
Selecting Anterior Segmental Osteotomy Versus Orthodontic Camouflage Treatment: Importance of the Incisor–Mandibular Plane Angle



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Variables
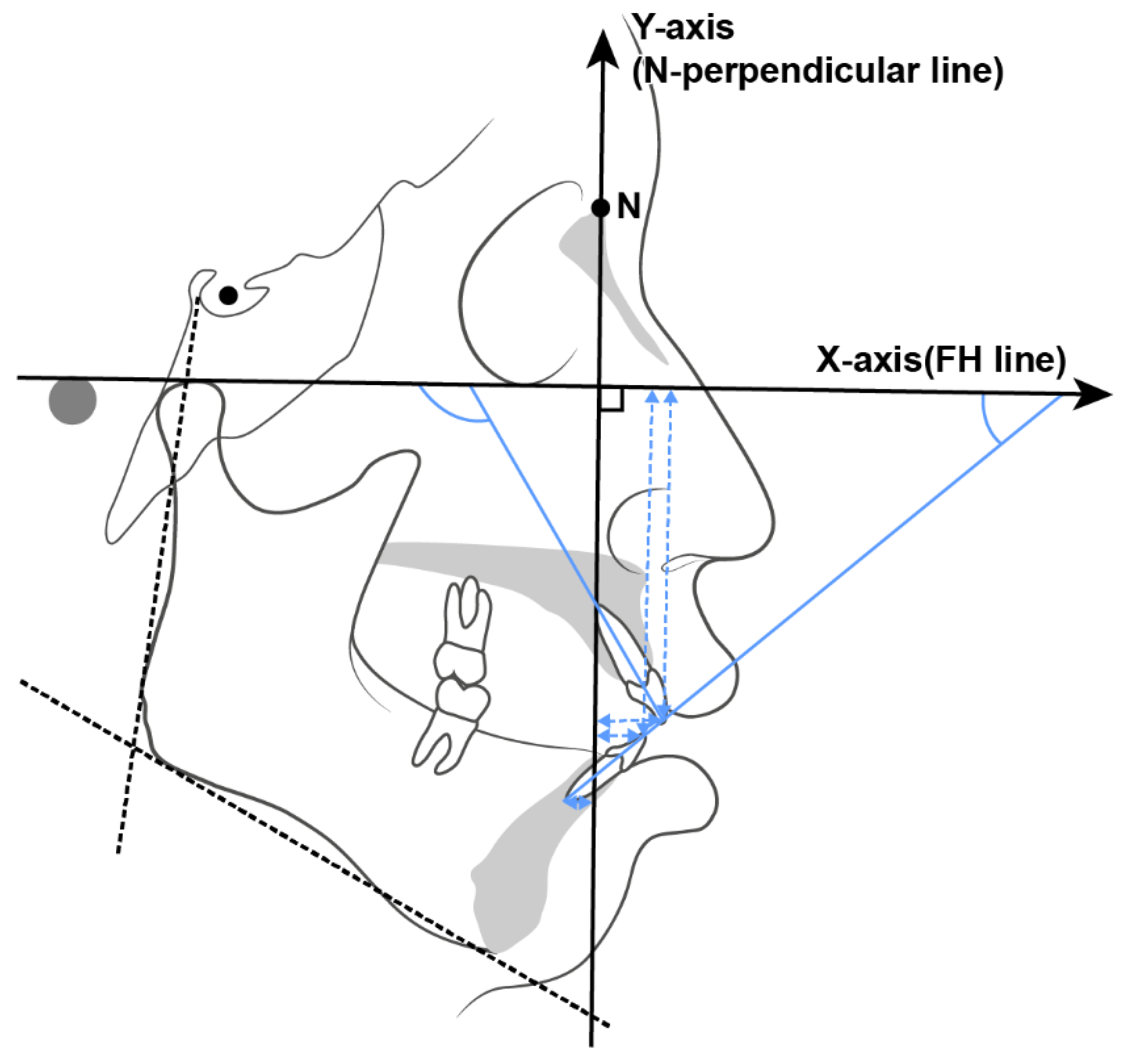
Cephalometric Measurement (Table 2)

{kind=link}
{kind=link}
{kind=link}
| Explanation | |
|---|---|
| Skeletal Measurements | |
| SNA (°) | Angle of nasion–sella to nasion–A point |
| SNB (°) | Angle of nasion–sella to nasion–B point |
| ANB (°) | Angle of A point–nasion to nasion–B point |
| FMA (°) | Angle of Frankfort horizontal plane (FH) and the mandibular plane |
| SN–GoMe (°) | Angle of sella–nasion to gonion–menton |
| A to N-perp (mm) | Distance between A point and N-perpendicular |
| B to N-perp (mm) | Distance between B point and N-perpendicular |
| Pog to N-perp (mm) | Distance between Pogonion point and N-perpendicular |
| A to FH (mm) | Distance between A point and FH plane |
| B to FH (mm) | Distance between B point and FH plane |
| FABA (°) | Angle of Frankfort horizontal plane (FH) to AB plane |
| Dental measurements | |
| U1 to FH (°) | Angle of FH to U1 axis |
| U1 to FH (mm) | Distances between U1 tip and FH |
| L1 to FH (°) | Angle of FH to L1 axis |
| L1 to FH (mm) | Distance between L1 tip and FH |
| U1 C_N-perp (mm) | Distance between U1 tip and N-perpendicular |
| U1 R_N-perp (mm) | Distance between U1 apex and N-perpendicular |
| L1 C_N-perp (mm) | Distance between L1 tip and N-perpendicular |
| L1 R_N-perp (mm) | Distance between L1 apex and N-perpendicular |
| FOP (Functional occlusal plane) | Angle of FH to line joins the midpoint of U6 and L6 with the midpoint of upper and lower premolars |
| BOP (Bisected occlusal plane) | Angle of FH to line that bisects the vertical distance between the upper and lower incisal tips (U1 tip, L1 tip) and the upper and lower first molar occlusal surface (U6 occlusal, L6 occlusal) |
| Interincisal angle (°) | Angle of U1 axis to L1 axis |
2.3. Data Collection Techniques
2.3.1. Surgical Procedures
2.3.2. TAD Placement Procedures
2.4. Data Analyses
3. Results
3.1. Pretreatment Comparison Between the ASO and NASO Groups (Table 3)
3.1.1. Skeletal Differences Before Treatment
| ASO Group | Non-ASO Group | |||||
|---|---|---|---|---|---|---|
| Measurements | Mean | SD | Mean | SD | Difference | p |
| SNA | 82.17 | 4.16 | 79.85 | 3.07 | 2.31 | 0.01 ** |
| SNB | 76.69 | 4.01 | 76.08 | 3.12 | 0.60 | 0.49 |
| ANB | 5.48 | 1.13 | 3.77 | 1.41 | 1.71 | 0.00 ** |
| FMA | 29.51 | 6.03 | 29.22 | 4.46 | 0.29 | 0.82 |
| SN-GoMe | 38.13 | 6.47 | 39.47 | 4.84 | −1.34 | 0.35 |
| A to N-perp | 0.87 | 3.13 | 0.11 | 2.91 | 0.76 | 0.31 |
