1. Introduction
Affecting 1 in every 800 live births globally [
1], cleft lip and palate represent the most prevalent craniofacial birth defects. The aim of the surgical hard and soft tissue closure is to restore the complete function of the stomatognathic system, ensuring that speech, chewing, and breathing are adequately supported [
2]. However, preoperative infant orthopedic interventions precede surgical cleft closure, beginning at birth and presenting unique challenges. Shortly after birth, a removable drinking plate is custom fabricated for each patient. This obturator not only separates the oral and nasal cavities, functioning as an artificial palatal roof to establish a physiological anterior caudal tongue position, but also enhances sucking and swallowing functions [
3]. Within the framework of Presurgical Infant Orthopedics (PSIO), 3D models of the patient’s upper jaw are digitally modified through incremental modification of the cleft region based on empirical judgment, aiming to align and harmonize the upper jaw segments toward a physiological arch form in preparation for surgical cleft closure.
This demands not only professional expertise but also, most importantly, a profound comprehension of the maxillary growth patterns by the practitioner.
Most previous studies have investigated morphological changes in the maxilla based on measurements taken from plaster casts [
4,
5,
6,
7] or digitized plaster models [
8,
9,
10,
11,
12,
13]. Traditional impression taking with alginate carries several risks. The complex anatomy of the cleft area increases the likelihood of the impression material tearing during the process. Impression material left unnoticed in the cleft area can cause inflammation in the surrounding tissues. In severe cases, torn impression material may lead to aspiration, necessitating immediate medical intervention [
14]. The mentioned risks associated with conventional impressions (CI) may be one reason why previous measuring studies based on plaster models have only produced models at a few points in time; therefore, the observation periods are very wide. If an alginate impression is poured incorrectly and contains bubbles or if the plaster used for the die material is either too thick or too thin, dimensional inaccuracies can occur. Furthermore, being brittle and bulky, the storage and retrieval of plaster casts is challenging [
15].
As advancements in digital technologies continue to reshape healthcare, the integration of digital impression methods with intraoral 3D scanners offers significant advantages. Digital impressions (intraoral 3D scan; IOS) for newborn infants with unilateral cleft lip and palate are safe, effective, and cost-efficient. Compared to conventional impression methods, they are not associated with serious risks. It is possible in rare cases for a patient to bite the tip of the intraoral 3D scanner during IOS, causing a slight superficial irritation of the mucosa, which will heal itself without medical intervention [
16]. Unlike conventional impressions, there is no comparable risk of material tearing. This makes repeated use possible throughout the course of therapy for reevaluation or therapy planning. Additionally, this new, risk-free impression-taking capability allows for rescanning of anatomically challenging areas that may not be optimally represented or are difficult to access due to cleft-related issues, ensuring the highest quality of digital maxillary models [
17]. The IOS offers accuracy comparable to that of conventional alginate impressions [
17]. It minimizes material-related errors commonly associated with traditional alginate methods [
15]. Since there is no need to customize and adapt an individual impression tray, IOS proves to be a time- and cost-efficient approach. With the appropriate expertise, an IOS can be completed within minutes, providing high-quality images of the individual jaw segment structures. IOS digital data can be easily stored, shared, and accessed, enhancing communication between clinicians and specialized healthcare centers. This streamlines workflows by eliminating physical plaster models, saving space, and preventing loss or damage. Even anatomically challenging areas can be rescanned as needed to ensure optimal quality of the digital upper jaw models [
17].
As previous measurement studies have largely been based on the analysis of digitized plaster models, which come with the previously mentioned limitations, new digital measurement methods are essential for analyzing maxillary growth and measuring the jaw segments of patients with unilateral cleft lip and palate to complete the digital workflow. With the advantages of intraoral 3D scanning (IOS) mentioned above, digital measurement methods improve the accuracy and reproducibility of assessments, which is crucial for identifying anatomical variations associated with unilateral cleft conditions. These advanced techniques allow for detailed maxillary analysis, enabling clinicians to capture subtle changes that might be overlooked by traditional methods. Through digital model analysis for these patients, specialized software patches allow for adjustments and continuous expansion of analyses. Collected measurement data remains permanently available, enabling the creation of comprehensive digital databases and can be easily shared between specialized centers. This digital workflow facilitates better communication and coordination among multidisciplinary teams who are necessarily involved in the therapy and long-term care of this special patient group.
Scientific research concerning growth-related changes of the maxillae in patients with unilateral cleft lip and palate vary in the number of measurement points and their terminology [
5,
10,
18,
19,
20,
21]. While existing studies measure the cleft width as the distance between the alveolar ridge crests of the larger and smaller segments, the actual point of closest approach between the segments is not evaluated. Furthermore, previous studies have not measured the subsegment width, which would allow for a more detailed assessment of growth processes in different sagittal regions of the alveolar ridges. Moreover, most previous measurement studies lack a precise guide for implementing a measurement method into the digital workflow.
The aim of this study was to introduce a new digital measurement method for digital models of patients with unilateral cleft lip and palate with the analysis software OnyxCeph3™ (Image Instruments® GmbH, Chemnitz, Germany) and its integration into the interdisciplinary Frankfurt approach. The integration of OnyxCeph3™ computer-aided measurement is expected to improve the accuracy and efficiency of evaluating digital models for patients with unilateral cleft lip and palate, facilitating more informed decisions and personalized treatment strategies, ultimately enhancing patient outcomes.
2. Materials and Methods
The following section outlines the complete digital workflow for measuring models of patients with unilateral cleft lip and palate. It presents an overview of the data collection and model preparation stages before moving on to an examination of the software and analysis protocol with a focus on their practical application.
