External Unilateral Fixator of Own Design for the Treatment of Selected Mandibular Fractures in Horses



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
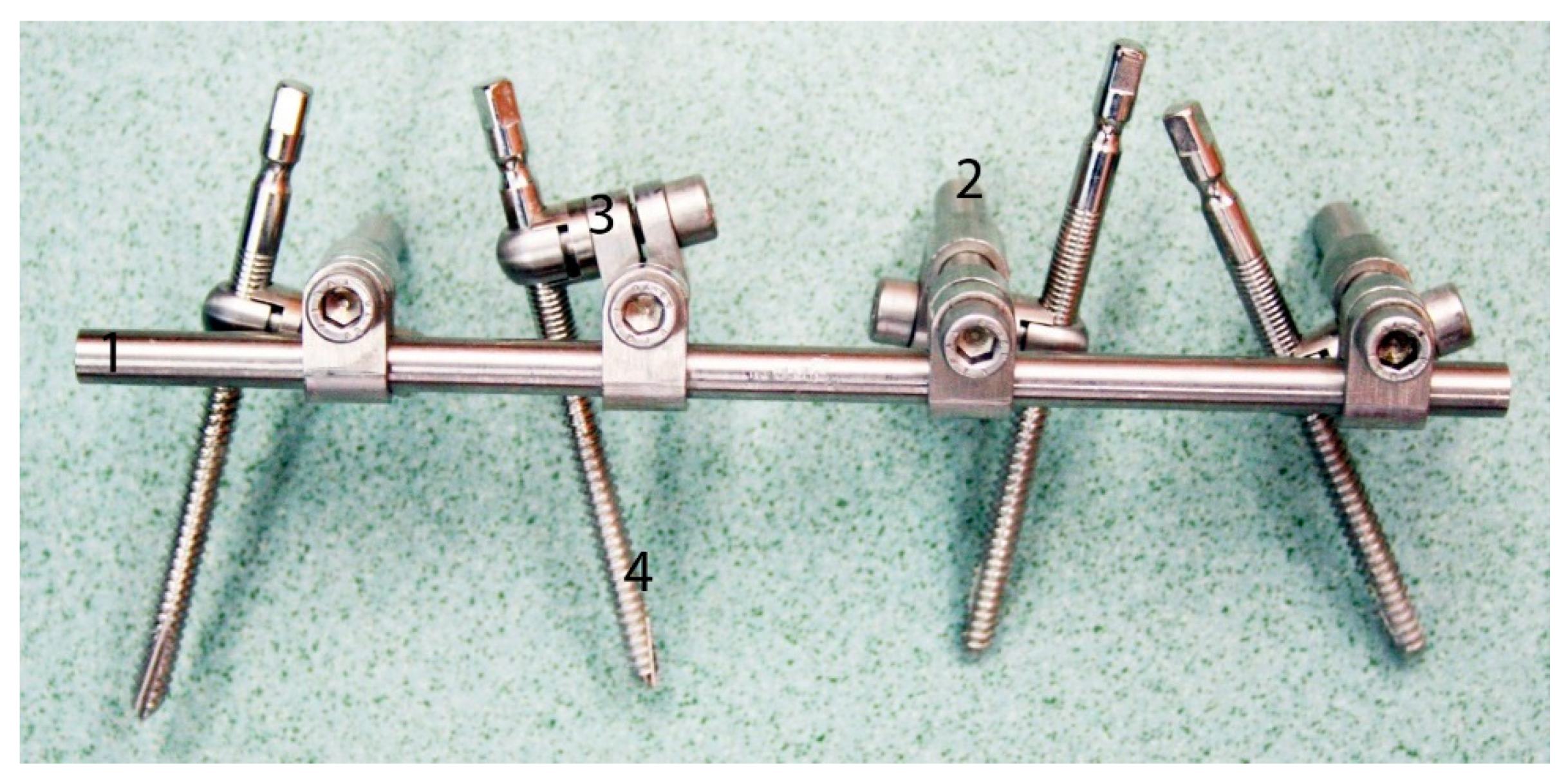
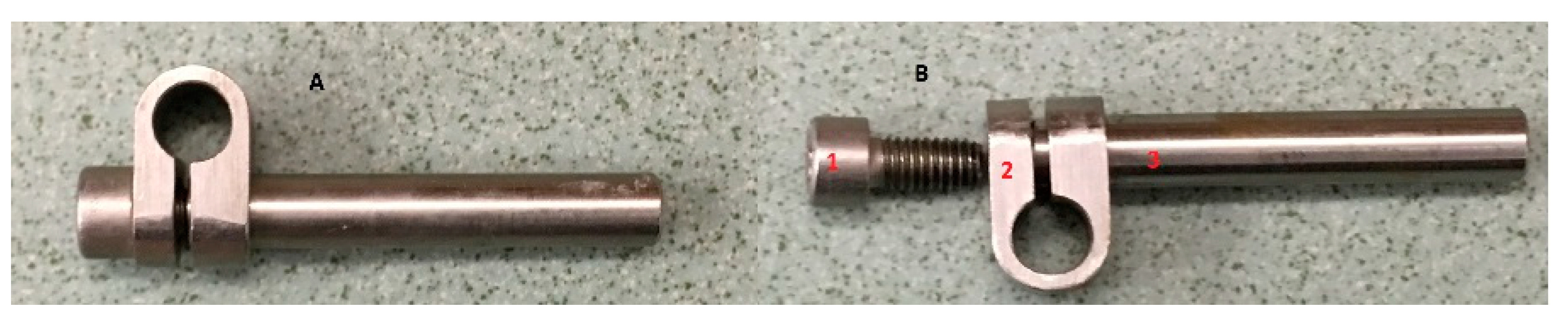
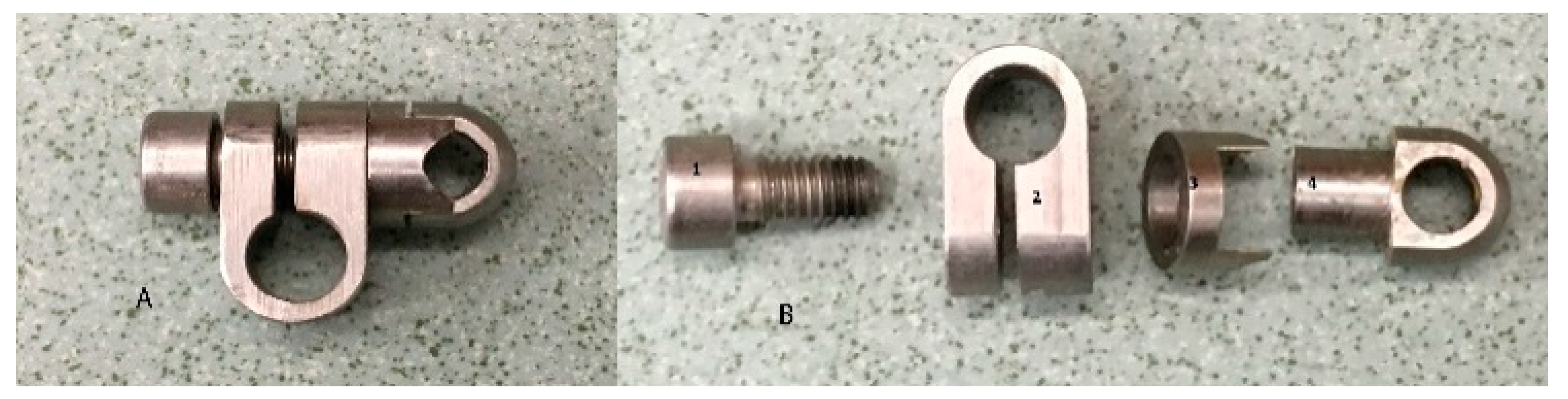
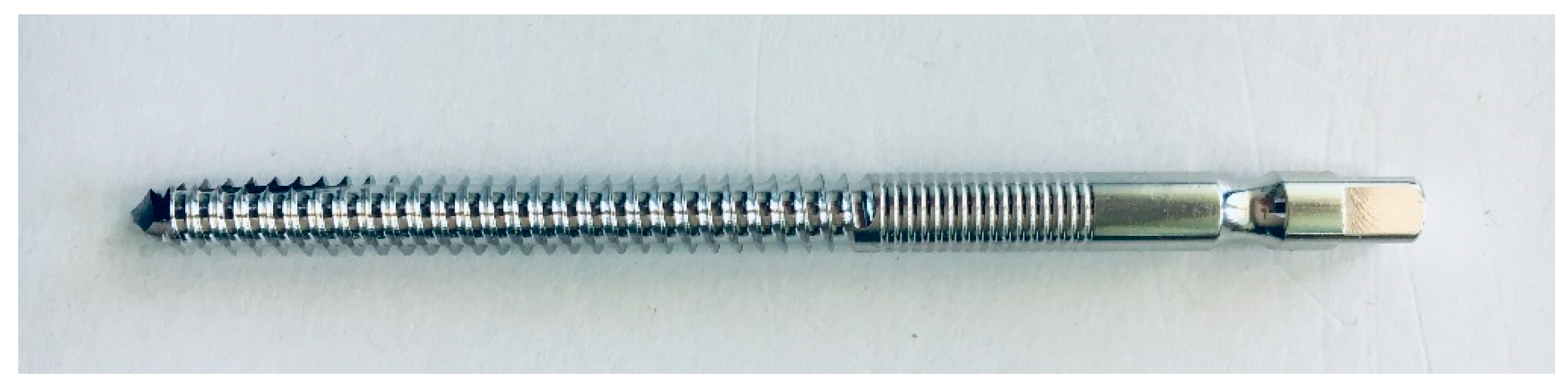
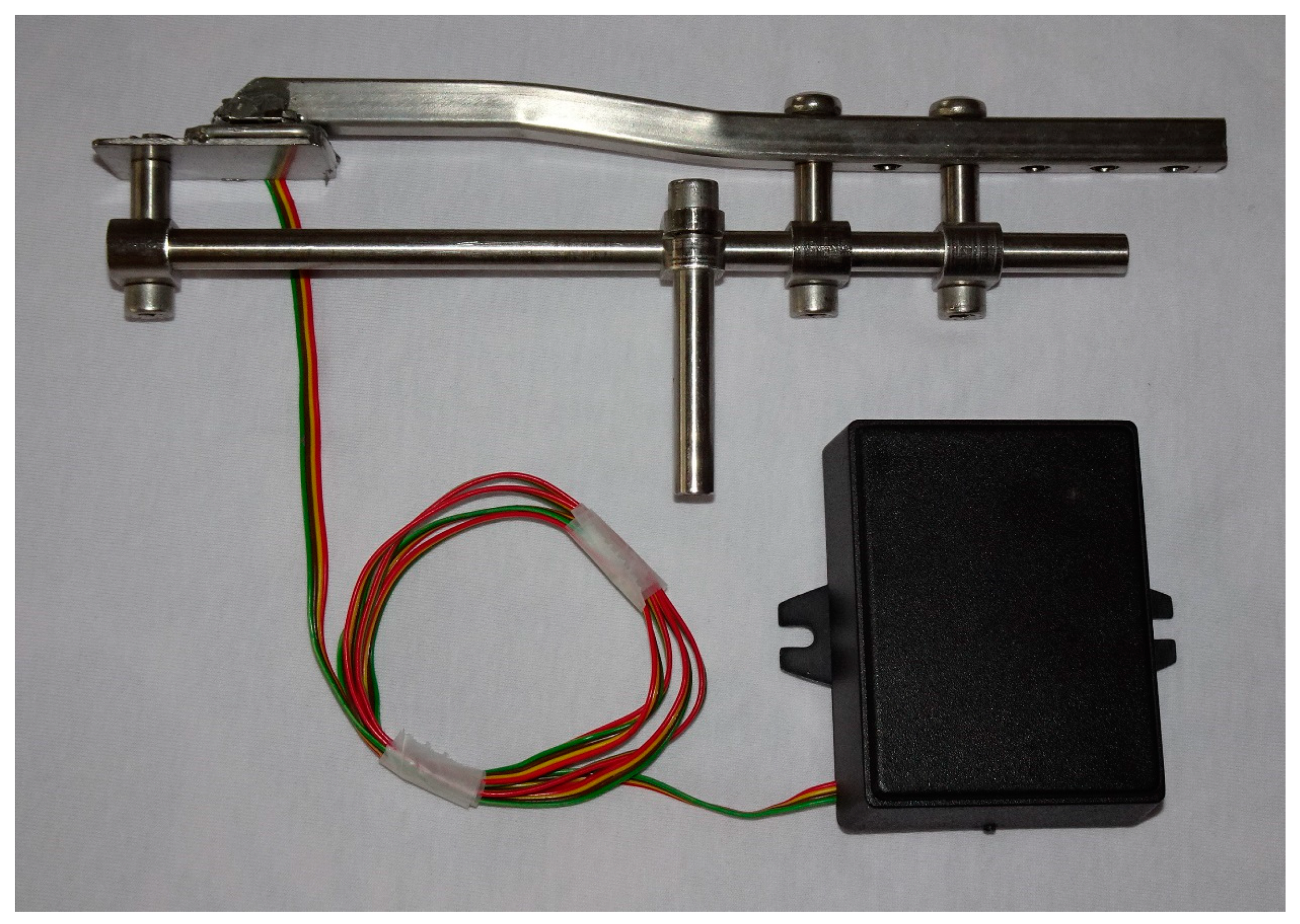
2.1. Structure of the Fixator
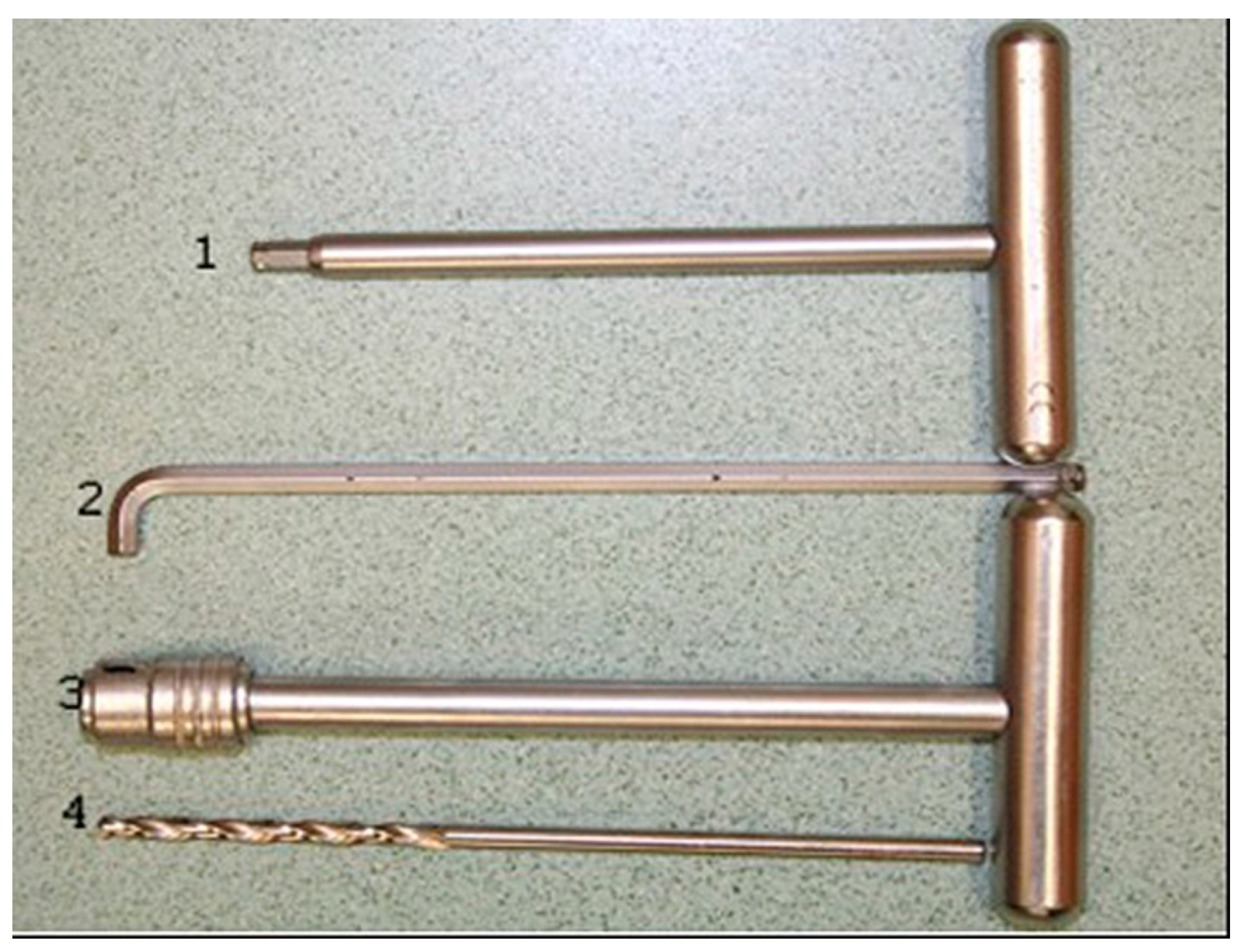
2.2. Instruments Used for Application
2.3. Surgical Technique Used for Application of the External Skeletal Fixator
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Monin, T. Tension band repair of equine mandibular fractures. J. Equine Med. Surg. 1977, 1, 325–329. [Google Scholar]
- DeBowes, R.M. Fractures of the mandible and maxilla. In Equine Fracture Repair, 1st ed.; Nixon, A.J., Ed.; W.B. Saunders Co.: Philadelphia, PA, USA, 1996; pp. 323–335. [Google Scholar]
- Tremaine, W.H. Management of equine mandibular injuries. Equine Vet. Educ. 1998, 10, 146–154. [Google Scholar] [CrossRef]
