
The Effectiveness of Story- and Quiz-Based Games in Digital Interventions for ADHD: A Comparative Approach


Abstract
1. Introduction
2. Materials and Methods
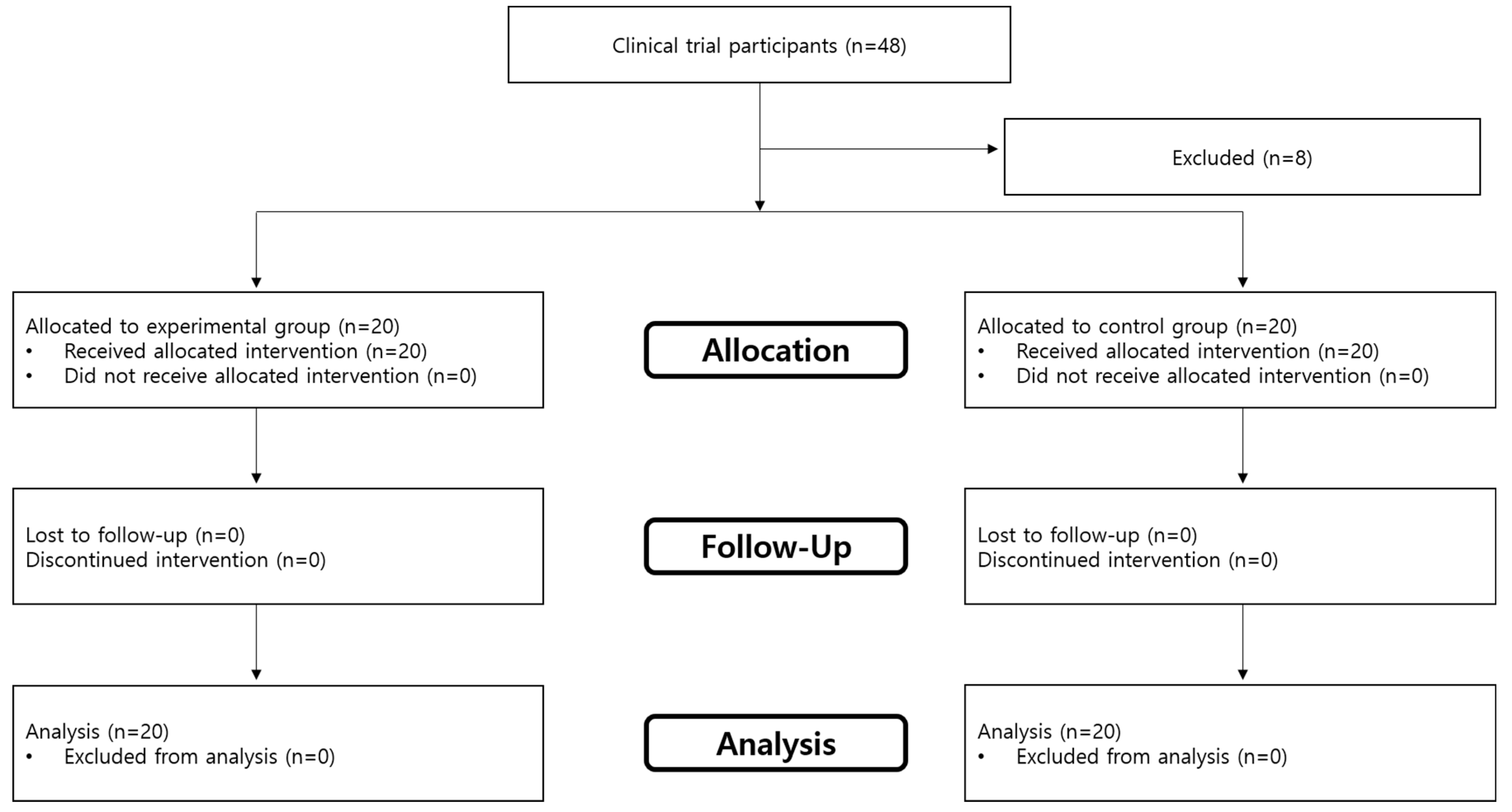
2.1. Study Participants
2.2. Experimental Methods
2.3. Duration of Study
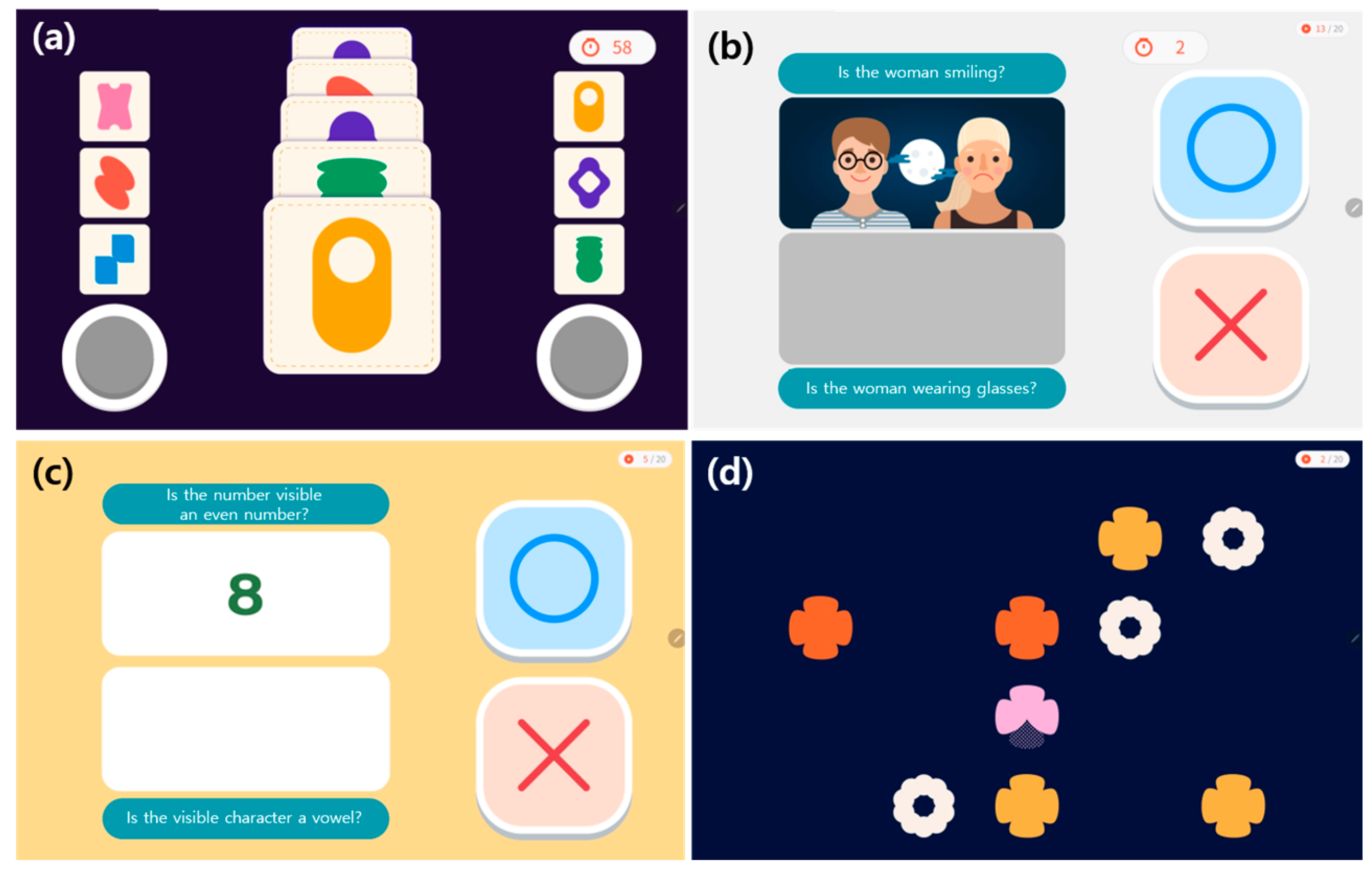
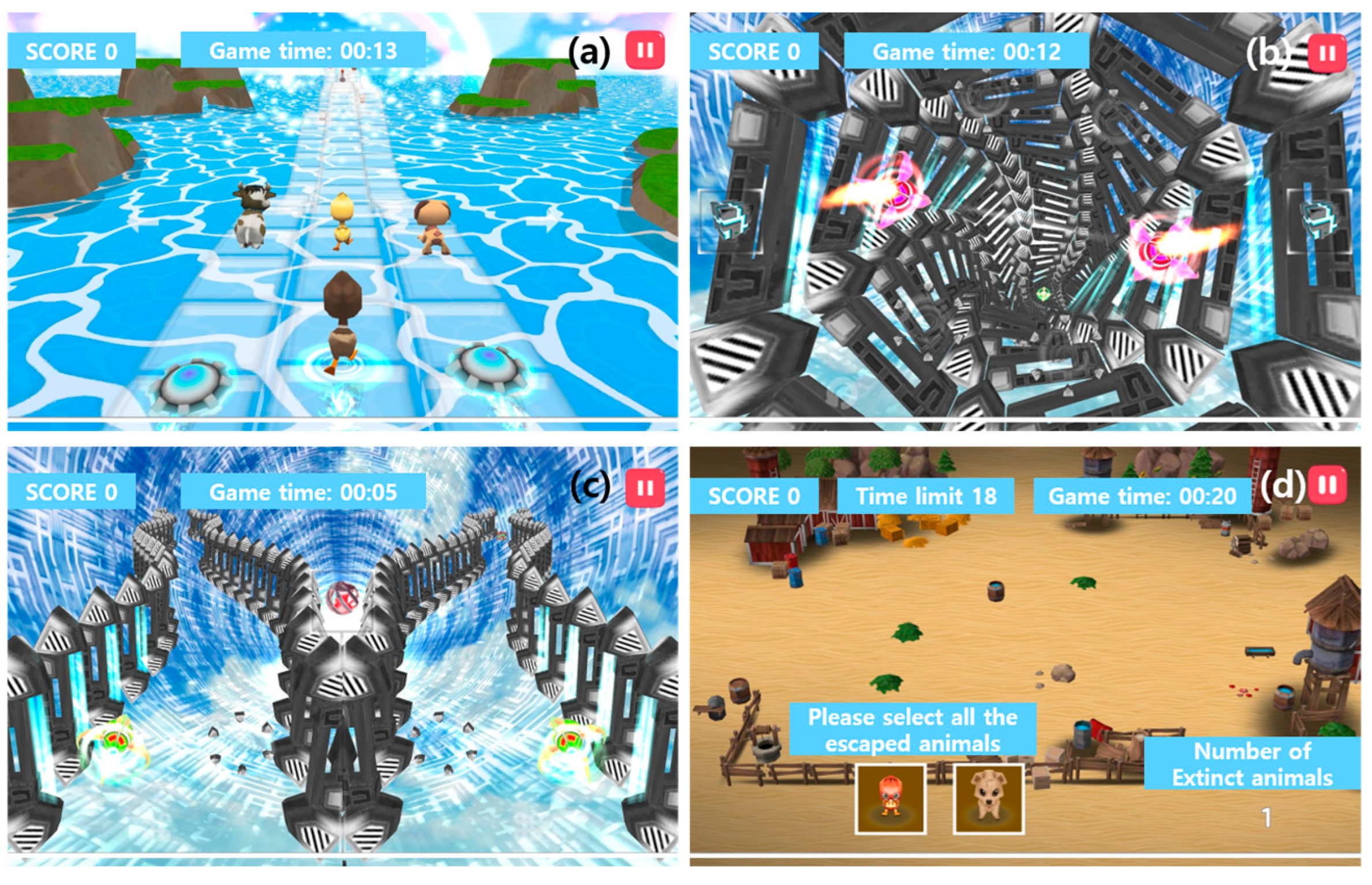
2.4. Types of Digital Therapeutic Tools
2.5. Data Analysis
3. Results
3.1. Participant Information
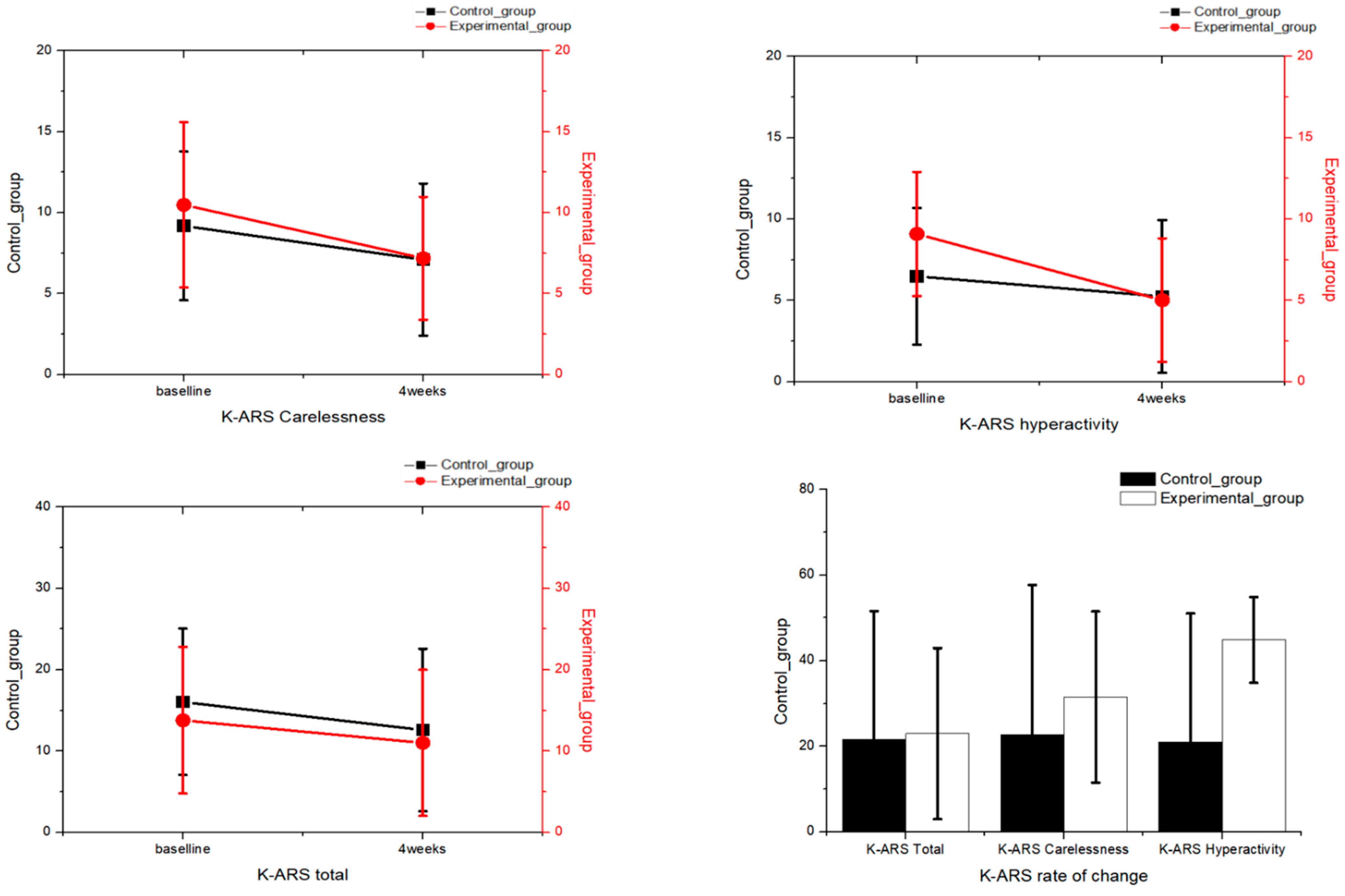
3.2. Attention Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ITT | Intention-to-treat |
| ADHD | Attention deficit hyperactivity disorder |
| CAT | Comprehension Attention Test |
| K-ARS | Korean ADHD Rating Scale |
| DTx | Digital therapeutics |
References
- Ayokunmi, L.A.; Seman, N.A.A.; Rashid, U.K.; Mohamad, A. The role of social media marketing as an ICT tool in improving supply chain sustainability of SMEs: A systematic literature review. Procedia Comput. Sci. 2025, 253, 1392–1401. [Google Scholar] [CrossRef]
- Saif, S.M.; Ansarullah, S.I.; Ben Othman, M.T.; Alshmrany, S.; Shafiq, M.; Hamam, H. Impact of ICT in modernizing the global education industry to yield better academic outreach. Sustainability 2022, 14, 6884. [Google Scholar] [CrossRef]
