A Parametric Identification Method of Human Gait Differences and its Application in Rehabilitation



Abstract
1. Introduction
2. Methods
2.1. Participants
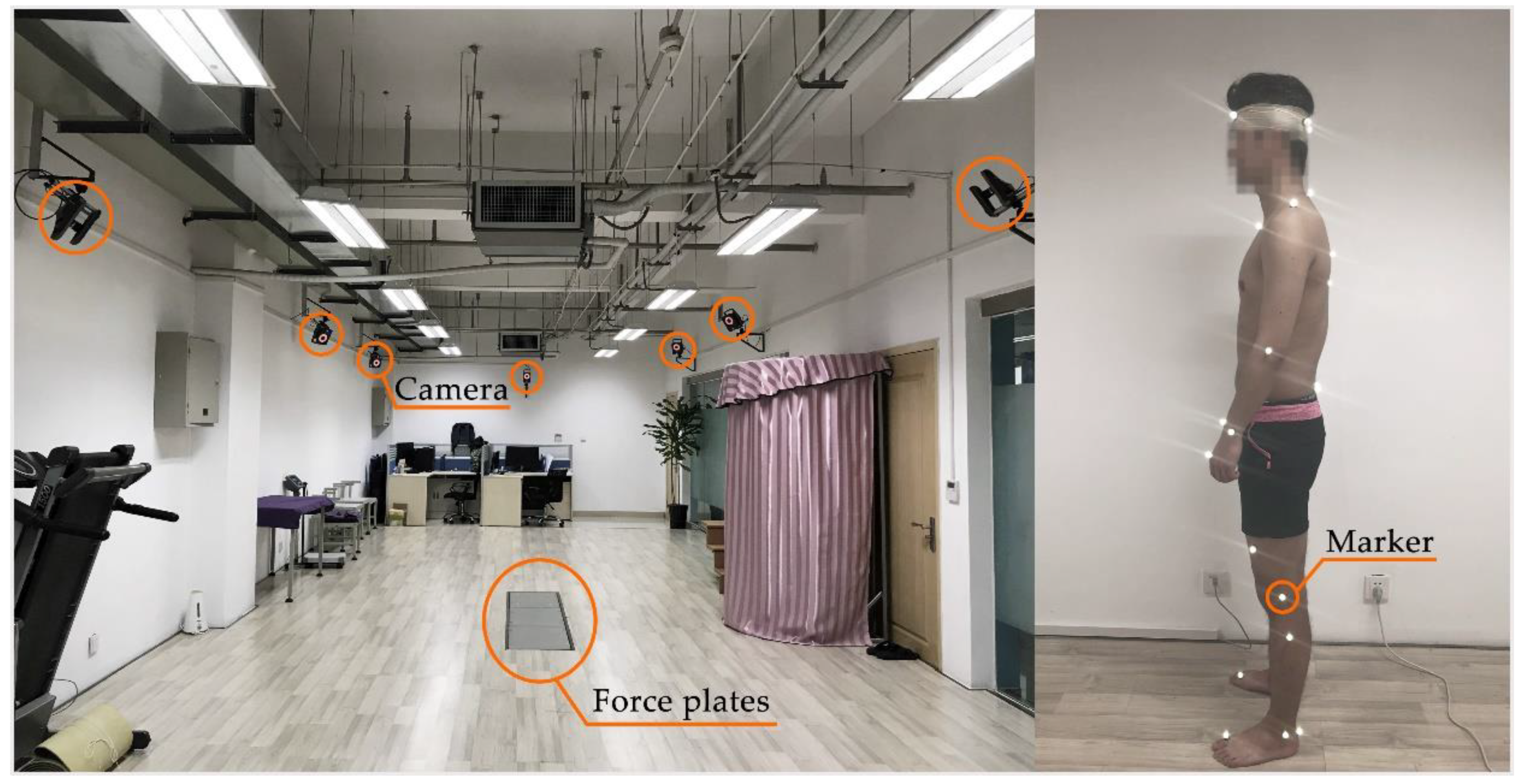
2.2. Data Collection and Processing
2.3. Mathematical Model Application
2.3.1. Mathematical Definition of GE-Bézier Curve
2.3.2. Geometric Properties
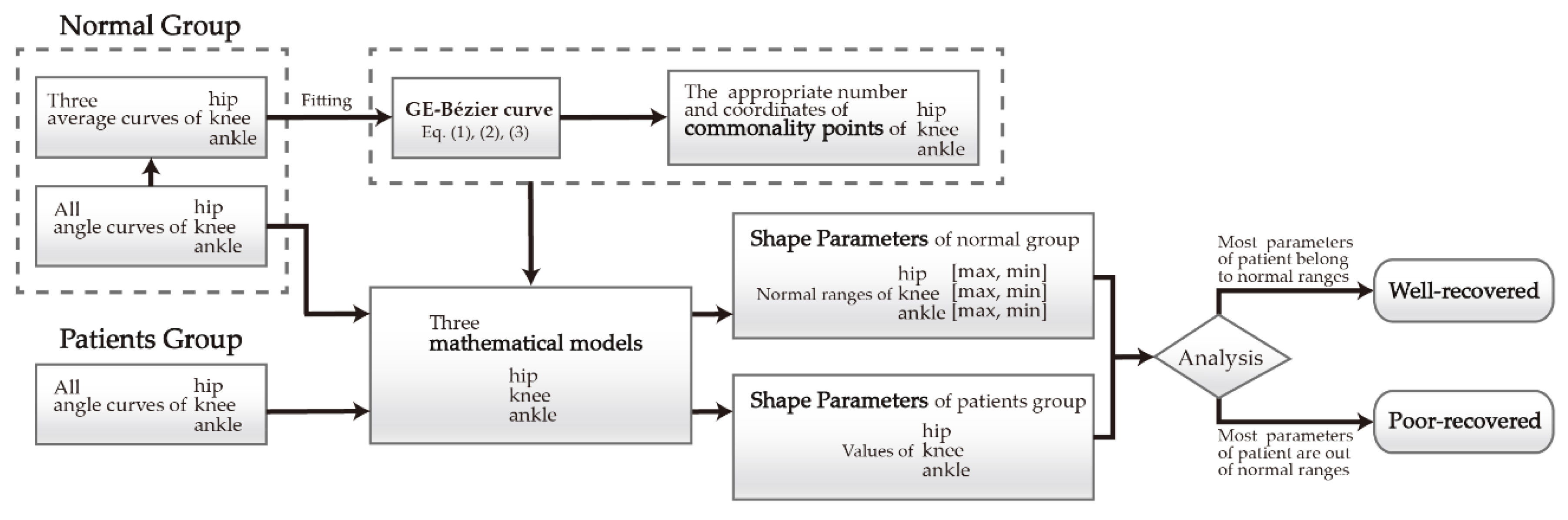
2.4. The Process of Implementation
3. Results
3.1. Normal Group
3.2. Patient Group
4. Discussion
4.1. Effects of Shape Parameters in Rehabilitation
4.2. Effects of Shape Parameters in Walking Postures
5. Conclusions
- The mathematical models were provided for the gait data of each participant, which not only contain the individual gait personality but also present the general gait regularity. In the models, the gait curve shapes of different participants in the same joint can be controlled by one group of commonality points, and the differences among local details of curves were reflected by different local shape parameters.
- For the normal ranges of shape parameters summarized from the normal group in this paper, they can be used as references for distinguishing normal and abnormal gait. The gait could be considered normal if shape parameters in the patient group belonged to these ranges, and if they were exceeded, especially for parameters with larger weights, the gait tended to be abnormal.
- The excess degrees of abnormal parameters can play a certain role in assisting the evaluation of the recovery status of patients. In this context, the degree of abnormal parameters of patients in the second month recovery period significantly exceeded those in the recovery period of six months, indicating that the former has a poor recovery status to a large extent.