- Peavey, C.L.; Edward, R.B., III; Escarcega, A.J.; Vanderby, R., Jr.; Markel, M.D. Fixation technique influences the monotonic properties of equine mandibular fracture constructs. Vet. Surg. 2003, 32, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Belsito, K.A.; Fischer, A.T. External skeletal fixation in the management of equine mandibular fractures: 16 cases (1988–1998). Equine Vet. J. 2001, 33, 176–183. [Google Scholar] [CrossRef]
- Widmer, A.; Fürst, A.; Bettschart, R.; Makara, M.; Geyer, H.; Kummer, M. Bilateral Iatrogenic Maxillary Fractures After Dental Treatment in Two Aged Horses. J. Vet. Dent. 2010, 3, 160–162. [Google Scholar] [CrossRef] [PubMed]
- Jansson, N. Conservative Management of Unilateral Fractures of the Mandibular Rami in Horses. Vet. Surg. 2016, 45, 1063–1065. [Google Scholar] [CrossRef] [PubMed]
- Haralambus, R.M.A.; Werren, C.; Brehm, W.; Tessier, C. Use of a Pinless External Fixator for Unilateral Mandibular Fracture Repair in nine Equids. Vet. Surg. 2010, 39, 761–764. [Google Scholar] [CrossRef] [PubMed]
- Lischer, C.J.; Fluri, E.; Kaser-Hotz, B.; Bettschart-Wolfenberger, R.; Auer, J.A. Pinless external fixation of mandible fractures in cattle. Vet. Surg. 1997, 26, 14–19. [Google Scholar] [CrossRef]