- Zhou, X.; Chen, L.H.; Chen, C.L. Collaborative learning by teaching: A pedagogy between learner-centered and learner-driven. Sustainability 2019, 11, 1174. [Google Scholar] [CrossRef]
- Gillantes, S.; Yreck, S. Teaching challenges using the Zoom application that focuses on student concentration in online classrooms. J. Asian Multicult. Res. Educ. Study 2021, 2, 16–20. [Google Scholar] [CrossRef]
- Sibley, M.H.; Ortiz, M.; Gaias, L.M.; Reyes, R.; Joshi, M.; Alexander, D.; Graziano, P. Top problems of adolescents and young adults with ADHD during the COVID-19 pandemic. J. Psychiatr. Res. 2021, 136, 190–197. [Google Scholar] [CrossRef]
- Xinran, H. The influence of college students’ self-cognition and learning environment on learning concentration in online learning. In Proceedings of the 5th International Conference on Mechanical, Control and Computer Engineering (ICMCCE), Harbin, China, 25–27 December 2020; IEEE: New York, NY, USA, 2020; pp. 1850–1854. [Google Scholar] [CrossRef]
- Coghill, D.; Banaschewski, T.; Cortese, S.; Asherson, P.; Brandeis, D.; Buitelaar, J.; Daley, D.; Danckaerts, M.; Dittmann, R.W.; Doepfner, M.; et al. The management of ADHD in