Abstract
Background: Impacted canines can adversely affect adjacent structures, particularly lateral incisors. The purpose was to determine the correlation between upper lateral incisor dimension and angular and linear positioning of upper impacted canines. Methods: The sample comprised 50 impacted canines, evaluated using cone-beam computed tomography (CBCT). Measurements included crown dimensions of lateral incisors and impacted canines, incisor root length, and the distance from the canine cusp to the occlusal plane. Angular positions of the canine were measured relative to the occlusal plane, facial midline, and palatine suture. Pearson correlations tested associations between canine position, lateral incisor dimensions, and maxillary transverse width. Results: Significant morphological differences for impacted canines and lateral incisors were found based on canine position and impaction type (unilateral or bilateral). A positive correlation was observed between lateral incisor crown size and canine cusp distance to the occlusal plane (r = +0.483, p < 0.001). Conversely, a negative correlation was noted between lateral incisor root length and canine angulation relative to the palatal suture (r = −0.356, p = 0.022). Conclusions: Impacted canine position is associated with changes in canine and lateral incisor dimensions, potentially affecting their alignment and root integrity. Correlations were also found between maxillary width, incisor morphology, and canine position.
1. Introduction
The occurrence of impacted maxillary canines has been reported to range from 1.6% to 4.7% [1].
Upper canines play very important roles and are key to facial aesthetics, as well as to the development of occlusion [2,3,4,5,6] and the dental arch. For this reason, this tooth is often referred to as the cornerstone of the dental arch [7,8].
Eruption is a complex process, and it can occur early, late, or even fail to take place. When the eruption period for the teeth is surpassed, they are considered impacted [9,10].
Despite extensive research, the precise etiology of canine impaction remains elusive [11]. Several etiological factors have been proposed—local, systemic, or genetic—with the latter currently considered the most influential. Zilberman et al. [12] emphasized the genetic theory. According to their study, there is a strong genetic influence on the development of maxillary canine impaction and the associated dental anomalies.
Rutledge et al. [13] emphasized a local etiology, attributing impaction to the agenesis of the ipsilateral lateral incisor [14]. These authors also describe a familial tendency, even suggesting the presence of a single gene. Palatally displaced canines have been identified as an autosomal dominant trait with low penetrance and variable expressivity [15,16]. Thus, the etiology of impacted canines is complex, likely influenced by both genetic and environmental factors, with variable presentation.
The most common localized factor is the discrepancy between arch length and tooth size [9,17]. Another local factor is the high position of the canines within the maxillary arch, as well as microdontia of the lateral incisors [15,18,19,20]. Other contributing factors may include the retention of primary canines, crowding in the upper arch, odontomas, and ankylosis of the maxillary canines [2,21].
Early detection of impacted canines significantly influences the success of their management and aids in the prevention of related complications [22], such as root resorption in neighboring teeth [2,23].
The diagnosis and localization of impacted canines are carried out through clinical and radiographic examination [2]. Clinical diagnosis is typically one of suspicion and requires radiographic confirmation in order to accurately assess the impaction. Until recently, conventional two-dimensional (2D) radiographic imaging—particularly panoramic radiographs—was commonly used for the localization of impacted canines, as well as for treatment planning and post-treatment outcome evaluation.
We can find that much of the existing research has scrutinized the form, dimensions, and structural characteristics of the lateral incisor relating to maxillary canine impaction [24,25,26,27,28,29,30], but little attention has been paid to its connection to the root of the lateral incisor [25,28]. One possible explanation for this gap in literature could be the reliance on two-dimensional radiographs for quantifying incisor root inclination.
With the advent and growing use of three-dimensional imaging modalities, we now have the ability to assess the tilt of the upper incisor root and its volumetric characteristics concerning impacted canine [31]. This advancement shows promise for improving our comprehension of the etiology of tooth impaction. Furthermore, in this way, neighboring anatomical structures and their relationships in the three spatial planes can be evaluated, allowing for the detection of possible dental anomalies [32].
The aim of this project was to assess the relationship between the spatial positioning of the ectopic maxillary canine and the dimensions of the adjacent lateral incisor and canine, as evaluated using 3D cone beam imaging. Additionally, the study aimed to investigate the prevalence of occurrence of resorption in the adjacent lateral incisor.
The null hypothesis was that there was no statistically significant relationship between the spatial positioning of the ectopic maxillary canine and the dimensions of the adjacent lateral incisor and canine.
2. Materials and Methods
2.1. Study Design and Subjects
This is an analytical, observational, cross-sectional study. The sample was consecutively selected from patients attending the Orthodontic Clinical Department of the Complutense University of Madrid (UCM).
