Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) Combined with Aerobic Exercise on the Recovery of Motor Function in Ischemic Stroke Rat Model



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Permanent Middle Cerebral Artery Occlusion Model (MCAO)
2.3. Neuromodulation
2.4. Aerobic Exercise
2.5. Garcia Test
2.6. Rotarod Test
2.7. Electrophysiological Evaluation
2.8. Histologic and Biochemical Evaluation
2.8.1. Infarct Volume Measurement
2.8.2. Western Blotting
3. Statistics
4. Results
4.1. Animals
4.2. Behavior Test
4.2.1. Rotarod Test
4.2.2. Garcia Test
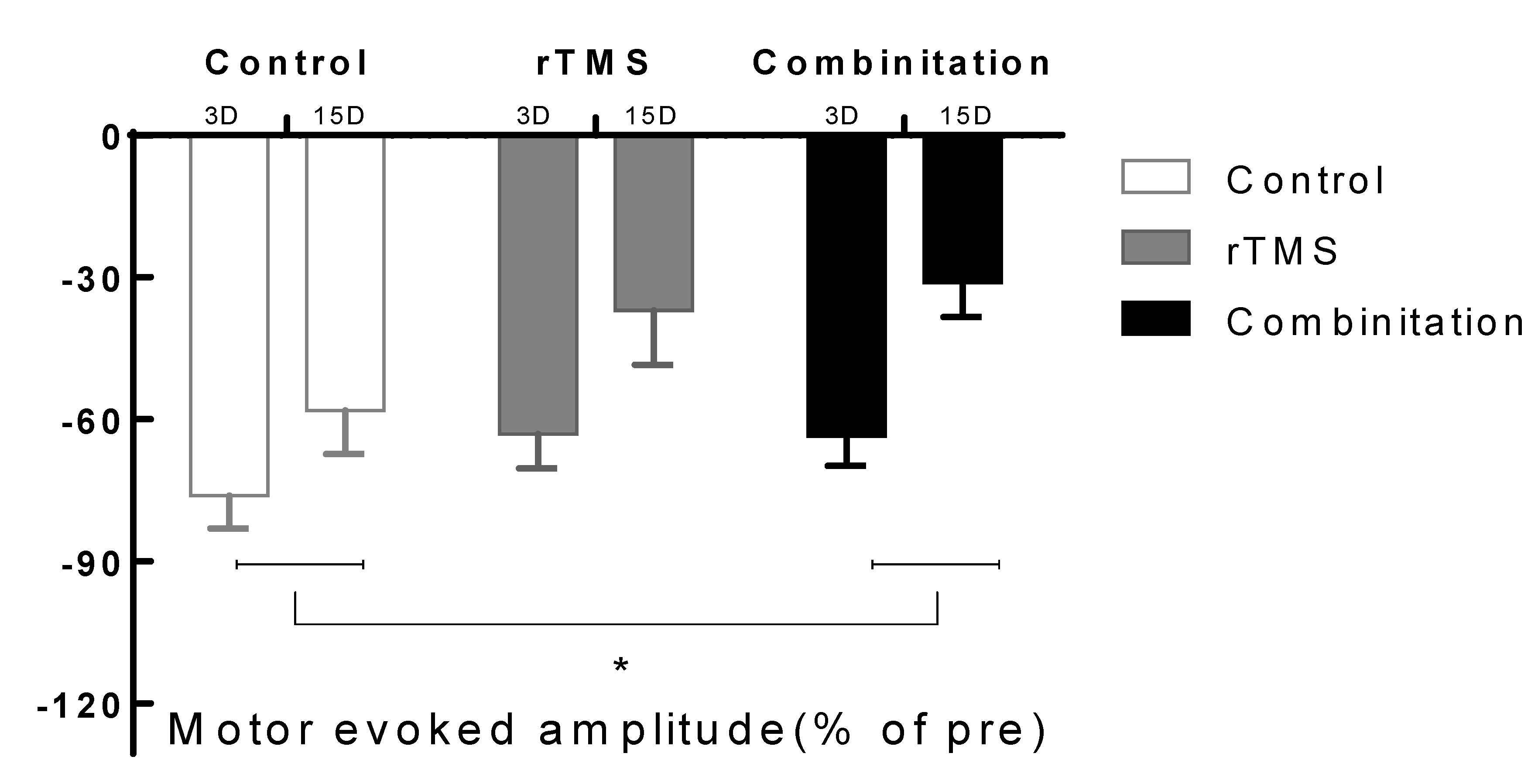
4.3. Electrophysiological Evaluation
4.4. Histologic and Biochemical Evaluation
4.4.1. Infarct Volume
4.4.2. Western Blotting
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, N.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics—2016 Update. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Thorsén, A.-M.; Holmqvist, L.W.; De Pedro-Cuesta, J.; Von Koch, L. A Randomized Controlled Trial of Early Supported Discharge and Continued Rehabilitation at Home after Stroke. Stroke 2005, 36, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Zheng, H.; Zhang, L.; Zhang, Q.; Li, L.; Pei, Z.; Hu, X. High-Frequency Repetitive Transcranial Magnetic Stimulation (rTMS) Improves Functional Recovery by Enhancing Neurogenesis and Activating BDNF/TrkB Signaling in Ischemic Rats. Int. J. Mol. Sci. 2017, 18, 455. [Google Scholar] [CrossRef]
- Guo, F.; Lou, J.; Han, X.; Deng, Y.; Huang, X. Repetitive Transcranial Magnetic Stimulation Ameliorates Cognitive Impairment by Enhancing Neurogenesis and Suppressing Apoptosis in the Hippocampus in Rats with Ischemic Stroke. Front. Physiol. 2017, 8, 559. [Google Scholar] [CrossRef]
- Yoon, K.J.; Lee, Y.-T.; Han, T.R. Mechanism of functional recovery after repetitive transcranial magnetic stimulation (rTMS) in the subacute cerebral ischemic rat model: Neural plasticity or anti-apoptosis? Exp. Brain Res. 2011, 214, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-W.; Bang, M.-S.; Han, T.-R.; Ko, Y.-J.; Yoon, B.-W.; Kim, J.-H.; Kang, L.-M.; Lee, K.-M.; Kim, M. Exercise increased BDNF and trkB in the contralateral hemisphere of the ischemic rat brain. Brain Res. 2005, 1052, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, K.; Sonoda, S.; Karasawa, N.; Yamada, K.; Shimpo, K.; Chihara, T.; Takeuchi, T.; Hasegawa, Y.; Kubo, K.-Y. Effects of exercise after focal cerebral cortex infarction on basal ganglion. Neurol. Sci. 2012, 34, 861–867. [Google Scholar] [CrossRef]
- Ferreira, A.F.B.; Real, C.; Rodrigues, A.C.; Alves, A.S.; Britto, L.R. Moderate exercise changes synaptic and cytoskeletal proteins in motor regions of the rat brain. Brain Res. 2010, 1361, 31–42. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, J.; Deng, Y.-H.; Zhang, P. The Effects of Early Exercise on Motor, Sense, and Memory Recovery in Rats with Stroke. Am. J. Phys. Med. Rehabil. 2017, 96, e36–e43. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Sakakima, H.; Khan, M.; Dhammu, T.S.; Shunmugavel, A.; Yoshida, Y.; Singh, I.; Singh, A.K. Stimulation of functional recovery via the mechanisms of neurorepair by S-nitrosoglutathione and motor exercise in a rat model of transient cerebral ischemia and reperfusion. Restor. Neurol. Neurosci. 