Abstract
Musculoskeletal disorders, particularly lower back pain, are common among healthcare workers due to frequent lifting, bending, and prolonged standing. To address this issue, we developed a lightweight, soft, and active exoskeleton designed to support lifting movements while maintaining user mobility and comfort. This paper presents the design of the exoskeleton. To assess the physiological effects on the wearer’s body, we conducted a biomechanical analysis, evaluating joint kinematics (hip and knee) and muscle activation (m. erector spinae and m. semitendinosus) during a lifting task. The results showed that the exoskeleton effectively reduced muscle activation in the m. erector spinae by 15.82 ± 13.35% and m. semitendinosus by 19.89 ± 20.84% without significantly altering the analyzed joint kinematics. These findings indicate that the system provides targeted support without restricting mobility, making it a promising tool for reducing physical strain in healthcare and other physically demanding professions.
1. Introduction
Musculoskeletal disorders, such as low back pain and disc herniations, are prevalent among workers whose jobs involve frequent, repetitive, and physically demanding tasks, particularly those that require the handling of heavy loads over extended periods [1]. One high-risk profession is caregiving, where daily tasks include lifting and transferring patients from beds to wheelchairs and assisting them in walking [2]. To mitigate these risks, various ergonomic aids, such as lifting devices, sliding boards, and techniques for back-friendly lifting, are available [3]. However, despite these measures, physical strain remains high, and many of these aids are either time-consuming to use, restricted to specific locations, or impractical for flexible application in dynamic work environments. As a result, an approach to reduce physical strain is the use of task-specific exoskeletons. These wearable support devices are designed to provide personalized and adaptable support in physically demanding work environments while addressing the limitations of traditional lifting aids [4,5]. However, exoskeletons do not reduce the external loads acting on the body; instead, they influence the distribution and management of these loads by the musculoskeletal system. Their assistive function primarily affects the internal strain on biological structures rather than eliminating the mechanical load itself. By redistributing forces from more vulnerable body regions, such as the lower back, to stronger areas, exoskeletons can reduce stress on specific muscle groups and joints. In the fields of healthcare and nursing, exoskeletons have received positive qualitative feedback, particularly regarding their ability to reduce pain and fatigue while improving posture [6]. By reducing back muscle activity [7] and spinal compression forces [8], these devices can lower the risk of developing lower back pain (LBP). Moreover, exoskeletons can help reduce common work-related risk factors for musculoskeletal disorders in the healthcare sector, such as high physical exertion, repetitive tasks, and prolonged awkward postures [9].
Exoskeletons vary in form, structure, and function, each with inherent advantages and limitations depending on the materials used, structural design, and intended applications [10,11,12,13]. A key structural distinction exists between soft and rigid exoskeletons. Soft materials, such as textiles and elastomers, offer flexibility and enhance user comfort, whereas rigid materials like metals and composites provide durability and superior load-bearing capacity. Due to their ability to withstand both tensile and compressive forces, rigid components are preferred for applications requiring higher force transmission. The choice of material is influenced by factors such as the level of support needed, duration of use, and user-specific requirements. To leverage the advantages of both material types, hybrid exoskeletons integrate soft fabrics at human-system interfaces while employing rigid components to redistribute supportive forces and counteract unwanted compression. This design approach strikes a balance between comfort and structural integrity, thereby optimizing performance for specific tasks [14].
Exoskeletons can provide support in five distinct ways: enabling, enhancing, facilitating, stabilizing, and complementing movement [5]. The specific type of support influences the design and functionality of the exoskeleton. To achieve these different forms of assistance, exoskeletons rely on various actuation methods and structural principles. Regarding their supportive function, exoskeletons can utilize either passive mechanisms, such as elastic bands or hydraulic cylinders, or active actuators, including electric motors and pneumatic systems. The choice of actuation method depends on factors such as the required force output, response dynamics, and capacity of the available power source. Passive exoskeletons are generally lightweight, cost-effective, and maintenance-friendly, making them suitable for tasks requiring lower assistance. In contrast, active exoskeletons can generate higher levels of support and allow precise, time-dependent force control, making them more adaptable to dynamic and demanding applications [15].
Advancements in exoskeleton technology have enabled the development of support systems that dynamically adjust their support characteristics based on the user’s movements and external conditions [16]. To achieve this, various sensors, such as capacitive force cells and inertial measurement units, are required to detect the interactions between the user, exoskeleton, and environment. By utilizing sensor data as input for the control strategy, adaptive exoskeletons offer enhanced usability and versatility across a broader range of tasks compared to passive systems. This optimization maximizes the exoskeleton’s potential while improving user comfort and productivity. However, these benefits come at the cost of increased complexity in development, maintenance, design, and energy consumption, emphasizing the need to carefully consider context-specific requirements and constraints [17].
Considering the working conditions of nurses and care workers in hospitals, healthcare facilities, or home care settings, exoskeletons must meet specific requirements to ensure safe and effective use during patient interactions. To accommodate the high range of motion required for lifting tasks, these systems should be lightweight and non-restrictive, minimizing interference with natural movements. Since nurses often work in confined spaces while lifting or transferring patients, wearable exoskeletons must be designed to fit closely with the wearer and remain unobtrusive [18]. Given these constraints, fabric-based exosuits are well-suited for prolonged wear in dynamic care environments due to their flexibility and comfort. However, caregiving tasks frequently involve handling heavy loads, making it essential to integrate rigid components for structural support and load-bearing capabilities. This is particularly important in active exoskeletons, where actuation mechanisms must provide the necessary assistance while adapting to various tasks [19].
In order to combine the advantages of lightweight passive exoskeletons with the adaptability of active systems, a compact active exoskeleton was developed, featuring an efficient and straightforward control strategy specifically tailored to assist lifting motions. This paper outlines the design of a newly developed exoskeleton aimed at supporting the lower back during lifting activities and presents an evaluation of its biomechanical impact. To assess the biomechanical effects, we analyzed the hip and leg kinematics and muscle activation in healthy participants while performing lifting tasks with and without the activated exoskeleton. The objective of this study was to examine variations in joint kinematics and muscle activity between the two experimental conditions. We hypothesized that the joint angle trajectories would remain unchanged due to the biomimetic design and highly dynamic actuation system. In contrast, we expected a reduction in muscle activation when using the exoskeleton, as the applied assistive force should alleviate the muscular strain during lifting.
2. Exoskeleton Functionality and Design
This section outlines the functional principles and technical components of the proposed exoskeleton. The key aspects of the concept, functionality, system design, actuation, control, and sensory systems are described in detail.