| A to FH | 35.77 | 3.35 | 34.65 | 4.22 | 1.11 | 0.24 |
| B to N-perp | −9.35 | 5.78 | −6.67 | 4.89 | −2.68 | 0.04 * |
| B to FH | 72.85 | 6.58 | 73.16 | 6.47 | 9.69 | 0.00 |
| Pog to N-perp | −10.41 | 6.80 | −8.84 | 5.94 | −1.56 | 0.32 |
| FABA | 77.79 | 3.64 | 80.13 | 3.80 | −2.33 | 0.01 * |
| U1 to FH (°) | 114.81 | 6.50 | 116.51 | 6.58 | −1.70 | 0.29 |
| U1 to FH (mm) | 63.50 | 4.17 | 57.50 | 5.87 | 6.00 | 0.00 ** |
| L1 to FH (°) | 45.68 | 4.84 | 51.83 | 7.23 | −6.15 | 0.00 ** |
| L1 to FH (mm) | 61.31 | 4.11 | 55.89 | 5.36 | 5.42 | 0.00 ** |
| U1 C to N-perp | 8.52 | 4.95 | 6.24 | 4.24 | 2.28 | 0.046 * |
| U1 R to N-perp | −2.99 | 3.99 | −4.19 | 2.93 | 1.20 | 0.16 |
| L1 C to N-perp | 5.16 | 4.89 | 2.87 | 4.17 | 2.29 | 0.04 * |
| L1 R to N-perp | −10.77 | 5.81 | −9.49 | 4.31 | −1.27 | 0.31 |
| Interincisal angle | 110.87 | 7.70 | 115.32 | 10.70 | −4.45 | 0.053 |
| BOP | 11.19 | 3.04 | 10.30 | 3.58 | 0.89 | 0.28 |
| FOP | 11.74 | 3.50 | 11.43 | 4.07 | 0.31 | 0.74 |
| IMPA | 104.81 | 6.95 | 98.94 | 7.46 | 5.87 | 0.00 ** |
3.1.2. Dental Differences Before Treatment
3.2. Post-Treatment Comparison Between the ASO and NASO Groups (Table 4)
3.2.1. Post-Treatment Skeletal Differences
| ASO Group | Non-ASO Group | |||||
|---|---|---|---|---|---|---|
| Measurements | Mean | SD | Mean | SD | Difference | p |
| SNA | 78.04 | 4.14 | 79.15 | 3.32 | −1.11 | 0.23 |
| SNB | 74.82 | 3.92 | 75.88 | 2.98 | −1.05 | 0.22 |
| ANB | 3.22 | 1.22 | 3.28 | 1.37 | −0.06 | 0.85 |
| FMA | 28.79 | 3.84 | 28.46 | 4.42 | 0.33 | 0.75 |
| SN-GoMe | 37.33 | 4.65 | 38.67 | 4.95 | −1.34 | 0.26 |
| A to N-perp | −3.86 | 2.76 | −0.72 | 2.78 | −3.13 | 0.00 ** |
| A to FH | 34.22 | 3.47 | 35.30 | 4.16 | −1.09 | 0.13 |
| B to N-perp | −13.10 | 5.29 | −7.05 | 4.36 | −6.06 | 0.00 ** |
| B to FH | 82.57 | 5.94 | 72.98 | 6.80 | 9.59 | 0.00 ** |
| Pog to N-perp | −11.13 | 5.80 | −8.16 | 5.52 | −2.97 | 0.04 * |
| FABA | 79.15 | 3.67 | 80.50 | 3.60 | −1.34 | 0.14 |
| U1 to FH (°) | 110.31 | 6.06 | 110.00 | 7.53 | 0.31 | 0.86 |
| U1 to FH (mm) | 62.90 | 4.42 | 57.26 | 5.60 | 5.65 | 0.00 ** |
| L1 to FH (°) | 51.86 | 6.34 | 62.99 | 7.97 | −11.13 | 0.00 ** |
| L1 to FH (mm) | 60.23 | 4.34 | 55.08 | 5.67 | 5.14 | 0.00 ** |
| U1 C to N-perp | 1.95 | 4.66 | 2.13 | 3.86 | −0.18 | 0.86 |
| U1 R to N-perp | −7.58 | 3.81 | −5.64 | 3.00 | −1.93 | 0.02 * |
| L1 C to N-perp | −1.16 | 4.75 | −1.00 | 3.75 | −0.16 | 0.88 |
| L1 R to N-perp | −15.23 | 5.36 | −9.71 | 4.27 | −5.52 | 0.00 ** |
| Interincisal angle | 121.56 | 9.49 | 132.99 | 11.88 | −11.44 | 0.00 ** |
| BOP | 12.17 | 3.69 | 10.88 | 4.09 | 1.29 | 0.18 |