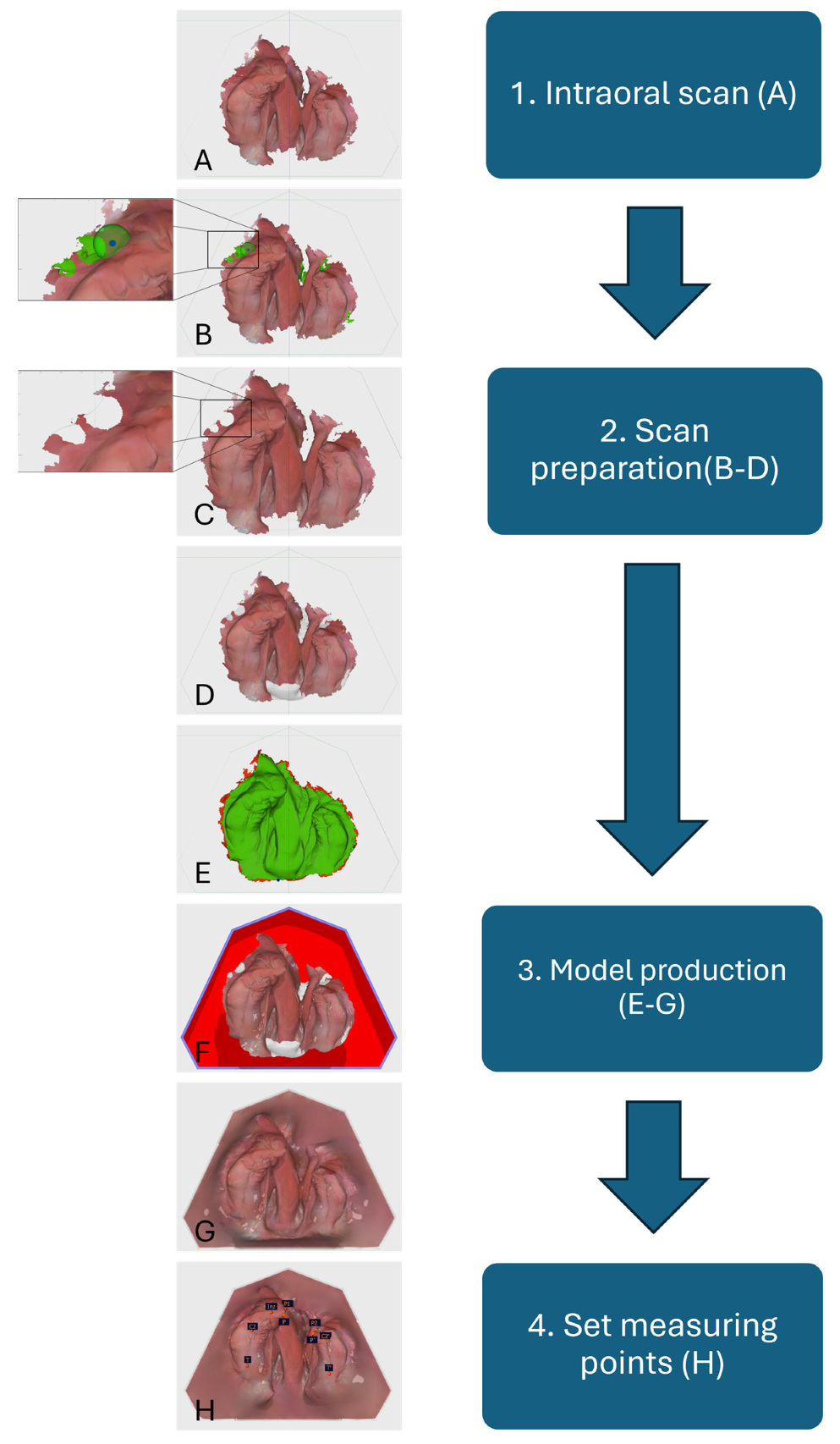
The digital workflow of the Frankfurt approach (
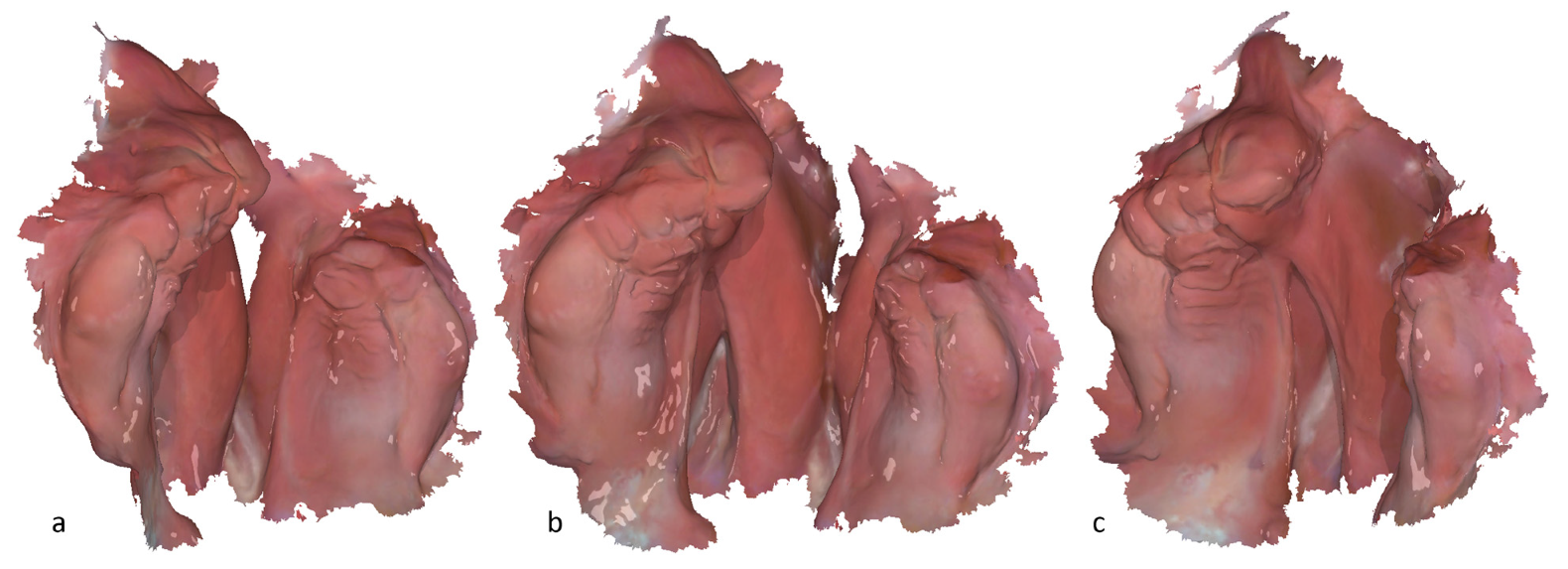
Figure 1, Step 1) initiates with an IOS, which serves as the foundation for subsequent digital measurement. IOS of the upper jaw segments is obtained using a 3Shape intraoral 3D scanner; both the Trios 3 and Trios 4 are in application (3Shape A/S, Copenhagen, Denmark). To ensure precise image acquisition and optimal texture quality, the intraoral 3D scanner undergoes weekly calibration per the manufacturer’s instructions. Before the initial 3D scan, the patient data are entered into the 3D scanner system. For the 3D-scanning procedure, the newborns are positioned supine on a pillow covered with a sterile pad. In order to achieve the best possible 3D scan quality, the patient’s jaw area is first cleaned superficially with the aid of a moistened gauze swab, and any adhesive cream residue is removed. Where possible, the jaw segments are then dried with the aid of dry gauze and a saliva ejector. The newborns remain awake and are not sedated during the IOS. A sterilized standard 3D scan tip of the corresponding 3Shape intraoral 3D scanner is used for the intraoral 3D scan, which typically takes about 3 min (
Figure 1 and
Figure 2). The IOS must be verified to ensure that all relevant anatomical features have been captured for subsequent measurement. Any missing or poorly captured areas of the alveolar ridge must be re-3D-scanned. Once the intraoral 3D scan is complete, a post-processing step is performed using the IOS software to generate an exportable 3D data set.
The model preparation ensures that the data are properly prepared and aligned for accurate measurement. Subsequently, the IOS data obtained are imported into the OnyxCeph
3™ software for processing and preparation for the digital measurement (
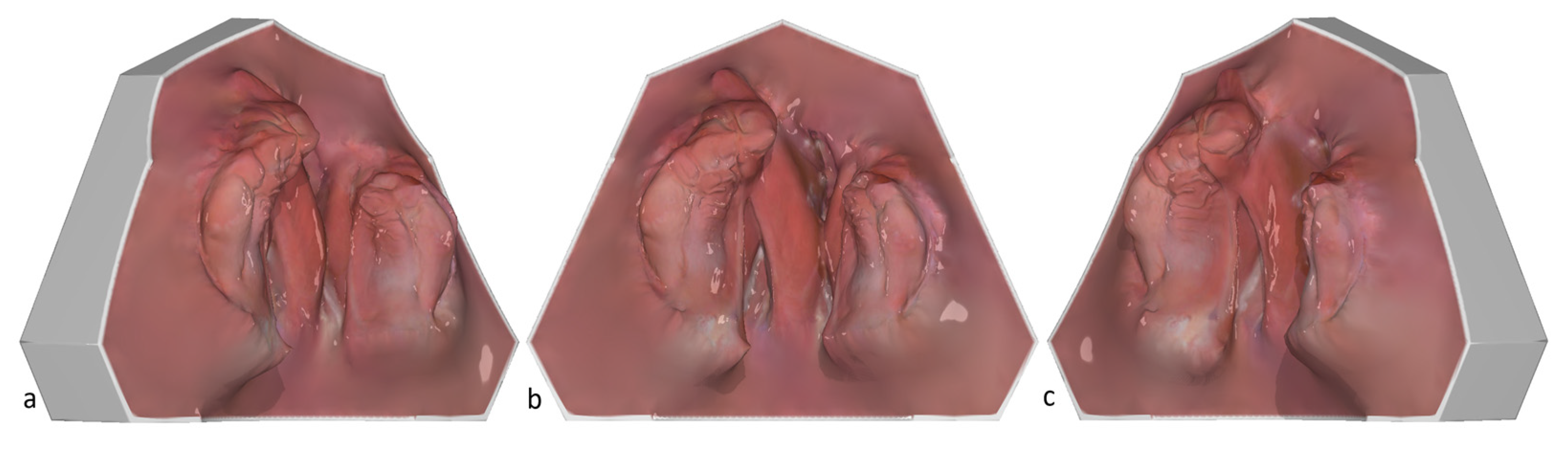
Figure 1, Step 2). The edges of the IOS are trimmed to eliminate any excess or irrelevant data. Subsequently, a 3D model is generated from the 3D data set using a base (
Figure 3, Step 3, and
Figure 1).
