1. Introduction
In recent years, particulate matter (PM) has emerged as a big problem in Korea. According to the Organization for Economic Cooperation and Development (OECD)’s annual report on the concentration of ultra-particulate matter in countries by 2017, the mean population was exposed to PM
2.5 and with pollution at 25.1 μg/m
3, Korea was the second worst of the member countries [
1], with a level twice as high as the average OECD member countries (12.5 μg/m
3) and 2.5 times higher than the World Health Organization (WHO)’s annual average recommended concentration (10 μg/m
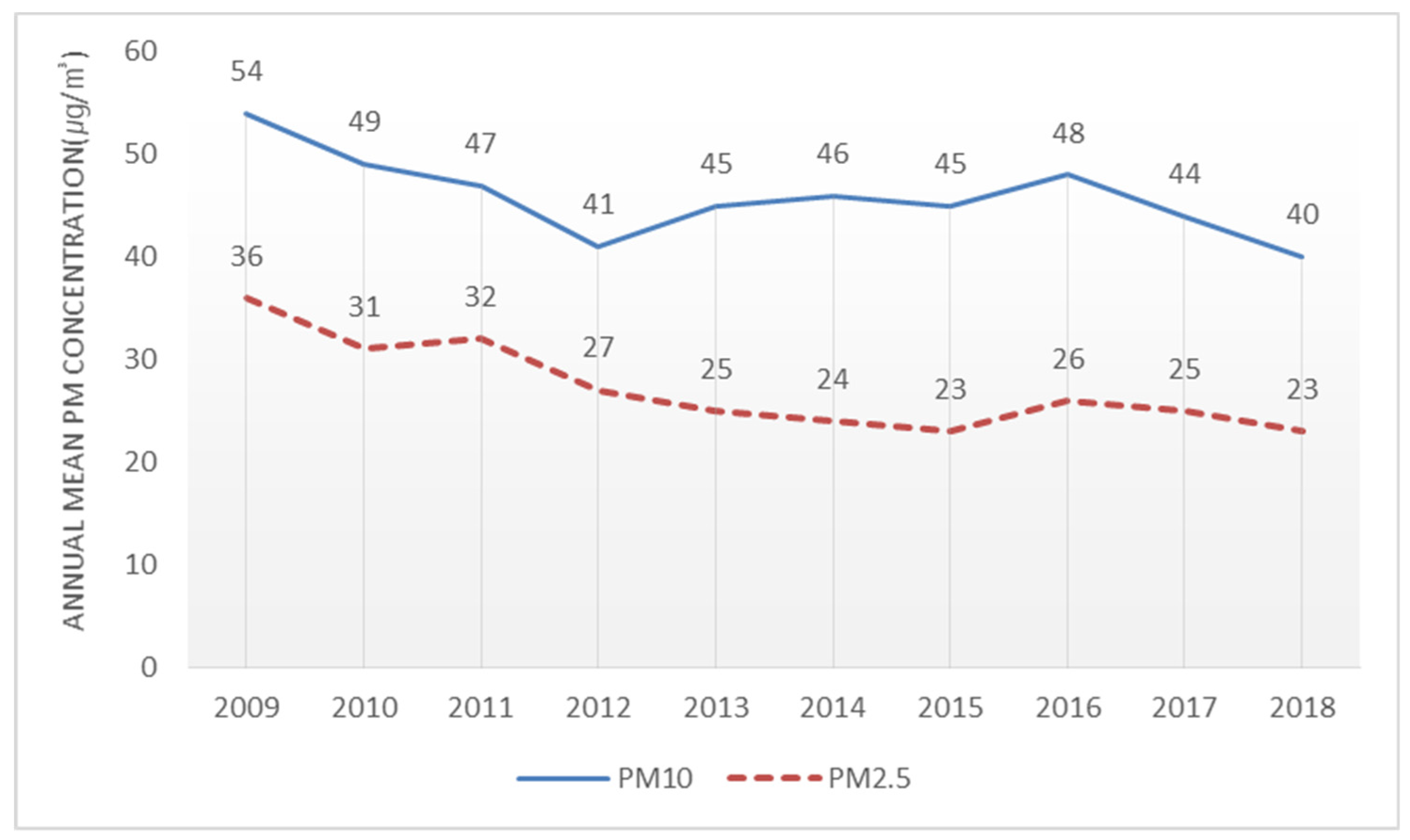
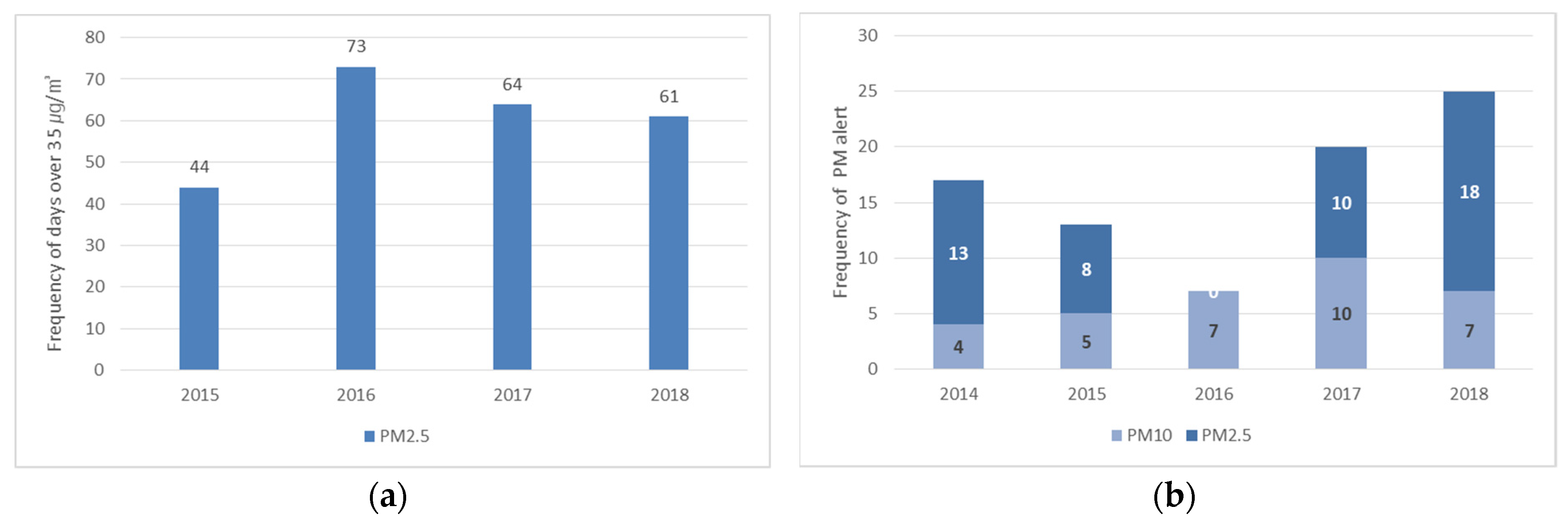
3). Based on Korea’s PM forecast, the number of “bad” (36–75 μg/m
3) and “very bad” (more than 76 μg/m
3) days in metropolitan areas increased from 62 in 2015 to 77 in 2018 [
2]. In early March 2019, Korea experienced the most severe PM situation. In Seoul, an 8-day ultra-particulate matter warning (PM
2.5 with a time-averaged concentration of more than 75 μg/m
3 for 2 h) and 2 days (March 5 and 6) with an alert level (an average PM
2.5 of more than 150 μg/m
3 for 2 h) [
3]. As a result, the PM levels became hazardous to health.
PM is a WHO Level 1 carcinogen that has negative effects on health, contributing to cardiovascular and respiratory diseases [
4,
5]. Choe and Lee [
6] investigated the effect of particulate emissions on specific diseases in Seoul and found that the number of hospitalizations for various respiratory diseases increased as the amount of ultra-PM increased. Korea’s increase in PM is related to rapid economic growth. Large cities, such as Seoul, have high levels of energy use resulting from the concentration of population and economic activity and their direct emission of air pollutants is high. Further, since its geographical location is on the mid-latitude westerly wind area, seasonal influx of PM from neighboring China also affects the increase of PM in Korea [
7].
According to the survey data on the perception of environmental problems among Koreans aged 13 and over, conducted by the Korea National Statistical Office (KNSO), 82.5% of respondents experience anxiety about PM [