- Henninger, R.W.; Beard, W.L.; Schneider, R.K.; Bramlage, L.R.; Burkhardt, H.A. Fractures of the rostral portion of the mandible and maxilla in horses: 89 cases (1979–1997). J. Am. Vet. Med. Assoc. 1999, 214, 1648–1652. [Google Scholar]
- Auer, J.A. Mandible, maxilla and skull. In AO Principles of Equine Ostheosynthesis; Fackelman, G.E., Auer, J.A., Nunamaker, D.M.N., Eds.; Thieme Verlag: Stuttgart, Germany, 2000; pp. 35–49. [Google Scholar]
- Auer, J.A. Craniomaxillofacial disorders. In Equine Surgery, 3rd ed.; Auer, J.A., Stick, J.A., Eds.; Saunders Elsevier: St. Louis, MO, USA, 2006; pp. 1341–1362. [Google Scholar]
- Kuemmerle, J.M.; Kummer, M.A.; Auer, J.A.; Nitzl, D.; Fürst, A.E. Locking compression plate osteosynthesis of complicated mandibular fractures in six horses. Vet. Comp. Orthop. Traumatol. 2009, 22, 54–58. [Google Scholar]
- Kuemmerle, J.M. Mandibular fractures in horses. Equine Vet. Educ. 2012, 24, 222–224. [Google Scholar] [CrossRef]
- Caldwell, F.J.; Davis, H.A. Surgical reconstruction of a severely comminuted mandibular fracture in a horse. Equine Vet. Educ. 2012, 24, 217–221. [Google Scholar] [CrossRef]