| FOP | 12.29 | 3.87 | 10.68 | 4.67 | 1.61 | 0.13 |
| IMPA | 99.34 | 7.39 | 88.54 | 7.54 | 10.80 | 0.00 ** |
3.2.2. Dental Differences Post-Treatment
3.3. Comparison of Pre- and Post-Treatment Changes in the ASO and NASO Groups (Table 5)
| (T1–T0) | (Δ ASO Group–Δ NASO Group) | ||||
|---|---|---|---|---|---|
| Measurements | ΔASO Mean | Δ NASO Mean | Mean Difference | SD Difference | p |
| SNA diff | −4.13 | −0.70 | −3.43 | 0.34 | 0.00 ** |
| SNB diff | −1.87 | −0.21 | −1.66 | 0.23 | 0.00 ** |
| ANB diff | −2.26 | −0.49 | −1.77 | 0.35 | 0.00 ** |
| FMA diff | −0.72 | −0.76 | 0.04 | 0.94 | 0.48 |
| SN-GoMe diff | −0.80 | −0.80 | 0.00 | 0.91 | 0.50 |
| A to N-perp diff | −4.73 | −0.84 | −3.89 | 0.48 | 0.00 ** |
| A to FH diff | −1.55 | 0.65 | −2.20 | 0.46 | 0.00 ** |
| B to N-perp diff | −3.76 | −0.38 | −3.38 | 0.62 | 0.00 ** |
| B to FH diff | −0.29 | −0.18 | −0.11 | 0.64 | 0.43 |
| Pog to N-perp diff | −0.73 | 0.68 | −1.41 | 0.83 | 0.048 * |
| FABA diff | 1.36 | 0.37 | 0.99 | 0.66 | 0.07 |
| U1 to FH (°) diff | −4.50 | −6.51 | 2.01 | 1.49 | 0.09 * |
| U1 to FH (mm) diff | −0.60 | −0.24 | −0.36 | 0.56 | 0.27 |
| L1 to FH (°) diff | 6.18 | 11.16 | −4.98 | 1.83 | 0.00 ** |
| L1 to FH (mm) diff | −1.08 | −0.81 | −0.27 | 0.55 | 0.31 |
| U1 C to N-perp diff | −6.57 | −4.11 | −2.46 | 0.79 | 0.00 ** |
| U1 R to N-perp diff | −4.58 | −1.45 | −3.14 | 0.53 | 0.00 ** |
| L1 C to N-perp diff | −6.31 | −3.87 | −2.44 | 0.75 | 0.00 ** |
| L1 R to N-perp diff | −4.47 | −0.22 | −4.25 | 0.60 | 0.00 ** |
| Interincisal angle diff | 10.69 | 17.67 | −6.98 | 2.71 | 0.01 ** |
| BOP diff | 0.98 | 0.58 | 0.40 | 0.58 | 0.25 |
| FOP diff | 0.54 | −0.76 | 1.30 | 0.82 | 0.06 |
| U1 movement diff | 6.76 | 5.80 | 0.97 | 0.62 | 0.06 |
| L1 movement diff | 6.59 | 5.55 | 1.04 | 0.60 | 0.04 * |
| IMPA diff | −5.46 | −10.40 | 4.93 | 2.12 | 0.01 * |
3.3.1. Skeletal Changes Pre- and Post-Treatment
3.3.2. Dental Changes Pre- and Post-Treatment
3.3.3. Borderline Cases After Treatment Comparison (Supplementary Table S1)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farrow, A.L.; Zarrinnia, K.; Azizi, K. Bimaxillary protrusion in black Americans—An esthetic evaluation and the treatment considerations. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Jayaratne, Y.S.; Zwahlen, R.A.; Lo, J.; Cheung, L.K. Facial soft tissue response to anterior segmental osteotomies: A systematic review. Int. J. Oral Maxillofac. Surg. 2010, 39, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.H.; Kim, B.H. Determinants of successful treatment of bimaxillary protrusion: Orthodontic treatment versus anterior segmental osteotomy. J. Craniofacial Surg. 2005, 16, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.G.; Mills, P.B.; Brenner, L.D. Maxillary and mandibular subapical osteotomies for the correction of anterior open-bite. Oral Surg. Oral Med. Oral Pathol. 