1. Introduction
At an international level, there are many studies on health impacts due to occupational and environmental exposure to noise. In general, these studies were developed using voluminous samples involving patient reports, distributing questionnaires, adopting cross-sectional studies based on databases, and comparing environmental noise levels measured using criteria curves. However, there are still few studies focusing exclusively on health impacts and discomfort due to low-frequency noise. One of the main reasons is the low sensitivity of the human auditory system to low frequencies. On the other hand, this type of noise has very particular characteristics and causes much more discomfort and long-term non-auditory effects [
1,
2,
3,
4].
Until the 1930s, it was believed that the effects of noise on health were restricted only to hearing loss. In a study published in the Journal of the Acoustical Society of America, Jüichi Obata et al. [
5] concluded that the effects of noise on human health went beyond hearing loss.
The 1970s were marked by the emergence of a series of studies addressing the annoyance caused by environmental noise [
3,
6,
7,
8,
9,
10,
11]. The most cited effects on human health refer to emotional changes, such as agitation and distraction [
12,
13,
14,
15,
16,
17], in addition to the association of low-frequency noise with cognitive alterations [
18], the development of cardiovascular diseases [
19,
20,
21], sleep disorders [
22,
23], and high blood pressure [
24].
Thus, the effects of noise pollution comprise “auditory effects”, which directly affect the human auditory system and “non-auditory effects”, i.e., the impact of noise on physiological functions. Regarding “non-hearing effects”, discomfort has been reported as the most frequent effect caused by exposure to low-frequency noise in humans [
5,
25,
26].
In addition, discomfort may vary from individual to individual and depends not only on the noise pressure levels but also on the exposure time, as well as the low frequency components present in the noise. Thus, noise levels that contain low frequency components tend to be more annoying than noise without such components [
5,
27].
Since 2000, the World Health Organization has recognized low-frequency noise as an environmental problem. In addition, the health impacts of low-frequency components on noise are estimated to be more severe [
5].
As urbanization has increased, noise pollution has become more acute and is currently the second most harmful environmental stressor in Europe. In Europe, this type of pollution has been considered a public health problem, whereby Portugal ranks fourth as the most affected country concerning noise pollution (23.0% of the population is affected by this type of pollution—[
28]). In Portugal, the northern region is the territory that suffers the most demographic pressure and where the electrical substation with the highest voltage at national level is located, the Substation of Riba d’Ave (south-west of the municipality of Guimarães). The village of Serzedelo is one of the 69 villages (until 2013) in the municipality of Guimarães and has the largest installed electrical substation in the country. Moreover, 80% of the region is under the influence of power poles and power lines, including 90 power poles and 12 power lines of high and very high voltage. In a survey carried out in 2010 by Azevedo [
29], out of the 1022 dwellings located in the village of Serzedelo, only 98 are at 250 m or more from the power poles and power lines of high and very high voltage, that is, 9.6% are very close to these elements (up to 250 m) [
29]. This generates a conflict regarding the use of space. Alves et al. (2015), in an evaluation of the impact of low-frequency noise pollution on the population of the village of Serzedelo, concluded that the measured low-frequency sound levels exceeded the criterion curve of the Department for Environment, Food and Rural Affairs methodology [
30], which makes that type of noise audible and annoying to the population.
Based on these assumptions, the guiding questions that underlie the present investigation are the following: (1) Do power poles and power lines cause discomfort due to low frequency noise? (2) Do power poles and power lines affect the quality of life of the population?
The noise levels emitted by power poles and power lines can be a potential source of low frequency noise and discomfort in residential areas [
1,
31]. Nevertheless, how the population perceives the noise emitted by power poles and power lines should be determined, corresponding to a more subjective approach and complementing a more objective approach. Thus, this article aims to analyze the impacts of low frequency sound pollution, emitted by power poles and power lines, in two predominantly urban areas of the municipality of Guimarães (north-western Portugal), from the objective approaches (noise level and sound recording measurements) and the subjective assessment of noise discomfort (distributing surveys to the resident population and adapted audiometric test performance). It is hypothesized that people living in these spaces develop more health problems (e.g., insomnia, irritation, depression) than those living far away from these places.