Informed consent was obtained from all patients and their legal guardians or parents to undergo 3D radiographic examination and for the utilization of the material for research purposes. The inclusion criteria comprised: (1) presence of maxillary impacted canine, (2) presence of ipsilateral upper lateral incisor, (3) patients in permanent dentition at V vertebral stage of growth, (4) Caucasian ethnicity, and (5) patients with non-severe malocclusions requiring orthognathic surgery. Exclusion criteria encompassed: (1) cone-beam computed tomographies (CBCTs) obtained from external radiological centers, (2) patients diagnosed with syndromes associated with dental inclusions or syndromes affecting bone metabolism, (3) patients who have been administered medication affecting bone metabolism, (4) agenesis or absence of upper incisors, canines, premolars, and/or first molars, and (5) patients who underwent previous orthodontic treatment. The study protocol obtained approval from the UCM Research Ethics Board (REB) with reference ID 33-231120.
This study is a continuation of a previous investigation that evaluated the transverse dimensions of the maxillary hemiarches in patients with impacted upper canines. In that earlier work, the sample size was calculated based on the study by Cacciatore et al. [33], using an alpha level of 0.05 and a beta level of 0.10 to achieve 90% power for detecting intragroup differences. Based on this calculation, a total of 46 canines was required. Ultimately, data from 50 impacted canines (from 37 patients) were collected. The maxillary canine was considered the unit of analysis, since in cases of bilateral impaction, each canine was treated as an independent and unrelated entity.
2.2. Radiographic Outcomes
All radiographic evaluations, including CBCT and orthopantomography (OPG) analyses, as well as measurements, were conducted by the same investigator.
All images were acquired with patients in a standing position using a consistent machine (Planmeca ProMax 3D CBCT; Planmeca OY, AsentaJankatu 6, Helsinki, Finland). Subsequently, DICOM (“Digital Imaging and Communication in Medicine”) records were transferred into the HorosTM platform (Horos Project, Annapolis, MD, USA) to orient the images.
Within the CBCT, the subsequent factors associated with the morphology of the impacted canines and ipsilateral lateral incisors were recorded:
- Mesiodistal diameter on the coronal section of the canine crown (MD3) (Figure 1).
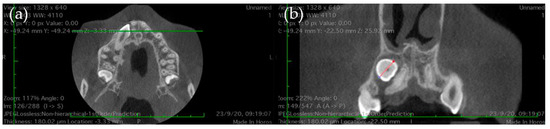 Figure 1. Canine crown mesiodistal diameter: (a) Orientation of the transverse axis in maximum mesiodistal contour (MD) of the canine crown. (b) MD3: coronal mesio-distal diameter of the canine.
Figure 1. Canine crown mesiodistal diameter: (a) Orientation of the transverse axis in maximum mesiodistal contour (MD) of the canine crown. (b) MD3: coronal mesio-distal diameter of the canine.
- Occlusogingival (OG3) and buccolingual crown length (BL3) of the canine (Figure 2).
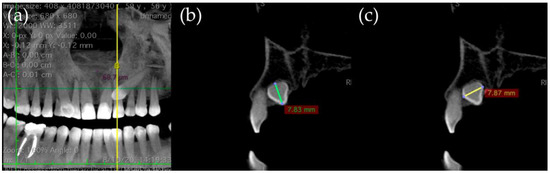 Figure 2. Canine crown occluso-gingival and bucco-lingual diameter: (a) Orientation of the longitudinal axis. (b) OG3: occluso-gingival coronal length of canine. (c) BL3: coronal bucco-lingual diameter of the canine.
Figure 2. Canine crown occluso-gingival and bucco-lingual diameter: (a) Orientation of the longitudinal axis. (b) OG3: occluso-gingival coronal length of canine. (c) BL3: coronal bucco-lingual diameter of the canine.
- Length of the lateral incisor´s root (LongRad2), and occlusogingival (OG2) and buccolingual crown length (BL2) (Figure 3).
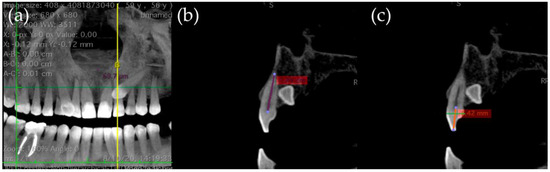 Figure 3. Lateral incisor measurements: (a) Orientation of the longitudinal axis. (b) LongRad2: root length of lateral incisor. (c) OG2: occluso-gingival length of lateral incisor and BL2: lateral incisor coronal bucco-lingual diameter.