1967, 23, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Chung, K.R.; Baek, S.H. Treatment outcomes of orthodontic treatment, corticotomy-assisted orthodontic treatment, and anterior segmental osteotomy for bimaxillary dentoalveolar protrusion. Plast. Reconstr. Surg. 2007, 120, 1027–1036. [Google Scholar] [CrossRef] [PubMed]
- Hwang, B.Y.; Choi, B.J.; Lee, B.S.; Kwon, Y.D.; Lee, J.W.; Jung, J.; Ohe, J.Y. Comparison between anterior segmental osteotomy versus conventional orthodontic treatment in root resorption: A radiographic study using cone-beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 34. [Google Scholar] [CrossRef] [PubMed]
- Yong, C.; Sng, T.; Quah, B.; Lee, C.; Lim, A.; Wong, R. The role of anterior segmental osteotomies in orthognathic surgery for protrusive faces in a Southeast Asian population: 10-year retrospective data of 51 patients treated in a single centre. Int. J. Oral Maxillofac. Surg. 2023, 52, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Tweed, C.H. The Frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am. J. Orthod. Oral Surg. 1946, 32, 175–230. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lim, S.-W.; Chan, V.; Hong, P.; Han, S.-B.; Chae, H.S. The surgical outcomes of anterior segmental osteotomy in Asian skeletal class II patients. Oral Maxillofac. Surg. 2024, 28, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.C.; Burstone, C.J. Soft-tissue profile--fallacies of hard-tissue standards in treatment planning. Am. J. Orthod. Dentofac. Orthop. 1986, 90, 52–62. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A., Jr. A method of cephalometric evaluation. Am. J. Orthod. 1984, 86, 449–469. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, J.L.; Proffit, W.R.; Sarver, D.M. The emerging soft tissue paradigm in orthodontic diagnosis and treatment planning. Clin. Orthod. Res. 1999, 2, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.T. Cephalometric soft tissue facial analysis. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Clérigues, M.; Montiel-Company, J.-M.; Almerich-Silla, J.-M.; García-Sanz, V.; Paredes-Gallardo, V.; Bellot-Arcís, C. Changes in the alveolar bone thickness of maxillary incisors after orthodontic treatment involving extractions—A systematic review and meta-analysis. J. Clin. Exp. Dent. 2019, 11, e76. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.-W.; Moon, S.C.; Baek, S.