2012, 30, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Li, J.; Lai, Q.; Rafols, J.A.; Luan, X.; Clark, J.; Diaz, F.G. Motor balance and coordination training enhances functional outcome in rat with transient middle cerebral artery occlusion. Neuroscience 2004, 123, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Lan, X.; Zhang, M.; Yang, W.; Zheng, Z.; Wu, Y.; Zeng, Q.; Liu, S.; Liu, K.; Li, G. Effect of treadmill exercise on 5-HT, 5-HT1A receptor and brain derived neurophic factor in rats after permanent middle cerebral artery occlusion. Neurol. Sci. 2013, 35, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.A.; Rallabandi, V.P.S.; Roy, P.K. Systems Biology of Immunomodulation for Post-Stroke Neuroplasticity: Multimodal Implications of Pharmacotherapy and Neurorehabilitation. Front. Neurol. 2016, 7, 103. [Google Scholar] [CrossRef]
- Jin, S.L.; Sohn, M.K.; Jee, S.J. Machanism Associated with Apoptosis after Repetitive Transcranial Magnetic Stimulation in Permanent Stroke Rat Model. J. Exp. Stroke Transl. Med. 2018, 11, 1–10. [Google Scholar]
- Chen, J.; Li, Y.; Wang, L.; Zhang, Z.; Lu, D.; Lu, M.; Chopp, M. Therapeutic benefit of intravenous administration of bone marrow stromal cells after cerebral ischemia in rats. Stroke 2001, 32, 1005–1011. [Google Scholar] [CrossRef]
- Garcia, J.H.; Wagner, S.; Liu, K.-F.; Hu, X.-J. Neurological Deficit and Extent of Neuronal Necrosis Attributable to Middle Cerebral Artery Occlusion in Rats. Stroke 1995, 26, 627–635. [Google Scholar] [CrossRef]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989, 20, 84–91. [Google Scholar] [CrossRef]
- Kim, Y.-H.; You, S.H.; Ko, M.-H.; Park, J.-W.; Lee, K.H.; Jang, S.H.; Yoo, W.; Hallett, M. Repetitive Transcranial Magnetic Stimulation–Induced Corticomotor Excitability and Associated Motor Skill Acquisition in Chronic Stroke. Stroke 2006, 37, 1471–1476. [Google Scholar] [CrossRef]
- Vanderwerker, C.J.; Ross, R.E.; Stimpson, K.H.; Embry, A.E.; Aaron, S.; Cence, B.; George, M.S.; Gregory, C.M. Combining therapeutic approaches: rTMS and aerobic exercise in post-stroke depression: A case series. Top. Stroke Rehabil. 2017, 25, 61–67. [Google Scholar] [CrossRef]
- Yang, Y.-R.; Tseng, C.-Y.; Chiou, S.-Y.; Liao, K.-K.; Cheng, S.-J.; Lai, K.-L.; Wang, R.-Y. Combination of rTMS and Treadmill Training Modulates Corticomotor Inhibition and Improves Walking in Parkinson Disease. Neurorehabilit. Neural Repair 2012, 27, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.-L.; Yan, L.; Guan, Y.-Z.; Cui, L.-Y. Effects of transcranial magnetic stimulation on motor cortical excitability and neurofunction after cerebral ischemia-reperfusion injury in rats. Chin. Med. Sci. J. 2005, 20, 226–230. [Google Scholar] [PubMed]
- Zhang, Q.-W.; Deng, X.-X.; Sun, X.; Xu, J.-X.; Sun, F.-Y. Exercise Promotes Axon Regeneration of Newborn Striatonigral and Corticonigral Projection Neurons in Rats after Ischemic Stroke. PLoS ONE 2013, 8, e80139. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, S.; Sakakima, H.; Sumizono, M.; Takada, S.; Terashi, T.; Yoshida, Y. The neuroprotective effects of preconditioning exercise on brain damage and neurotrophic factors after focal brain ischemia in rats. Behav. Brain Res. 2016, 303, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Pin-Barre, C.; Constans, A.; Brisswalter, J.; Pellegrino, C.; Laurin, J. Effects of High- Versus Moderate-Intensity Training on Neuroplasticity and Functional Recovery After Focal Ischemia. Stroke 2017, 48, 2855–2864. [Google Scholar] [CrossRef]