The software OnyxCeph
3™, developed by Image Instruments
® GmbH in Chemnitz, Germany, is implemented for processing the 3D digital dental models of patients with unilateral cleft lip and palate. Developed as a “native network application for patient- and case-related management of 2D and 3D image data” [
22], this application facilitates advanced 3D data processing and visualization and also enables precise measurements.
The digital cleft palate models can be precisely measured with the modules “Model Alignment” and “Evaluation” in the OnyxCeph
3™ software. The system enables the users to define measurement points, which are subsequently saved as X, Y, and Z coordinates (
Figure 1, Step 4). By utilizing vector calculations, the positions of the entities in three-dimensional space can be determined in terms of distance. These distances can then be assessed relative to one another, such as through angle measurements. Additionally, the distance from individual measurement points to constructed reference planes can be calculated. The area of a specified region can also be computed by aggregating the surface areas of the known polygons within that defined area. In collaboration with OnyxCeph
3™, we implemented patches that were adapted to our specific Frankfurt approach requirements for measuring models with one-sided cleft lip and palate in the evaluation software. The respective built-in patches to analyze our key anatomical landmarks are available for use in the Measurement module of the software.
Critical anatomical and constructed landmarks on cleft lip and palate models are defined below to ensure consistent measurements.
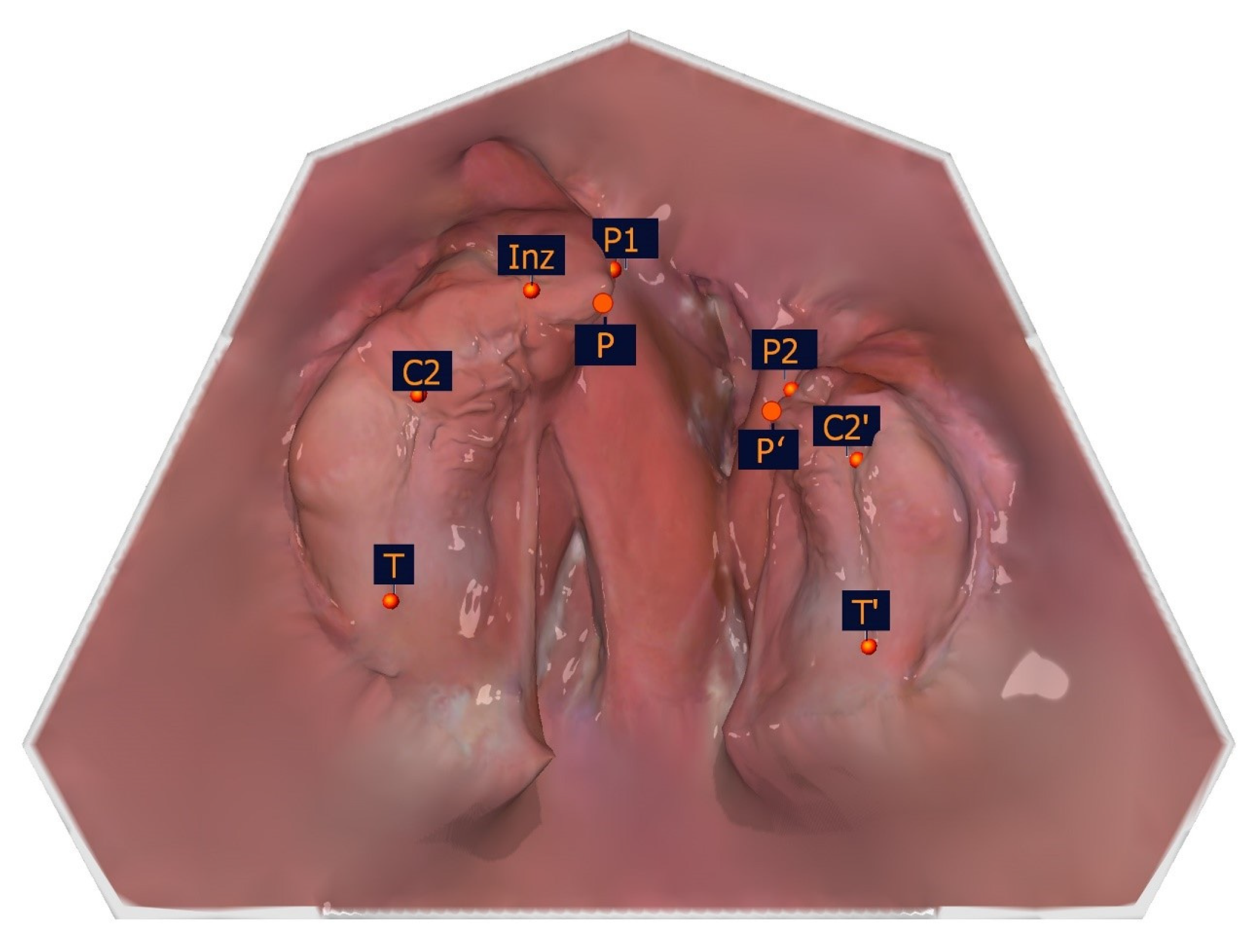
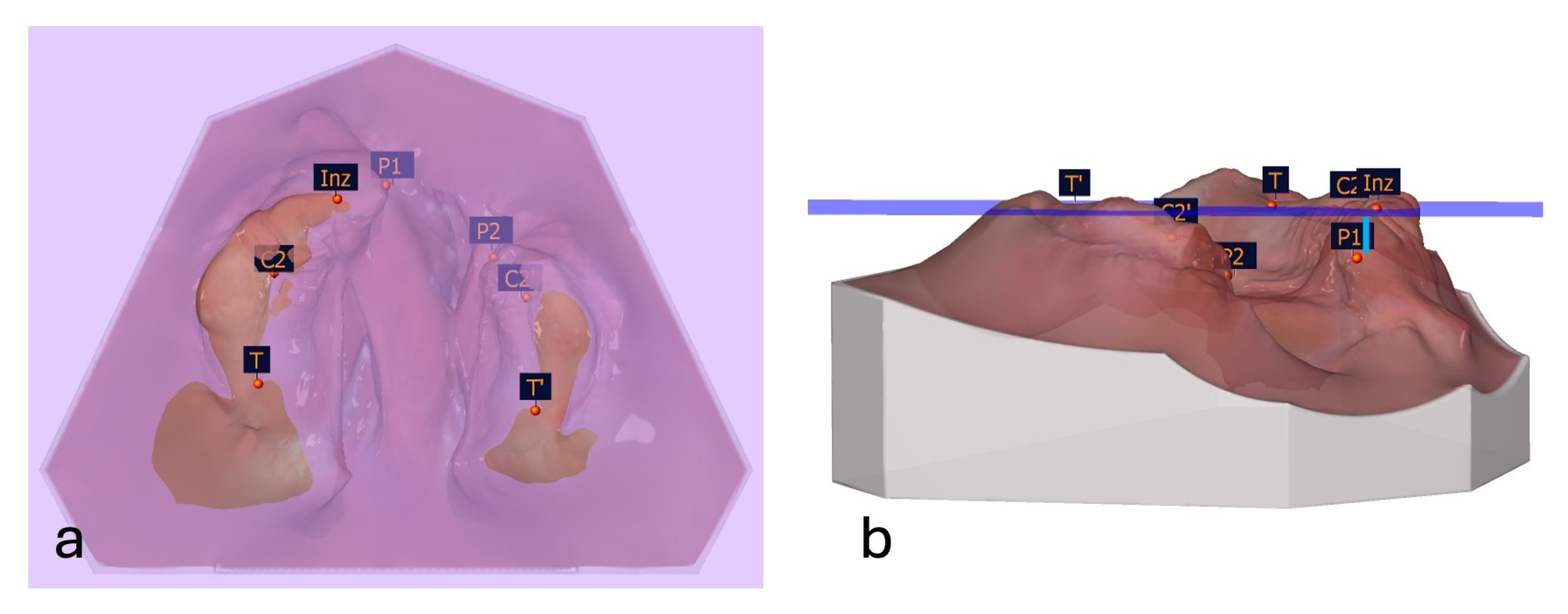
The selection of the measuring points detailed in
Table 1 was based on a number of factors, including the publications of Mazaheri et al. [
18], Ashley-Montagu [
19], Sillman [
20], and Robertson [
21]. If a point appears on both jaw segments, a ′ indicates that the point is located on the smaller jaw segment.