- Shape parameters can help analyze abnormal postures during walking. For the patients with an ankle fracture in this paper, it could be estimated that the flexion movements of three lower joints were limited to various degrees corresponding to the abnormal parameters, and these abnormal gait characteristics can in return provide references for rehabilitation guidance.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Afiah, I.N.; Nakashima, H.; Loh, P.Y.; Muraki, S. An exploratory investigation of changes in gait parameters with age in elderly Japanese women. SpringerPlus 2016, 5, 1069–1083. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Changes in gait symmetry and velocity after stroke: A cross-sectional study from weeks to years after stroke. Neurorehabil. Neural Repair 2010, 24, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Worsley, P.; Whatling, G.; Barrett, D.; Holt, C.; Stokes, M.; Taylor, M. Assessing changes in subjective and objective function from pre- to post-knee arthroplasty using the Cardiff Dempster–Shafer theory classifier. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Whittle, M.W. Gait Analysis; Butterworth-Heinemann: London, UK, 1991; pp. 130–173. [Google Scholar]
- Kirtley, C. Clinical Gait Analysis; Elsevier Health Sciences: Philadelphia, PA, USA, 2006; pp. 5–14. [Google Scholar]
- Crabtree, C.A.; Higginson, J.S. Modeling neuromuscular effects of ankle foot orthoses (AFOs) in computer simulations of gait. Gait Posture 2009, 29, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.O.; Kang, H.S.; Kim, J.H.; Min, B.G. Virtual anatomy and movement of lower extremities using virtual reality modeling language. J. Digit. Imaging 2000, 13, 238–240. [Google Scholar] [CrossRef]
- Lapham, A.C.; Bartlett, R.M. The use of artificial intelligence in the analysis of sports performance: A review of applications in human gait analysis and future directions for sports biomechanics. J. Sports Sci. 1995, 13, 229–237. [Google Scholar] [CrossRef]
- Figueiredo, J.; Santos, C.P.; Moreno, J.C. Automatic recognition of gait patterns in human motor disorders using machine learning: A review. Med. Eng. Phys. 2018, 53, 1–12. [Google Scholar] [CrossRef]
- Caldas, R.; Mundt, M.; Potthast, W.; Fernando, B.D.L.N.; Markert, B. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef]
- Nolan, H.; Evi, V.; Ann, H.; Luc, V.; Vincent, V.R.; Wim, S. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar]
- Bae, S.; Armstrong, T.J. A finger motion model for reach and grasp. Int. J Ind. Erg. 2011, 41, 79–89. [Google Scholar] [CrossRef]
- Stimpson, K.H.; Heitkamp, L.N.; Horne, J.S.; Dean, J.C. Effects of walking speed on the step-by-step control of step width. J. Biomech. 2017, 68, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.J.; Wang, M.J.J. The change of gait parameters during walking at different percentage of preferred walking speed for healthy adults aged 20–60 years. Gait Posture 2010, 31, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Mutoh, T.; Mutoh, T.; Tsubone, H.; Takada, M.; Doumura, M.; Ihara, M.; Shimomura, H.; Taki, Y.; Ihara, M. Impact of serial gait analyses on long-term outcome of hippotherapy in children and adolescents with cerebral palsy. Complement. Clin. Pract. 2018, 30, 19–23. [Google Scholar] [CrossRef]
