Vocal Pitch Discrimination in Children with and without Vocal Fold Nodules

{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Children with Vocal Fold Nodules (CwVN)
2.3. Children with Typical Voices (CwTV)
2.4. Adults
2.5. Stimuli Development and Presentation
2.6. Experimental Design
2.6.1. Training
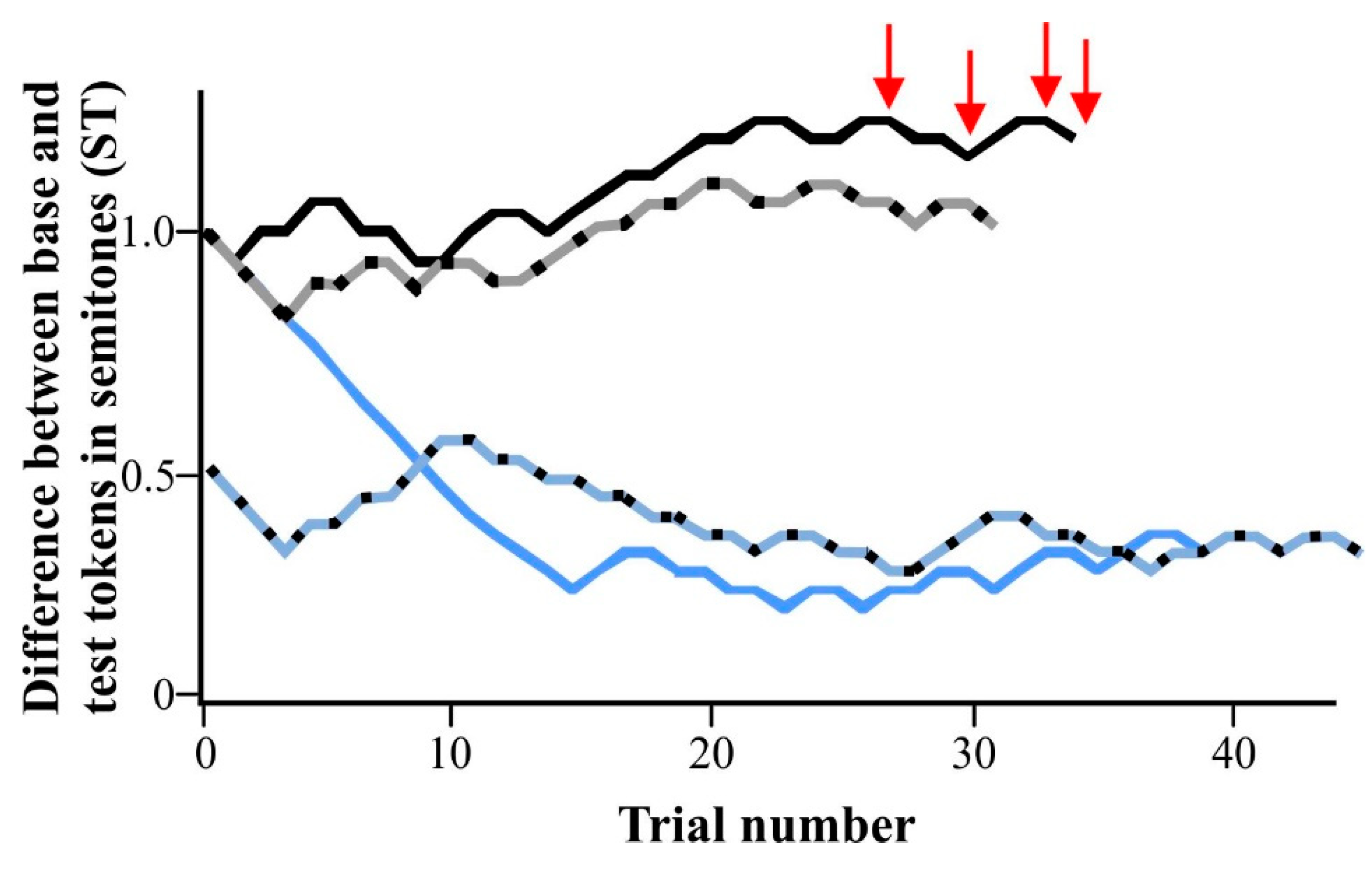
2.6.2. Experimental Paradigm
2.7. Data Analysis
2.7.1. Comparison between CwTV and CwVN Groups
2.7.2. Comparison among Younger CwTV, Older CwTV, and Adult Groups
3. Results
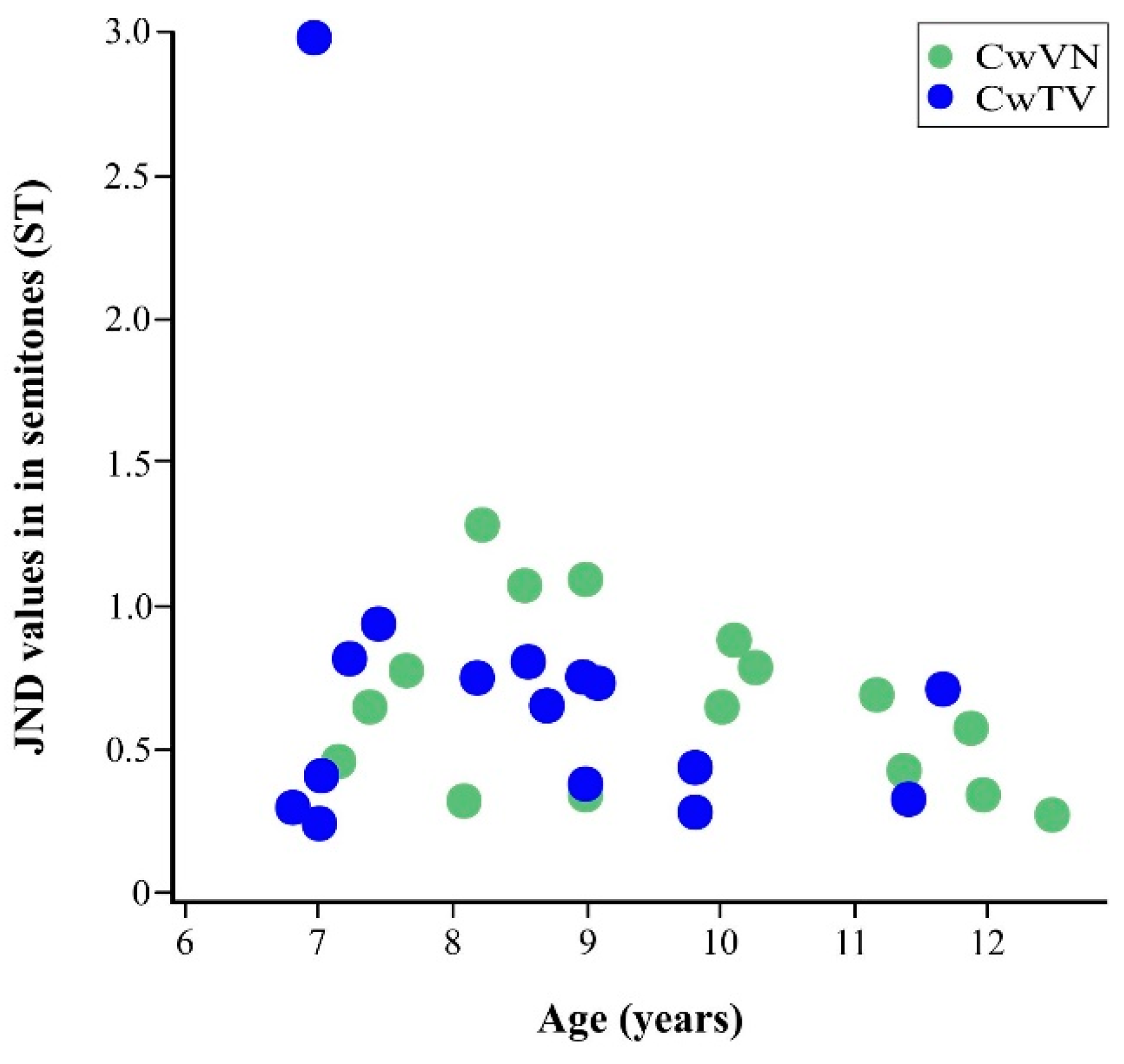
3.1. Comparison between CwTV and CwVN Groups
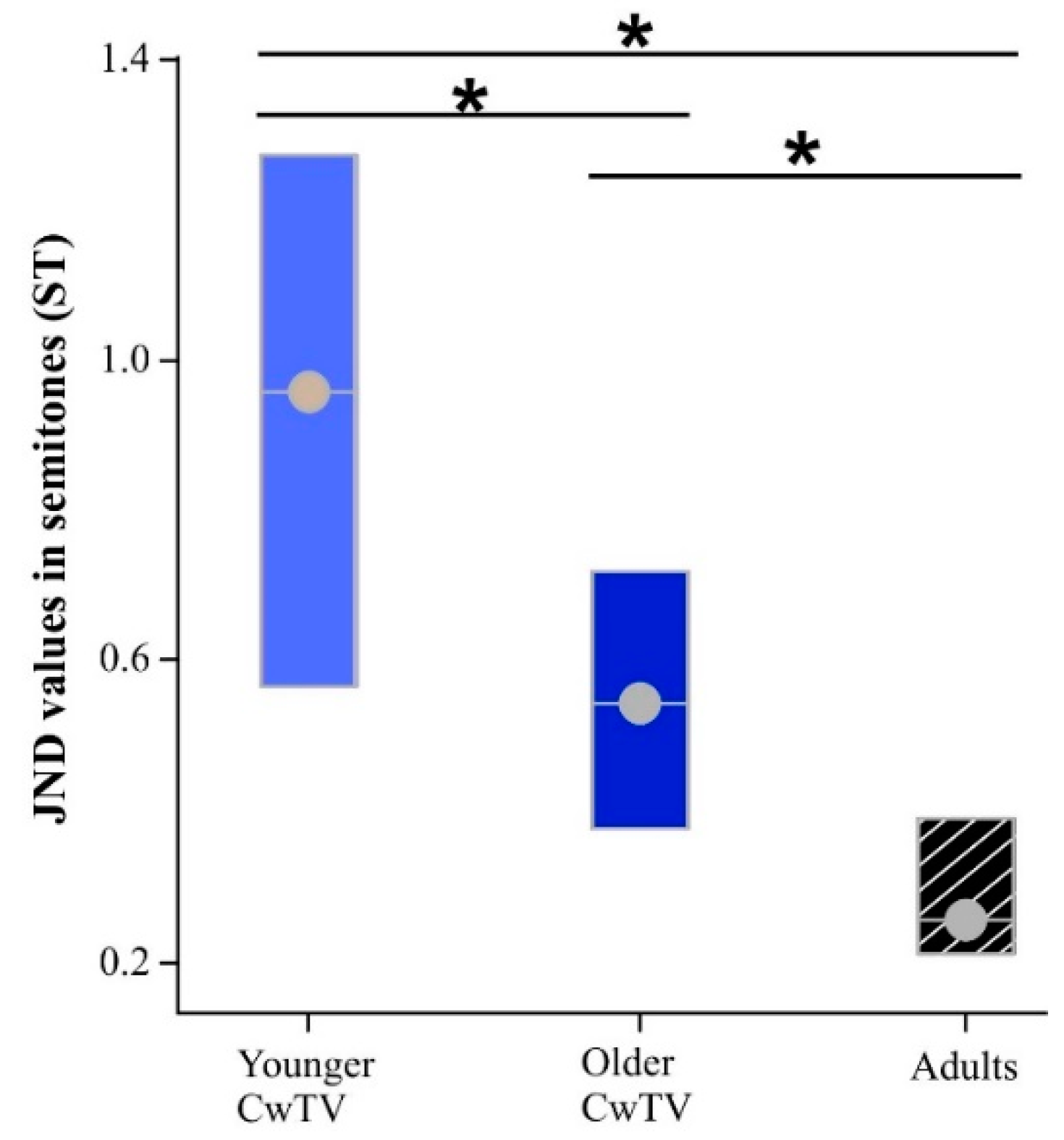
3.2. Comparison among Younger CwTV, Older CwTV, and Adult Groups
4. Discussion
4.1. Comparison between CwTV and CwVN Groups
4.2. Comparison among Younger CwTV, Older CwTV, and Adult Groups
4.3. Clinical Implications for Voice Therapy in CwVN
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Connor, N.P.; Cohen, S.B.; Theis, S.M.; Thibeault, S.L.; Heatley, D.G.; Bless, D.M. Attitudes of children with dysphonia. J. Voice 2008, 22, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Carroll, L.M.; Mudd, P.; Zur, K.B. Severity of voice handicap in children diagnosed with elevated lesions. Otolaryngol. Head Neck Surg. 2013, 149, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Verduyckt, I.; Remacle, M.; Jamart, J.; Benderitter, C.; Morsomme, D. Voice-related complaints in the pediatric population. J. Voice 2011, 25, 373–380. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.S. Benign lesions of the pediatric vocal folds: Nodules, webs, and cysts. In Clinical Management of Children’s Voice Disorders; Hartnick, C., Boseley, M., Eds.; Plural Publishing: San Diego, CA, USA, 2010; pp. 145–163. [Google Scholar]
- Shearer, W.M. Diagnosis and treatment of voice disorders in school children. J. Speech Hear. Disord. 1972, 37, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.K.; Harvey Woodnorth, G.; Glynn, A.; Nuss, R.C. Pediatric vocal nodules: Correlation with perceptual voice analysis. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Angelillo, I.F.; Di Costanzo, B.; Costa, G.; Barillari, M.; Barillari, U. Epidemiological study on vocal disorders in paediatric age. J. Prev. Med. Hyg. 2008, 49, 1–5. [Google Scholar]