2.1. Concept and Functionality
The developed exoskeleton is designed to support lifting movements from the ground to the hip height, such as squat lifting. By providing mechanical support to the lumbar region, the exoskeleton aims to reduce the risk of lower back pain and injuries associated with lifting, bending, and standing for prolonged periods. Considering the primary involvement of the lower back muscles in lifting tasks, the system follows a biomimetic design using a cable-driven mechanism that runs parallel to the involved muscle chain during upper body extension. This biologically inspired approach allows for the use of smaller actuators and a more compact, form-fitting design compared to systems that use direct-mounted actuators positioned parallel to the hip joint, which requires high torque. To replicate the function of the back muscles and provide effective support, the system generates tensile forces that, together with a lever arm, produce torque around the hip joint. However, these tensile forces also introduce compression forces that must be redirected away from sensitive body areas, such as the spine, to avoid discomfort or unintended strain. To address this, the exoskeleton incorporates materials that are rigid in compression to effectively transmit support forces while remaining flexible along the vertical axis to allow for natural upper body flexion.
To estimate the required dynamics of the actuation units, the tension force and shortening velocity of the steel cable were approximated based on insights from the literature. To calculate the hip joint torque, the relative weights of the upper body segments and their respective distances from the lumbosacral joint were obtained from Grieve and Pheasant [20]. Figure 1 illustrates an example of the absolute values for a 62 kg person. The right side depicts the main concept of the exoskeleton.
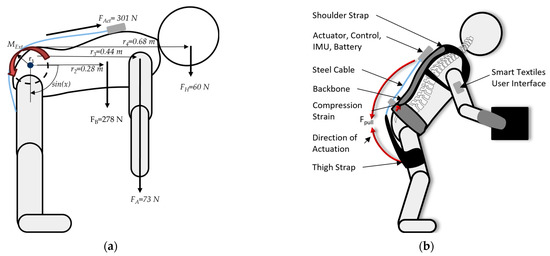
Figure 1.
(a) Segment weights and distances from the lumbosacral joint [20] and (b) illustration of the concept.
The force required to be applied to the steel cables is determined using the following formula, which is derived from the torque equation at the hip joint considering the weight distribution of the upper body, arms, and head:
where represent the weights of the body (B), arms (A), and head (H), and denote the corresponding lever arms. The parameter refers to the lever arm from the hip joint to the cable with approximately , considering a pulley system, while accounts for the upper body bending angle. Since the goal is to support 30% of the body weight against gravity, the required actuation force is reduced by 70%. Consequently, at a bending angle of , the minimum force required to provide support during lifting is . Considering a more moderate bending angle of during a semi-squat lift, the required force is .
In addition to the required tension, the overall dynamics of the actuation unit depend on the shortening velocity of the steel cable. This velocity determines how quickly the system can adapt to the movement and provide effective support. In the context of nursing tasks, Jang et al. [21] provide insights into the kinematics of everyday caregiving activities. Based on their findings, the mean sagittal angular velocity of the upper body is reported as . To approximate the required linear shortening velocity of the steel cable, the following equation is used, which is based on the calculation of the chord length:
where is the shortening of the steel cable, is the time interval, and represents the angular displacement during one second, derived from the mean angular velocity . This results in a required minimum shortening velocity of .
To ensure a high level of comfort and flexibility, the design incorporates soft fabrics as human-system interfaces. The shoulder straps and hip belt, worn like a backpack, distribute the actuation forces to the upper body. Additionally, the thigh straps serve as an anchor point, allowing the force to be applied below the hip joint. A pulley integrated into the hip belt provides the necessary lever arm by guiding the steel cable.
2.2. Exoskeleton Design
The active back exoskeleton combines soft and rigid materials, with all components easily adaptable to different users. Soft textiles serve as human-system interfaces, ensuring high wearing comfort without restricting passive joint movement. The exoskeleton supports the wearer during lifting tasks by generating a backward pulling force on the upper body, which is applied using an electric actuator. Force transmission follows a path from the actuator, located at the back of the shoulder vest, to the back of the thigh via a steel cable. Two pulleys on each side guide the cable and maintain a consistent lever arm relative to the body. The total mass of the exoskeleton is currently 3.3 kg (without a special focus on lightweight design).
The exoskeleton consists of four main components: (1) a supporting and force-transmitting structure, (2) an actuation system, (3) a sensory system, and (4) a control unit. The system is illustrated in Figure 2 with each component described in the following sections.
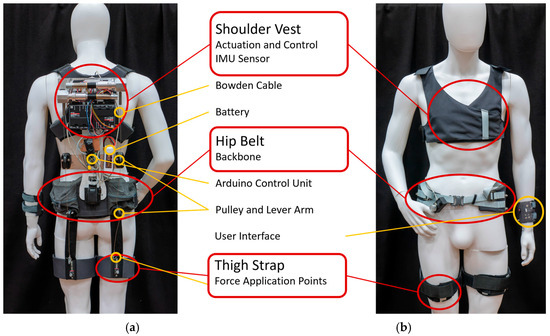
Figure 2.
(a) rear view and (b) frontal view of the exoskeleton.
2.2.1. Supporting and Force-Transmitting Structure
An important component of exoskeleton functionality is its structural design, which enables effective force transmission from the actuator to the body. To meet the two key requirements of efficient force transfer and high wearing comfort with user adaptability, carefully selected materials with specific properties are used.
The structure consists of four main elements: (1) shoulder vest, (2) hip belt, and (3) thigh straps, which serve as human-system interfaces, ensuring comfort and adaptability. Additionally, (4) two steel cables connect the actuator to the body to facilitate force transmission.
The supporting structure comprises four main parts:
- (1)
- Force Transmission—Two steel cables (1.5 mm diameter, tensile strength 1570 Nm/mm2; 7 × 7) are used to transmit the actuation force from the actor—which is located at the back of the shoulder west—to the back of the thighs, using the thigh straps, to ensure a supporting force along the spine and hip. To maintain a consistent distance between the body and the cable, two pulleys (PA6 plastic, 35 mm Ø, low-friction ball bearing) are used in the lumbar spine area and at the lower part of the hip belt. This creates a 10 cm lever arm around the hip, enabling the lifting of the upper body and extension of the thighs. Therefore, two-way support is provided for both the upper and lower body around the hip, which acts as a fulcrum.
- (2)
- Shoulder Vest—A shoulder vest is created using a soft and unstretchable 1000 D Cordura® nylon fabric. It has two functions: (1) to guarantee high wearing comfort and (2) to transmit the actuation strain to the torso. Regarding wearing comfort, the vest is soft and adaptable to different body shapes by adjusting the size using Velcro tapes at the shoulders and sides of the torso. Moreover, the closed-cell EVA foam material at the back helps prevent painful pressure points. To effectively transmit the actuation force to the upper body, the used fabric is stiff when tension is applied (tensile strength > 1800 N). The backbone between the shoulder vest and hip belt transmits the force from the actuator to the hip and is attached to the vest by a ball bearing, allowing free mobility of the upper torso.