- Debi, R.; Elbaz, A.; Mor, A.; Kahn, G.; Peskin, B.; Beer, Y.; Agar, G.; Morag, G.; Segal, G. Knee osteoarthritis, degenerative meniscal lesion and osteonecrosis of the knee: Can a simple gait test direct us to a better clinical diagnosis. Orthop. Traumatol. Surg. Res. 2017, 103, 603–608. [Google Scholar] [CrossRef]
- Honda, K.; Sekiguchi, Y.; Muraki, T.; Izumi, S.I. The differences in sagittal plane whole-body angular momentum during gait between patients with hemiparesis and healthy people. J. Biomech. 2019, 86, 204–209. [Google Scholar] [CrossRef]
- Wren, T.A.L.; Gorton, G.E., III; Õunpuu, S.; Tucker, C.A. Efficacy of clinical gait analysis: A systematic review. Gait Posture 2011, 34, 149–153. [Google Scholar] [CrossRef]
- Papageorgiou, E.; Nieuwenhuys, A.; Vandekerckhove, I.; Van Campenhout, A.; Ortibus, E.; Desloovere, K. Systematic review on gait classifications in children with cerebral palsy: An update. Gait Posture 2019, 69, 209–223. [Google Scholar] [CrossRef]
- Elbaz, A.; Mor, A.; Segal, G.; Bar, D.; Monda, M.K.; Kish, B.; Nyska, M.; Palmanovich, E. Lower extremity kinematic profile of gait of patients after ankle fracture: A case-control study. J. Foot Ankle. Surg. 2016, 55, 918–921. [Google Scholar] [CrossRef]
- Siasios, I.D.; Spanos, S.L.; Kanellopoulos, A.K.; Fotiadou, A.; Pollina, J.; Schneider, D.; Becker, A.; Dimopoulos, V.G.; Fountas, K.N. The role of gait analysis in the evaluation of patients with cervical myelopathy: A literature review study. World Neurosurg. 2017, 101, 275–282. [Google Scholar] [CrossRef]
- Rucco, R.; Agosti, V.; Jacini, F.; Sorrentino, P.; Varriale, P.; Stefano, M.D.; Milan, G.; Montella, P.; Sorrentino, G. Spatio-temporal and kinematic gait analysis in patients with Frontotemporal dementia and Alzheimer’s disease through 3D motion capture. Gait Posture 2017, 52, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Goffredo, M.; Iacovelli, C.; Russo, E.F.; Pournajaf, S.; Blasi, C.D.; Galafate, D.; Pellicciari, L.; Agosti, M.; Filoni, S.; Aprile, I.; et al. Stroke Gait Rehabilitation: A Comparison of End-Effector, Overground Exoskeleton, and Conventional Gait Training. Appl. Sci. 2019, 9, 2627. [Google Scholar] [CrossRef]
- Cimolin, V.; Galli, M. Summary measures for clinical gait analysis: A literature review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Huang, S.; Xu, Y.; Li, J.; Yu, L. The Movement Model of the Knee Joint during Human Walking. In Proceedings of the IEEE International Conference on Intelligent Human-machine Systems & Cybernetics, Hangzhou, China, 26–27 August 2013. [Google Scholar]
- Prautzsch, H.; Boehm, W.; Paluszny, M. Bézier and B-Spline Techniques; Springer Science & Business Media: New York, NY, USA, 2002; pp. 9–22. [Google Scholar]
- Piegl, L.; Tiller, W. The NURBS Book, 2nd ed.; Springer: New York, NY, USA, 1997; pp. 7–101. [Google Scholar]
- Shen, W.; Chai, C.K. Research on motion optimization for quadruped robot based on swing-leg retraction. Trans. Beijing Inst. Technol. 2018, 38, 1269–1275. (In Chinese) [Google Scholar]