Figure 3. Lateral incisor measurements: (a) Orientation of the longitudinal axis. (b) LongRad2: root length of lateral incisor. (c) OG2: occluso-gingival length of lateral incisor and BL2: lateral incisor coronal bucco-lingual diameter.
- Mesiodistal crown diameter of the lateral incisor (MD2) (Figure 4).
 Figure 4. Transverse diameter: (a) MD2: mesio-distal coronal diameter of the lateral incisor. (b) Transv4: maxillary width of the palatal cusp of the right first premolar to the left first premolar. (c) Transv6: maxillary width of mesiopalatine cusp from right first molar to left first molar.
Figure 4. Transverse diameter: (a) MD2: mesio-distal coronal diameter of the lateral incisor. (b) Transv4: maxillary width of the palatal cusp of the right first premolar to the left first premolar. (c) Transv6: maxillary width of mesiopalatine cusp from right first molar to left first molar. - The width across the maxillary arch was measured as follows:
- Transverse distance between the palatal cusps of upper first premolars (1.4 and 2.4 teeth) (Transv4).
- Transverse distance between mesiopalatine cusps of upper first molars (1.6 and 2.6 teeth) (Transv6) (Figure 4).
External root resorption of the upper lateral incisor was evaluated on sagittal and axial CBCT slices, defined as clear substance loss on the root surface. It was recorded as a dichotomous outcome, noted as ‘Yes’ (1) or ‘No’ (0).
The primary dependent variables included angular and linear measures of the canine position, which were as follows:
- The angle formed between the canine´s longitudinal axis and the occlusal plane passing through the cusps of the first molar and premolars (Ang3Poe).
- Angle connecting the canine´s longitudinal axis and the midline, observed in the frontal plane (Ang3LMf).
- Angle among the longitudinal alignment of the canine and the palatal suture, noted in the transverse plane (Ang3LMt).
- Linear measurement of the distance between the canine cusp and the occlusal plane (in millimeters) along the sagittal plane (DCPo) (Figure 5).
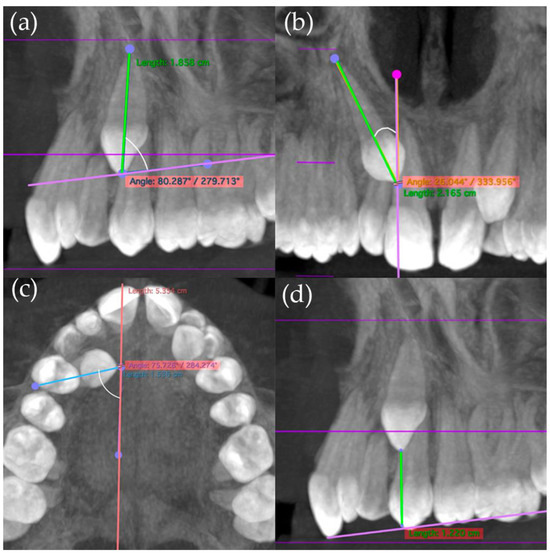 Figure 5. Canine angular and linear measurements: (a) Ang3Poe: angle of the canine with respect to the occlusal plane. (b) Ang3LMf: angle of the canine with respect to the palatal suture. (c) Ang3LMt: angle of the canine in relation to the midline. (d) DCPo: distance from the canine cusp to the occlusal plane.
Figure 5. Canine angular and linear measurements: (a) Ang3Poe: angle of the canine with respect to the occlusal plane. (b) Ang3LMf: angle of the canine with respect to the palatal suture. (c) Ang3LMt: angle of the canine in relation to the midline. (d) DCPo: distance from the canine cusp to the occlusal plane.
On the OPGs obtained from CBCTs, the following measures were taken:
- Mesiodistal position of the cusp tip of the canine according to Ericson and Kurol [34,35]. The described five sectors are defined by the longitudinal axes of the permanent central and lateral incisors and parallel lines passing through the contact points between the central incisors, the lateral and central incisors, and the mesial and distal surfaces of the deciduous canines. Sector 1 represents the most distal position, while Sector 5 corresponds to the most mesial location [36].
- Angulation of the long axis of the upper canine relative to the central line (Ang3LMfP).
2.3. Statistical Analysis:
Patient data were organized in an Excel Data Sheet 16.41 Mac (Microsoft Corporation, Redmond, WA, United States) and then transferred to the Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM Corp, Armonk, NY, United States) for analysis.
Categorical variables were compared using the Chi-square test. Following confirmation of normal data distribution, Student’s t-tests and ANOVA were employed. Subsequently, post hoc tests (Bonferroni correction) were conducted for pairwise comparisons.