- Leeper, H.A., Jr.; Leonard, J.E.; Iverson, R.L. Otorhinolaryngologic screening of children with vocal quality disturbances. Int. J. Pediatr. Otorhinolaryngol. 1980, 2, 123–131. [Google Scholar] [CrossRef]
- Miller, S.Q.; Madison, C.L. Public school voice clinics, part II: Diagnosis and recommendations—A 10-year review. Lang. Speech Hear. Serv. Sch. 1984, 15, 58–64. [Google Scholar] [CrossRef]
- Mortensen, M.; Schaberg, M.; Woo, P. Diagnostic contributions of videolaryngostroboscopy in the pediatric population. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 75–79. [Google Scholar] [CrossRef]
- Kiliç, M.A.; Okur, E.; Yildirim, I.; Güzelsoy, S. The prevalence of vocal fold nodules in school age children. Int. J. Pediatr. Otorhinolaryngol. 2004, 68, 409–412. [Google Scholar] [CrossRef]
- Watts, C.R. Behavioral voice therapy in school-age children with vocal fold nodules. EBP Briefs 2012, 6, 1–9. [Google Scholar]
- Verdolini Abbott, K. Some guiding principles in emerging models of voice therapy for children. Semin. Speech Lang. 2013, 34, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Verdolini Abbott, K.; Yee-Key Li, N.; Hersan, R.; Kessler, L. Voice therapy for children. In Clinical Management of Children’s Voice Disorders; Hartnick, C., Boseley, M., Eds.; Plural Publishing: San Diego, CA, USA, 2010; pp. 111–133. [Google Scholar]
- Woodnorth, G.H.; Nuss, R.C. Pediatric benign vocal fold lesions: A team approach. Perspect. Voice Dis. 2009, 19, 105–112. [Google Scholar] [CrossRef]
- Wilson, D.K. Voice Problems of Children; Williams & Wilkins: Philadelphia, PA, USA, 1987. [Google Scholar]
- Lee, E.-K.; Son, Y.-I. Muscle tension dysphonia in children: Voice characteristics and outcome of voice therapy. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Connelly, A.; Clement, W.; Kubba, H. Management of dysphonia in children. J. Laryngol. Otol. 2009, 123, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.S.; Pettit, J.M.; Sherblom, J.C. Management of vocal nodules: A regional survey of otolaryngologists and speech-language pathologists. J. Speech Lang. Hear. Res. 1991, 34, 229–235. [Google Scholar] [CrossRef]
