Efficacy of Collagen-Based Membranes in Alveolar Bone Augmentation



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Bone Augmentation Surgical Protocol
2.3. Implantation Protocol
2.4. Radiographic Examination
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tallgren, A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J. Prosthet. Dent. 2003, 89, 427–435. [Google Scholar] [CrossRef]
- Carlsson, G.E.; Thilander, H.; Hedegard, B. Histologic changes in the upper alveolar process after extractions with or without insertion of an immediate full denture. Acta Odontol. Scand. 1967, 25, 21–43. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef]
- Leong, D.J.; Oh, T.J.; Benavides, E.; Al-Hezaimi, K.; Misch, C.E.; Wang, H.L. Comparison between sandwich bone augmentation and allogenic block graft for vertical ridge augmentation in the posterior mandible. Implant Dent. 2015, 24, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.P.; Magner, A.W.; Fletcher, P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J. Periodontol. 1992, 63, 995–996. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Ostman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Aloy-Prosper, A.; Penarrocha-Oltra, D.; Penarrocha-Diago, M.; Penarrocha-Diago, M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, e251–e258. [Google Scholar] [CrossRef] [PubMed]
- Milinkovic, I.; Cordaro, L. Are there specific indications for the different alveolar bone augmentation procedures for implant placement? A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 606–625. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruiz, R.A.; Calvo-Guirado, J.L.; Abboud, M.; Ramirez-Fernández, M.P.; Maté-Sánchez, J.E.; Negri, B.; Won, A.; Romanos, G. Porous titanium granules in critical size defects of rabbit tibia with or without membranes. Int. J. Oral Sci. 2014, 6, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruiz, R.; Romanos, G.E.; Alexandre Gerhke, S.; Gomez-Moreno, G.; Mate-Sanchez de Val, J.E.; Calvo-Guirado, J.L. Biological effects of compressive forces exerted on particulate bone grafts during socket preservation: Animal study. Clin. Oral Implants Res. 2018, 29, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Rothamel, D.; Herten, M.; Sager, M.; Becker, J. Angiogenesis pattern of native and cross-linked collagen membranes: An immunohistochemical study in the rat. Clin. Oral Implants Res. 2006, 17, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Delgado, L.M.; Bayon, Y.; Pandit, A.; Zeugolis, D.I. To cross-link or not to cross-link? Cross-linking associated foreign body response of collagen-based devices. Tissue Eng. Part B Rev. 2015, 21, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Becker, J.; Al-Nawas, B.; Klein, M.O.; Schliephake, H.; Terheyden, H.; Schwarz, F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: A prospective, randomized-controlled double-blinded clinical multicenter study. Clin. Oral Implants Res. 2009, 20, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, A.; Gissel, K.; Soudan, M.; Kleber, B.M.; Pitaru, S.; Dietrich, T. Randomized controlled trial on lateral augmentation using two collagen membranes: Morphometric results on mineralized tissue compound. J. Clin. Periodontol. 2011, 38, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Charulatha, V.; Rajaram, A. Influence of different crosslinking treatments on the physical properties of collagen membranes. Biomaterials 2003, 24, 759–767. [Google Scholar] [CrossRef]