The Pearson correlation test was used to explore the association among the canine and lateral incisor dimensions and the angular position of the canine, as well as to examine the relationship between the transverse dimension of the maxilla and the position of the canine. The alpha level was defined at p ≤ 0.05.
3. Results
The same researcher conducted measurements twice in five patients to assess intra-observer reproducibility. The intraclass correlation coefficient ranged from r = 0.92 to r = 0.95, indicating high consistency.
3.1. Patient Characteristics
In this study, the clinical records of 240 consecutive patients with impacted canines treated between 2015 and 2021 were reviewed. After applying the inclusion and exclusion criteria and evaluating the quality of the radiographic records, 37 consecutive patients with 50 impacted canines were included, based on the previously calculated sample size. Patients were excluded due to ineligibility or poor-quality X-rays or dental casts.
The final sample, assessed using CBCT imaging, included 23 women (62.16%) and 14 men (37.84%), with ages ranging from 10.49 to 56.91 years (mean age: 16.37 years; SD: 7.78 years).
3.2. Canine Bucco-Palatal Position
Significant statistical results (p < 0.05) were observed in the comparison using Student´s t-test based on the buccolingual position for several parameters:
The distance from the canine cusp to the occlusal plane was greater in cases of buccal impactions.
The canine angulation in relation to the occlusal plane was greater in palatal impactions.
Similarly, in relation to the palatal suture, the angulation of the canine was also greater in palatal impactions (Table 1).

Table 1.
Comparison between canine buccal and palatal position.
3.3. Unilateral or Bilateral Inclusion
Linear and angular measurements were also compared depending on unilateral or bilateral inclusion: statistically significant values were found for angulation with respect to the midline in orthopantomography and for maxillary width, both of which were higher in unilateral impactions (Table 2).
Table 2.
Comparison between unilateral or bilateral inclusion.
3.4. Morphology of the Impacted Canines and Ipsilateral Lateral Incisors
Comparisons between unilateral and bilateral impactions revealed statistically significant differences in the occlusogingival length of the canine crown (p = 0.020) and the lateral incisor crown (p = 0.028). Specifically, canine crowns were longer in bilateral impactions, while lateral incisor crowns were longer in unilateral cases. Additionally, a significant difference was found in the mesiodistal width of the lateral incisor crown between unilateral and bilateral impactions, with a mean difference of 0.78 mm (p = 0.010), being larger in unilateral cases.
Regarding the mesiodistal location of the impacted canines, ANOVA revealed significant differences according to the impaction sector. Post hoc tests showed that the occlusogingival length of the canine crown was significantly greater in sector 3 than in sector 1 (p = 0.021). Furthermore, the buccolingual width of the lateral incisor crown was significantly larger in cases with canines in sector 1 compared to those in sector 4 (p = 0.047). Similarly, the occlusogingival length of the lateral incisor crown was greater in sector 1 compared to sector 4 (p = 0.044). In all cases, measurements were greater in sector 1.
3.5. Correlation Between Variables
Correlations between the quantitative variables assessed in the study are detailed in Table 3. Several statistically significant correlations were observed between the dimensions of lateral incisors, canine position, and transverse maxillary widths. A moderate positive correlation was found between mesiodistal crown width of the lateral incisor and the distance from the canine cusp to the occlusal plane (r = 0.483, p < 0.001), while a negative correlation emerged between lateral incisor root length and canine angulation relative to the palatal suture (r = −0.356, p = 0.022). Similarly, the mesiodistal crown width of the lateral incisor was negatively associated with canine angulation relative to the occlusal plane (r = −0.408, p = 0.004) and positively correlated with maxillary width at the premolar level (Transv_4_4) (r = 0.291, p = 0.047).
Table 3.
Correlation between crown measurements of lateral incisors and canines, root lengths of lateral incisors, transverse maxillary widths, and the linear and angular measurements of canine position.
Regarding root dimensions, root length of the lateral incisor showed a strong positive correlation with transverse width at the premolar level (r = 0.487, p = 0.001). The occluso-gingival crown length of the lateral incisor also presented a significant negative correlation with canine angulation relative to the palatal suture (r = −0.446, p = 0.002).
For the canine, its mesiodistal crown width was positively correlated with the distance from the cusp to the occlusal plane (r = 0.319, p = 0.031), and its occluso-gingival crown length showed a significant positive association with transverse premolar width (r = 0.328, p = 0.023) and a negative correlation with canine angulation relative to both the palatal suture (r = −0.455, p = 0.001) and the midline (r = −0.389, p = 0.005).