- Signorelli, M.E.; Madill, C.J.; McCabe, P. The management of vocal fold nodules in children: A national survey of speech-language pathologists. Int. J. Speech Lang. Pathol. 2011, 13, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.J.; Pentz, A.L. Otolaryngologists’ opinions of voice therapy for vocal nodules in children. Lang. Speech Hear. Serv. Sch. 1987, 18, 172–178. [Google Scholar] [CrossRef]
- Ongkasuwan, J.; Friedman, E.M. Is voice therapy effective in the management of vocal fold nodules in children? Laryngoscope 2013, 123, 2930–2931. [Google Scholar] [CrossRef]
- Deal, R.E.; McClain, B.; Sudderth, J.F. Identification, evaluation, therapy, and follow-up for children with vocal nodules in a public school setting. J. Speech Hear. Disord. 1976, 41, 390–397. [Google Scholar] [CrossRef]
- Trani, M.; Ghidini, A.; Bergamini, G.; Presutti, L. Voice therapy in pediatric functional dysphonia: A prospective study. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Benninger, M.S. Levels of evidence in the voice literature. J. Voice 2011, 25, 653–656. [Google Scholar] [CrossRef] [PubMed]
- Benninger, M.S. Quality of the voice literature: What is there and what is missing. J. Voice 2011, 25, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; McGlashan, J. Surgical versus non-surgical interventions for vocal cord nodules. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Hartnick, C.; Ballif, C.; De Guzman, V.; Sataloff, R.; Campisi, P.; Kerschner, J.; Shembel, A.; Reda, D.; Shi, H.; Zacny, E.S. Indirect vs. direct voice therapy for children with vocal nodules: A randomized clinical trial. Arch. Otolaryngol. Head Neck Surg. 2018, 144, 156–163. [Google Scholar]
- Boseley, M.E.; Cunningham, M.J.; Volk, M.S.; Hartnick, C.J. Validation of the pediatric voice-related quality-of-life survey. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.L.; Summers, A.C. Voice Treatment for Children and Adolescents; United Nations Publications: New York, NY, USA, 2002. [Google Scholar]
- Eggers, K.; Luc, F.; van den Bergh, B.R. Factorial temperament structure in stuttering, voice-disordered, and typically developing children. J. Speech Lang. Hear. Res. 2009, 52, 1610–1622. [Google Scholar] [CrossRef]
- Andrews, M.L. Voice Therapy for Children: The Elementary School Years; Longman Publishing Group: Harlow, UK, 1986. [Google Scholar]