- (3)
- Hip Belt with Backbone—The hip belt is also made of Cordura® fabrics with an EVA foam inlet and a size-adaptable strap. In the lumbar region, a spinal support structure (aluminum, 2 mm thickness) is attached to facilitate the transmission of compressive forces along the spinal axis to the pelvic region. As the flexibility of the hip belt contrasts with the force transmission of the backbone, a PA12 plastic inlay is integrated into the hip belt to prevent deformation and effectively apply force to the hip. In addition to the backbone stiffness along the longitudinal axis, it is flexible along the sagittal axis, allowing for bending forward and backward movements. For lateral bending movements along the transverse axis, the backbone is mounted to the hip belt using a needle bearing. To adjust the size of the exoskeleton according to the length of the wearers back, a mechanism enables the backbone to move in and out.
- (4)
- Thigh Straps—Using straps, the actuation force can be applied to the thighs to support hip extension during lifting. The straps must be tightened comfortably to match the shape of the thighs. In contrast, a high stiffness is required to transmit the force from the attached steel cable. To fulfill both requirements, the thigh straps are made of inner and outer components. The inner component is made of elastic Lycra® fabric (25% Spandex, 75% Nylon) fabric to be able to tighten it firmly to the body without slipping. The outer component comprises a plastic inlay to which the steel cable is attached. Both components are connected to each other, and the straps are tightened using a Velcro fastener. Therefore, the applied force can be effectively transmitted to the thigh using a stiff material while maintaining wearing comfort due to the flexible fabric.
2.2.2. Actuation
The actuation part was composed of two electric EC-4 maxon motors (22 mm, 90 W) in combination with a GP 22 planetary gearhead with a reduction ratio of 62:1 and the positioning control EPOS4 50/5. The nominal torque of the motor is 45 mNm, with a nominal speed of 15,000 rpm. The planetary gearhead has a nominal output torque of 3 Nm and a maximum permissible input speed of 12,000 rpm. Considering a gear ratio of 62:1, the final output of the actuator provides a torque of approximately 2.79 Nm at 193 rpm. The motor-gearhead combination was specifically chosen to meet the force and velocity requirements via a pulley system while keeping the system compact and lightweight (~193 g incl. gearhead) for wearable application. Considering the calculated required force of minimum and a shortening velocity of , we created a pulley with a diameter of in order to coil the steel cable by the torque of the motor. Using this setup, the tension force is calculated with
where M is the maximum torque of the motor, and r is the radius of the pulley.
The theoretically possible shortening velocity for each single side of the actuation unit is estimated with
where C is the circumference of the pulley, and n is the number of revolutions per minute of the motor. The power for the motors and controls is supplied by a 12-V DC lithium polymer battery.
2.2.3. Sensory
To detect lifting motion in the sagittal plane, three inertial measurement units (IMU) are attached to the top end of the backbone and thighs. These sensors continuously track motion by measuring the angle and angular velocity, providing real-time data on body movement. The BNO055 IMU Sensor integrates accelerometer, gyroscope, and magnetometer readings and performs internal signal fusion and filtering, delivering absolute orientation data (e.g., Euler angles) without requiring additional filtering in the microcontroller. This built-in processing improves the stability and accuracy of angle measurements during dynamic activities, such as lifting. Due to variations in postures among different users, the sensors are calibrated by resetting to zero when the user is in an upright standing position, ensuring accurate angle measurements relative to the body’s natural posture.
The IMU data is processed to determine the relative angle and angular velocity between the thighs and the upper body. This information is then used as input for the control algorithm, which dynamically adjusts the torque of the motors to provide the appropriate level of support. By continuously monitoring movement patterns, the exoskeleton can adapt to different lifting techniques and user behaviors, ensuring optimal assistance while minimizing the risk of harmful overloading.
2.2.4. Control
An Arduino Uno serves as the central processing unit for handling the sensory input signals and controlling the actuation output. It processes real-time data from inertial measurement units (IMUs) and translates them into control commands for the exoskeleton motors. To ensure a reliable and intuitive assistance system, a straightforward control algorithm is implemented, which adjusts the actuation force based on the bending angle of the hip joint.
To effectively categorize movement patterns, the algorithm classifies the wearer’s posture and actions into three distinct phases: (1) bending forward, (2) holding the position, and (3) bending upward (lifting). No active support is provided during the forward bending. However, a low-level pre-tension of 10% of the maximum motor torque is applied to prevent slack in the steel cables, ensuring a smooth and rapid engagement during subsequent movements. When the user reaches a holding position, the support force is dynamically calculated based on the bending angle. From an upright posture (0° hip flexion) to a 45° bending position, the supportive force follows a sinusoidal curve, gradually increasing from 0% to 70% of the maximum motor torque. The final 30% of the motor torque is allocated to support the lifting phase, providing assistance as the wearer straightens up.
To enhance robustness and prevent unintentional activation, an additional filtering mechanism is implemented. The system monitors angular velocity, applying a minimum threshold of 25 rad/s to reliably detect lifting movements while preventing false activation caused by minor swaying of the upper body in the sagittal plane.
2.2.5. Smart Textile User Interface
To enable the intuitive control of the exoskeleton and allow users to adjust key parameters, such as the supporting force, a wearable user interface was developed using smart textiles (Figure 3). The interface is designed as a wrist-worn device, ensuring easy accessibility while maintaining comfort and flexibility during use. The base structure consists of fabric materials, which allow the interface to be securely wrapped around the wearer’s wrist.
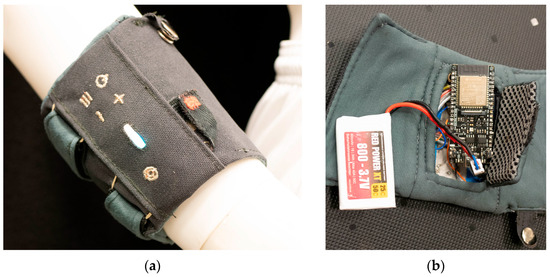
Figure 3.
Smart textile user interface (a) outside and (b) inside view with Arduino and battery.
The embedded hardware within the textile structure includes an Arduino microcontroller equipped with a Bluetooth module, which enables wireless data transmission to the exoskeleton. The system is powered by a 4.7V LiPo battery to ensure a compact and portable power supply for prolonged operation.
The user interface provides seamless control over the exoskeleton’s functions. A power button allows the user to switch the system on and off, while the plus and minus buttons enable real-time adjustment of the supporting force. The current force level is visually represented by an RGB-LED bar, which offers instant feedback on the exoskeleton’s assistance intensity. Additionally, a menu and reset button are integrated for further customization and system management.
To enhance usability and durability, the interface buttons are made of conductive yarn, allowing for touch-sensitive interaction while maintaining a lightweight and flexible design. However, physical manual buttons are implemented for essential functions, such as powering the interface and activating a key lock function to prevent unintended inputs. The use of smart textiles, wireless communication, and intuitive controls is intended to ensure user-friendly and efficient interaction with the exoskeleton, enhancing both functionality and user experience.