- Beard, W. Fracture repair techniques for the equine mandible and maxilla. Equine Vet. Educ. 2009, 21, 352–357. [Google Scholar] [CrossRef]
- Durket, E.; Kersh, K.; Dembek, K.; Riedesel, E.; Silverstone, A.; Kraus, K.H. Influence of plate type and placement on the immobilization of bilateral equine mandibular osteotomies: Ex vivo study. Vet. Surg. 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Amerinatanzi, A.; Mehrabi, R.; Ibrahim, H.; Dehghan, A.; Moghaddam, N.S.; Elahinia, M. Predicting the Biodegradation of Magnesium Alloy Implants: Modeling, Parameter Identification, and Validation. Bioengineering 2018, 5, 105. [Google Scholar] [CrossRef] [PubMed]
- Beste, K.; Glass, K.; Watkins, J. Intramedullary, Interlocking Nail Fixation Alone or in Combination with a Cranial Bone Plate to Repair Diaphyseal Femur Fractures in 16 Foals Weighing Less than 250 kg (1993–2016). Vet. Comp. Orthop. Traumatol. 2018, 31, A1–A25. [Google Scholar] [CrossRef]
- Sisk, T.D. External fixation. Historic review, advantages, disadvantages, complications and indications. Clin. Orthop. Relat. Res. 1983, 180, 15–21. [Google Scholar]
- Vogel, S.R.; Anderson, D.E. External Skeletal Fixation of Fractures in Cattle. Vet. Clin. Food Anim. 2014, 30, 127–142. [Google Scholar] [CrossRef]