- Heng Tam, K.; Carding, P.; Madill, C.J. The relationship between voice quality and pitch discrimination ability in a population with features of mild vocal hyperfunction. In Proceedings of the 47th Annual Symposium Care of the Pofessional Voice, Philadelphia, PA, USA, 30 May–3 June 2018; Available online: https://voicefoundation.org/wp-content/uploads/2018/04/All-Abstracts_2018.pdf (accessed on 1 September 2018).
- Halliday, L.F.; Taylor, J.L.; Edmondson-Jones, A.M.; Moore, D.R. Frequency discrimination learning in children. J. Am. Acad. Audiol. 2008, 123, 4393–4402. [Google Scholar] [CrossRef]
- Moore, D.R.; Ferguson, M.A.; Halliday, L.F.; Riley, A. Frequency discrimination in children: Perception, learning and attention. Hear. Res. 2008, 238, 147–154. [Google Scholar] [CrossRef]
- Banai, K. Auditory frequency discrimination development depends on the assessment procedure. J. Basic Clin. Physiol. Pharmacol. 2008, 19, 209–222. [Google Scholar] [CrossRef]
- Thompson, N.C.; Cranford, J.L.; Hoyer, E. Brief-tone frequency discrimination by children. J. Speech Lang. Hear. Res. 1999, 42, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.K.; Neff, D.L. Development of basic auditory discrimination in preschool children. Psychol. Sci. 1993, 4, 104–107. [Google Scholar] [CrossRef]
- Maxon, A.B.; Hochberg, I. Development of psychoacoustic behavior: Sensitivity and discrimination. Ear. Hear. 1982, 3, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Buss, E.; Flaherty, M.M.; Leibold, L.J. Development of frequency discrimination at 250 Hz is similar for tone and/ba/stimuli. J. Acoust. Soc. Am. 2017, 142, EL150–EL154. [Google Scholar] [CrossRef] [PubMed]
- Deroche, M.L.; Zion, D.J.; Schurman, J.R.; Chatterjee, M. Sensitivity of school-aged children to pitch-related cues. J. Acoust. Soc. Am. 2012, 131, 2938–2947. [Google Scholar] [CrossRef] [PubMed]
- Cacace, A.T.; McFarland, D.J. Factors influencing tests of auditory processing: A perspective on current issues and relevant concerns. J. Am. Acad. Audiol. 2013, 24, 572–589. [Google Scholar]
- Andrews, M.L.; Madeira, S.S. The assessment of pitch discrimination ability in young children. J. Speech Hear. Disord. 1977, 42, 279–286. [Google Scholar] [CrossRef]