8]. Kim et al. [
9] observed that Koreans regard PM as the most serious social risk factor. Because national concern about PM has been increasing, the government introduced a comprehensive plan for PM in 2017. In 2018, it attempted to reduce PM emissions by enforcing a Special Act on Particulate Matter in major cities across the country, including the capital region [
10]. The Ministry of Environment, in consideration of atmospheric environmental standards and health effects, produced a PM forecasting system, which presents the levels of PM as well as countermeasures [
11]. However, despite the various risk indicators for PM and notwithstanding the government measures, the residents of Seoul are notably passive in protecting individuals and society from PM despite viewing it as a threat [
12]. To prevent and reduce the PM generated by anthropogenic rather than natural factors, public efforts must be accompanied by measures at the national level. Without ensuring that residents understand PM, it is predicted that reduction measures will be ineffective. Therefore, this study aims to identify levels of awareness of PM, recognition of indoor air quality, symptoms of PM exposure experienced by residents and coping behavior in relation to PM in Seoul. Specific research questions are as follows:
First, how do residents perceive the indoor air quality, how do they feel PM symptoms and how do they behave in response to PM?
Second, do the different characteristics of residents produce any variations in behavior in response to PM?
Third, what are the impediments to the proper responses to PM by residents?
In this study, we have sought to understand the perceptions of PM and the subsequent response behaviors of residents, as well as to identify the causes of these behaviors. It is critical to understand and solve the barriers to public engagement to avoid the worst consequences of PM. The results of this study are expected to be used as basic data for effective governmental measures to reduce PM.