children and adolescents: Bringing evidence to the clinic: Perspective from the European ADHD Guidelines Group (EAGG). Eur. Child Adolesc. Psychiatry 2023, 32, 1337–1361. [Google Scholar] [CrossRef]
- Sun, T.H.; Yeom, J.W.; Choi, K.Y.; Kim, J.L.; Lee, H.J.; Kim, H.J.; Cho, C.H. Potential effectiveness of digital therapeutics specialized in executive functions as adjunctive treatment for clinical symptoms of attention-deficit/hyperactivity disorder: A feasibility study. Front. Psychiatry 2023, 14, 1169030. [Google Scholar] [CrossRef]
- Chenais, N.; Görgen, A. Immersive interfaces for clinical applications: Current status and future perspective. Front. Neurorobotics 2024, 18, 1362444. [Google Scholar] [CrossRef]
- Alotaibi, M.S. Game-based learning in early childhood education: A systematic review and meta-analysis. Front. Psychol. 2024, 15, 1307881. [Google Scholar] [CrossRef]
- Bilan, D.S.; Chicchi Giglioli, I.A.; Cuesta, P.; Cañadas, E.; de Ramón, I.; Maestú, F.; Alda, J.; Ramos-Quiroga, J.A.; Herrera, J.A.; Amado, A.; et al. Decreased impulsiveness and MEG normalization after AI-digital therapy in ADHD children: A RCT. NPJ Ment. Health Res. 2025, 4, 1. [Google Scholar] [CrossRef]