- Sutcliffe, P.; Bishop, D. Psychophysical design influences frequency discrimination performance in young children. J. Exp. Child. Psychol. 2005, 91, 249–270. [Google Scholar] [CrossRef]
- Green, G. Psycho-behavioral characteristics of children with vocal nodules: WPBIC ratings. J. Speech Hear. Disord. 1989, 54, 306–312. [Google Scholar] [CrossRef]
- D’Alatri, L.; Petrelli, L.; Calò, L.; Picciotti, P.M.; Marchese, M.R.; Bussu, F. Vocal fold nodules in school age children: Attention deficit hyperactivity disorder as a potential risk factor. J. Voice 2015, 29, 287–291. [Google Scholar] [CrossRef]
- Lee, J.M.; Roy, N.; Dietrich, M. Personality, psychological factors, and behavioral tendencies in children with vocal nodules: A systematic review. J. Voice 2018. [Google Scholar] [CrossRef] [PubMed]
- Roy, N.; Holt, K.I.; Redmond, S.; Muntz, H. Behavioral characteristics of children with vocal fold nodules. J. Voice 2007, 21, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Erdur, O.; Herguner, A.; Ozturk, K.; Kibar, E.; Elsurer, C.; Bozkurt, M.K.; Herguner, S. Attention deficit hyperactivity disorder symptoms in children with vocal fold nodules. Int. J. Pediatr. Otorhinolaryngol. 2016, 85, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Dobres, R.; Lee, L.; Stemple, J.C.; Kummer, A.W.; Kretschmer, L.W. Description of laryngeal pathologies in children evaluated by otolaryngologists. J. Speech Hear. Disord. 1990, 55, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Kempster, G.B.; Gerratt, B.R.; Abbott, K.V.; Barkmeier-Kraemer, J.; Hillman, R.E. Consensus auditory-perceptual evaluation of voice: Development of a standardized clinical protocol. Am. J. Speech. Lang. Pathol. 2009, 18, 124–132. [Google Scholar] [CrossRef]
- Boersma, P.; Weenink, D. [Computer program]. In Praat: Doing Phonetics by Computer; Phonetic Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Infusino, S.A.; Diercks, G.R.; Rogers, D.J.; Garcia, J.; Ojha, S.; Maurer, R.; Bunting, G.; Hartnick, C.J. Establishment of a normative cepstral pediatric acoustic database. Arch. Otolaryngol. Head Neck Surg. 2015, 141, 358–363. [Google Scholar] [CrossRef]