3. Materials and Methods
3.1. Participants and Questionnaire Design
This study surveyed the residents of Seoul. To identify differences in the response to PM associated with gender and age, respondents were divided into three groups. A total of 171 respondents were used for the analysis. The groups were 20-year-old college students (N = 70, gender = 32 male and 38 female, mean age = 21.88, SD = 2.33), 30- to 40-year-old male workers (N = 51, mean age = 41.11, SD = 5.45) and 30- to 40-year-old housewives (N = 50, mean age = 37.06, SD = 4.33). The questionnaire comprised five main parts. The first part included questions about the quality of indoor air perceived by residents in the home. The second part addressed the health of the residents in terms of objective symptoms, subjective symptoms and health behaviors concerning the symptoms. The third section elicited the residents’ responses to PM, dividing them into mitigating behavior, adaptive behavior and behavior intentions. The fourth part sought to ascertain the psychological causes of interference with the response behaviors of the residents to PM and the final content consisted of questions investigating the residents’ overall knowledge of PM.
3.2. Measures
3.2.1. Measuring Response Behaviors to Particulate Matter
Mitigating behavior and adaptive behavior are countermeasures to deal with risk. Swart and Raes [
15] define “mitigation” as an anthropogenic intervention to reduce the sources of air pollution, whereas “adaptation” is an adjustment in natural or human systems in response to climatic stimuli. Mitigation is a way to reduce the cause of hazards associated with PM. Usually, the benefits of mitigating behavior are not seen in the short term, so it is considered a long-term countermeasure [
16]. Mitigating behavior is a personal effort to reduce the generation of PM, which includes “using public transportation to reduce atmospheric gas generation”, “not using electricity and heating to restrain unnecessary energy use”, “using kitchen utensils that generate less harmful gas” and other similar measures. Adaptation refers to controlling the damage caused by PM.