- Chacko, A.; Merrill, B.M.; Kofler, M.J.; Fabiano, G.A. Improving the efficacy and effectiveness of evidence-based psychosocial interventions for attention-deficit/hyperactivity disorder (ADHD) in children and adolescents. Transl. Psychiatry 2024, 14, 244. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.; Offidani, E.; Taraboanta, L.; Lakhan, S.E.; Campellone, T.R. Appropriate controls for digital therapeutic clinical trials: A narrative review of control conditions in clinical trials of digital therapeutics (DTx) deploying psychosocial, cognitive, or behavioral content. Front. Digit. Health 2022, 4, 823977. [Google Scholar] [CrossRef] [PubMed]
- Brynte, C.; Khemiri, L.; Stenström, H.; Konstenius, M.; Lindström, N.J.; Franck, J. Impulsive choice in individuals with comorbid amphetamine use disorder and attention deficit-hyperactivity disorder. BMC Psychiatry 2023, 23, 537. [Google Scholar] [CrossRef]
- Patrickson, B.; Shams, L.; Fouyaxis, J.; Strobel, J.; Schubert, K.O.; Musker, M.; Bidargaddi, N. Evolving adult ADHD care: Preparatory evaluation of a prototype digital service model innovation for ADHD care. Int. J. Environ. Res. Public Health 2024, 21, 582. [Google Scholar] [CrossRef]