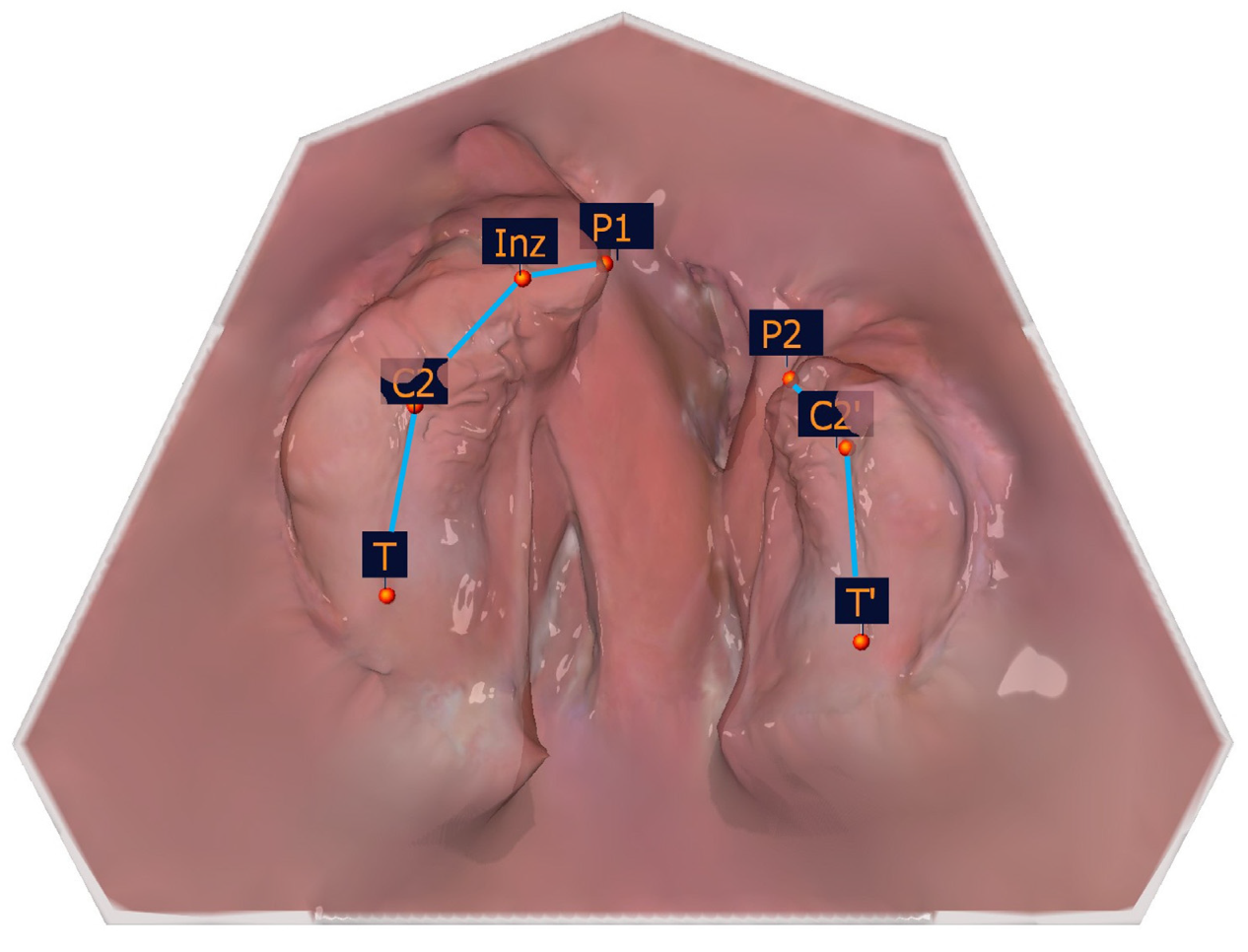
Figure 4 and
Table 1 show the measuring points on a dental left-sided cleft lip and palate model.
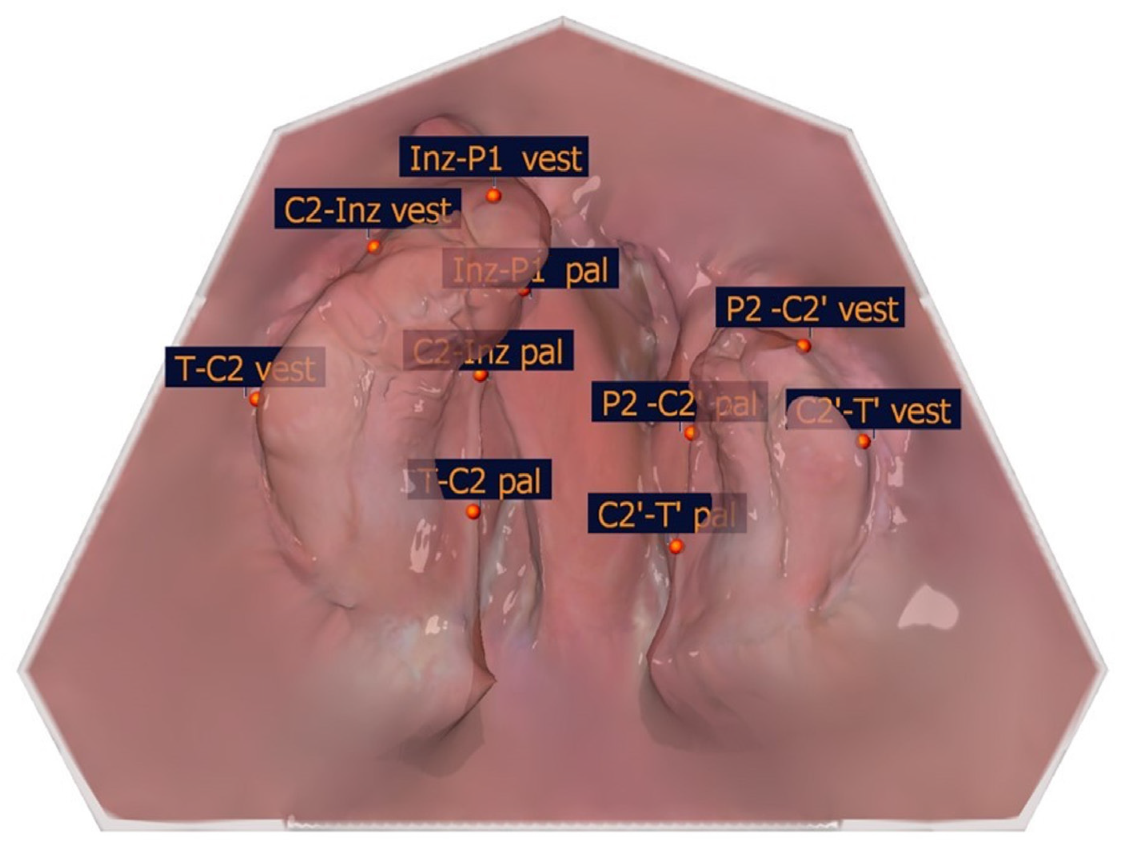
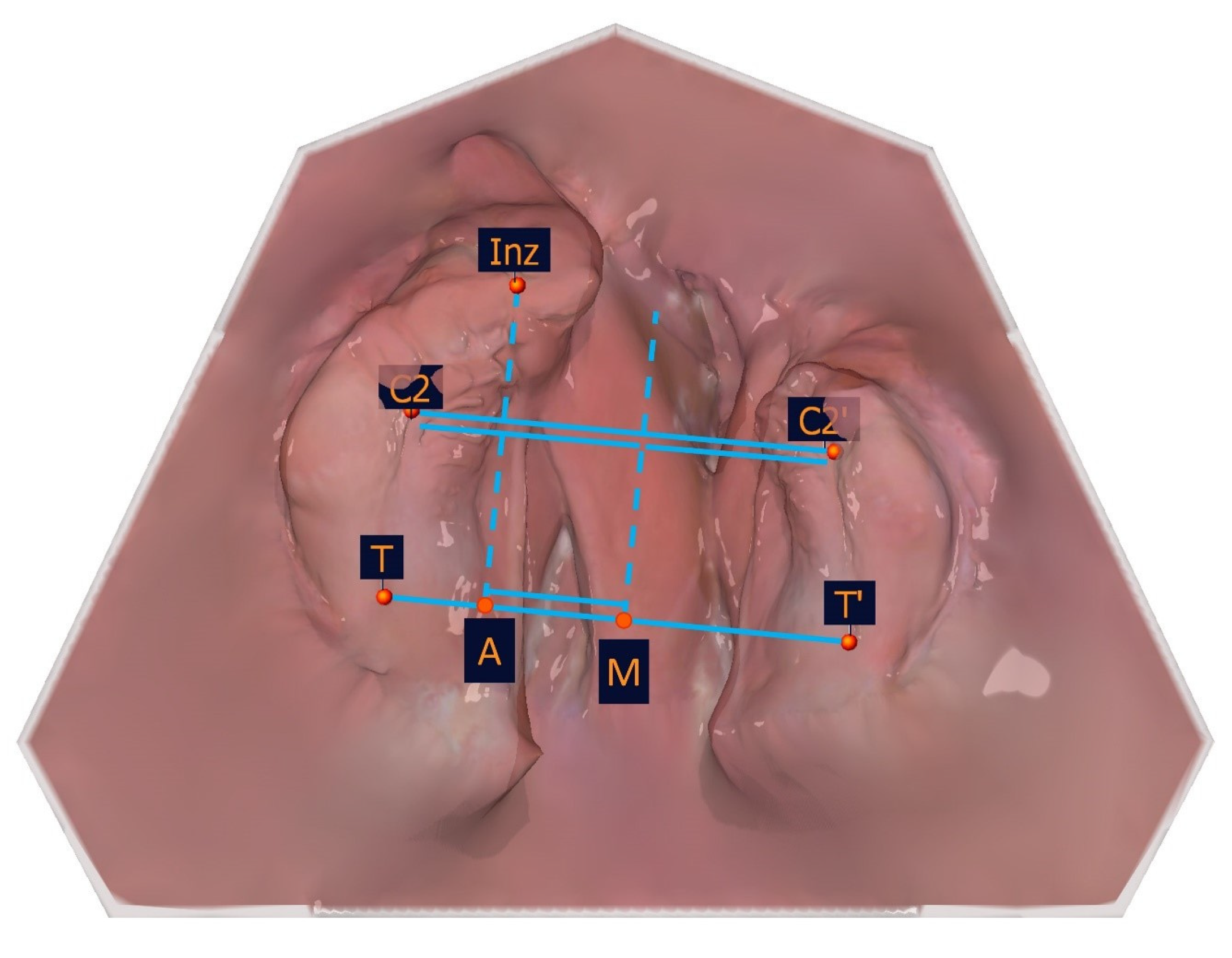
To identify the transversal landmarks, the large and small segments were divided into the subsegments (T-C2, C2-Inz, and Inz-P1 for the large segment and P2-C2′ and C2′-T′ for the small segment). The most vestibular and most palatal points in each section were determined (
Table 2,
Figure 5).
The following constructed measuring points are based on the measurement points listed in
Table 1 and are shown in
Table 3 and
Figure 6. These and the measurement points form the basis for the subsequent distance and angle measurements.
The measurement points of the alveolar cleft width are shown in
Table 4 and
Figure 7.