Adaptive behavior can reduce the risks associated with PM by prophylactic and post-exposure measures that minimize the negative effects of PM [
17]. In contrast to mitigating behavior, from which long-term effects arise, the effects of adaptive behavior are immediate and are characterized by the matching of subject and beneficiary [
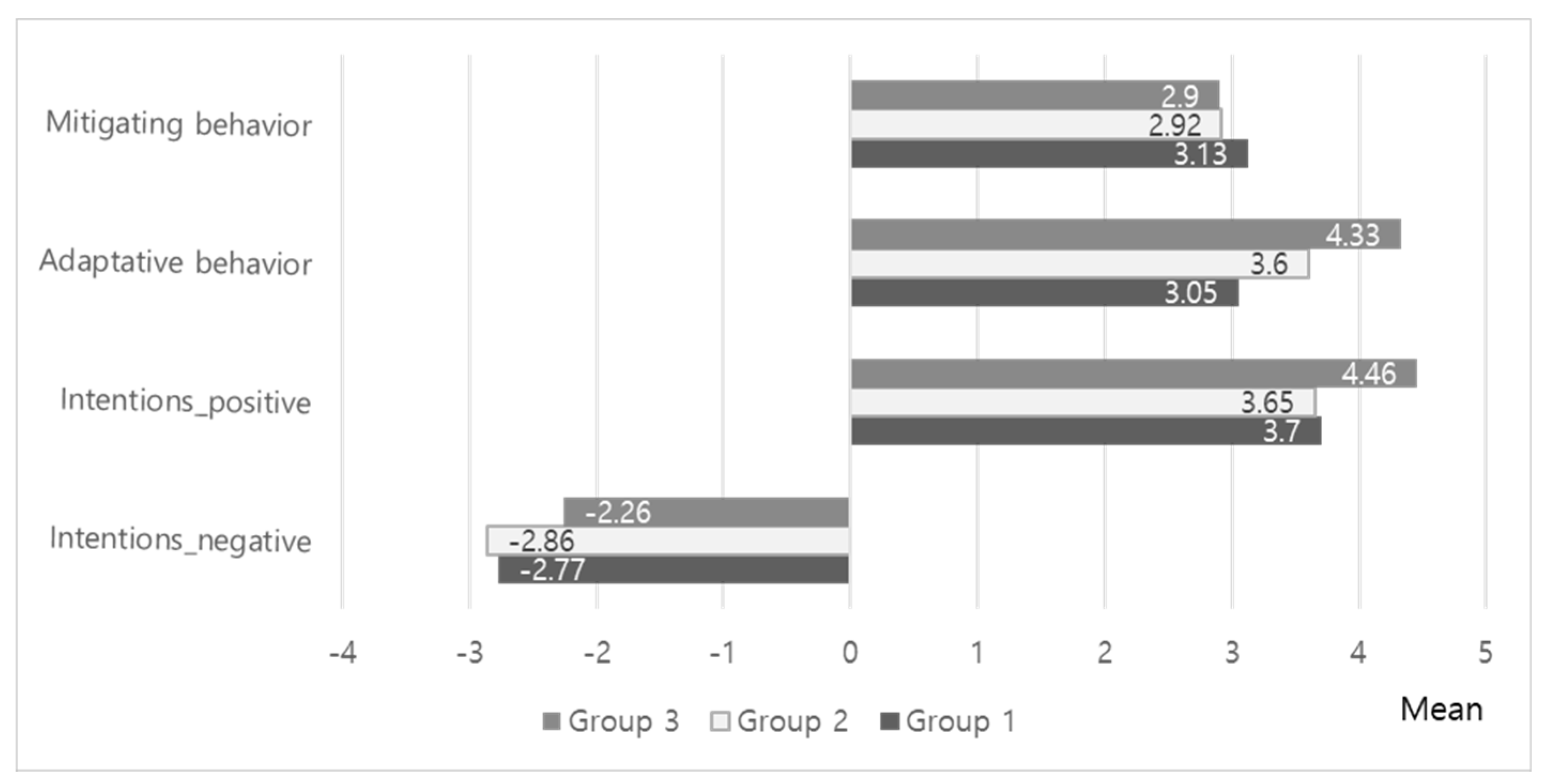
18]. Adaptive behavior is action to prevent the damage caused to individuals by high concentrations of dust. Behavioral intentions signify an individual’s specific willingness to act in response to PM and include two positive intentions. To achieve sustainable development policies, it is necessary to integrate mitigating actions that directly reduce the concentration of PM and adaptive prevention actions that reduce the impact of the existing dust risk. In this study, mitigating behavior, adaptive behavior and the behavioral intentions of Seoul residents are explored, as shown in
Table 4.
3.2.2. Measuring Psychological Attributes that Hinder Reactions to Particulate Matter
Gilfford [
19] observed that most people find environmental sustainability to be an important issue but that psychological barriers prevent them from engaging in sufficient actions to address it. These psychological barriers impede the behavioral choices that would facilitate mitigation, adaptation and environmental sustainability [
20]. Risk perception is a factor that affects human attitudes and behavioral intentions and that is very important in making individual decisions about a behavior [
21]. Brewer et al. [
22] explained three dimensions of risk perception. The first is the likelihood that one will be harmed by the hazard; the second is susceptibility, referring to an individual’s constitutional vulnerability to a hazard; and the third is severity, indicating the extent of harm a hazard may cause. Psychological distance describes how individuals participate in future events [
23]. The perceived distance of events indicates how they are mentally construed. As the perceived distance increases, events are interpreted as more abstract, decontextualized and conceived in generalized terms. When events become closer, they use more specific, contextualized and detailed features [