- Sun, X.R.; Zang, X.Z.; Liu, Y.X.; Lin, Z.K. Dynamic analysis and gait planning of biped robot with underactuated ankle. J. Harbin Univ. Commer. (Nat. Sci.) 2017, 33, 319–323. (In Chinese) [Google Scholar]
- Guo, Q.W.; Xiong, J.; Zhu, G.Q. Extensions of C-Bézier curves and surfaces. Comput. Eng. Appl. 2009, 45, 170–173. [Google Scholar]
- Han, X.A.; Huang, X.L.; Ma, Y.C. Shape analysis of cubic trigonometric Bézier curves with a shape parameter. Appl. Math. Comput. 2010, 217, 2527–2533. [Google Scholar] [CrossRef]
- Qin, X.Q.; Hu, G.; Yang, Y.; Wei, G. Construction of PH splines based on H-Bézier curves. Appl. Math. Comput. 2014, 238, 460–467. [Google Scholar] [CrossRef]
- Liu, Z.; Chen, X.Y.; Jiang, P. A class of generalized Bézier curves and surfaces with multiple shape parameters. J. Comput.-Aided Des. Comput. Graph. 2010, 22, 838–844. [Google Scholar] [CrossRef]
- Yang, L.Q.; Zeng, X.M. Bézier curves and surfaces with shape parameter. Int. J. Comput. Math. 2009, 86, 1253–1263. [Google Scholar] [CrossRef]
- Ri, K. Bézier curves with multi-shape-parameters. J. Zj. Univ. (Sci. Ed.) 2010, 37, 401–405. [Google Scholar]
- Hu, G. Research on the Theory and Applications of the Generalized Bézier Curves and Surfaces with Shape Parameters. Ph.D. Thesis, Xi’an University of Technology, Xi’an, China, 2016. [Google Scholar]
- Qin, X.Q.; Hu, G.; Zhang, N.J.; Shen, X.L.; Yang, Y. A novel extension to the polynomial basis functions describing Bezier curves and surfaces of degree n with multiple shape parameters. Appl. Math. Comput. 2013, 223, 1–16. [Google Scholar] [CrossRef]
- Liu, F.; Ji, X.M.; Gong, L.Q. A CAD modeling method for car form design based on CE-Bézier. In Proceedings of the 11th International Conferences on Computer Graphics, Visualization, Computer Vision and Image Processing (IADIS: 2017), Lisbon, Portugal, 21 July 2017. [Google Scholar]
- Guo, L.; Ji, X.M.; Hu, G.; Chu, J.J. Car headlight shape design based on cubic Q-Bézier curves. China Mech. Eng. 2013, 24, 1961–1969. (In Chinese) [Google Scholar]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Cui, Y.H.; Ji, X.M.; Wang, X.P. A method of measuring and analyzing the regularity of human gait. In Proceedings of the International Conference on Mathematics, Modelling, Simulation and Algorithms (MMSA 2018), Chengdu, China, 25–26 March 2018. [Google Scholar]
- Protopapadaki, A.; Drechsler, W.I.; Cramp, M.C.; Coutts, F.J.; Scott, O.M. Hip, knee, ankle kinematics and kinetics during stair ascent and descent in healthy young individuals. Clin. Biomech. 2007, 22, 203–210. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Joints | Number of Commonality Points | Number of Shape Parameters | Goodness of Fit |
|---|---|---|---|
| Hip | 4 | 2 | 0.69 |
| 5 | 3 | 1 | |
| 6 | 4 | 1 | |
| Knee | 4 | 2 | 0.71 |
| 5 | 3 | 0.91 | |
| 6 | 4 | 0.99 | |
| Ankle | 7 | 5 | 0.93 |
| 8 | 6 | 0.99 | |
| 9 | 7 | 1 |
| Coordinates of Commonality Points | ||||||||
|---|---|---|---|---|---|---|---|---|
| Hip | 0.00,30.00 | 15.30,32.62 | 63.79,−64.87 | 73.30,37.28 | 100.00,27.83 | |||
| Knee | 0.00,4.99 | 19.31,27.70 | 57.28,−47.12 | 69.36,90.93 | 100.00,3.53 | |||