3. Evaluation
In order to evaluate the design concept of the exoskeleton, we conducted a study to evaluate the supportive function of the exoskeleton without restricting the lifting task. Using the described back exoskeleton, we assess the body kinematics and muscle activity of the m. erector spinae. In addition, we present the initial feedback and observations from the participants to gain insights into their subjective perception, acceptance, and usability.
This study was conducted in accordance with the guidelines of the Declaration of Helsinki. Informed consent was obtained from all participants, who were free to withdraw from the study at any time. The study was approved by the local ethics committee. The experiments were conducted after explaining the nature and possible consequences of exoskeletal systems.
3.1. Participants
Ten male subjects (n = 10 men; age 25 ± 3 years; mass 85 ± 14 kg) were recruited for the study from the student body of the Helmut-Schmidt-University. The test subjects had no previous experience with exoskeletons or biomechanical evaluations. Only healthy participants without low back pain or other impairments that affected lifting movements were considered eligible for the study.
3.2. Experimental Design
To measure body kinematics during the task, a mobile Xsens MTw Awinda System was used (Xsens Technologies BV, Enschede, The Netherlands). This device shows acceptable to excellent reliability and validity [22]. The muscle activity of the m. erector spinae and m. semitendinosus was recorded using a Myon 320 system (Myon AG, Schwarzenberg, Switzerland). The system exhibits good to acceptable reliability [23]. The sensor placement was conducted according to the SENIAM guidelines. To synchronize both systems, a trigger signal from Xsens was used to mark the start and stop of the EMG measurement.
Initially, a calibration walk consisting of eight circular steps was performed to calibrate the Xsens system. Subsequently, each participant donned the exoskeleton and adjusted the fit of the hip belt and shoulder vest. The thigh straps were fastened around the thighs of the participants. After activating the system, the participants were given a five-minute familiarization period to adapt to the exoskeleton and reduce the likelihood of adopting unintended protective postures during use. During the exoskeleton condition, the system was set to provide full support at 100%. They completed a lifting task in which they lifted a 10 kg object with both hands using two handles attached to the left and right of the object from the ground and placed it on a platform in front of them at hip height (Figure 4). After lifting the load, each participant placed it back on the floor in the starting position. The task consisted of 12 repetitions, performed at a frequency of 15 lifts per minute. A metronome was used to maintain a constant speed, which provided an acoustic signal for lifting and lowering the weight. The task was repeated with and without the exoskeleton, while the trials were randomized and stopped after the first signs of pain or any abnormal functions of the exoskeleton.
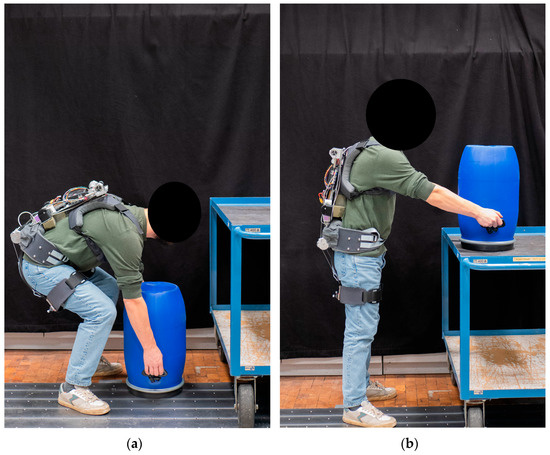
Figure 4.
Lifting task (exoskeleton condition) from (a) ground onto (b) platform.
3.3. Data Collection and Analyis
The data were captured using the provided Xsens Analyze software and ProEMG Software (2.1.3.6, Myon AG, Schwarzenberg, Switzerland, Win10) for the Myon320 system. To evaluate the exoskeleton’s supportive function, the muscle activity of the m. erector spinae and m. semitendinosus, which plays a key role in lifting tasks, was analyzed. The EMG data were rectified, bandpass filtered (4th order Butterworth filter; cut-off frequency, 20–220 Hz), and normalized to the peak value of the trial without the exoskeleton. In Xsens Analyze, start and end events were set in the kinematic data. The movement cycle began at 0% in a vertical body posture before grasping the object and ended at 100% in a vertical body posture after setting the weight down on the platform. The hip angle was analyzed in both the sagittal and frontal planes, and the knee angle was in the sagittal plane, as the exoskeleton primarily supports lifting movements involving forward and downward motion, which is likely to affect these degrees of freedom.
The data were further processed using MATLAB (9.5.0.944444, R2018b, MathworksTm Inc., Natick, MA, USA, Win10). The kinematic and EMG data were cut from the start to the end of the events and time-normalized to 101 data points. The first and last repetitions are then removed, and the remaining repetitions are averaged. Therefore, 10 repetitions for each condition were included to calculate the mean trajectories of the hip in the sagittal plane.
Following the biomechanical assessments, the exoskeleton design was evaluated in terms of subjective perception, user acceptance, and usability. Participants were invited to share their overall impressions, focusing on aspects such as the perceived effectiveness of lifting assistance, localized discomfort, and ease of size adjustment while wearing the system.
3.4. Statistical Analysis
To analyze the continuous one-dimensional biomechanical data, a statistical parametric mapping (SPM1d) analysis was conducted using the open-source software package from www.spm1D.org within MATLAB. This method allows for a detailed statistical comparison of time-series data, ensuring a comprehensive evaluation of biomechanical differences.
Following the approach described by Pataky [24], a paired t-test was performed to compare the conditions with and without the exoskeleton. This test assesses whether significant differences exist across the entire time series. The null hypothesis—stating that no difference exists between the conditions—was rejected if the computed SPM{t} value exceeded the critical threshold. Significant differences are visually represented by gray-shaded areas in the statistical test results table. All statistical comparisons were performed with SPM1d using a significance level of α = 0.05.
4. Results
This section presents the outcomes of the biomechanical evaluation, including the kinematic and EMG Data of the assisted and unassisted conditions, as well as the subjective user experience.
4.1. Kinematic Data
The mean kinematic trajectories of the hip and knee joints in the sagittal and frontal planes are depicted on the left side of Figure 5, Figure 6 and Figure 7. The baseline kinematics without the exoskeleton are represented by the blue curve, while the red curve illustrates the kinematics when wearing the exoskeleton. The motion sequence begins in an upright position, followed by grasping the object, and concludes once the object is placed on the platform, returning to an upright posture.

Figure 5.
(a) Mean sagittal hip angle during lifting task with (red) and without (blue) exoskeleton and (b) statistical 1D SPM test; * critical t-value.
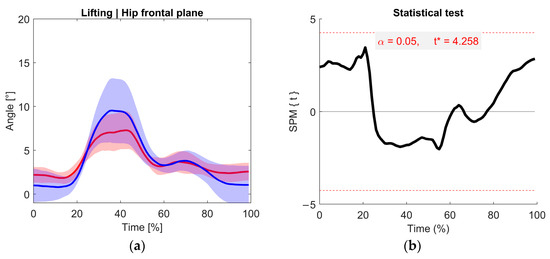
Figure 6.