3.6. Root Resorption
Regarding root resorption in adjacent teeth, 18 lateral incisors (36%) exhibited signs of resorption, with occurrences in 25% of women and 8% of men. However, no significant differences were found (p = 0.227).
4. Discussion
The aim of this project was to determine the relationship between the spatial position of the impacted maxillary canine and the dimensions of the canine and adjacent lateral incisor, as well as to investigate the prevalence of the occurrence of resorption in the neighboring lateral incisor. Additionally, we aimed to examine the potential impact of the upper lateral incisor root on the inclination of the adjacent canine. In the first case, we obtained significant results; a positive correlation (+0.483) was identified between the lateral incisor crown size and the distance of the canine cusp to the bite plane (p < 0.001). Conversely, a negative correlation (−0.356) was noted between the lateral incisor root length and the canine angulation relative to the palatal suture (p = 0.022).
Two etiological factors are believed to cause impacted canines in the palate: genetic predisposition and improper orientation (due to missing or underdeveloped lateral incisors). In contrast, buccally impacted canines are thought to result from the early loss of primary teeth and deficiencies in the dental arch [37]. This fact was not taken into account in our study since all patients were in the permanent dentition.
The orientation theory suggests that bilateral canine impaction is, in many cases, genetically determined [11,38]. Ross et al. [39] observed a higher percentage of bilateral impactions (107 out of 207 cases; 51.69%) and attributed this variation to differences in population samples and ethnic diversity. Studies indicate that Asian populations exhibit fewer bilateral impactions compared to individuals from multiethnic groups outside the United States [40,41,42,43]. The profile of our study population was similar to that of previous studies regarding the buccal or palatal location of the impactions, with 70% being palatal and 30% buccal, and their unilateral or bilateral presence, with 52% being bilateral and 48% unilateral.
However, variations in the prevalence rates reported in the literature may also stem from the use of CBCT scans in different populations, as well as non-standardized assessment tools for identifying impacted canines [44].
Rafflenbeul et al. [45] found that buccal displacement occurred almost as frequently as palatal displacement (38.5% and 41%, respectively), a finding that is uncommon in Caucasian populations [14].
In regard to the methodology used, Ross et al. [39] mentioned that the occlusal plane is not a stable reference plane, as it is of dental origin, and it could complicate comparisons before and after treatment. In their study, they use the palatal plane to quantify the inclination of the canines, as it has a local and skeletal basis [46]. However, since our study uses only initial orthodontic records, the reference of the occlusal plane could be considered as an acceptable reference, validated by other studies [35,36]. Moreover, in our study, we considered not only the occlusal plane but also other reference planes, such as the midline palatal suture.
We noted a longer lateral incisor root and a wider mesiodistal crown diameter in cases with a greater transverse maxillary width. Alshehri et al. [7] showed that altered or increased mesiodistal lateral crown dimensions (MD) could potentially serve as indicators of impacted canines and found that the size of the maxillary skeleton and the width of the dental arch play a crucial role in establishing the configuration and alignment of maxillary canine impaction.
Concerning the type of the impaction, in our study we noted a larger angulation of the canine in cases of unilateral impactions, as well as Dağsuyu et al. [2], which showed notable differences between the right and left upper impacted canines in terms of their angulation with the midline and occlusal plane.
Regarding the inclination angle of the canine, we observed that canines with a greater buccopalatal diameter showed a greater angulation relative to the occlusal plane. In this way, we observed that lateral incisors with a shorter root and crown, as well as a smaller mesiodistal size, presented a greater angulation of the canine in relation to the palatal suture. Similarly, we noted a greater angulation of the canines in reference to the midline in cases where the root and crown length of the lateral incisors was shorter.
Sajnani et al. [47] discovered that the distance from the tip of the canine cusp to the occlusal plane became the strongest predictor of maxillary canine impaction.
In our study, we found that the canines were larger when located in sector 1 compared to the lateral incisor. Alqerban et al. [31] suggested that the angulation of the canine towards the lateral incisor is a key predictor of canine impaction, highlighting the importance of assessing this factor in future research endeavors. Koral et al. [30] concluded that the volume of the lateral incisor, the mesiodistal and buccolingual width of the lateral incisor crown and root, the total length of the lateral incisor, and the lateral incisor angulation to the midline and the axis of the adjacent canine were found to be strong predictors of maxillary canine impaction.
Based on the results, the null hypothesis stating that there is no association between the spatial position of the impacted maxillary canine and the dimensions or resorption of the adjacent lateral incisor was rejected. The findings demonstrated significant associations between canine position and the morphology of adjacent lateral incisors, thereby supporting the alternative hypothesis.