The segment length measurements are shown in detail in
Table 4 and
Figure 8.
The large and small segments were divided into subsegments to identify the transversal landmarks (T-C2, C2-Inz, and Inz-P1 for the large segment and P2-C2′ and C2′-T′for the small segment). The most vestibular and most palatal points in each section were determined. For the segmental width measurements, the greatest distance perpendicular to the length measuring sections of the partial jaw segments defines the greatest width of the jaw segments. The segment width measurements are shown in
Table 4, and an exemplar is shown in
Figure 9.
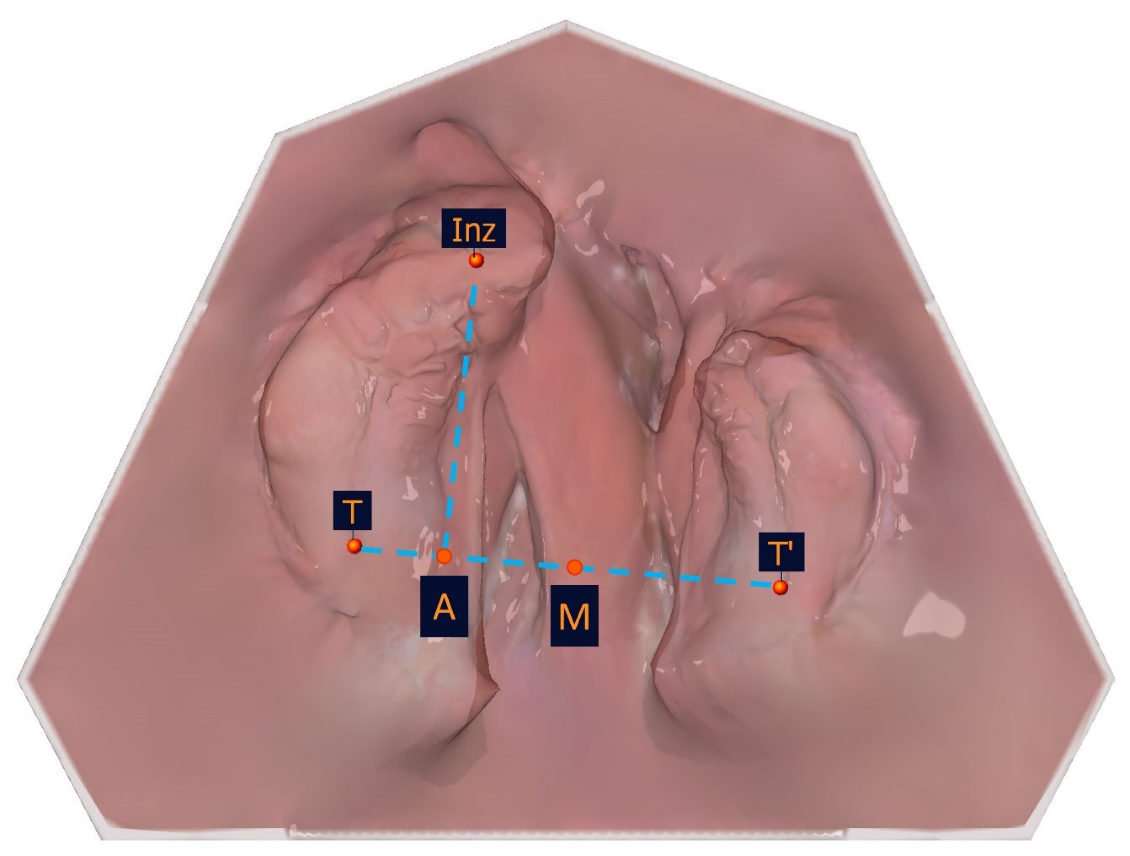
To measure the vertical, a reference plane was created through the points T, T′, and Inz, to which the respective vertical distance of the P and C points of both segments was evaluated (
Table 5,
Figure 11).