(a) Mean frontal hip angle during lifting task with (red) and without (blue) exoskeleton and (b) statistical 1D SPM test; * critical t-value.
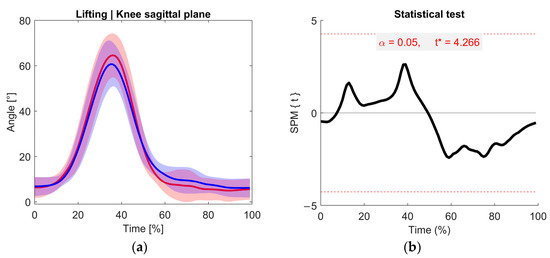
Figure 7.
(a) Mean sagittal knee angle during lifting task with (red) and without (blue) exoskeleton and (b) statistical 1D SPM test; * critical t-value.
During the grasping phase, the hip joint flexes up to approximately 100 degrees (Figure 5). As the object was lifted, the flexion angle decreased to around 25°. When bending forward again to place the object onto the platform, the hip joint reaches a more flexed position of about 35 degrees. Following this, the participants return to an upright position, completing the movement sequence.
The corresponding statistical analysis is shown on the right side of Figure 5. The SPM{t} curve (black) is displayed alongside the critical threshold (red, dashed line). If the SPM{t} value exceeds the critical value, statistically significant differences are observed. However, as indicated in the figure, no significant differences were found between the two conditions (with and without exoskeleton) across the entire movement cycle. This suggests that the exoskeleton does not fundamentally alter hip joint kinematics in the sagittal plane during the lifting task.
Figure 6 illustrates the hip angle in the frontal plane. During the descent to grasp the object, the hip moves into greater abduction, reaching approximately 10 degrees. When using the exoskeleton, the abduction angle is reduced by 2–3 degrees compared to the baseline condition. However, this reduction is not statistically significant. As the participant returns to an upright position and lifts the object onto the platform, the hip angle returns to a neutral posture of approximately 0 degrees. Throughout the entire movement cycle, no statistically significant differences between the conditions were observed, as shown on the right side of the following figure.
In Figure 7, the knee angle in the sagittal plane is shown. When bending forward to grasp an object, knee flexion increases to approximately 65°. During the lifting phase, as the upper body straightens, the knee angle extends back to around 5° in an upright position. No significant differences in knee flexion were observed between the conditions with and without the exoskeleton. As shown on the left side of the following figure, the knee follows a similar flexion-extension pattern in both conditions, indicating that the exoskeleton does not impose movement restrictions or alter the knee kinematics during the lifting task.
4.2. EMG Data
The mean EMG data of the m. erector spinae and m. semitendinosus muscles are depicted in Figure 8 and Figure 9, respectively. As the motion capture and EMG systems were synchronized, the lifting cycle of the EMG data was equivalent to the percentage time of the kinematics data. Likewise, the blue curve corresponds to the baseline condition, and the red curve corresponds to the repetitions with the exoskeleton.
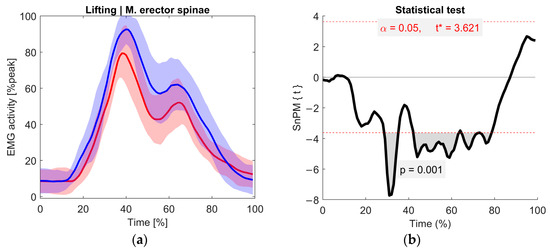
Figure 8.
(a) Mean activity of m. erector spinae during lifting task with (red) and without (blue) exoskeleton and (b) paired-samples t-test statistic SPM {t}; * critical t-value.
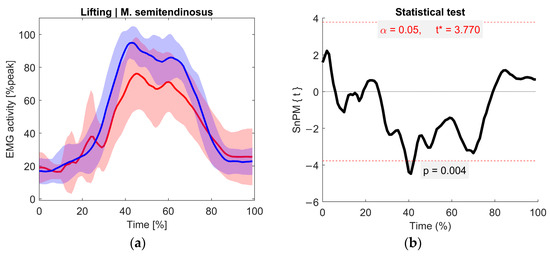
Figure 9.
(a) Mean activity of m. semitendinosus during the lifting task with (red) and without (blue) exoskeleton and (b) paired-samples t-test statistic SPM {t}; * critical t-value.
Throughout the lifting task, two distinct peaks in the muscle activation of the m. erector spinae can be observed. The first peak, occurring at approximately 40% of the movement cycle, corresponds to the increased strain on the back muscles when lifting the weight from the ground. The second peak represents the subsequent muscle effort required when bending forward to place the weight on the platform.
When comparing the conditions with and without the exoskeleton, higher muscle activation is visually noticeable without the exoskeleton between 18% and 85% of the movement cycle. The maximum reduction in muscle activation when using the exoskeleton occurs at 38% of the motion cycle, with a recorded decrease of 15.82 ± 13.35%.
The corresponding statistical test results are illustrated on the right side of Figure 8. A significant difference in muscle activation is evident between 25% and 80% of the movement cycle, except for a short, non-significant phase, around 40%. During this moment, the participant grasped the object and initiated the uplift motion.
The EMG data of the m. semitendinosus are shown in Figure 9. A reduction in muscle activation can be observed during the load phase from 30 to 80% of the movement cycle. Due to the high variability in muscle activation, a statistically significant difference was observed only at approximately 40%, with a peak reduction of 19.89 ± 20.84%. This section corresponds to the initial phase of lifting weights from the ground. This phase coincides with a gap in the significance test for the m. erector spinae, suggesting a temporary shift in support from the lower back muscles to the posterior thigh muscles during the task.
4.3. User Feedback
Overall, the participants indicated that the exoskeleton was straightforward to operate and offered a high level of comfort during use. They noted that soft textile components at the user-system interfaces effectively minimized the risk of pressure points, allowing for a non-restrictive fit throughout the movement.
The system can be applied and removed independently by the user in less than three minutes without the need for external assistance. The adjustable design of the hip belt and supporting structure was particularly appreciated, resembling a backpack configuration with the use of straps, buckles, and Velcro closures. This self-adjustment feature ensured that the exoskeleton could be tailored to different body shapes and sizes without any complications. Additionally, the lightweight design was not perceived as a burden, and joint flexibility ensured unrestricted movement, including walking, lateral bending, and forward bending.
Regarding usability, the participants praised the simple and intuitive operation of the system, noting that only an On/Off switch was required to start the assistive function. However, during lifting tasks, some users felt that the dynamic response of the assistive force was slightly delayed when performing rapid movements. A few test participants suggested that a more adaptive or responsive control system could further enhance the experience, particularly when handling rapid or repetitive lifting sequences.