This research comprises a study of “exposed” and “unexposed” individuals carried out in the village of Serzedelo, which was classified as an “exposed” territory because of the high concentration of power poles and power lines. The second concerns the village of Abação (São Tomé) classified as “unexposed” due to the inexistence of this type of infrastructure.
At an international level, existing production concerning the low frequency noise still remains very low. This paper can contribute to more complete methodologies to assess low-frequency noise discomfort. Additionally, it not only considers objective evaluation parameters (noise level measurement), but it also takes into account the perception of discomfort obtained from the surveys and the audiometric tests adapted to low frequencies. In addition, this type of study can contribute to the formulation of public policies in terms of installing power poles and power lines in residential areas.
This article is structured in four sections. This section includes a literature review on noise pollution, as well as impacts on the well-being of the population and an introduction to the subject.
Section 2 presents the methodology used in the objective and subjective dimensions of the investigation.
Section 3 comprises the results and the discussion. In
Section 4, we present some conclusions obtained from this investigation and suggestions for future investigations.
4. Conclusions
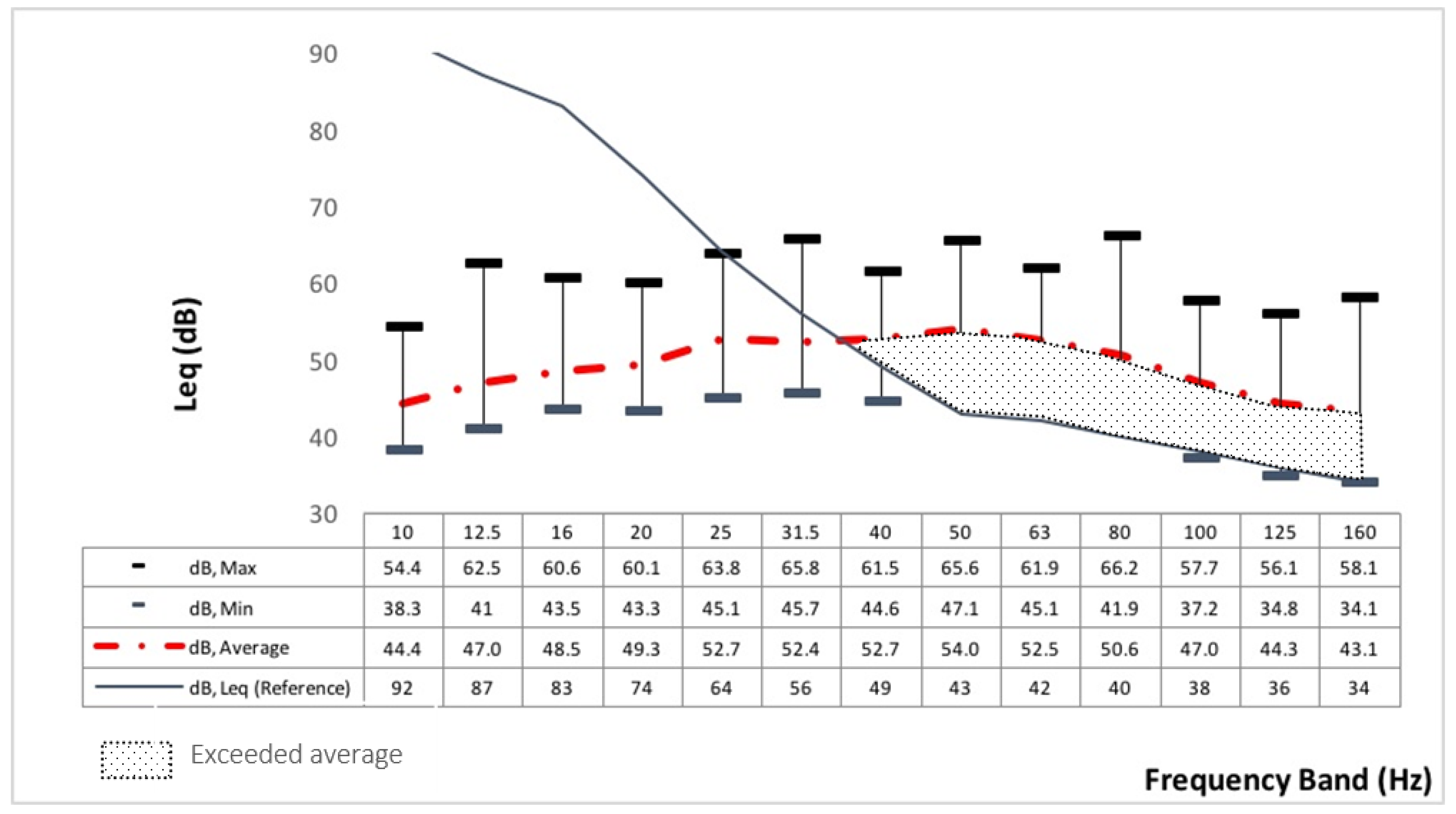
The research carried out reveals a novelty in Portugal, whether in the social sciences or the more exact ones, such as environmental acoustics. The originality of the research derived from considering the health impacts on the population due to the noise emitted by the power poles and power lines in residential areas, from the sound level measurements, besides distributing surveys and adapted audiometric test performance. Regarding