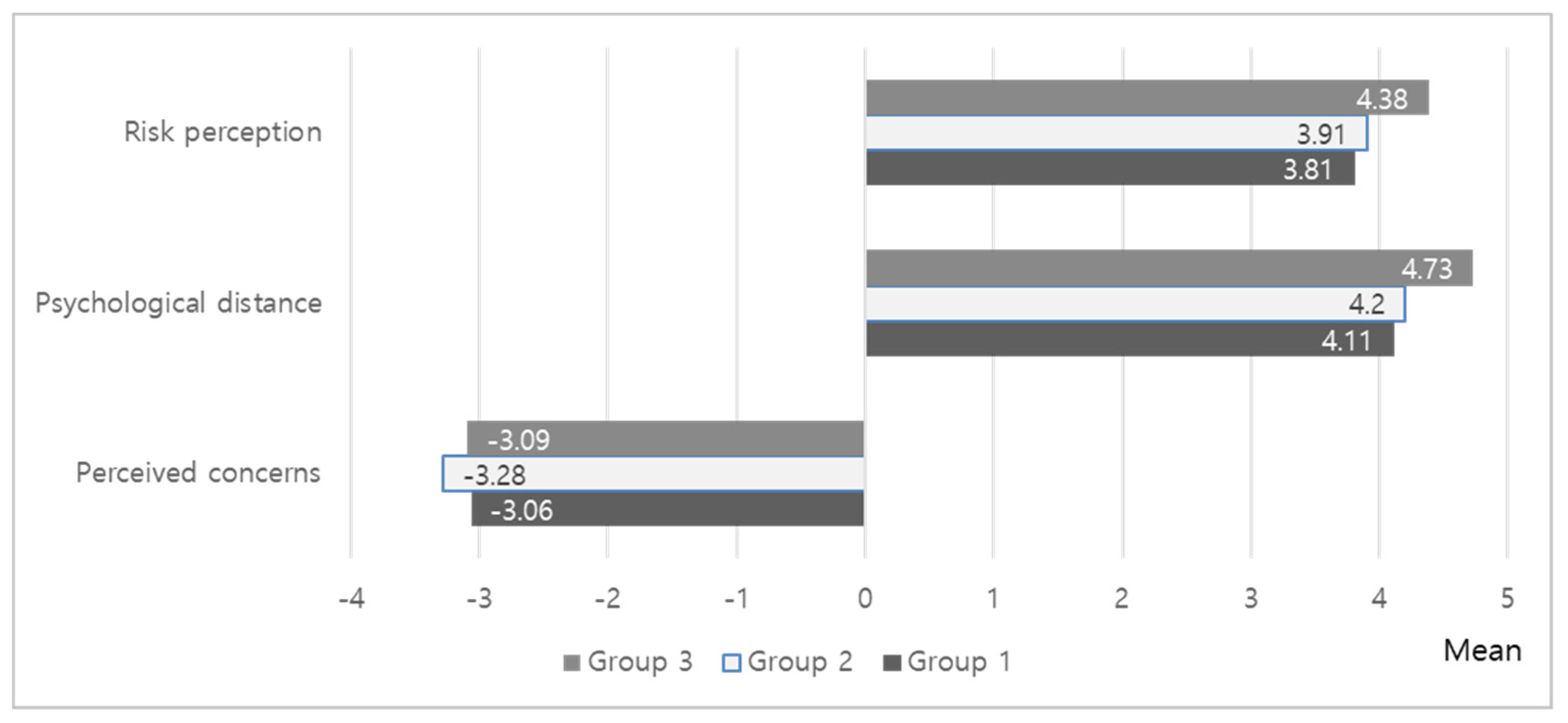
24]. The psychological distance for PM was evaluated using the four distance domains of geography, temporality, socialization and awareness. In addition, this research investigated various barriers increasing the perceived concern of the public, such as information distrust, externalizing responsibility and uncertainty about the causes of PM pollution. In this study, to understand the effects of response behaviors to PM, the psychological attributes of the residents were classified into nine concepts within three domains: “risk perception”, “psychological distance”, and “perceived concerns” (
Table 5).
3.3. Methodology
This research used a questionnaire to collect its data; the survey was conducted online in March 2019 and the data were analyzed using IBM’s SPSS Statistics Program 23. The question concerning residents’ perceptions of indoor air quality comprised positive and negative language (the semantic differential method). We distinguished between positive vocabulary and negative vocabulary over five levels, asking residents to assign one level to each question according to their perceptions. The vocabulary used to measure the indoor air quality of residents included “bad”, “good”, “stuffy”, “refreshed”, “unpleasant”, and “comfortable”. A five-point Likert scale was used to assess the symptoms, behaviors and psychological responses of residents, ranging from “very unlikely” (1 point), to “unlikely” (2 points), to “average” (3 points), to likely (4 points), to “very likely” (5 points). Questions measuring residents’ knowledge of PM could be answered as “right” (○) or “wrong” (X) and the “right” answers were added to produce a score.
An ANOVA was used for the statistical analysis to determine whether there were differences in behavior as a response to PM, according to the characteristics of residents. Participants were divided into three groups based on their genders and ages: college students in their twenties, male workers in their thirties and forties and female housewives in their thirties and forties. In