One of the main limitations of this study is its cross-sectional design, which allows for the identification of associations but does not establish causality. This inherent limitation suggests that any relationships observed between the positioning of the maxillary canine and the dimensions of the lateral incisor should be interpreted with caution. Longitudinal studies are necessary to explore causal relationships more thoroughly and to track changes over time.
Additional limitations include the fact that the sample size calculation was done for a different outcome, as this study shows secondary data of a larger project. This may have limited the capacity to obtain statistically significant differences. Further studies are needed to determine the relationship of the maxillary lateral incisor in the impaction of the maxillary canine. There is a potential selection bias, as this is not a random sample. Future studies are needed with a segmentation of the sample by gender in order to eliminate confounding factors.
5. Conclusions
We can conclude that there exists a relationship between the impaction of the maxillary canine and the lateral incisor sizes. Associations were found between the horizontal width of the maxilla and the lateral incisors, as well as the position of the impacted canines.
Statistically significant associations were identified between the position of the canine and its own coronal size. Identifying factors potentially associated with maxillary canine impaction holds significance for predicting impactions and facilitating timely intervention.
Further research with larger samples and longitudinal designs is needed to confirm these findings and better understand the angular and linear relationships observed in CBCT imaging.
Author Contributions
Conceptualization, G.A.-L., E.M.-M., J.M. and C.M.; methodology, C.M.; software, P.F.-P., validation, P.F.-P., G.A.-L. and C.M.; formal analysis, P.F.-P. and C.M.; investigation, P.F.-P. and C.M.; resources, P.F.-P., G.A.-L. and J.M..; data curation, P.F.-P.; writing—original draft preparation, P.F.-P. and C.M.; writing—review and editing, P.F.-P., T.P.-M. and C.M.; visualization, P.F.-P.; supervision, C.M. and T.P.-M.; project administration, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Hospital Clínico San Carlos de Madrid (internal code 33/231120-E_Tesis; date of approval: 18 April 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We would like to thank the BIOCRAN (Craniofacial Biology: Orthodontics and Dentofacial Orthopedics) Research Group, and the Orthodontic Section, Faculty of Odontology, Complutense University of Madrid, for their support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lövgren, M.L.; Dahl, O.; Uribe, P.; Ransjö, M.; Westerlund, A. Prevalence of impacted maxillary canines—An epidemiological study in a region with systematically implemented interceptive treatment. Eur. J. Orthod. 2019, 41, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Dagsuyu, I.M.; Kahraman, F.; Oksayan, R. Three-dimensional evaluation of angular, linear, and resorption features of maxillary impacted canines on cone-beam computed tomography. Oral. Radiol. 2018, 34, 66–72. [Google Scholar] [CrossRef]
- Uribe, P.; Ransjö, M.; Westerlund, A. Clinical predictors of maxillary canine impaction: A novel approach using multivariate analysis. Eur. J. Orthod. 2016, 39, 153–160. [Google Scholar] [CrossRef][Green Version]
- Ali, B.; Shaikh, A.; Fida, M. Association between sella turcica bridging and palatal canine impaction. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Fernández, E.; Bravo, L.A.; Canteras, M. Eruption of the permanent upper canine: A radiologic study. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 414–420. [Google Scholar] [CrossRef]
- Amuk, M.; Gul Amuk, N.; Ozturk, T. Effects of root–cortex relationship, root shape, and impaction side on treatment duration and root resorption of impacted canines. Eur. J. Orthod. 2021, 43, 508–515. [Google Scholar] [CrossRef]
- Alshehri, A.; Hakami, Z.; Marran, K.; Qaysi, A.; Shabi, M.; Bokhari, A. Unilateral vs Bilateral Maxillary Canine Impaction: A Cone-Beam Computed Tomography Study of Patterns and Associations. J. Contemp. Dent. Pract. 2023, 24, 21–28. [Google Scholar] [CrossRef]
- Katz, M.I. Angle classification revisited 2: A modified Angle classification. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 277–284. [Google Scholar] [CrossRef]