the first question formulated in the introduction to this paper, “Do power poles and power lines cause discomfort due to low-frequency noise?” the distance between the receiver and the source may interfere with the degree of discomfort experienced by individuals. Especially due to the specific characteristics of high propagation of low-frequency noise and its low absorption by materials and the environment. For the results presented here, the sound was recorded to 5 m of distance from the source (400 kV power pole) and was audible to the “exposed” and “unexposed” volunteers during the adapted audiometric tests. The noise level measurements exceeded the criterion curve of the DEFRA methodology [
30]. The difference in the exceeded average of 4.3 dB shows a considerable difference between the two villages. If the source evaluated was only from the power poles and power lines, it could be induced that in the “exposed” group, the source more than doubled compared to the “unexposed” group.
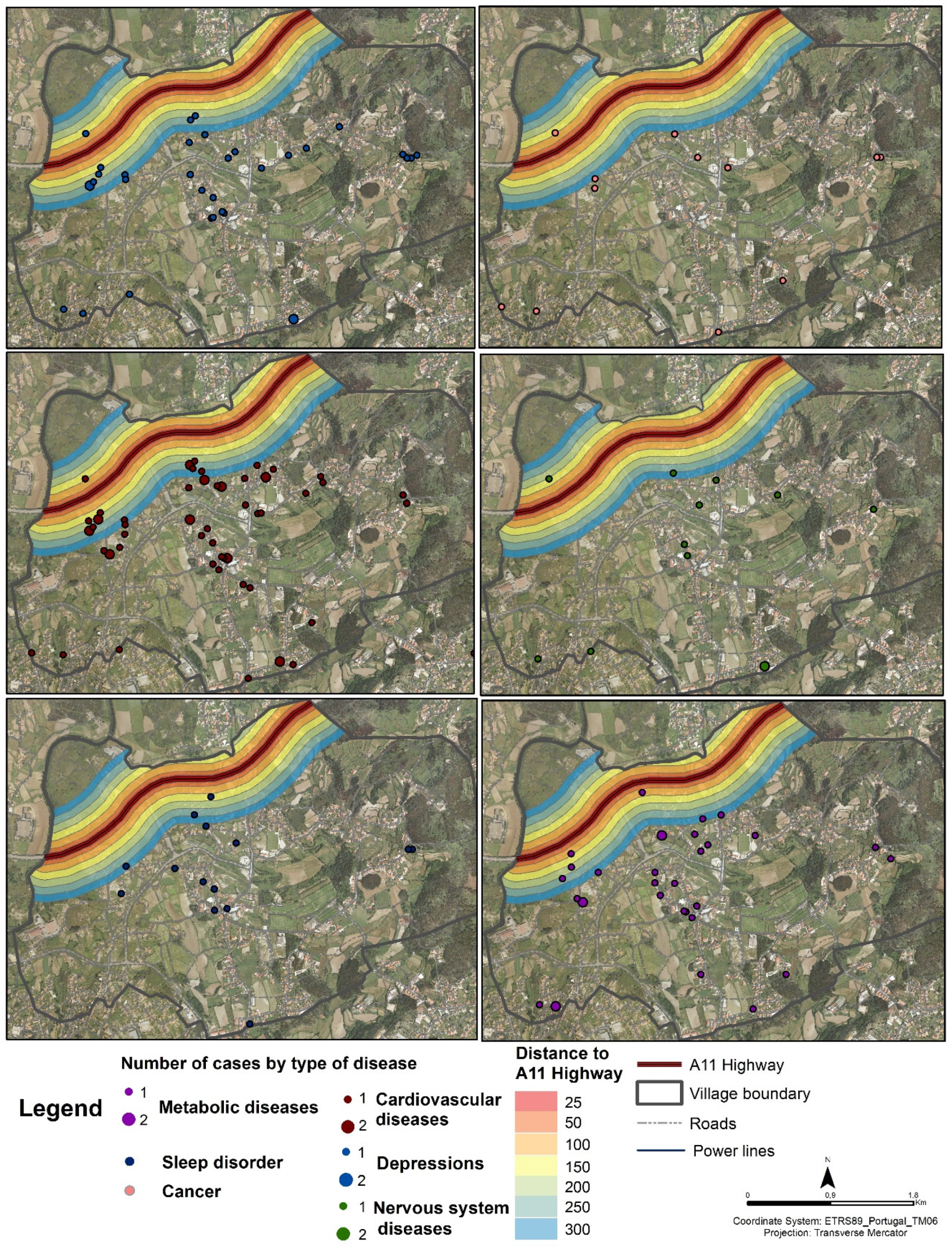
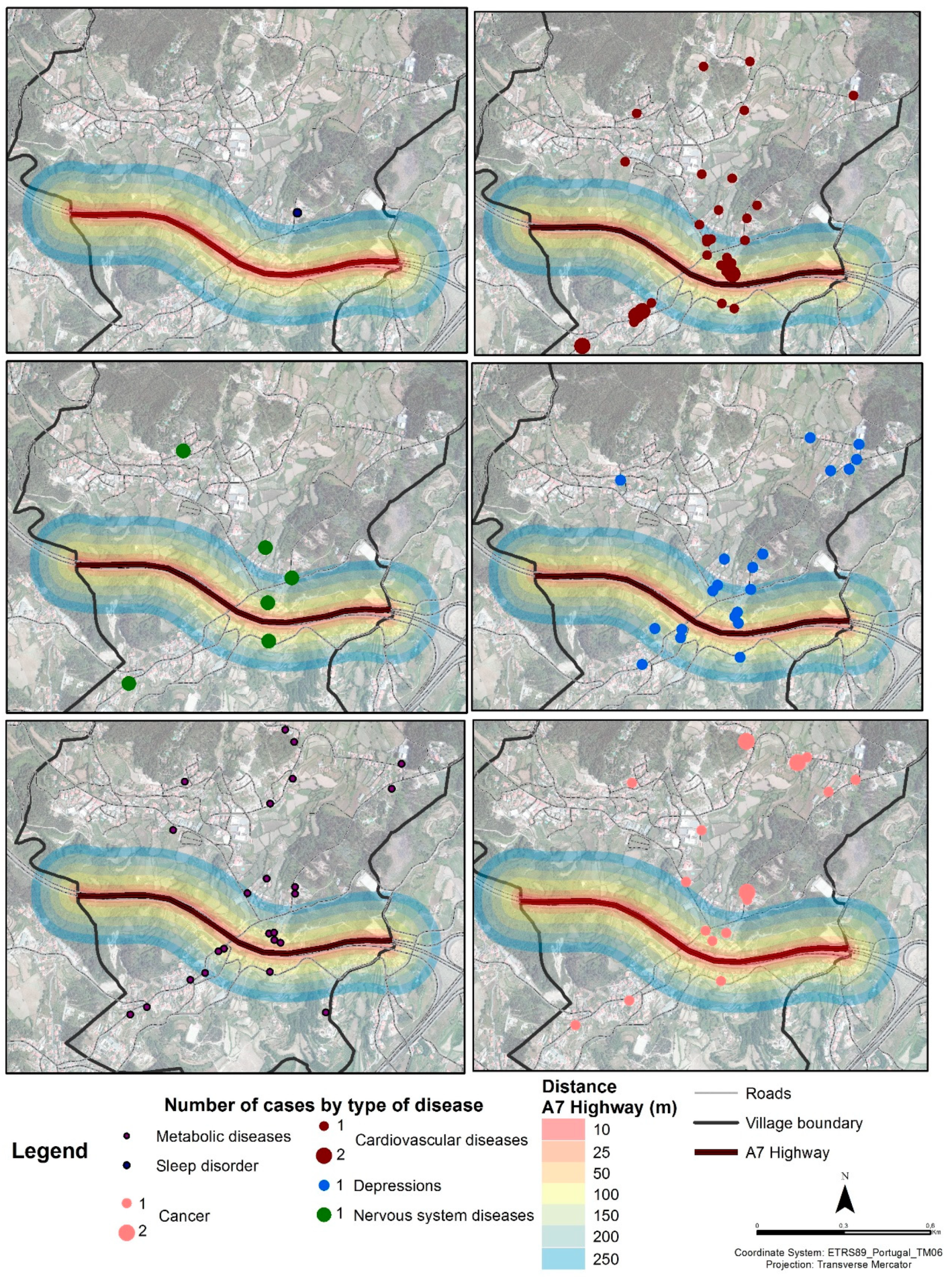
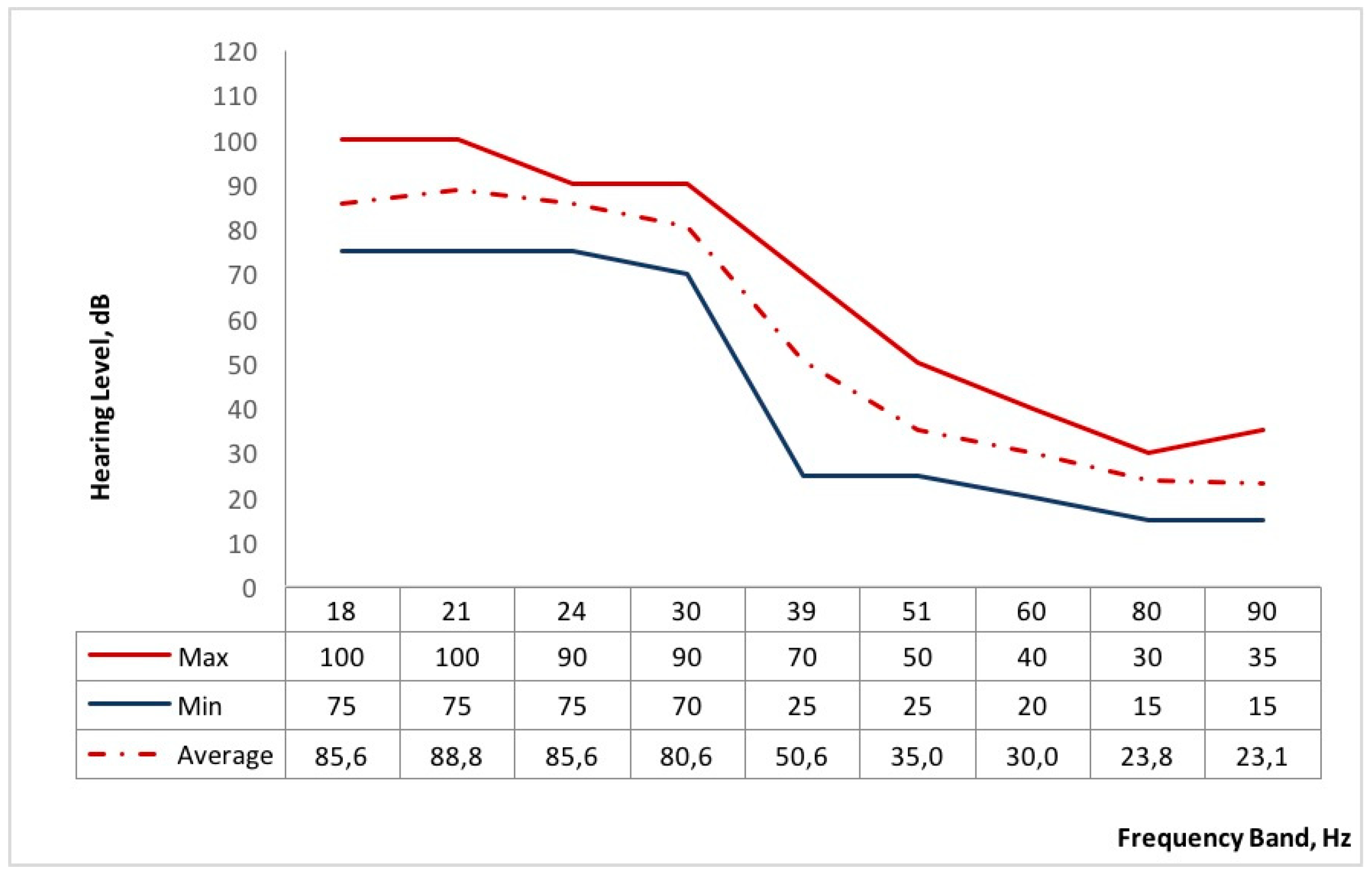
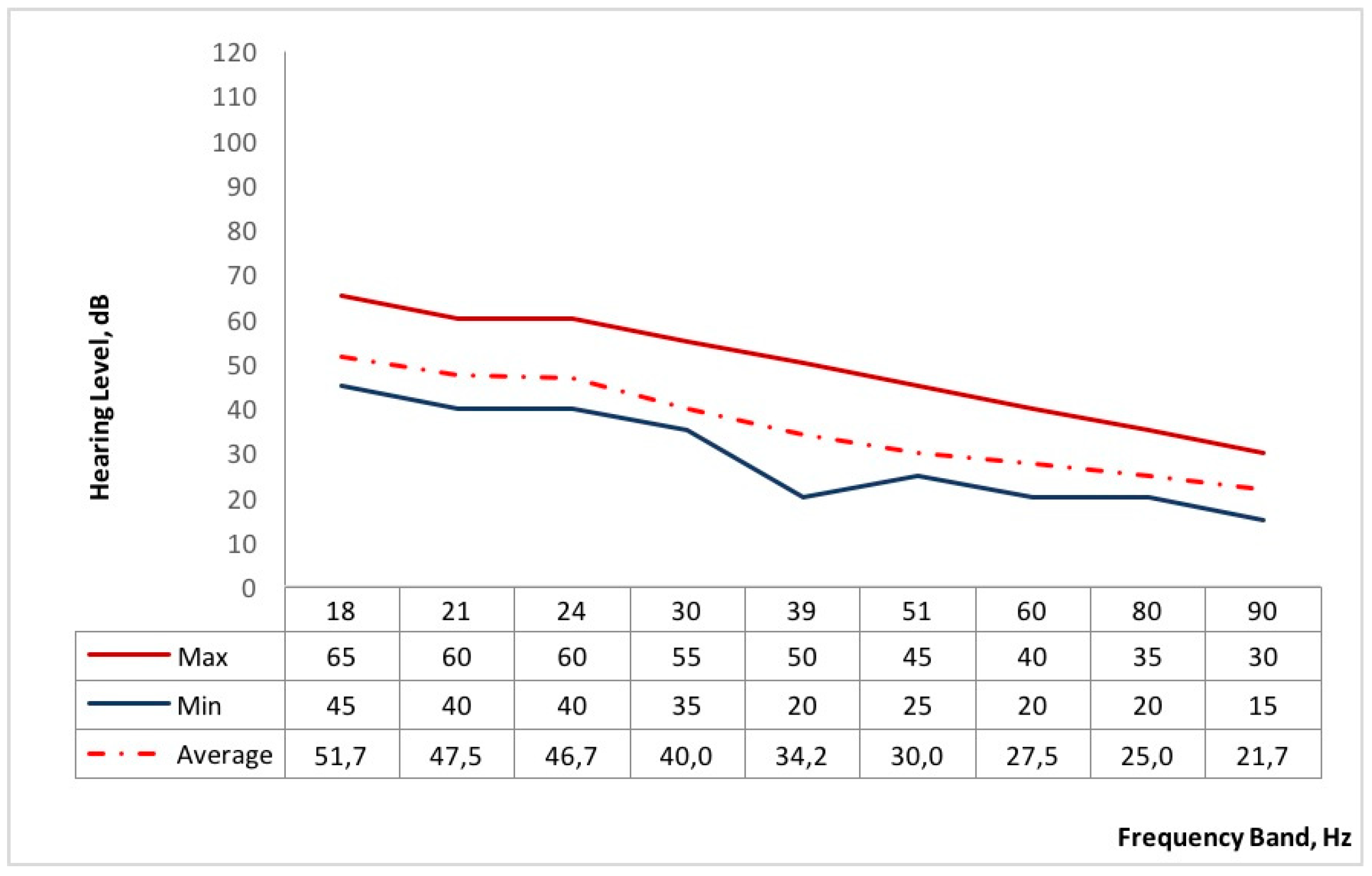
Regarding the second question, “Do power poles and power lines affect the population’s quality of life”?, the results of the audiometric tests showed a significant difference between the two groups, mainly the hearing threshold below 39 Hz, which shows that the “exposed” volunteers are not very sensitive to the low frequencies. This implies that the “exposed” group needs a greater sound intensity to perceive the noise, especially in the lower frequencies. As most interviewees have lived most of their lives in Serzedelo, this low sensitivity to low frequencies could be a consequence of the long period of exposure to the noise emitted by power poles and power lines. In turn, the “unexposed” group tends to perceive the noise at a slightly lower