- Huang, S.; Zhang, T.; Lu, Q.; Xiong, X.; Liu, Z.; Sun, D. Clinical study on the intervention effect of digital therapy on children with attention deficit hyperactivity disorder (ADHD). Sci. Rep. 2024, 14, 23733. [Google Scholar] [CrossRef]
- Park, D.W.; Jang, C.O. Development of digital contents for ADHD treatment specialized for VR-based children. Int. J. Adv. Cult. Technol. 2023, 11, 302–309. [Google Scholar]
- Matsumoto, M.; Vilaboa, C.; Aliagas Marin, C.; Correro Iglesias, C.; Espallargas Carvajal, L.A. Children’s digital practices and family dynamics during the COVID-19 lockdown: Contrasting children’s and parents’ perspectives. J. Fam. Stud. 2025, 31, 140–160. [Google Scholar] [CrossRef]
- Maniruzzaman, M.; Hirooka, K.; Tomioka, Y.; Hasan, M.A.M.; Hwang, Y.S.; Megumi, A.; Yasumura, A.; Shin, J. Machine learning-based ADHD detection from fNIRs signal during reverse Stroop tasks. IEEE Access 2024, 12, 82984–82995. [Google Scholar] [CrossRef]
- Feng, S.; Bao, M.; Wang, J.; Ye, J.; Wang, J.; Li, W.; Jiang, K.; Yao, L. Efficacy and Safety of a Serious-Game-Like Digital Therapy Intervention for Chinese ADHD Children: A Pilot Study, 2024. Available online: https://www.researchsquare.com/article/rs-4303654/v1 (accessed on 3 April 2025).