Overall, the participants described the experience of working with the exoskeleton as “natural” and supportive, emphasizing that it felt like an extension of their own body rather than an external device. Many expressed interest in using the exoskeleton in real-world applications, particularly in occupations involving repetitive lifting tasks, as they experienced a notable reduction in lower back strain.
5. Discussion
The findings are interpreted and discussed in relation to the research objectives, with a particular focus on the exoskeleton’s supportive function, user experience, and implications for future development and application.
5.1. Exoskeleton Design
The purpose of this design approach was to develop an exoskeleton that physically supports care workers during lifting tasks. Therefore, the design was tailored to the needs of healthcare professionals, considering the physical demands of their daily tasks. The priority was to create a lightweight and compact system that could be worn close to the body without restricting natural movements. This requirement aligns with the findings of previous studies (e.g., [25]), which emphasized that wearing comfort is a critical factor for the acceptance of exoskeletons. To ensure high wearing comfort, the exoskeleton was primarily constructed using flexible textile materials. Textile-based designs have been increasingly explored in exoskeleton research [26] because they allow better adaptability to different body shapes and reduce pressure points. In our design, textiles were used at human-system interfaces to ensure optimal comfort and fit. This contrasts with rigid exoskeletons, which tend to cause discomfort when worn for extended periods of time [27,28].
The exoskeleton utilizes a cable-driven force transmission system, which enables the efficient transfer of actuation forces from electric motors to the human body. In this design, cables are wound around spools and tensioned by actuators, thereby generating assistive forces that support the user during lifting tasks. This cable-driven approach is commonly used in soft exosuits (e.g., [29,30]) due to its ability to transmit forces over a distance while allowing for a more compact and lightweight actuator placement. A key advantage of cable-driven systems is their flexibility, which allows actuators to be positioned away from the joints, thereby reducing local bulkiness and maintaining user mobility. Compared to rigid linkages, cable-driven systems offer a more compliant interaction with the human body, which is particularly beneficial in applications requiring comfort and adaptability, such as healthcare exoskeletons. However, cable-driven transmission also presents challenges. One issue is the compression forces that arise in the opposite direction of the tensile force. These undesired forces must be absorbed either by the exoskeleton structure or redirected away from the user’s body to prevent discomfort or instability. Furthermore, friction and backlash effects can reduce the efficiency of force transmission, leading to delays in the response time and potential energy losses [31,32]. To mitigate these drawbacks, low-friction sheaths can be used to guide the cables, and optimized control algorithms can help compensate for transmission delays. Rigid components, such as plastic and aluminum elements, were strategically integrated for force transmission. These materials enable efficient force transfer without a significant increase in weight. Similar hybrid designs have been employed in other soft exosuits [33], demonstrating that the combination of soft and rigid structures can effectively balance comfort and functionality.
While the current design offers high usability and comfort, there is still room for further improvement. One key area is dynamic adaptability, where future iterations could integrate real-time motion adaptation algorithms based on AI-driven movement prediction. This enhances the responsiveness of the assistive force, allowing for more seamless support during lifting tasks. Some users reported a slight delay in the system response, particularly during fast movements. This reduced responsiveness can be attributed to the system’s structural composition, which primarily relies on soft and textile materials. While these materials ensure comfort and adaptability, they also introduce flexibility, leading to shifts in human−technology interfaces and causing minor delays in force transmission. As a result, the overall acceleration and speed capabilities of the exoskeleton were affected. Although this aspect was not a major concern for all participants, it represents a relevant functional limitation that requires further research. Future developments should aim to reduce this latency through both hardware optimizations, such as components with reduced flexibility while maintaining ergonomic design, and improved control algorithms capable of predictive force modulation. Additionally, the use of actuators with higher acceleration and speed characteristics can significantly reduce the perceived delay. Replacing the current motor with a drive system optimized for dynamic response would allow the exoskeleton to adapt more rapidly to sudden changes in user movement, thereby improving the overall support performance during faster movements and dynamic high-load scenarios.
Therefore, the actuator represents another limiting factor, operating near the lower threshold of the required torque and angular velocity. Future improvements in actuation could not only increase the system’s responsiveness but also enhance the user experience by integrating more compact and quieter actuators, making the exoskeleton less noticeable in quiet work environments such as hospitals. Another important aspect is material optimization, where the integration of advanced lightweight composites can help reduce the overall weight while maintaining the necessary structural integrity.
The exoskeleton was originally designed for healthcare professionals, but its use can be expanded to other physically demanding jobs. Possible applications include logistics, warehouse work, and personal caregiving at home. Adapting this technology to these fields would allow a broader range of users to benefit from its support.
5.2. Influence on Kinematics and Muscle Activity
The biomechanical evaluation of the exoskeleton focused on its effect on the muscle activity of the m. erector spinae during a lifting task and its impact on hip and knee joint kinematics. The results indicate a 14% reduction in muscle activity when using the exoskeleton compared to the baseline condition without support. This reduction suggests that the exoskeleton effectively offloads the lower back muscles, potentially lowering the risk of muscle fatigue and long-term strain-related injury. Such a reduction is particularly relevant for healthcare workers who frequently perform physically demanding tasks, such as lifting and repositioning patients, which expose them to a high risk of low back pain and musculoskeletal disorders [34]. Other exoskeletons designed for caregiving support have shown similar results [35,36]. Greater reductions in lumbar muscle activity have also been reported depending on different exoskeleton designs and actuation methods [7,37].
The combined weight of the participants and the lifted load likely contributed to a lower reduction in musculoskeletal strain than initially calculated in the design requirements, which aimed for 30% relief. The required actuator force was calculated based on the gravitational forces of the individual body segments involved in the lifting motion. However, only 30% of the required force was considered in the exoskeleton design to provide supportive assistance. It is important to note that the applied actuator force does not directly translate into an equivalent reduction in muscle activity, as the biomechanical effects depend not only on the external supportive force but also on the complex interactions between active and passive musculoskeletal structures [38,39]. The discrepancy between the calculated force and measured muscle activity reduction highlights the importance of comprehensive biomechanical evaluations to assess the actual unloading effect and optimize the system performance across different users and task conditions.
Interestingly, the analysis of hip and knee flexion in the sagittal plane showed no significant difference between the conditions with and without the exoskeleton. This suggests that the device does not restrict movement patterns and allows the wearer to maintain their typical lifting technique regarding the analyzed degrees of freedom. From a design perspective, this is a positive outcome as it confirms that the exoskeleton aligns with the user’s motions without introducing unwanted compensatory movements that could lead to discomfort or other musculoskeletal issues. Other exoskeletons have shown reductions in the knee and hip range of motion, as well as reduced trunk flexion during the lifting phase [7].