sound intensity due to the fact that this village is free from these infrastructures. Additionally, the “exposed” group has a greater number of respondents with health problems (e.g., cardiovascular diseases, insomnia and depression), which may be caused from the characteristics of the place where they live and, probably mainly, from exposure to low-frequency noise emitted by power poles and power lines.
Case-control type studies seem to be the most appropriate for the continuation of this type of research. It is essential to monitor the daily life of the interviewees and their lifestyles (for example, diet and sleep quality), aspects related to work dynamics such as current occupation and previous occupation, genetic predispositions, that is, the history of cases of illness in the immediate family circle, and the characteristics of the structure of the house. However, it is worth mentioning the complexity of conducting a case-control study, due to the difficulty of accessing information on patient morbidity and access to the patient database that is subject to confidentiality. In addition, a study of this nature would take several years.
It is expected that in future studies this type of evaluation can be explored by varying the distance between the receiver and the source. This may provide important information on the definition of the limits for installing power poles and power lines in residential areas, based not only on the objective component (measurement of sound levels and setting the minimum limit of evaluation below the usual 50 Hz), but also considering the subjective component, that is, the perception of discomfort reported by the exposed population.
Finally, we propose that investigations of this type should consider the subjective parameters for the evaluation of noise discomfort, that is, the perception of the population.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}