- Al-Kyssi, H.A.; Al-Mogahed, N.M.; Altawili, Z.M.; Dahan, F.N.; Almashraqi, A.A.; Aldhorae, K.; Alhammadi, M.S. Predictive factors associated with adjacent teeth root resorption of palatally impacted canines in Arabian population: A cone-beam computed tomography analysis. BMC Oral Health 2022, 22, 220. [Google Scholar] [CrossRef]
- Litsas, G.; Acar, A. A Review of Early Displaced Maxillary Canines: Etiology, Diagnosis and Interceptive Treatment. Open Dent. J. 2011, 5, 39. [Google Scholar] [CrossRef]
- Papageorgiou, S.N.; Seehra, J.; Cobourne, M.T.; Kanavakis, G. Does Current Evidence Support the Discussion Around the Guidance Theory? A Systematic Review and Meta-Analysis on the Association Between Maxillary Lateral Incisor Agenesis and Displacement or Impaction of the Permanent Canine. Orthod. Craniofacial Res. 2025, 28, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Zilberman, Y.; Cohen, B.; Becker, A. Familial trends in palatal canines, anomalous lateral incisors, and related phenomena. Eur. J. Orthod. 1990, 12, 135–139. [Google Scholar] [CrossRef]
- Rutledge, M.S.; Hartsfield, J.K. Genetic Factors in the Etiology of Palatally Displaced Canines. Semin. Orthod. 2010, 16, 165–171. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L.; Kataja, M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994, 64, 250–256. [Google Scholar] [CrossRef]
- Becker, A.; Peck, S.; Peck, L.; Kataja, M. Palatal canine displacement: Guidance theory or an anomaly of genetic origin? A letter to the editor from Adrian Becker, with a response from Sheldon and Leena Peck, and Matti Kataja. Angle Orthod. 1995, 65, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Liuk, I.W.; Olive, R.J.; Griffin, M.; Monsour, P. Associations between palatally displaced canines and maxillary lateral incisors. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 622–632. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Asiri, H.A.; Almashraqi, A.A. Incidence, severity and orthodontic treatment difficulty index of impacted canines in Saudi population. J. Clin. Exp. Dent. 2018, 10, e327–e334. [Google Scholar] [CrossRef]
- Bishara, S.E.; Ortho, D. Impacted maxillary canines: A review. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 159–171. [Google Scholar] [CrossRef]
- Martinez Madero, E.; García Montarelo, J.; Aguayo, G.S.; Martin, C. Comparison between Digital Casts and Cone Beam Computed Tomography for Measuring Maxillary Transverse Dimensions in Patients with Impacted Canines. Children 2022, 9, 278. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L.; Kataja, M. Concomitant occurrence of canine malposition and tooth agenesis: Evidence of orofacial genetic fields. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 657–660. [Google Scholar] [CrossRef]
- da Silva Santos, L.M.; Bastos, L.C.; Oliveira-Santos, C.; da Silva, S.J.A.; Neves, F.S.; Campos, P.S.F. Cone-beam computed tomography findings of impacted upper canines. Imaging Sci. Dent. 2014, 44, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Stabryła, J.; Zadurska, M.; Plakwicz, P.; Kukuła, K.T.; Czochrowska, E.M. Comparisons of Dental Anomalies in Orthodontic Patients with Impacted Maxillary and Mandibular Canines. Diagnostics 2023, 13, 2766. [Google Scholar] [CrossRef] [PubMed]
- Bianco, E.; Mirabelli, L.; Basilicata, M.; Bruno, G.; De Stefani, A.; Du, L.; Maddalone, M. Cone Beam Computed Tomography (CBCT) Aid in the Management of Apical Root Resorption of Impacted Maxillary Canines and Physiologically Erupted Maxillary Canines after Orthodontic Treatment. Appl. Sci. 2024, 14, 886. [Google Scholar] [CrossRef]
- Sobhani, F.; Miresmaeili, A.; Mahjub, H.; Farhadian, M. Statistical shape analysis of maxillary palatal morphology in patients with palatally displaced canines. BMC Med. Imaging 2023, 23, 198. [Google Scholar] [CrossRef]
- Light, N.; Chaushu, S.; Major, P.W.; Flores-Mir, C. 3D Analysis of maxillary incisor root inclinations in cases of unilateral maxillary canine impaction. Eur. J. Orthod. 2022, 44, 396–403. [Google Scholar] [CrossRef]
- Pereira, P.M.; Ferreira, A.P.; Tavares, P.; Braga, A.C. Different Manifestations of Class II Division 2 Incisor Retroclination and their Association with Dental Anomalies. J. Orthod. 2013, 40, 299–306. [Google Scholar] [CrossRef]
- Lüdicke, G.; Harzer, W.; Tausche, E. Incisor Inclination—Risk Factor for Palatally-impacted Canines. J. Orofac. Orthop. Fortschritte Kieferorthop. 2008, 69, 357–364. [Google Scholar] [CrossRef]