However, as this study was conducted with a relatively homogeneous and small sample size of only 10 participants, the generalizability of the findings is limited, particularly in the context of clinical applications. While initial insights into biomechanical effects and user acceptance could be obtained, the sample size restricts the statistical power of the analysis and may not capture the variability present in broader or more diverse populations. This limitation is especially relevant when considering clinical populations, which may differ substantially in terms of physical condition, age, or motor capabilities. To address this, future research should include a larger number of participants across different demographic groups and use cases, including individuals with musculoskeletal or neurological impairments. Such studies would allow subgroup analyses and a better understanding of how user characteristics influence device interaction. Additionally, longitudinal studies could provide valuable information on learning effects, long-term usability, and user adherence over time. Moreover, different lifting conditions, such as higher loads, repetitive lifting tasks, and asymmetric lifting, should be tested to evaluate the exoskeleton’s effectiveness across various real-world scenarios.
In addition to increasing the number of test participants, future research should incorporate additional biomechanical and physiological measures, such as muscle fatigue analysis (via EMG median frequency), metabolic cost measurements, and subjective workload assessments (e.g., Borg scale). These metrics would provide a more comprehensive understanding of how exoskeletons affect long-term usability, user comfort, and fatigue resistance. Especially during repetitive lifting tasks, monitoring changes in EMG signal characteristics or oxygen consumption over time could help identify whether the system reduces physical strain or delays fatigue onset. Furthermore, metabolic data, such as heart rate or respiratory exchange ratio, could serve as valuable indicators of overall energy efficiency during assisted vs. unassisted conditions. Kinematic analyses beyond the hip joint—such as lumbar spine motion—could further reveal how the exoskeleton interacts with whole-body movement patterns. Furthermore, future studies should evaluate long-term user acceptance in real-world healthcare environments and explore the impact of exoskeleton-assisted lifting on musculoskeletal health.
6. Conclusions
In conclusion, we presented the design of a lightweight exoskeleton to support the back muscles during lifting tasks. The initial results demonstrate the potential of the exoskeleton to reduce lower back muscle strain without restricting movement, making it a promising solution for occupational lifting tasks in healthcare and other physically demanding professions. Future studies are essential for optimizing the design, functionality, and long-term impact of the device, ensuring that it provides effective and user-friendly assistance in various workplace environments.
Author Contributions
Conceptualization and methodology, T.S. and R.W.; investigation, T.S.; writing—original draft preparation, T.S.; writing—review and editing, T.S. and R.W.; visualization, T.S.; and supervision, R.W. All authors have read and agreed to the published version of this manuscript.
Funding
This research was funded by dtec.bw—Digitalization and Technology Research Center of the Bundeswehr [project KIKU]. Dtec.bw is funded by the European Union—Next Generation EU.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Department of Psychology of the Helmut−Schmidt University. 2024_011. 29.08.24.
Informed Consent Statement
Informed consent was obtained from all the participants involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Acknowledgments
The authors created a fully articulated text version. This fully articulated text was reviewed by ChatGPT-4o for clarity while keeping all citations and links. The edited output of ChatGPT was then again reviewed and edited by the authors. ChatGPT was not used to generate the text. The authors would like to thank Maik Thiel from Texthiel Design and Rebekka Jochem for their support in manufacturing the textile components and smart textile user interface.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Krishnan, K.S.; Raju, G.; Shawkataly, O. Prevalence of Work-Related Musculoskeletal Disorders: Psychological and Physical Risk Factors. Int. J. Environ. Res. Public Health 2021, 18, 9361. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.G.; Kotowski, S.E. Prevalence of Musculoskeletal Disorders for Nurses in Hospitals, Long-Term Care Facilities, and Home Health Care: A Comprehensive Review. Hum. Factors 2015, 57, 754–792. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; McNoe, B.; Derrett, S.; Harcombe, H. Interventions to prevent and reduce the impact of musculoskeletal injuries among nurses: A systematic review. Int. J. Nurs. Stud. 2018, 82, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Theurel, J.; Desbrosses, K. Occupational Exoskeletons: Overview of Their Benefits and Limitations in Preventing Work-Related Musculoskeletal Disorders. IISE Trans. Occup. Ergon. Hum. Factors 2019, 7, 264–280. [Google Scholar] [CrossRef]
- Karafillidis, A.; Weidner, R. Developing Support Technologies; Springer International Publishing: Cham, Switzerland, 2018; ISBN 978-3-030-01835-1. [Google Scholar]
- Farah, L.; Roll, D.; Sorais, A.; Vallée, A. Assessment of Exoskeletons on Nurses’ Quality of Work Life: A Pilot Study at Foch Hospital. Nurs. Rep. 2023, 13, 780–791. [Google Scholar] [CrossRef]
- Reimeir, B.; Calisti, M.; Mittermeier, R.; Ralfs, L.; Weidner, R. Effects of back-support exoskeletons with different functional mechanisms on trunk muscle activity and kinematics. Wearable Technol. 2023, 4, e12. [Google Scholar] [CrossRef]
- Koopman, A.S.; Näf, M.; Baltrusch, S.J.; Kingma, I.; Rodriguez-Guerrero, C.; Babič, J.; de Looze, M.P.; van Dieën, J.H. Biomechanical evaluation of a new passive back support exoskeleton. J. Biomech. 2020, 105, 109795. [Google Scholar] [CrossRef]
- Nourollahi, M.; Afshari, D.; Dianat, I. Awkward trunk postures and their relationship with low back pain in hospital nurses. Work 2018, 59, 317–323. [Google Scholar] [CrossRef]
- Liang, F.; Mo, L.; Sun, Y.; Guo, C.; Gao, F.; Liao, W.-H.; Cao, J.; Li, B.; Song, Z.; Wang, D.; et al. Interlimb and Intralimb Synergy Modeling for Lower Limb Assistive Devices: Modeling Methods and Feature Selection. Cyborg Bionic Syst. 2024, 5, 122. [Google Scholar] [CrossRef]
- Ali, A.; Fontanari, V.; Schmoelz, W.; Agrawal, S.K. Systematic Review of Back-Support Exoskeletons and Soft Robotic Suits. Front. Bioeng. Biotechnol. 2021, 9, 765257. [Google Scholar] [CrossRef]