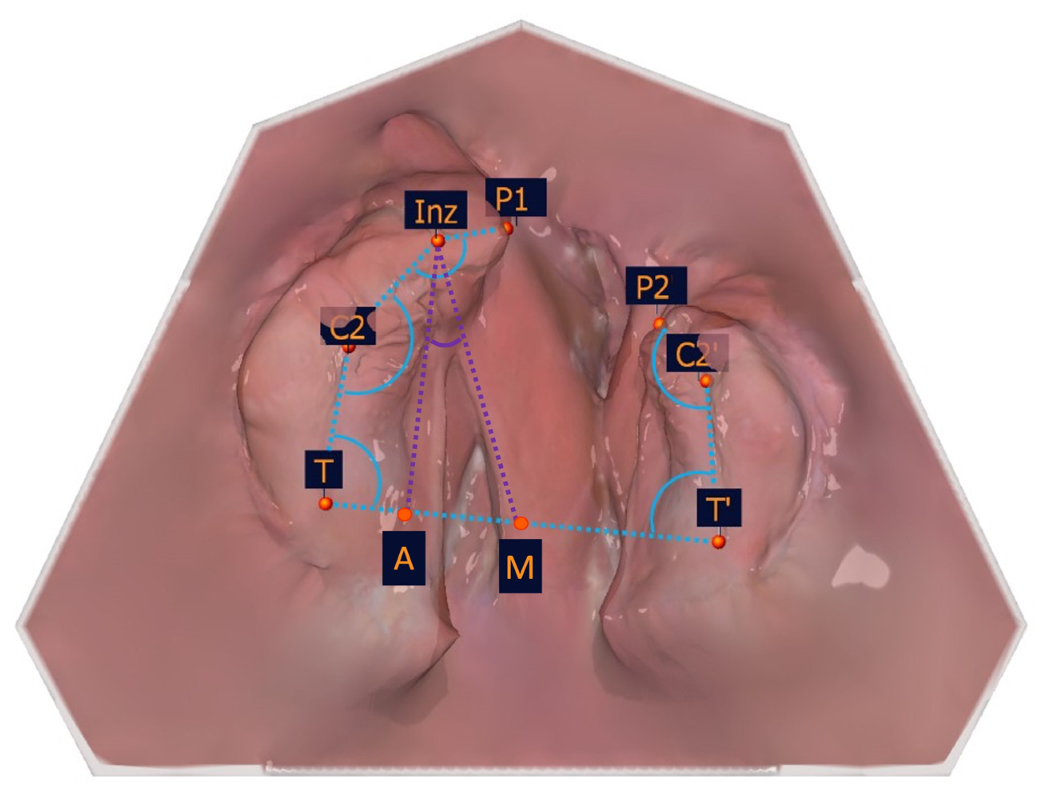
The angular measurements describe the position of individual measuring sections in relation to each other. The values are presented in ° degrees (
Table 5,
Figure 12).
The appropriate measurement points are manually selected by the clinician and can be deleted and reset or repositioned as many times as required by selecting the points individually. The corresponding distances and angles are measured digitally, and the measurement result is displayed in a corresponding table in the analysis software, which can be printed (
Figure 1, Step 6).
The computer-aided measurement of digital models for patients with unilateral cleft lip and palate in OnyxCeph3™ is precise, user-friendly, feasible, and quick to implement. The time required to measure all the distances and angles presented is approximately 5 min. Model measurement can begin after the IOS data are imported into the OnyxCeph3™ software. The model can be analyzed at any point in time. If the morphological changes in the maxilla are relevant for the further treatment of the newborn, the digital analysis can be performed immediately after the IOS. This enables timely interdisciplinary decisions to be made about treatment, such as planning a new orthodontic drinking plate, and, if necessary, to discuss these directly with the parents and schedule further treatment steps. The measurement method is designed to evaluate digital models created by IOS but can also be used for plaster models digitized by a model 3D scanner. Digital analysis with OnyxCeph3™ presented in this approach requires three-dimensional data sets; therefore, the intraoral 3D scan does not necessarily have to be performed with a 3Shape intraoral 3D scanner but can be performed with any software-compatible intraoral 3D scanner.
3. Discussion
Intraoral 3D scanning (IOS) has revolutionized the field of dentistry and orthodontics, offering a digital alternative to conventional impressions (CIs). IOS has several advantages, especially for use in infants with cleft lip and palate. One of the notable advantages of IOS and the digital model preparation is its speed. CIs, which typically involve the use of alginate or putty materials, are time-consuming, as an individual impression tray must be customized for each patient. In contrast, IOS can capture highly detailed 3D images in a matter of minutes, significantly reducing the time required for diagnosis, treatment planning, and preparation [
16,
23]. Moreover, IOS provides highly accurate digital impressions, reducing the risk of material-related errors such as distortion, bubbles, or tearing that can occur with traditional alginate impressions [
15]. Several scientific studies have focused on comparing the accuracy of conventional plaster models and digital jaw models. While research groups around Patel [
24] and El Naghy [
25] utilized superimposition exclusively, Okazaki et al. [
26] concentrated on intra-arch measurements, and Unnikrishnan et al. [
17] integrated both intra-arch measurements and surface discrepancy analyses to evaluate the accuracy of IOS compared to CIs. The authors demonstrated that there were no significant variations between the superimposed models created from the IOS and CIs in neonates with cleft lip and palate. The results were consistent regardless of cleft severity (size) or type (unilateral/bilateral). Furthermore, there were no significant differences in either the type of measurement or the compared impression variants (alginate, IOS, and putty), showing that IOS has comparable accuracy to CIs [
17]. The digital data acquired through IOS can be easily stored, shared, and accessed by other clinicians, improving communication and collaboration between practitioners and specialized healthcare centers. This facilitates a more efficient, streamlined digital workflow by eliminating the need for physical plaster models, saving storage space and reducing the risk of lost impressions or damaged plaster models [
15].
The most important advantage of IOS is in patient safety. CI taking carries several risks. The complex anatomy of the cleft area increases the likelihood of the impression material tearing during the process. Impression material left unnoticed in the cleft area can cause inflammation in the surrounding tissues. In severe cases, torn impression material may lead to aspiration and respiratory obstruction, necessitating immediate medical intervention [
14,
27]. IOS has not been associated with any risks or complications. It rarely happens that a patient bites the intraoral 3D scan tip during 3D scanning, but when it does occur, it results in a slight superficial irritation of the mucosae and will heal itself without any medical intervention [
16]. In particular, this new ability to take a risk-free impression allows for re-3D-scanning of anatomically challenging areas that are not optimally represented or that are, for cleft-related reasons, difficult to access to ensure optimal quality of the digital maxillary models. Completed in just a few minutes, yielding high-quality images of the individual jaw segment structures, IOS is a fast, accurate, and safe procedure.