- Maturo, S.; Hill, C.; Bunting, G.; Ballif, C.; Maurer, R.; Hartnick, C. Establishment of a normative pediatric acoustic database. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 956–961. [Google Scholar] [CrossRef]
- Heller Murray, E.S.; Lupiani, A.A.; Kolin, K.R.; Segina, R.K.; Stepp, C.E. Pitch shifting with the commercially available eventide eclipse: Intended and unintended changes to the speech signal. J. Speech Lang. Hear. Res. 2019, 62, 2270–2279. [Google Scholar] [CrossRef]
- Macmillan, N.A.; Creelman, C.D. Adaptive Methods for Estimating Empirical Thresholds. In Detection Theory: A User’s Guide; Cambridge University Press: New York, NY, USA, 1991; pp. 183–208. [Google Scholar]
- Levitt, H. Transformed up-down methods in psychoacoustics. J. Am. Acad. Audiol. 1971, 49, 467–477. [Google Scholar] [CrossRef]
- Minitab Inc. Minitab Statistical Software; Minitab Inc.: State College, PA, USA, 2012. [Google Scholar]
- Nagy, A.; Elshafei, R.; Mahmoud, S. Correlating undiagnosed hearing impairment with hyperfunctional sysphonia. J. Voice 2019. [Google Scholar] [CrossRef]
- Baker, B.M.; Baker, C.D.; Le, H.T. Vocal quality, articulation and audiological characteristics of children and young adults with diagnosed allergies. Ann. Otol. Rhinol. Laryngol. 1982, 91, 277–280. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heller Murray, E.S.; Hseu, A.F.; Nuss, R.C.; Harvey Woodnorth, G.; Stepp, C.E. Vocal Pitch Discrimination in Children with and without Vocal Fold Nodules. Appl. Sci. 2019, 9, 3042. https://doi.org/10.3390/app9153042
Heller Murray ES, Hseu AF, Nuss RC, Harvey Woodnorth G, Stepp CE. Vocal Pitch Discrimination in Children with and without Vocal Fold Nodules. Applied Sciences. 2019; 9(15):3042. https://doi.org/10.3390/app9153042
Chicago/Turabian StyleHeller Murray, Elizabeth S., Anne F. Hseu, Roger C. Nuss, Geralyn Harvey Woodnorth, and Cara E. Stepp. 2019. "Vocal Pitch Discrimination in Children with and without Vocal Fold Nodules" Applied Sciences 9, no. 15: 3042. https://doi.org/10.3390/app9153042
APA StyleHeller Murray, E. S., Hseu, A. F., Nuss, R. C., Harvey Woodnorth, G., & Stepp, C. E. (2019). Vocal Pitch Discrimination in Children with and without Vocal Fold Nodules. Applied Sciences, 9(15), 3042. https://doi.org/10.3390/app9153042