addition to the response behavior, we compared differences between the groups in terms of environmental exposures to PM, perceived symptoms and psychological attributes. Further, post-hoc tests were conducted to analyze variations between groups. Multiple regression analysis was conducted to identify the factors influencing response behavior.
5. Discussion and Conclusions
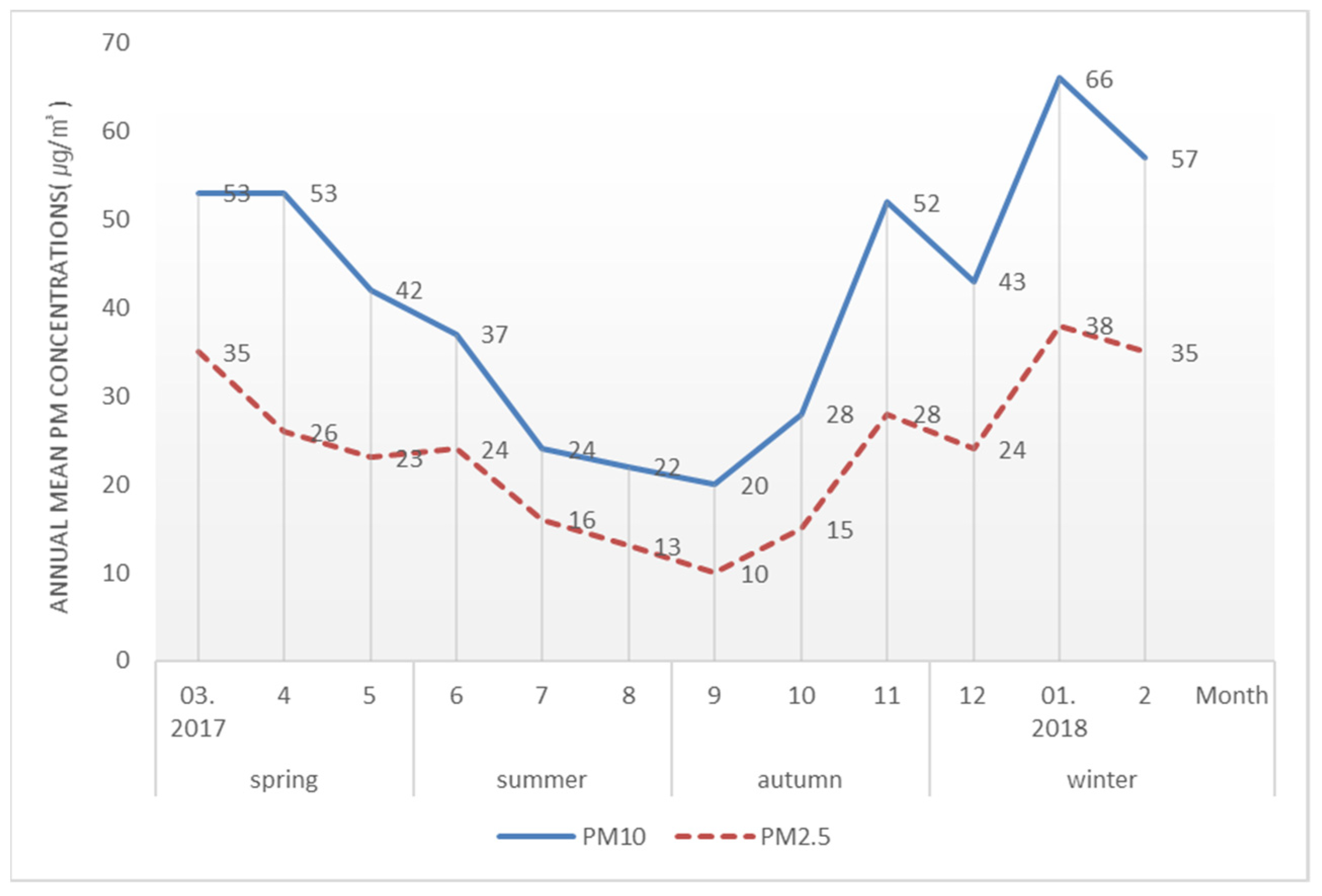
In Seoul, it is inadvisable to go out on any day, except in summer, as a result of the PM concentration and its effect on human health. When the WHO standard is applied, the concentration of PM in Seoul is revealed to be remarkably high and cases of excessive concentration exceeding the daily average atmospheric environment standard are also frequent. The government has been pursuing various policies to reduce PM concentration but the concentration of PM has not improved to the extent that people recognize any change. Research has shown that most people believe PM to be an important problem but do not undertake enough mitigating behaviors to prevent its occurrence. Reliable research should be preceded by an analysis of cause and effect before the preparation of PM countermeasures. We sought to understand residents’ perceptions of PM, their response behaviors and the psychological causes of these behaviors; the main findings of this study are as follows.
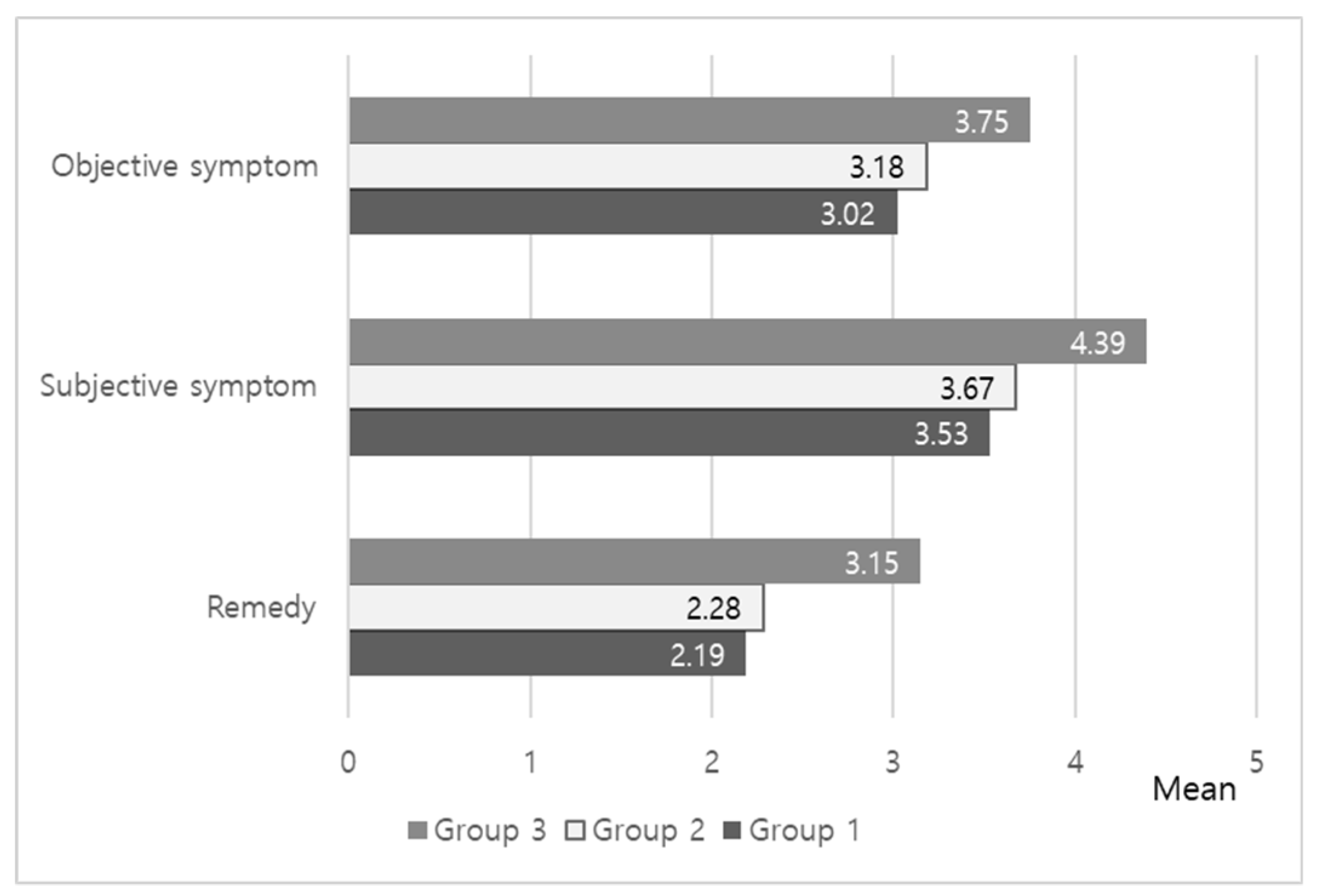
First, to identify the perceived indoor air quality of the residents, the questionnaire was distributed at a time when the concentration of PM had been significant throughout the year; thus, residents’ interest in indoor air quality was great. However, despite high outdoor concentrations of PM, the indoor air quality was not considered poor or dissatisfactory. The symptoms that residents attributed to PM were not physical, such as allergies or bronchitis. They more commonly experienced psychological stress or anxiety, feeling that PM had a negative effect on health and was interfering more frequently with daily life, in that residents were going out less often to avoid it.