-H. Morphometric evaluation of changes in the alveolar bone and roots of the maxillary anterior teeth before and after en masse retraction using cone-beam computed tomography. Angle Orthod. 2013, 83, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-J.; Ge, Z.-P.; Ma, R.-H.; Hou, J.-X.; Li, G. A six-site method for the evaluation of periodontal bone loss in cone-beam CT images. Dentomaxillofac. Radiol. 2016, 45, 20150265. [Google Scholar] [CrossRef] [PubMed]
- Son, E.J.; Kim, S.J.; Hong, C.; Chan, V.; Sim, H.Y.; Ji, S.; Hong, S.Y.; Baik, U.B.; Shin, J.W.; Kim, Y.H.; et al. A study on the morphologic change of palatal alveolar bone shape after intrusion and retraction of maxillary incisors. Sci. Rep. 2020, 10, 14454. [Google Scholar] [CrossRef] [PubMed]
- Sarikaya, S.; Haydar, B.; Ciǧer, S.; Ariyürek, M. Changes in alveolar bone thickness due to retraction of anterior teeth. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 15–26. [Google Scholar] [CrossRef] [PubMed]


| ASO | SD | Non-ASO | SD | p-Value | ||
|---|---|---|---|---|---|---|
| Categorical | Male | 9 | 9 | 0.924 | ||
| Female | 22 | 27 | 0.924 | |||
| Extraction (U4s/U5s) | 28/2 | 24/12 | 0.02 * | |||
| Numeric | Age (y) | 36.8 | 7.5 | 31.43 | 4.3 | 0.04 * |
| ANB (deg) | 5.48 | 1.13 | 3.77 | 1.41 | 0.00 ** | |
| ANB range | 3.14 < ASO < 7.15 | 3.1 < NASO < 4.49 | ||||
| SN-GoMe (deg) | 38.13 | 6.47 | 39.65 | 4.22 | 0.24 | |
| U1 to FH (deg) | 114.81 | 6.5 | 116.51 | 6.58 | 0.29 | |
| IMPA (deg) | 104.81 | 6.95 | 98.94 | 7.46 | 0.00 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, P.; Kim, Y.H.; Choo, H.; Choi, Y.-J.; Chae, H.S. Selecting Anterior Segmental Osteotomy Versus Orthodontic Camouflage Treatment: Importance of the Incisor–Mandibular Plane Angle. Appl. Sci. 2025, 15, 4849. https://doi.org/10.3390/app15094849
Hong P, Kim YH, Choo H, Choi Y-J, Chae HS. Selecting Anterior Segmental Osteotomy Versus Orthodontic Camouflage Treatment: Importance of the Incisor–Mandibular Plane Angle. Applied Sciences. 2025; 15(9):4849. https://doi.org/10.3390/app15094849
Chicago/Turabian StyleHong, Pureum, Young Ho Kim, Hyunhee Choo, Young-Jin Choi, and Hwa Sung Chae. 2025. "Selecting Anterior Segmental Osteotomy Versus Orthodontic Camouflage Treatment: Importance of the Incisor–Mandibular Plane Angle" Applied Sciences 15, no. 9: 4849. https://doi.org/10.3390/app15094849
APA StyleHong, P., Kim, Y. H., Choo, H., Choi, Y.-J., & Chae, H. S. (2025). Selecting Anterior Segmental Osteotomy Versus Orthodontic Camouflage Treatment: Importance of the Incisor–Mandibular Plane Angle. Applied Sciences, 15(9), 4849. https://doi.org/10.3390/app15094849