Despite the advantages, the initial investment in intraoral 3D scanners can be prohibitively high. High-quality intraoral 3D scanners are cost-intensive, making them less accessible to small practices or solo practitioners. It is therefore difficult to implement this approach consistently in various healthcare facilities, especially in resource-limited environments. The need for regular software updates and maintenance further adds to the financial burden. It is worth considering that the quality of the intraoral 3D scan depends in particular on the respective intraoral 3D scanner. The size of the 3D scan tip, the speed of image generation and the software error correction algorithm can affect the intraoral 3D scan result. The 3D scan quality also relies on the patient’s cooperation. Movement intensity or screaming during IOS and the amount of saliva/mucus production can be influencing factors that reduce the 3D scan quality. Although IOS is generally user-friendly, it still requires a certain level of expertise and experience to obtain accurate and reliable results. The clinician must master the technique of IOS, manage issues such as motion artifacts, and ensure proper alignment of the 3D scanner within the patient’s mouth. The 3D scan tips for use in newborns with cleft lip and palate are not special but standard 3D scan tips, designed in size and shape for 3D-scanning adolescents and adults. Their use in this special field of application therefore requires some practice. Inadequate training or insufficient experience can lead to suboptimal 3D scans [
23].
Especially in the application for patients with cleft lip and palate, IOS may struggle with certain clinical situations. The depth of field of the intraoral 3D scanner poses a significant challenge when imaging deeper structures between the jaw segments within the cleft area. For a 3D scan to be considered successful, all jaw segments must be registered as a continuous surface. Occasionally, the software fails to identify the entire jaw as a contiguous structure, which can result in important sections being inadvertently removed from the final 3D scan, requiring the user to build virtual bridges. The digital data generated by IOS can be large and complex, requiring robust storage solutions and careful management. Secure data storage is critical, particularly when handling sensitive patient information. Moreover, compatibility between different 3D-scanning devices and digital analyzing software can be an issue, requiring practitioners to invest in standardized systems or risk encountering difficulties with data transfer. Digital data processing requires a properly functioning hardware and software connection and is therefore sensitive to network faults.
The OnyxCeph3™ software provides a wide range of patient- and case-related 2D and 3D imaging capabilities for use in everyday clinical dental and orthodontic practice. The digital analysis presented in this study is a new innovative model analysis created specifically for use with models of patients with unilateral cleft lip and palate and can easily be added to the existing OnyxCeph3™ basic version.
Several studies have investigated morphological changes in the maxilla based on measurements taken from plaster casts [
4,
5,
6,
7] or digitized plaster models [
8,
9,
10,
11,
12,
13]. The limitations of plaster casts in terms of patient safety, material-related inaccuracy, and level of detail have already been described. Digital impressions are a viable alternative as they are at least equal to conventional impressions in terms of accuracy [
17,
24,
25,
26] and superior in terms of patient safety, speed, and reproducibility [
14,
16,
27]. To complete the digital workflow, new digital measurement methods are essential for analyzing maxillary growth and measuring the jaw segments of patients with unilateral cleft lip and palate. With the advantages of intraoral 3D scanning mentioned above, digital measurement methods improve the accuracy and reproducibility of assessments, which is crucial for identifying anatomical variations associated with unilateral cleft conditions.
These advanced techniques allow for detailed maxillary analysis, enabling clinicians to capture subtle changes that might be overlooked in traditional methods. The ability to capture detailed surface textures also facilitates the measurement of relevant anatomical surface structures of the maxillary tissues, leading to improved clinical measurement outcomes. Intraoral 3D scanners can capture fine details of the mucosae tissues, providing highly accurate 3D representations without the risk of distortion or material shrinkage that can occur with plaster models. Since digital models are not dependent on manual techniques, such as mixing and pouring plaster, there is a reduced risk of human error. Accurate measurements are essential not only for treatment planning but also for tracking patient progress over time and assessing the effectiveness of interventions. Moreover, digital measuring methods streamline workflow and facilitate better communication among multidisciplinary teams.
As there is no need to cast alginate impressions or digitize plaster casts, model measurement can begin immediately once the digital 3D scan data set has been imported into the OnyxCeph3™ software. Therapy-relevant morphological changes can be assessed instantly after the 3D scan, and therapy can be adjusted accordingly. Since the digital model analysis takes limited time, the interdisciplinary coordination regarding the growth-related morphological changes in the maxilla of the newborn can be carried out directly during the patient’s appointment. Parents and caregivers can be directly involved in the treatment planning process, and follow-up appointments can be arranged directly. The ability to define reference planes using digital measurement enables new measurement methods.
As digitization continues, additional points, planes, and angles can be added to the digital analysis for even more detailed analysis. For long-term measurement studies, digital storage and unrestricted access to high-quality models even after many years of treatment is a great advantage. Further extensions of existing analyses can also be carried out in the future by duplicating the stored models on existing models, thus creating larger data pools for interdisciplinary studies. However, while the benefits of digital model analysis are undeniable, there are several challenges and limitations that need to be considered. As with IOS, the initial investment in analysis software can be prohibitive, particularly for smaller practices or solo practitioners with already existing analysis software. Using the digital model analysis means that the practitioner is dependent on technology. It requires functional computer and software conditions. Moreover, the presented computer-aided measurement method of unilateral cleft lip and palate models in OnyxCeph3TM assumes familiarity with the software, limiting accessibility for practitioners new to the tool. The digital model analysis additionally requires profound comprehension of the maxillary anatomy of patients with cleft lip and palate from the practitioner. Moreover, it hast to be considered the challenges in identifying measurement points when measuring models with cleft lip and palate include the anatomical complexity and variability of the cleft region. The irregularities in the structure of the soft tissues and the alveolar ridge can make it difficult to accurately locate consistent reference points. Variations in cleft severity and age-related structural changes can complicate the identification of measurement points. These factors can lead to measurement errors or inconsistencies. It may be helpful to conduct digital model analysis on colored intraoral scans to better detect anatomical landmarks. Moreover, patient-related factors, such as mouth opening and compliance, which are also influenced by comorbidities, play a role. Similarly, observer-related errors, such as scanning experience, can be relevant. Measurement-device-related errors, like measurement accuracy, must also be considered.
Most studies measuring models with cleft lip and palate are based on the landmarks established by Ashley-Montagu [
19] in 1934 using plaster casts of healthy subjects. These are typical anatomical landmarks on the mucosal surface of the upper jaw that could be related to the underlying bony structures. The points were first applied by Sillman [
20] and have since been widely used in many growth studies of patients with unilateral cleft lip and palate.