- Ralfs, L.; Hoffmann, N.; Weidner, R. Approach of a Decision Support Matrix for the Implementation of Exoskeletons in Industrial Workplaces. In Annals of Scientific Society for Assembly, Handling and Industrial Robotics 2021; Schüppstuhl, T., Ed.; Springer International Publishing AG: Cham, Switzerland, 2022; pp. 165–176. ISBN 978-3-030-74031-3. [Google Scholar]
- Inoue, Y.; Kuroda, Y.; Yamanoi, Y.; Yabuki, Y.; Yokoi, H. Development of Wrist Separated Exoskeleton Socket of Myoelectric Prosthesis Hand for Symbrachydactyly. Cyborg Bionic Syst. 2024, 5, 141. [Google Scholar] [CrossRef]
- Morris, L.; Diteesawat, R.S.; Rahman, N.; Turton, A.; Cramp, M.; Rossiter, J. The-state-of-the-art of soft robotics to assist mobility: A review of physiotherapist and patient identified limitations of current lower-limb exoskeletons and the potential soft-robotic solutions. J. Neuroeng. Rehabil. 2023, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Preethichandra, D.M.G.; Piyathilaka, L.; Sul, J.-H.; Izhar, U.; Samarasinghe, R.; Arachchige, S.D.; de Silva, L.C. Passive and Active Exoskeleton Solutions: Sensors, Actuators, Applications, and Recent Trends. Sensors 2024, 24, 7095. [Google Scholar] [CrossRef] [PubMed]
- Ott, O.; Ralfs, L.; Weidner, R. Framework for qualifying exoskeletons as adaptive support technology. Front. Robot. AI 2022, 9, 951382. [Google Scholar] [CrossRef]
- Neťuková, S.; Bejtic, M.; Malá, C.; Horáková, L.; Kutílek, P.; Kauler, J.; Krupička, R. Lower Limb Exoskeleton Sensors: State-of-the-Art. Sensors 2022, 22, 9091. [Google Scholar] [CrossRef]
- Rayssiguie, E.; Erden, M.S. A Review of Exoskeletons Considering Nurses. Sensors 2022, 22, 7035. [Google Scholar] [CrossRef]
- Turja, T.; Saurio, R.; Katila, J.; Hennala, L.; Pekkarinen, S.; Melkas, H. Intention to Use Exoskeletons in Geriatric Care Work: Need for Ergonomic and Social Design. Ergon. Des. 2020, 30, 106480462096157. [Google Scholar] [CrossRef]
- Grieve, D.W.; Pheasant, S.T. Biomechanics. In The Body at Work: Biological Ergonomics; Singleton, W.T., Ed.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 1982; pp. 71–161. ISBN 0521240875. [Google Scholar]
- Jang, R.; Karwowski, W.; Quesada, P.M.; Rodrick, D.; Sherehiy, B.; Cronin, S.N.; Layer, J.K. Biomechanical evaluation of nursing tasks in a hospital setting. Ergonomics 2007, 50, 1835–1855. [Google Scholar] [CrossRef]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef]
- Sorbie, G.G.; Williams, M.J.; Boyle, D.W.; Gray, A.; Brouner, J.; Gibson, N.; Baker, J.S.; Easton, C.; Ugbolue, U.C. Intra-session and Inter-day Reliability of the Myon 320 Electromyography System During Sub-maximal Contractions. Front. Physiol. 2018, 9, 309. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Engin. 2012, 15, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Elprama, S.A.; Vanderborght, B.; Jacobs, A. An industrial exoskeleton user acceptance framework based on a literature review of empirical studies. Appl. Ergon. 2022, 100, 103615. [Google Scholar] [CrossRef] [PubMed]
- Bardi, E.; Gandolla, M.; Braghin, F.; Resta, F.; Pedrocchi, A.L.G.; Ambrosini, E. Upper limb soft robotic wearable devices: A systematic review. J. Neuroeng. Rehabil. 2022, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhou, D.; Leng, Y. A Systematic Review on Rigid Exoskeleton Robot Design for Wearing Comfort: Joint Self-Alignment, Attachment Interface, and Structure Customization. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 3815–3827. [Google Scholar] [CrossRef]
- Bosch, T.; van Eck, J.; Knitel, K.; de Looze, M. The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Appl. Ergon. 2016, 54, 212–217. [Google Scholar] [CrossRef]
- Zhong, B.; Shen, M.; Liu, H.; Zhao, Y.; Qian, Q.; Wang, W.; Yu, H.; Zhang, M. A Cable-Driven Exoskeleton With Personalized Assistance Improves the Gait Metrics of People in Subacute Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 2560–2569. [Google Scholar] [CrossRef]
- Guo, S.; Zheng, T.; Ju, H.; Zhao, J.; Zhu, Y. Development of a Cable-Driven Upper Limb Exosuit for Both Pulling and Lifting. In Proceedings of the 2024 10th International Conference on Mechatronics and Robotics Engineering, ICMRE 2024, Milan, Italy, 27–29 February 2024; Maciolek, W., Ed.; IEEE: Piscataway, NJ, USA, 2024; pp. 120–124, ISBN 979-8-3503-9427-6. [Google Scholar]
- Xiloyannis, M.; Chiaradia, D.; Frisoli, A.; Masia, L. Physiological and kinematic effects of a soft exosuit on arm movements. J. Neuroeng. Rehabil. 2019, 16, 29. [Google Scholar] [CrossRef]
- Cappello, L.; Binh, D.K.; Yen, S.-C.; Masia, L. Design and preliminary characterization of a soft wearable exoskeleton for upper limb. In Proceedings of the 6th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), UTown, Singapore, 26–29 June 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 623–630, ISBN 978-1-5090-3287-7. [Google Scholar]
- Hussain, F.; Goecke, R.; Mohammadian, M. Exoskeleton robots for lower limb assistance: A review of materials, actuation, and manufacturing methods. Proc. Inst. Mech. Eng. H 2021, 235, 1375–1385. [Google Scholar] [CrossRef]
- Aleid, A.A.; Eid Elshnawie, H.A.; Ammar, A. Assessing the Work Activities Related to Musculoskeletal Disorder among Critical Care Nurses. Crit. Care Res. Pract. 2021, 2021, 8896806. [Google Scholar] [CrossRef]
- von Glinski, A.; Yilmaz, E.; Mrotzek, S.; Marek, E.; Jettkant, B.; Brinkemper, A.; Fisahn, C.; Schildhauer, T.A.; Geßmann, J. Effectiveness of an on-body lifting aid (HAL® for care support) to reduce lower back muscle activity during repetitive lifting tasks. J. Clin. Neurosci. 2019, 63, 249–255. [Google Scholar] [CrossRef]
- Hwang, J.; Kumar Yerriboina, V.N.; Ari, H.; Kim, J.H. Effects of passive back-support exoskeletons on physical demands and usability during patient transfer tasks. Appl. Ergon. 2021, 93, 103373. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Linnenberg, C.; Weidner, R.; Wulfsberg, J. Development of A Soft Power Suit for Lower Back Assistance. In Proceedings of the 2019 International Conference on Robotics and Automation (ICRA), Montreal, QC, Canada, 20–24 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 5103–5109, ISBN 978-1-5386-6027-0. [Google Scholar]
- Fanti, V.; Sanguineti, V.; Caldwell, D.G.; Ortiz, J.; Di Natali, C. Assessment methodology for human-exoskeleton interactions: Kinetic analysis based on muscle activation. Front. Neurorobot. 2022, 16, 982950. [Google Scholar] [CrossRef]
- Missiroli, F.; Lotti, N.; Xiloyannis, M.; Sloot, L.H.; Riener, R.; Masia, L. Relationship Between Muscular Activity and Assistance Magnitude for a Myoelectric Model Based Controlled Exosuit. Front. Robot. AI 2020, 7, 595844. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).