schwartz, M.L.; Krishna, V.; Sammartino, F.; Lozano, A.M.; Hynynen, K. Predicting lesion size by accumulated thermal dose in MR-guided focused ultrasound for essential tremor. Med. Phys. 2018, 45, 4704–4710. [Google Scholar] [CrossRef]
- Pineda-Pardo, J.A.; Urso, D.; Martínez-Fernández, R.; Rodríguez-Rojas, R.; Del-Alamo, M.; Millar Vernetti, P.; Máñez-Miró, J.U.; Hernández-Fernández, F.; de Luis-Pastor, E.; Vela-Desojo, L.; et al. Transcranial Magnetic Resonance-Guided Focused Ultrasound Thalamotomy in Essential Tremor: A Comprehensive Lesion Characterization. Neurosurgery 2020, 87, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Gagliardo, C.; Marrale, M.; D’Angelo, C.; Cannella, R.; Collura, G.; Iacopino, G.; D’Amelio, M.; Napoli, A.; Bartolotta, T.V.; Catalano, C.; et al. Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound Treatment at 1.5 T: A Retrospective Study on Treatmentand Patient-Related Parameters Obtained From 52 Procedures. Front. Phys. 2020, 7, 223. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Axial FRFSE T2-Weighed Images | |||
|---|---|---|---|
| 2ch-FUS Coil | Body-RF Coil | 8ch-HEAD Coil | |
| Slice thickness (mm) | 2.0 | 2.0 | 2.0 |
| Slice gap | 0 | 0 | 0 |
| Number or slice | 19 | 19 | 19 |
| TR (ms) | 4461 | 4461 | 4380 |
| TE (ms) | 103 | 103 | 108 |
| Matrix | 384 × 288 | 384 × 288 | 320 × 288 |
| NEX | 2 | 2 | 5 |
| FOV (cm) | 22 × 22 | 22 × 22 | 24 × 24 |
| Acquisition time (min) | 4:06 | 4:06 | 4:06 |
| Characteristics | Number |
|---|---|
| Patients | 8 |
| Sex | |
| Males | 7 (87.5%) |
| Females | 1 (12.5%) |
| Age (years) | |
| Mean ± SD (range) | 74.1 ± 5.4 (65–81) |
| Thalamotomy side | |
| Left Vim | 8 (100%) |
| Right Vim | 0 (0%) |
| SDR | |
| Mean ± SD (range) | 0.48 ± 0.04 (0.42–0.59) |
| Skull area | |
| Mean ± SD (range) | 343.6 ± 18.2 (323–371) |
| Treatment elements | |
| Mean ± SD (range) | 948 ± 48.1 (839–996) |
| Number of sonications | |
| Mean ± SD (range) | 11.7 ± 2.1 (9–15) |
| Number of High-energy sonications (Stage IV) | |
| Mean ± SD (range) | 4.0 ± 1.0 (2–5) |
| Energy (Joule) | |
| Mean ± SD (range) | 11696.5 ± 6646.4 (4536–28062) |
| Power (Watt) | |
| Mean ± SD (range) | 628.7 ± 97.6 (438–791) |
| Time (seconds) | |
| Mean ± SD (range) | 19.5 ± 8.5 (11–41) |
| Maximum temperatures (°C) | |
| Mean ± SD (range) | 55.5 ± 2.7 (51–62) |
| Average temperatures (°C) | |
| Mean ± SD (range) | 52.7 ± 2.3 (49–57) |
| 2ch-FUS SNR | Body-RF SNR | 8ch-HEAD SNR | p Value 2ch-FUS vs. body-RF | p Value 2ch-FUS vs. 8ch-HEAD | ICC (95% CI) | |
|---|---|---|---|---|---|---|
| Reader 1 | 10.54 (9.05, 12.61) | 2.96 (2.77, 3.31) | 16.24 (13.10, 19.95) | <0.001 | <0.001 | 0.85 (0.78, 0.89) |
| Reader 2 | 9.52 (7.74, 11.36) | 2.99 (2.83, 3.26) | 13.24 (10.67, 18.31) | <0.001 | <0.001 |
| 2ch-FUS | Body-RF | 8ch-HEAD | p Value 2ch-FUS vs Body-RF | p Value 2ch-FUS vs 8ch-HEAD | k Value (95% CI) | |
|---|---|---|---|---|---|---|
| Zone I | ||||||
| Present | 0.82 (0.59, 1.00) | |||||
| Reader 1 | 6 (75.0) | 0 (0) | 8 (100) | 0.031 | 0.500 | |
| Reader 2 | 8 (100) | 0 (0) | 8 (100) | 0.008 | 1.000 | |
| Zone II | ||||||
| Present | 0.90 (0.71, 1.00) | |||||
| Reader 1 | 8 (100) | 1 (12.5) | 8 (100) | 0.016 | 1.00 | |
| Reader 2 | 8 (100) | 0 (0) | 8 (100) | 0.008 | 1.00 | |
| Zone III | ||||||
| Present | 0.91 (0.75, 1.00) | |||||
| Reader 1 | 3 (37.5) | 2 (25.0) | 8 (100) | 1.000 | 0.063 | |
| Reader 2 | 3 (37.5) | 3 (37.5) | 8 (100) | 1.000 | 0.063 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gagliardo, C.; Cannella, R.; D’Angelo, C.; Toia, P.; Salvaggio, G.; Feraco, P.; Marrale, M.; Iacopino, D.G.; D’Amelio, M.; La Tona, G.; et al. Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound with a 1.5 Tesla Scanner: A Prospective Intraindividual Comparison Study of Intraoperative Imaging. Brain Sci. 2021, 11, 46. https://doi.org/10.3390/brainsci11010046
Gagliardo C, Cannella R, D’Angelo C, Toia P, Salvaggio G, Feraco P, Marrale M, Iacopino DG, D’Amelio M, La Tona G, et al. Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound with a 1.5 Tesla Scanner: A Prospective Intraindividual Comparison Study of Intraoperative Imaging. Brain Sciences. 2021; 11(1):46. https://doi.org/10.3390/brainsci11010046
Chicago/Turabian StyleGagliardo, Cesare, Roberto Cannella, Costanza D’Angelo, Patrizia Toia, Giuseppe Salvaggio, Paola Feraco, Maurizio Marrale, Domenico Gerardo Iacopino, Marco D’Amelio, Giuseppe La Tona, and et al. 2021. "Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound with a 1.5 Tesla Scanner: A Prospective Intraindividual Comparison Study of Intraoperative Imaging" Brain Sciences 11, no. 1: 46. https://doi.org/10.3390/brainsci11010046
APA StyleGagliardo, C., Cannella, R., D’Angelo, C., Toia, P., Salvaggio, G., Feraco, P., Marrale, M., Iacopino, D. G., D’Amelio, M., La Tona, G., La Grutta, L., & Midiri, M. (2021). Transcranial Magnetic Resonance Imaging-Guided Focused Ultrasound with a 1.5 Tesla Scanner: A Prospective Intraindividual Comparison Study of Intraoperative Imaging. Brain Sciences, 11(1), 46. https://doi.org/10.3390/brainsci11010046