- Perme, M.P.; Manevski, D. Confidence intervals for the Mann–Whitney test. Stat. Methods Med. Res. 2019, 28, 3755–3768. [Google Scholar] [CrossRef]
- Janssen, L.; Kan, C.C.; Carpentier, P.J.; Sizoo, B.; Hepark, S.; Schellekens, M.P.J.; Donders, A.R.T.; Buitelaar, J.K.; Speckens, A.E.M. Mindfulness-based cognitive therapy v. treatment as usual in adults with ADHD: A multicentre, single-blind, randomised controlled trial. Psychol. Med. 2019, 49, 55–65. [Google Scholar] [CrossRef]
- Jang, M.S.; Chung, S.K.; Yang, J.C.; Park, J.I.; Kwon, J.H.; Park, T.W. Association of the Comprehensive Attention Test and the Korean Wechsler Intelligence Scale for Children–Fourth Edition in children and adolescents with attention-deficit/hyperactivity disorder. J. Korean Acad. Child Adolesc. Psychiatry 2023, 34, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Li, F.; Wu, Y.; Liu, X.; Zheng, Q.; Qi, Y.; Huang, H.; Xu, G.; Liu, Z.; He, F.; et al. A mobile device-based game prototype for ADHD: Development and preliminary feasibility testing. Transl. Psychiatry 2024, 14, 251. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.M.; Lee, J.S.; Kim, S.Y.; Kim, H.W. Diagnostic significance of comprehensive attention test in children and adolescents with attention-deficit hyperactivity disorder. J. Korean Acad. Child Adolesc. Psychiatry 2011, 22, 246–252. [Google Scholar] [CrossRef]
- Kim, K.M.; Ha, M.; Lim, M.H.; Kwon, H.J.; Yoo, S.J.; Kim, E.; Paik, K.C. The symptom trajectory of attention-deficit hyperactivity disorder in Korean school-age children. Psychiatry Investig. 2018, 15, 470–475. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, J.H.; Jeong, M.Y.; Lee, Y.S.; Shin, J.E.; Lee, Y.J. Reliability and validity of the Korean version of the Parental Stress Scale for children with attention-deficit/hyperactivity disorder. Psychiatry Investig. 2021, 18, 1188–1197. [Google Scholar] [CrossRef]
- Mishra, P.; Singh, U.; Pandey, C.M.; Mishra, P.; Pandey, G. Application of Student’s t-test, analysis of variance, and covariance. Ann. Card. Anaesth. 2019, 22, 407–411. [Google Scholar] [CrossRef]
- Casas, M.; Rösler, M.; Sandra Kooij, J.J.; Ginsberg, Y.; Ramos-Quiroga, J.A.; Heger, S.; Berwaerts, J.; Dejonckheere, J.; van der Vorst, E.; Schäuble, B. Efficacy and safety of prolonged-release OROS methylphenidate in adults with attention deficit/hyperactivity disorder: A 13-week, randomized, double-blind, placebo-controlled, fixed-dose study. World J. Biol. Psychiatry 2013, 14, 268–281. [Google Scholar] [CrossRef]
- Gadbury, G.L.; Coffey, C.S.; Allison, D.B. Modern statistical methods for handling missing repeated measurements in obesity trial data: Beyond LOCF. Obes. Rev. 2003, 4, 175–184. [Google Scholar] [CrossRef]
- Ekinci, Ö.; Doğan, Ö.İ.; Yaşöz, C.; Ekinci, N.; Baş, S.A.İ.; Adak, İ. Clinical correlates of restrictive type attention deficit hyperactivity disorder in adolescents. Haydarpaşa Numune Med. J. 2021, 61, 295–299. [Google Scholar] [CrossRef]
- Park, E.; Cho, M.; Ki, C.S. Correct use of repeated measures analysis of variance. Korean J. Lab. Med. 2009, 29, 1–9. [Google Scholar] [CrossRef]
- Lee, J.H.; Herzog, T.A.; Meade, C.D.; Webb, M.S.; Brandon, T.H. The use of GEE for analyzing longitudinal binomial data: A primer using data from a tobacco intervention. Addict. Behav. 2007, 32, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Levine, T.R.; Hullett, C.R. Eta squared, partial eta squared, and misreporting of effect size in communication research. Hum. Commun. Res. 2002, 28, 612–625. [Google Scholar] [CrossRef]