- Kim, M.-Y.; Lee, J.-U.; Hwang, B.-Y. The Effect of Low Frequency Repetitive Transcranial Magnetic Stimulation Combined with Range of Motion Exercise on Paretic Hand Function in Female Patients after Stroke. Neurosci. Med. 2013, 4, 77–83. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, X.; Luo, J.; Li, L.; Chen, X.; Ruxun, H.; Pei, Z. Physical exercise improves functional recovery through mitigation of autophagy, attenuation of apoptosis and enhancement of neurogenesis after MCAO in rats. BMC Neurosci. 2013, 14, 46. [Google Scholar] [CrossRef]
- Chen, A.; Xiong, L.-J.; Tong, Y.; Mao, M. The neuroprotective roles of BDNF in hypoxic ischemic brain injury. Biomed. Rep. 2012, 1, 167–176. [Google Scholar] [CrossRef]
- Jung, S.H.; Shin, J.E.; Jeong, Y.-S.; Shin, H.-I. Changes in motor cortical excitability induced by high-frequency repetitive transcranial magnetic stimulation of different stimulation durations. Clin. Neurophysiol. 2008, 119, 71–79. [Google Scholar] [CrossRef]
- Ploughman, M.; Austin, M.W.; Glynn, L.; Corbett, D.; Alcock, L. The Effects of Poststroke Aerobic Exercise on Neuroplasticity: A Systematic Review of Animal and Clinical Studies. Transl. Stroke Res. 2014, 6, 13–28. [Google Scholar] [CrossRef]
- Berretta, A.; Tzeng, Y.-C.; Clarkson, A. Post-stroke recovery: The role of activity-dependent release of brain-derived neurotrophic factor. Expert Rev. Neurother. 2014, 14, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Ploughman, M.; Windle, V.; MacLellan, C.L.; White, N.; Doré, J.J.; Corbett, D. Brain-Derived Neurotrophic Factor Contributes to Recovery of Skilled Reaching After Focal Ischemia in Rats. Stroke 2009, 40, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, F.; Sakakima, H.; Yoshida, Y. The effects of early exercise on brain damage and recovery after focal cerebral infarction in rats. Acta Physiol. 2010, 201, 275–287. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, J.; Kim, C.-S.; Kim, Y.; Sohn, M.K.; Jee, S. Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) Combined with Aerobic Exercise on the Recovery of Motor Function in Ischemic Stroke Rat Model. Brain Sci. 2020, 10, 186. https://doi.org/10.3390/brainsci10030186
Cui J, Kim C-S, Kim Y, Sohn MK, Jee S. Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) Combined with Aerobic Exercise on the Recovery of Motor Function in Ischemic Stroke Rat Model. Brain Sciences. 2020; 10(3):186. https://doi.org/10.3390/brainsci10030186
Chicago/Turabian StyleCui, Juanxiu, Cuk-Seong Kim, Yeongwook Kim, Min Kyun Sohn, and Sungju Jee. 2020. "Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) Combined with Aerobic Exercise on the Recovery of Motor Function in Ischemic Stroke Rat Model" Brain Sciences 10, no. 3: 186. https://doi.org/10.3390/brainsci10030186
APA StyleCui, J., Kim, C.-S., Kim, Y., Sohn, M. K., & Jee, S. (2020). Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) Combined with Aerobic Exercise on the Recovery of Motor Function in Ischemic Stroke Rat Model. Brain Sciences, 10(3), 186. https://doi.org/10.3390/brainsci10030186