- Turek, B.; Potyński, A.; Wajler, C.; Szara, T.; Czopowicz, M.; Drewnowska, O. Biomechanical study in vitro on the use of self-designed external fixator in diaphyseal III metacarpal fractures in horses. Polish J. Vet. Sci. 2015, 18, 323–332. [Google Scholar] [CrossRef]
- Turek, B.; Potyński, A.; Drewnowska, O. Own-design external fixator for the treatment of diaphyseal fractures of the third metacarpal bone in horses. Med. Weter. 2016, 72, 197–202. [Google Scholar]
- Lescun, T.B.; Baird, D.K.; Oliver, L.J.; Adams, S.B.; Hawkins, J.F.; Moore, G.E. Comparison of hydroxyapatite-coated and uncoated pins for transfixation casting in horses. Am. J. Vet. Res. 2012, 73, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Dehghanghadikolaei, A.; Ibrahim, H.; Amerinatanzi, A.; Ashemi, M.; Moghaddam, N.S.; Elahinia, M. Improving corrosion resistance of additively manufactured nickel–titanium biomedical devices by micro-arc oxidation process. J. Mater. Sci. 2019, 54, 7333–7355. [Google Scholar] [CrossRef]
- Wagner, M. General principles for the clinical use of the LCP. Injury 2003, 34 (Suppl. 2), B31–B42. [Google Scholar] [CrossRef] [PubMed]
- Auer, J.; Grainger, D. Fracture management in horses: Where have we been and where are we going? Vet. J. 2015, 206, 5–14. [Google Scholar] [CrossRef] [PubMed]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turek, B.; Drewnowska, O.; Kapłan, M. External Unilateral Fixator of Own Design for the Treatment of Selected Mandibular Fractures in Horses. Appl. Sci. 2019, 9, 2624. https://doi.org/10.3390/app9132624
Turek B, Drewnowska O, Kapłan M. External Unilateral Fixator of Own Design for the Treatment of Selected Mandibular Fractures in Horses. Applied Sciences. 2019; 9(13):2624. https://doi.org/10.3390/app9132624
Chicago/Turabian StyleTurek, Bernard, Olga Drewnowska, and Marcin Kapłan. 2019. "External Unilateral Fixator of Own Design for the Treatment of Selected Mandibular Fractures in Horses" Applied Sciences 9, no. 13: 2624. https://doi.org/10.3390/app9132624
APA StyleTurek, B., Drewnowska, O., & Kapłan, M. (2019). External Unilateral Fixator of Own Design for the Treatment of Selected Mandibular Fractures in Horses. Applied Sciences, 9(13), 2624. https://doi.org/10.3390/app9132624