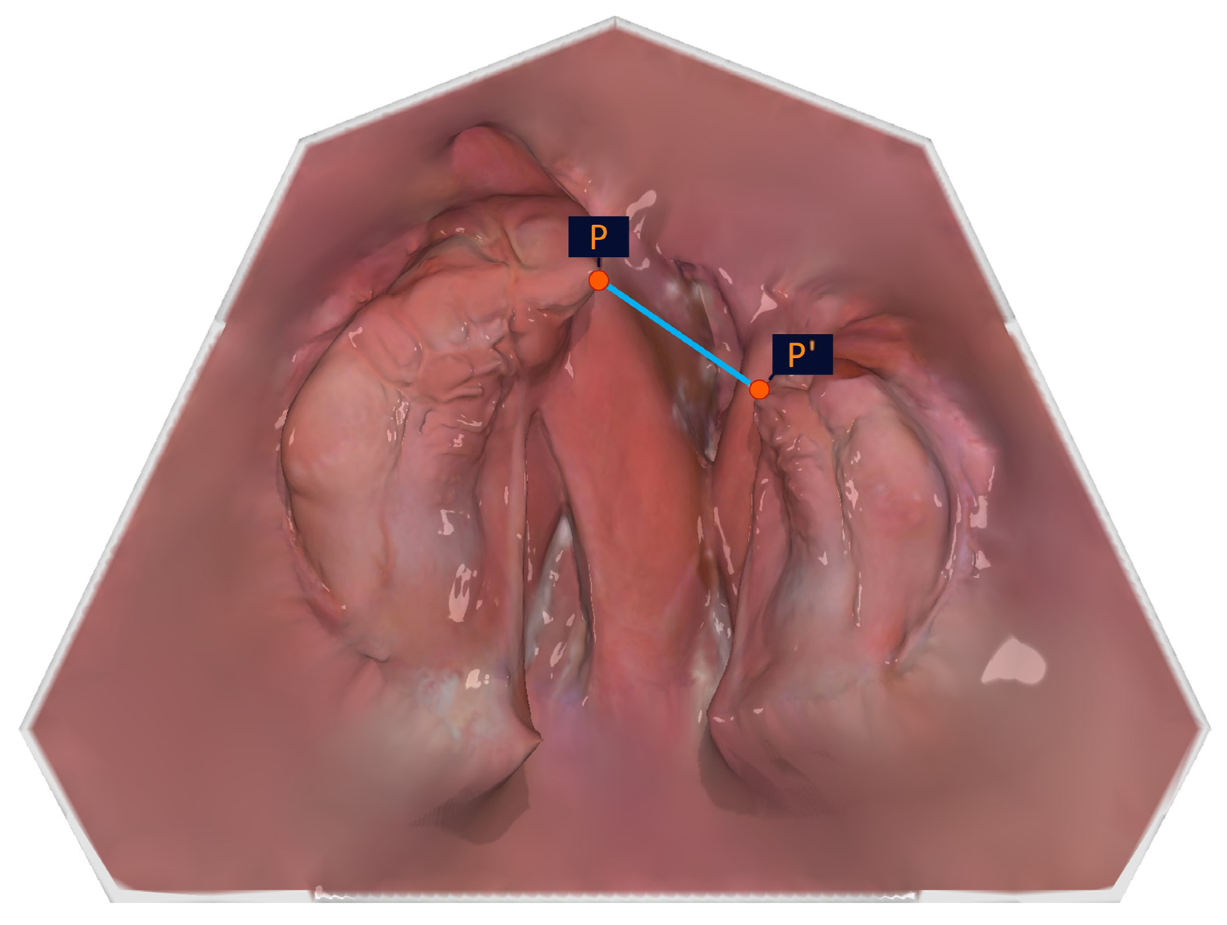
As the cleft edge of the crest of the alveolar ridge (large/small segment; P1/P2) does not represent the shortest distance between the large and the small segments in the pole region, it was important to the authors to include the outermost and foremost points of the alveolar ridge (points P and P′) in the analysis, which describe the closest approach of the segments.
The measurement of individual subsegment widths described in this approach has not previously been described in this way in the literature. Clearly reproducible points to measure are required for these measurements.
Since the vertical changes in the cleft cannot be assessed from the anatomical points alone without skull-related registration, a reference plane must be constructed. The original definition of a reference plane for the vertical analysis can also be referred to Ashley-Montagu [
19]. Defined by connecting the incisor and tuberosity points, he termed it the palatal plane (reference plane). In this context, the use of the incisor point in cleft patients is a challenge, as it is often unsuitable as a reference point due to distortion and delocalization. Therefore, in the vertical measurements, only the respective changes in the two mirrored points C2/C2′ and P1/P2 are considered in relation to each other. It should be mentioned, however, that if the vertical axis alternates in any of the three measuring points (T-T′-Inz), the reference plane is affected, and the distance measurements to the points to be examined (C-P1-P2-C′) are altered.
Previous studies on the measurement of models with cleft lip and palate vary in the number of measurement points and their terminology [
5,
10,
18,
19,
20,
28,
29]. Studies based on the manual measurement of plaster models from patients with cleft lip and palate often relied on tracing photographic enlargements of these models [
5,
20]. This method does not allow for the precise three-dimensional placement of measurement points. Furthermore, an analysis of cleft width, as presented in our study, is not feasible with this approach. The measurement points defining the smallest distance between the poles of the jaw segments are located in the cleft area. Depending on the angle of the photograph, an occlusal view may not accurately capture this region. Other authors, such as Ashley-Montague [
19], used a specially developed dental pantograph for projecting the measurement points of plaster models. This measurement method also comes with the aforementioned limitations. A study by Sillman [
20] based on manual measurement using calipers to measure the distance between various measurement points. However, measurements related to constructed reference planes, such as those achievable through digital measurement, cannot be implemented with this method.
A study by Braumann et al. [
10] is based on the digital measurement of digitized plaster models. While the cleft width is not measured in greater detail, additional measurement points are used, primarily for transverse analysis. Segment widths are not determined, but the alveolar ridges are divided into three-dimensional subsegments, and their volume is measured digitally. A 2020 study by Bruggink et al. [
28] measured digitized plaster models. Selected measurement distances were analyzed, but angle measurements and segment width measurements were not performed. In 2020, Batra et al. [
29] published a study on the digital measurement of intraoral scan data using MESH Labs and Ortho Analyzer software. However, the measurement distances used in the study did not include width measurements or specific cleft width measurements. A 2024 study by Tabellion et al. [
30] measured digitized plaster models using Onyx Ceph
3TM and presented the analysis of various measurement distances and angles. However, the methodology of the measurements and the detailed procedural approach were not evaluated in the study. A recent literature review by Unnikrishnan et al. [
17] from 2024 examines measurement studies based on digital impressions. Okazaki et al. [
26] found no significant dimensional differences in cleft width and alveolar ridge width measurements between 3D-printed models, digital models generated by IOS, and plaster models obtained through conventional impressions. Similarly, a study by Soliman et al. [
31] from 2024 reported no differences between 3D-printed models and plaster models for the same measurement distances. “A narrative review on non-invasive diagnostic tools for the analysis of dental arches in orofacial cleft patients” by Jorge et al. [
13] from 2022 concluded that digital measuring tools, which evaluate the dental arches of children with CLP, are reproducible and reliable. The studies presented, which are comparable to the measurement method we outlined, were based on the digital measurement of digitized plaster models. Ambrosio et al. [
32] evaluated in 2022 the volume of the dental arches in children with unilateral cleft lip and palate on digitized dental casts. Prado et al. [
33] measured in 2021 the surface changes in digitized plaster casts.
The various studies evaluating growth changes in the maxilla of patients with unilateral cleft lip and palate differ in the methodology of model acquisition, the number and nomenclature of measurement points, and the type of measurement used. Therefore, the choice of terms and the selection of anatomical points presented in this study do not constitute a general justification. We selected these points to ensure they are easily identifiable and accurately represent the features we wish to measure. To provide an accurate and generally comparable representation, the respective anatomical description is given. The digital analysis presented could also be supplemented with several additional useful points, measuring distances and angles. Therefore, it would be desirable in the future to establish a uniform digital measurement analysis with a consistent number of standardized, named, and defined measurement points, measuring distances and angles, across specialized centers in order to make the upper jaw measurements of patients with unilateral cleft lip and palate more comparable. A full digital workflow including digital model analysis is increasingly relevant for future directions, particularly due to its potential to integrate artificial intelligence (AI) and automate landmark identifications. As AI technologies advance, they can enhance the accuracy and efficiency of identifying and measuring critical anatomical structures, reducing the subjectivity and variability that can arise from manual landmark positioning. Automated landmark detection can streamline the analysis process, making it not only faster but also consistent, while AI algorithms can learn from large center-wide data sets to improve over time. This integration can significantly enhance the precision of digital model assessments, providing research with reliable, reproducible results that are essential for long-term studies and clinical applications, particularly in complex rehabilitations like in cleft lip and palate patients. Moreover, the ability to process large amounts of data can facilitate large-scale, longitudinal studies, fostering a deeper understanding of growth patterns and treatment outcomes in patients with cleft lip and palate.




 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}