- Jung, R.E.; Fenner, N.; Hammerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implants Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Owens, K.W.; Yukna, R.A. Collagen membrane resorption in dogs: A comparative study. Implant Dent. 2001, 10, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Sela, M.N.; Kohavi, D.; Krausz, E.; Steinberg, D.; Rosen, G. Enzymatic degradation of collagen-guided tissue regeneration membranes by periodontal bacteria. Clin. Oral Implants Res. 2003, 14, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Zubery, Y.; Goldlust, A.; Alves, A.; Nir, E. Ossification of a novel cross-linked porcine collagen barrier in guided bone regeneration in dogs. J. Periodontol. 2007, 78, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Zubery, Y.; Nir, E.; Goldlust, A. Ossification of a collagen membrane cross-linked by sugar: A human case series. J. Periodontol. 2008, 79, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.G.K.; Oh, J.H. Recent advances in dental implants. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 33. [Google Scholar] [CrossRef] [PubMed]
- Park, J.C.; Kim, Y.H.; Choi, H.S.; Oh, J.S.; Shin, S.H.; Kim, Y.D. The rate and stability of mandibular block bone graft in recent 5 years. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 21. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
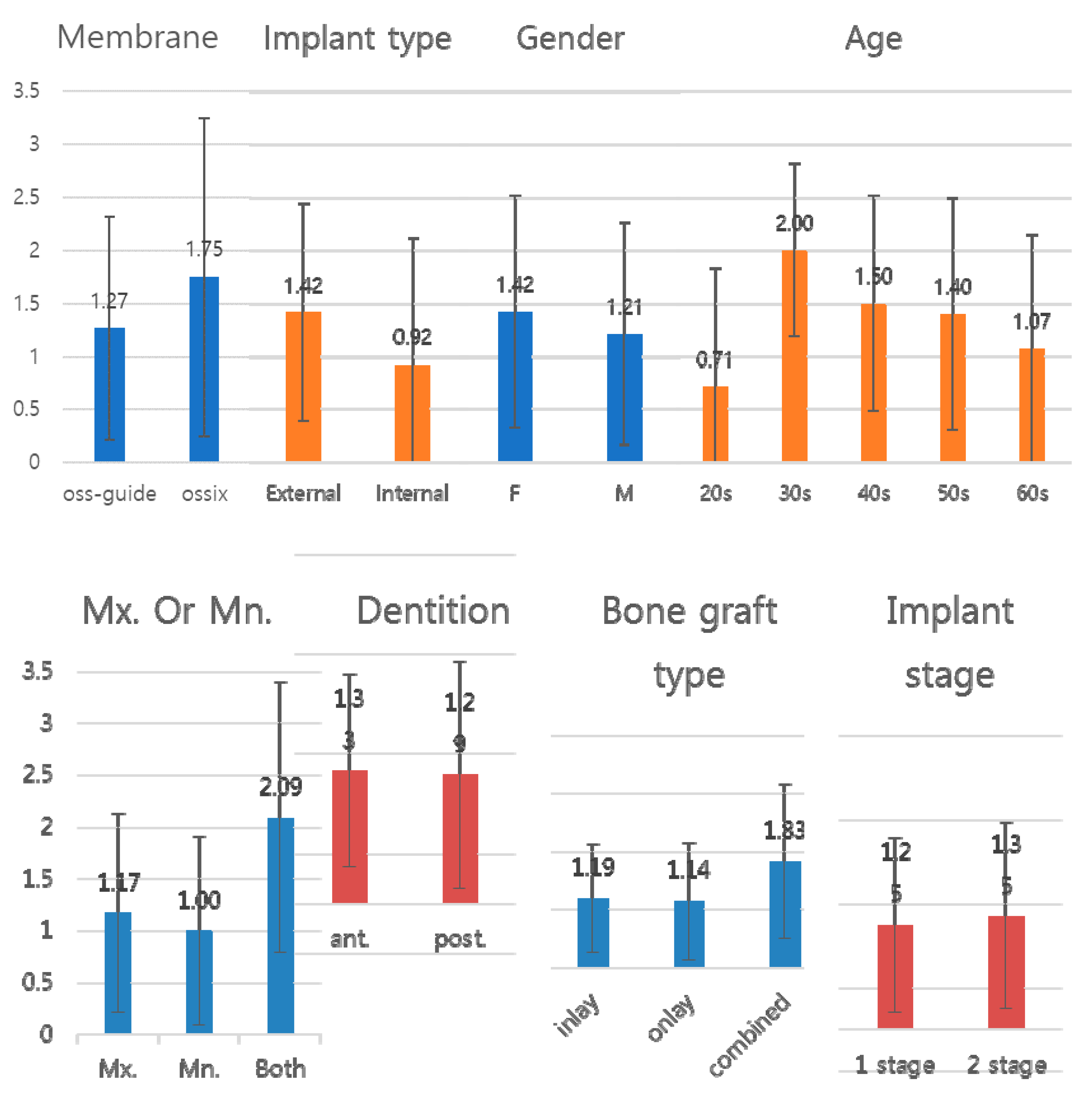
| Factors | Number of Patients | Number of Exposed Threads | F Value | p (<F) | |
|---|---|---|---|---|---|
| Gender | M | 30 | 1.212121 | 0.56 | 0.457 |
| F | 26 | 1.423077 | |||
| Age | 20s | 7 | 0.714286 | 0.026 | 0.871 |
| 30s | 4 | 2.000000 | |||
| 40s | 14 | 1.500000 | |||
| 50s | 17 | 1.400000 | |||
| Above 60s | 14 | 1.250000 | |||
| Mx. or Mn. | Mx. | 32 | 1.171429 | 4.174 | 0.020 (*) |
| Mn. | 13 | 1.000000 | |||
| both | 11 | 2.090909 | |||
| Extracted teeth position (dentition) | Ant. | 21 | 1.333333 | 0.022 | 0.882 |
| Post. | 35 | 1.289474 | |||
| Bone graft type | Horizontal | 23 | 1.192308 | 1.903 | 0.159 |
| Vertical | 21 | 1.142857 | |||
| Combined | 12 | 1.833333 | |||
| Implantation stage | 1 stage | 28 | 1.250000 | 0.139 | 0.711 |
| 2 stage | 28 | 1.354839 | |||
| Implant type | External | 43 | 1.418605 | 2.156 | 0.148 |
| Internal | 13 | 0.923077 | |||
| Membrane type | NCLM | 52 | 1.269231 | 0.736 | 0.395 |
| CLM | 4 | 1.750000 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, N.-R.; Sándor, G.K.; Kim, Y.-D. Efficacy of Collagen-Based Membranes in Alveolar Bone Augmentation. Appl. Sci. 2018, 8, 2048. https://doi.org/10.3390/app8112048
Choi N-R, Sándor GK, Kim Y-D. Efficacy of Collagen-Based Membranes in Alveolar Bone Augmentation. Applied Sciences. 2018; 8(11):2048. https://doi.org/10.3390/app8112048
Chicago/Turabian StyleChoi, Na-Rae, George K. Sándor, and Yong-Deok Kim. 2018. "Efficacy of Collagen-Based Membranes in Alveolar Bone Augmentation" Applied Sciences 8, no. 11: 2048. https://doi.org/10.3390/app8112048
APA StyleChoi, N.-R., Sándor, G. K., & Kim, Y.-D. (2018). Efficacy of Collagen-Based Membranes in Alveolar Bone Augmentation. Applied Sciences, 8(11), 2048. https://doi.org/10.3390/app8112048