| Ankle | 0.00,−5.35 | 8.26,−17.37 | 17.36,1.62 | 35.83,−3.41 | 54.83,17.49 | 67.63,−43.10 | 81.35,9.04 | 100.00,−4.65 |
| Shape Parameters of Normal Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hip | Knee | Ankle | ||||||||||
| 1 | −2.20 | 0.67 | −2.18 | −0.55 | 0.78 | −1.24 | −0.97 a | −12.37 | −5.62 | −4.62 | −6.67 | −2.77 |
| 2 | −1.94 | 0.72 | −1.13 | −2.90 b | 0.91 | −1.75 | −4.57 | −13.80 b | 6.50 a | −17.75 b | −3.82 a | −5.72 b |
| 3 | −1.24 | 1.81 a | −2.41 b | −2.77 | 1.32 | −2.26 | −2.27 | −11.92 | −16.50 | −1.37 | −8.02 | −0.05 a |
| 4 | −2.66 b | 0.42 b | −0.54 a | −1.96 | 0.61 b | −1.77 | −5.12 | 5.58 a | −19.75 b | −2.50 | −11.92 b | −2.92 |
| 5 | 0.04 a | 1.32 | −0.73 | 0.68 a | 1.23 a | −1.13 a | −4.15 | −5.10 | −6.62 | −13.00 | −8.55 | −4.60 |
| 6 | −2.18 | 1.70 | −2.26 | −1.84 | 0.66 | −2.10 | −3.47 | −1.57 | −19.37 | −0.12 a | −4.50 | −3.12 |
| 7 | −2.33 | 1.14 | −2.18 | −1.98 | 0.92 | −1.96 | −2.02 | −6.75 | −12.62 | −5.62 | −10.57 | −3.02 |
| 8 | −1.84 | 0.73 | −2.11 | −1.67 | 0.93 | −2.11 | −3.65 | −11.47 | −9.87 | −12.25 | −7.27 | −4.92 |
| 9 | −2.38 | 0.61 | −2.04 | −2.38 | 0.99 | −2.20 b | −2.92 | −11.10 | −2.37 | −15.12 | −9.82 | −2.85 |
| 10 | −2.03 | 0.92 | −2.12 | −1.96 | 1.14 | −1.80 | −5.67 b | −10.65 | −7.37 | −11.50 | −9.45 | −4.45 |
| Avg. | −1.88 | 1.01 | −1.77 | −1.73 | 0.95 | −1.83 | −3.48 | −7.89 | −9.36 | −8.38 | −8.06 | −3.44 |
| Shape Parameters of the Patient Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hip | Knee | Ankle | ||||||||||
| A | −2.26 | 0.02 * | −2.77 * | −2.80 | 1.08 | −2.96 * | −6.00 * | −13.20 | 1.12 | −17.00 | −15.00 * | −5.87 * |
| B | −2.33 | 0.10 * | −2.84 * | −2.38 | 1.04 | −2.87 * | −6.00 * | −14.32 * | 5.62 | −15.25 | −15.00 * | −5.40 |
| C | −0.44 | 0.23 * | −2.38 | −2.33 | 0.92 | −2.70 * | −4.70 | −9.90 | −16.87 | −5.62 | −13.80 * | −3.47 |
| D | −2.10 | 0.30 * | −2.90 * | −2.56 | 0.42 * | −1.15 | −0.07 * | −14.85 * | −15.12 | 0.25 * | −11.77 | −3.62 |
| E | −1.24 | 0.61 | −0.44 * | −2.11 | 0.50 * | −2.16 | 0.07 * | −12.07 | −4.62 | −14.12 | −6.60 | −5.60 |
| F | −2.33 | 1.14 | −1.47 | −0.87 | 0.46 * | −1.50 | −3.70 | −8.55 | −18.62 | −4.62 | −5.92 | −5.97 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, J.; Cui, Y.; Ji, X.; Wang, X.; Hu, G.; Liu, F. A Parametric Identification Method of Human Gait Differences and its Application in Rehabilitation. Appl. Sci. 2019, 9, 4581. https://doi.org/10.3390/app9214581
Gao J, Cui Y, Ji X, Wang X, Hu G, Liu F. A Parametric Identification Method of Human Gait Differences and its Application in Rehabilitation. Applied Sciences. 2019; 9(21):4581. https://doi.org/10.3390/app9214581
Chicago/Turabian StyleGao, Jing, Yahui Cui, Xiaomin Ji, Xupeng Wang, Gang Hu, and Fan Liu. 2019. "A Parametric Identification Method of Human Gait Differences and its Application in Rehabilitation" Applied Sciences 9, no. 21: 4581. https://doi.org/10.3390/app9214581
APA StyleGao, J., Cui, Y., Ji, X., Wang, X., Hu, G., & Liu, F. (2019). A Parametric Identification Method of Human Gait Differences and its Application in Rehabilitation. Applied Sciences, 9(21), 4581. https://doi.org/10.3390/app9214581