Second, the problem with the PM-related behaviors of residents in Seoul was that many people did not take actual action despite their willingness to do so. Mitigating behavior to try to minimize PM generation was less common than adaptive behavior to protect individuals from the risks of PM. This may have been because of the nature of mitigating behavior, which often entails loss or inconvenience. Even if the risks associated with PM were largely recognized, it would be necessary to compensate for the loss when the habitual behavior of individuals was abandoned in favor of following the recommended behavior. Unlike preventive actions to protect individuals from PM, compensation for mitigating behavior is only likely to be achieved in the distant future and even then, such compensation would provide a social rather than an individual benefit. This suggests that more persuasive strategies should be employed to stimulate changes in individual behaviors for collective interests.
Third, the psychological characteristics of individuals can either hinder or promote action for environmental sustainability. The greater the perceived risk and the more psychological that risk, the more likely it is that an active response will occur. Analysis of the psychological factors affecting residents in Seoul revealed that they perceived the risk of PM to be very close (in terms of psychological distance). However, despite revealing significant levels of risk perception and psychological distance, the results of this study did not show active response behaviors. Attention must be paid to the externalizing of responsibility among the psychological causes of this lack of action. This study found distrust of and uncertainty about PM information to be largely unrecognized as causes of apathy; on the contrary, understanding PM saturation to be externally produced was the main reason for inaction. If external factors are emphasized as the cause of the problem, it is possible that individuals perceive the risk as uncontrollable, which may nullify their will to respond. The results of this study also suggest that residents’ psychological barriers have a negative effect on their response behaviors for the reduction of PM.