- Putra, A.S.; Warnars, H.L.H.S.; Abbas, B.S.; Trisetyarso, A.; Suparta, W.; Kang, C.H. Gamification in the e-learning process for children with attention deficit hyperactivity disorder (ADHD). In Proceedings of the 2018 Indonesian Association for Pattern Recognition International Conference (INAPR), Jakarta, Indonesia, 7–8 September 2018; pp. 182–185. [Google Scholar] [CrossRef]
- Pandian, G.S.B.; Jain, A.; Raza, Q.; Sahu, K.K. Digital health interventions (DHI) for the treatment of attention deficit hyperactivity disorder (ADHD) in children—a comparative review of literature among various treatment and DHI. Psychiatry Res. 2021, 297, 113742. [Google Scholar] [CrossRef] [PubMed]
- Sanuki, F.; Nakphu, N.; Tahara, A.; Iramina, K. The comparison of electroencephalography power and event related potential in success and failure during multitask game. Front. Neurorobotics 2022, 16, 1044071. [Google Scholar] [CrossRef]
- Washington, P.; Wall, D.P. A review of and roadmap for data science and machine learning for the neuropsychiatric phenotype of autism. Annu. Rev. Biomed. Data Sci. 2023, 6, 211–228. [Google Scholar] [CrossRef]
- Antonopoulou, H.; Halkiopoulos, C.; Gkintoni, E.; Katsimpelis, A. Application of gamification tools for identification of neurocognitive and social function in distance learning education. Int. J. Learn. Teach. Educ. Res. 2022, 21, 367–400. [Google Scholar] [CrossRef]
- Skalski, S.; Pochwatko, G.; Balas, R. Impact of motivation on selected aspects of attention in children with ADHD. Child Psychiatry Hum. Dev. 2021, 52, 586–595. [Google Scholar] [CrossRef]
- Wang, H.; Sun, C.T. Game reward systems: Gaming experiences and social meanings. In Proceedings of the DiGRA 2011 Conference: Think Design Play, Utrecht, The Netherlands, 14–17 September 2011. [Google Scholar]
- Mitsea, E.; Drigas, A.; Skianis, C. VR gaming for meta-skills training in special education: The role of metacognition, motivations, and emotional intelligence. Educ. Sci. 2023, 13, 639. [Google Scholar] [CrossRef]
- Biederman, J.; Faraone, S.V.; Monuteaux, M.C.; Bober, M.; Cadogen, E. Gender effects on attention-deficit/hyperactivity disorder in adults, revisited. Biol. Psychiatry 2004, 55, 692–700. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group (N = 20) | Control Group (N = 20) | p-Value | ||||
|---|---|---|---|---|---|---|
| Mean or N | SD or % | N | % | |||
| Gender | 0.024 * | |||||
| Boy | 16 | 80 | 11 | 55 | ||
| Girl | 4 | 20 | 9 | 45 | ||
| Age | 0.838 * | |||||
| 6–7 | 2 | 10 | 2 | 10 | ||
| 8–9 | 10 | 50 | 12 | 60 | ||
| 10–11 | 4 | 20 | 4 | 20 | ||
| 12–13 | 4 | 20 | 2 | 10 | ||
| 9.3 | 2.67 | 8.85 | 2.58 | 0.59 ** | ||
| Experimental Group (N = 20) | Control Group (N = 20) | p-Value | Effect Size | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Simple selection (visual) | Baseline | 3.07 | 0.81 | 3.05 | 0.49 | 0.165 * | |
| Four weeks | 3.59 | 0.57 | 3.40 | 0.33 | 0.849 * | ||
| p-value | 0.024 ** | 0.520 ** | 0.039 *** | 0.042 ## | |||
| Effect size | 0.667 # | 0.742 # | |||||
| Change rate | −16.94 | 29.63 | −11.48 | 32.65 | 0.028 * | ||
| Simple selection (auditory) | Baseline | 1.10 | 0.58 | 1.78 | 1.27 | 0.097 * | |
| Four weeks | 1.25 | 1.16 | 1.54 | 0.63 | 0.880 * | ||
| p-value | 0.749 ** | 0.410 ** | 0.146 *** | 0.025 ## | |||
| Effect size | 0.269 # | 0.196 # | |||||
| Change rate | −13.64 | −100 | 13.48 | 50.39 | 0.112 * | ||
| Sustained inhibition | Baseline | 2.05 | 1.08 | 2.38 | 0.75 | 0.475 * | |
| Four weeks | 2.31 | 0.54 | 2.46 | 1.02 | 0.514 * | ||
| p-value | 0.679 ** | 0.157 ** | 0.040 ** | 0.009 ## | |||
| Effect size | 0.250 # | 0.111 # | |||||
| Change rate | −12.68 | 50 | −3.36 | −36 | 0.014 * | ||
| Interference selection | Baseline | 0.62 | 0.76 | 0.57 | 0.36 | 0.498 * | |
| Four weeks | 0.80 | 0.50 | 0.84 | 0.45 | 0.106 * | ||