- Dekel, E.; Nucci, L.; Weill, T.; Flores-Mir, C.; Becker, A.; Perillo, L.; Chaushu, S. Impaction of maxillary canines and its effect on the position of adjacent teeth and canine development: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e135–e147. [Google Scholar] [CrossRef]
- Oliveira, T.C.P.d.; Copello, F.M.; Paes-Souza, S.d.A.; Castro, A.C.R.d.; Nojima, L.I.; Gonçalves Nojima, M.d.C. Influence of the maxillary dimensions and lateral incisor anatomy on the palatal impaction of maxillary permanent canines: A three-dimensional case-control study. Int. Orthod. 2023, 21, 100804. [Google Scholar] [CrossRef]
- Koral, S.; Arman Özçırpıcı, A.; Tunçer, N. Association Between Impacted Maxillary Canines and Adjacent Lateral Incisors: A Retrospective Study with Cone Beam Computed Tomography. Turk. J. Orthod. 2021, 34, 207–213. [Google Scholar] [CrossRef]
- Alqerban, A.; Jacobs, R.; Fieuws, S.; Willems, G. Radiographic predictors for maxillary canine impaction. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 345–354. [Google Scholar] [CrossRef]
- Eslami, E.; Barkhordar, H.; Abramovitch, K.; Kim, J.; Masoud, M.I. Cone-beam computed tomography vs conventional radiography in visualization of maxillary impacted-canine localization: A systematic review of comparative studies. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, G.; Poletti, L.; Sforza, C. Early diagnosed impacted maxillary canines and the morphology of the maxilla: A three-dimensional study. Prog. Orthod. 2018, 19, 20. [Google Scholar] [CrossRef]
- Ericson, S.; Kurol, J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur. J. Orthod. 1988, 10, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Ericson, S.; Kurol, J. Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur. J. Orthod. 1986, 8, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Ericson, S.; Kurol, J. Resorption of maxillary lateral incisors caused by ectopic eruption of the canines: A clinical and radiographic analysis of predisposing factors. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 503–513. [Google Scholar] [CrossRef]
- Yan, B.; Sun, Z.; Fields, H.; Wang, L.; Luo, L. Etiologic factors for buccal and palatal maxillary canine impaction: A perspective based on cone-beam computed tomography analyses. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 527–534. [Google Scholar] [CrossRef]
- Becker, A.; Chaushu, S. Etiology of maxillary canine impaction: A review. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 557–567. [Google Scholar] [CrossRef]
- Ross, G.; Abu Arqub, S.; Mehta, S.; Vishwanath, M.; Tadinada, A.; Yadav, S.; Upadhyay, M. Estimating the 3-D location of impacted maxillary canines: A CBCT-based analysis of severity of impaction. Orthod. Craniofacial Res. 2023, 26, 81–90. [Google Scholar] [CrossRef]
- Liu, D.-G.; Zhang, W.-L.; Zhang, Z.-Y.; Wu, Y.-T.; Ma, X.-C. Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 91–98. [Google Scholar] [CrossRef]
- Becker, A.; Chaushu, S. Long-term follow-up of severely resorbed maxillary incisors after resolution of an etiologically associated impacted canine. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 650–654. [Google Scholar] [CrossRef]
- Almuhtaseb, E.; Mao, J.; Mahony, D.; Bader, R.; Zhang, Z.-X. Three-dimensional localization of impacted canines and root resorption assessment using cone beam computed tomography. J. Huazhong Univ. Sci. Technol. Med. Sci. 2014, 34, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.; Liang, H.; Benson, B.; Flint, D.; Cho, B. The assessment of impacted maxillary canine position with panoramic radiography and cone beam CT. Dentomaxillofac. Radiol. 2014, 41, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Alyami, B.; Braimah, R.; Alharieth, S. Prevalence and pattern of impacted canines in Najran, South Western Saudi Arabian population. Saudi Dent. J. 2020, 32, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Rafflenbeul, F.; Gros, C.-I.; Lefebvre, F.; Bahi-Gross, S.; Maizeray, R.; Bolender, Y. Prevalence and risk factors of root resorption of adjacent teeth in maxillary canine impaction, among untreated children and adolescents. Eur. J. Orthod. 2018, 41, 447–453. [Google Scholar] [CrossRef]
- Schmidt, A.D.; Kokich, V.G. Periodontal response to early uncovering, autonomous eruption, and orthodontic alignment of palatally impacted maxillary canines. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 449–455. [Google Scholar] [CrossRef]
- Sajnani, A.K.; King, N.M. Early prediction of maxillary canine impaction from panoramic radiographs. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 45–51. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).