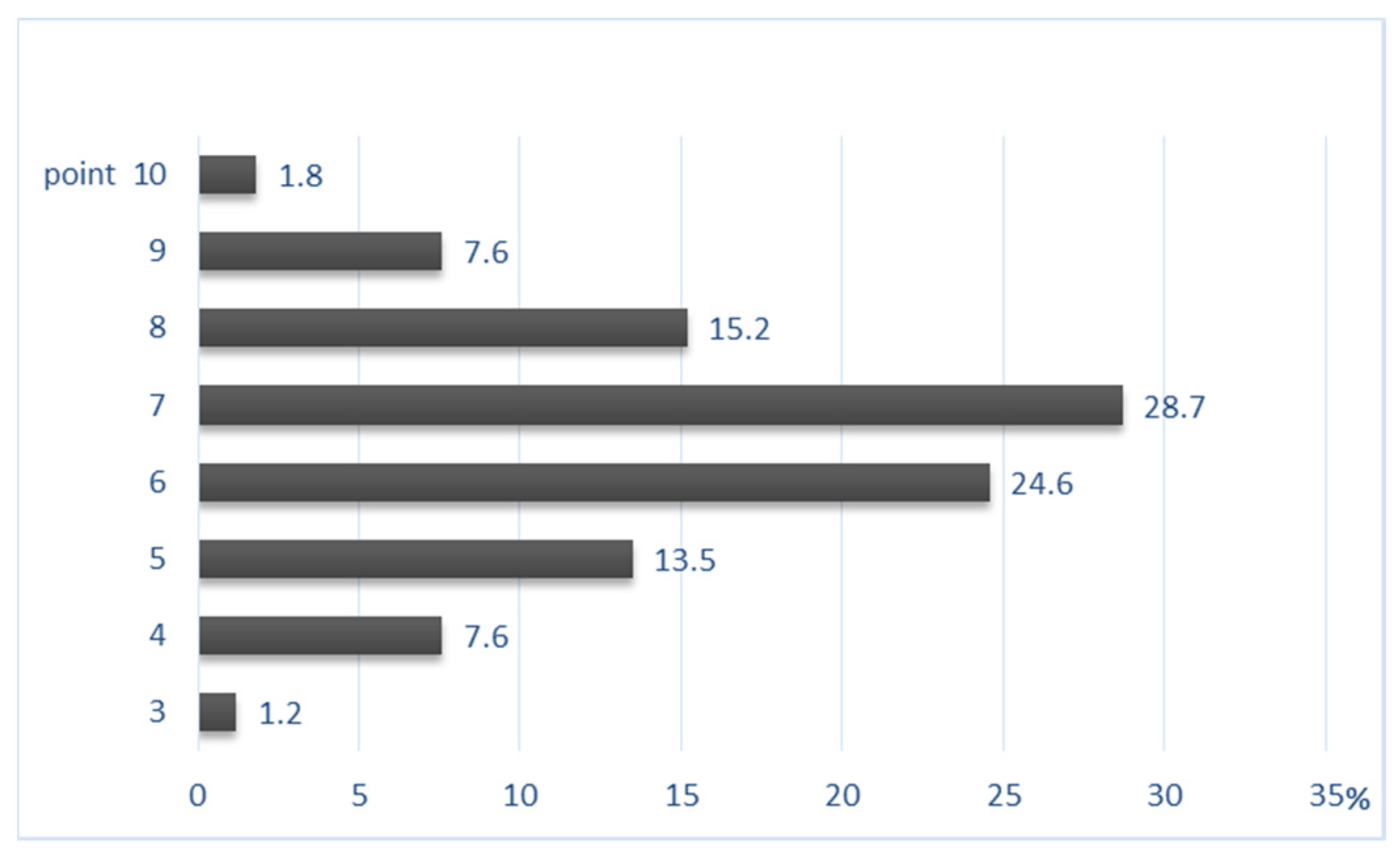
Fourth, the results of the correlation analysis show that the most influential factor in PM-related behavior was psychological attributes but that physical symptoms also affect response behaviors to PM. This result is meaningful in that it indicates desirable directions for PM policy. Based on the analysis of psychological factors, it was found that, because PM is also produced by individuals, active prevention is likely to occur if the importance of personal responses is conveyed. While knowledge of PM was not found to significantly affect response behaviors, residents in Seoul showed an average score of 6.56 out of 10 for PM knowledge. Lack of knowledge and understanding of the PM problem hinders appropriate response behavior. It is necessary to provide accurate and correct PM education and continuously available reliable information to enhance the knowledge of PM. In addition,
There was significant variation in residents’ perceptions, response behaviors and psychological attributes concerning PM based on gender and age. Conversely, the time during which residents undertook external activities exposed to PM did not significantly affect PM-related symptoms or behavior. In contrast to college students in their twenties and male workers in their thirties and forties who remained outdoors for 5 h on average, women in their thirties and forties who stayed outdoors for only 3 h on average responded more sensitively to PM-related symptoms and their commitment to PM reduction and mitigating actions was much greater. Similarly, the results of the psychological factor analysis for PM showed that the group of women in their thirties and forties were more aware of the risks than the other groups and felt those risks to be closer psychologically. However, it is the younger generations who will become the subjects of society in future and will need to face these problems and solve them. There is an urgent need for plans to increase awareness of the risks and the will of the public to act.
Government efforts to reduce PM have focused primarily on expensive communication campaigns. However, the results of this study suggest that the mere encouragement of attitudinal change is not effective; public engagement in terms of accurate PM knowledge, health education and the study of various personal characteristics and psychological causes is required.
This study identified residents’ thoughts, response behaviors and psychological factors relating to PM and showed that personal characteristics, cognition and emotions affect behavioral intentions. Unlike previous studies, the significance of this research is that it seeks to understand residents’ behaviors in a multidimensional way. Psychological factors are expected to be used effectively to motivate individuals to protect themselves from the risks of PM exposure. The residents of Seoul involved in this study were well aware of the risks of PM but felt that its generation and any possible solutions were external and therefore beyond their control. This situation is likely to prevent public action to protect individuals and the society. It is recommended that we shift our focus from risk and attention to participation and action. It is expected that a proper direction for efficient PM reduction can be established using these results.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}