| p-value | 0.064 ** | 0.077 ** | 0.043 *** | 0.002 ## | |||
| Effect size | 0.246 # | 0.780 # | |||||
| Change rate | −29.03 | 34.21 | −47.37 | −25 | 0.579 * | ||
| Total CAT score | Change rate | 40.2 | 10.4 | 34.0 | 17.2 | 0.038 * | 0. 436 # |
| Experimental Group (N = 20) | Control Group (N = 20) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Simple selection (visual) | Baseline | 0.28 | 0.38 | 0.36 | 0.31 | 0.491 * | |
| Four weeks | 0.87 | 0.38 | 0.36 | 0.31 | 0.754 * | ||
| p-value | 0.151 ** | 0.110 ** | 0.044 *** | ||||
| Change rate | −141.67 | −393.55 | −35.71 | −28.95 | 0.028 * | ||
| N | % | N | % | ||||
| Deterioration | 8 | 40.0 | 5 | 25.0 | 0.854 *** | ||
| Pre-post change | No change | 0 | 0.0 | 1 | 5.0 | ||
| Improvement | 12 | 60.0 | 14 | 70.0 | |||
| Simple selection (auditory) | Baseline | 0.72 | 0.54 | 0.47 | 0.20 | 0.084 * | |
| Four weeks | 0.86 | 0.74 | 0.62 | 0.32 | 0.490 * | ||
| p-value | 0.460 ** | 0.140 ** | 0.579 *** | ||||
| Change rate | −19.44 | −64.44 | −31.91 | −60.00 | 0.549 * | ||
| N | % | N | % | ||||
| Deterioration | 2 | 10 | 6 | 30 | 0.451 **** | ||
| Pre-post change | No change | 3 | 15 | 0 | 0 | ||
| Improvement | 15 | 75 | 14 | 70 | |||
| Interference selection | Baseline | 0.70 | 0.08 | 0.77 | 0.21 | 0.742 * | |
| Four weeks | 0.67 | 0.15 | 0.57 | 0.27 | 0.212 * | ||
| p-value | 0.620 ** | 0.001 ** | 0.143 *** | ||||
| Change rate | 4.29 | −87.50 | 25.97 | −28.57 | 0.026 * | ||
| N | % | N | % | ||||
| Deterioration | 10 | 50 | 10 | 50 | 0.025 **** | ||
| Pre-post change | No change | 2 | 10 | 7 | 35 | ||
| Improvement | 8 | 40 | 3 | 15 | |||
| Sustained inhibition | Baseline | 0.42 | 0.30 | 0.45 | 0.15 | 0.880 * | |
| Four weeks | 0.70 | 0.27 | 0.64 | 0.04 | 0.214 * | ||
| p-value | 0.423 ** | 0.118 ** | 0.016 *** | ||||
| Change rate | −66.67 | 10.00 | −42.22 | 73.33 | 0.042 * | ||
| N | % | N | % | ||||
| Deterioration | 11 | 55 | 12 | 60 | 0.280 **** | ||
| Pre-post change | No change | 0 | 0 | 0 | 0 | ||
| Improvement | 9 | 45 | 8 | 40 | |||
| Experimental Group (N = 20) | Control Group (N = 20) | p-Value | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| K-ARS Inattention | Baseline | 10.48 | 0.48 | 9.18 | 0.18 | 0.108 * |
| Four weeks | 7.18 | 1.10 | 7.10 | 2.48 | 0.908 * | |
| p-value | 0.008 ** | 0.346 ** | 0.498 *** | |||
| Change rate | 31.49 | −129.17 | 22.66 | −1277.78 | 0.670 * | |
| K-ARS Hyperactivity–Impulsivity | Baseline | 9.08 | 1.05 | 6.48 | 2.58 | 0.242 * |
| Four weeks | 5.01 | 5.18 | 5.24 | 4.03 | 0.729 * | |
| p-value | 0.010 ** | 0.102 ** | 0.18 *** | |||
| Change rate | 44.82 | −393.33 | 20.99 | −56.20 | 0.002 * | |
| K-ARS Total Score | Baseline | 15.77 | 6.18 | 16.04 | 4.28 | 0.108 * |
| Four weeks | 12.15 | 8.29 | 12.58 | 9.15 | 0.910 * | |
| p-value | 0.026 ** | 0.580 ** | 0.012 *** | |||
| Change rate | 22.95 | −34.14 | 21.57 | −133.79 | 0.025 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-C. The Effectiveness of Story- and Quiz-Based Games in Digital Interventions for ADHD: A Comparative Approach. Appl. Sci. 2025, 15, 4334. https://doi.org/10.3390/app15084334
Kim S-C. The Effectiveness of Story- and Quiz-Based Games in Digital Interventions for ADHD: A Comparative Approach. Applied Sciences. 2025; 15(8):4334. https://doi.org/10.3390/app15084334
Chicago/Turabian StyleKim, Seon-Chil. 2025. "The Effectiveness of Story- and Quiz-Based Games in Digital Interventions for ADHD: A Comparative Approach" Applied Sciences 15, no. 8: 4334. https://doi.org/10.3390/app15084334
APA StyleKim, S.-C. (2025). The Effectiveness of Story- and Quiz-Based Games in Digital Interventions for ADHD: A Comparative Approach. Applied Sciences, 15(8), 4334. https://doi.org/10.3390/app15084334