

The Effects of 4-Week Respiratory Muscle Training on Cardiopulmonary Parameters and Cognitive Function in Male Patients with OSA

 ,
, 
 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Inclusion Criteria
2.3. Measurements
2.3.1. Anthropometric Characteristics and Body Composition
2.3.2. Pulmonary Function Test and Respiratory Muscle Strength
2.3.3. Physical Fitness Tests
2.3.4. Cognitive and Sleep Quality Assessment
2.3.5. Interventions Program
2.3.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eckert, D.J.; Malhotra, A. Pathophysiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.; Hunter, M.; Budgeon, C.; Murray, K.; Knuiman, M.; Hui, J.; Hillman, D.; Singh, B.; James, A. The prevalence and comorbidities of obstructive sleep apnea in middle-aged men and women: The Busselton Healthy Ageing Study. J. Clin. Sleep. Med. 2021, 17, 2029–2039. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Punjabi, N.M. The epidemiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef]
- Crivelli, L.; Palmer, K.; Calandri, I.; Guekht, A.; Beghi, E.; Carroll, W.; Frontera, J.; García-Azorín, D.; Westenberg, E.; Winkler, A.S.; et al. Changes in cognitive functioning after COVID-19: A systematic review and meta-analysis. Alzheimers Dement. 2022, 18, 1047–1066. [Google Scholar] [CrossRef]
- Krysta, K.; Bratek, A.; Zawada, K.; Stepańczak, R. Cognitive deficits in adults with obstructive sleep apnea compared to children and adolescents. J. Neural Transm. 2017, 124 (Suppl. S1), 187–201. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Vavougios, G.D.; Astara, K.; Mysiris, D.S.; Tsirimona, G.; Papayianni, E.; Boutlas, S.; Daniil, Z.; Hadjigeorgiou, G.; Bargiotas, P.; et al. The Impact of Different Exercise Modes in Fitness and Cognitive Indicators: Hybrid versus Tele-Exercise in Patients with Long Post-COVID-19 Syndrome. Brain Sci. 2024, 14, 693. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Simpson, L.; McArdle, N.; Eastwood, P.R.; Ward, K.L.; Cooper, M.N.; Wilson, A.C.; Hillman, D.R.; Palmer, L.J.; Mukherjee, S. Physical Inactivity Is Associated with Moderate-Severe Obstructive Sleep Apnea. J. Clin. Sleep. Med. 2015, 11, 1091–1099. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Pitris, K.; Constantinidou, F.; Adamide, T.; Frangopoulos, F.; Bargiotas, P. The impact of a 12-week tele-exercise program on cognitive function and cerebral oxygenation in patients with OSA: Randomized controlled trial-protocol study. Front. Sports Act. Living 2024, 6, 1418439. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Astara, K.; Karetsi, E.; Daniil, Z.; Gourgoulianis, K.I. Respiratory Muscle Strength as an Indicator of the Severity of the Apnea-Hypopnea Index: Stepping Towards the Distinction Between Sleep Apnea and Breath Holding. Cureus 2021, 13, e14015. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Kline, C.E.; Youngstedt, S.D. Effects of exercise training on sleep apnea: A meta-analysis. Lung 2014, 192, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Weaver, T.E.; Grunstein, R.R. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep. Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Weaver, T.E.; Sawyer, A.M. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: Implications for future interventions. Indian. J. Med. Res. 2010, 131, 245–258. [Google Scholar] [PubMed]
- Stavrou, V.T.; Astara, K.; Tourlakopoulos, K.N.; Papayianni, E.; Boutlas, S.; Vavougios, G.D.; Daniil, Z.; Gourgoulianis, K.I. Obstructive Sleep Apnea Syndrome: The Effect of Acute and Chronic Responses of Exercise. Front. Med. 2021, 8, 806924. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.; Karetsi, E.; Daniil, Z.; Gourgoulianis, K.I. 4 weeks exercise in obstructive sleep apnea syndrome patient with type 2 diabetes mellitus and without continuous positive airway pressure treatment: A case report. Sleep Med. Res. 2019, 10, 54–57. [Google Scholar] [CrossRef]
- Resneck, J.S., Jr. Revisions to the Declaration of Helsinki on Its 60th Anniversary: A Modernized Set of Ethical Principles to Promote and Ensure Respect for Participants in a Rapidly Innovating Medical Research Ecosystem. JAMA 2025, 333, 15–17. [Google Scholar] [CrossRef]
- Gleeson, M.; McNicholas, W.T. Bidirectional relationships of comorbidity with obstructive sleep apnoea. Eur. Respir. Rev. 2022, 31, 210256. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Astara, K.; Daniil, Z.; Gourgoulianis, K.I.; Kalabakas, K.; Karagiannis, D.; Basdekis, G. The reciprocal association between fitness indicators and sleep quality in the context of recent sport injury. Int. J. Environ. Res. Public Health 2020, 17, 4810. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Tourlakopoulos, K.N.; Daniil, Z.; Gourgoulianis, K.I. Respiratory Muscle Strength: New Technology for Easy Assessment. Cureus 2021, 13, e14803. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.T.; Astara, K.; Ioannidis, P.; Vavougios, G.D.; Daniil, Z.; Gourgoulianis, K.I. Tele-Exercise in Non-Hospitalized versus Hospitalized Post-COVID-19 Patients. Sports 2022, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Mosteller, R.D. Simplified Calculation of Body-Surface Area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar]
- Rauter, S.; Simenko, J. Morphological Asymmetries Profile and the Difference between Low- and High-Performing Road Cyclists Using 3D Scanning. Biology 2021, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, I.M.; Houri Neto, M.; Montemezzo, D.; Silva, L.A.; Andrade, A.D.; Parreira, V.F. Predictive equations for respiratory muscle strength according to international and Brazilian guidelines. Braz. J. Phys. Ther. 2014, 18, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.; Boutou, A.K.; Vavougios, G.D.; Pastaka, C.; Gourgoulianis, K.I.; Koutedakis, Y.; Daniil, Z.; Karetsi, E. The use of cardiopulmonary exercise testing in identifying the presence of obstructive sleep apnea syndrome in patients with compatible symptomatology. Respir. Physiol. Neurobiol. 2019, 262, 26–31. [Google Scholar] [CrossRef] [PubMed]
- DeMers, D.; Wachs, D. Physiology, Mean Arterial Pressure. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.T.; Karetsi, E.; Gourgoulianis, K.I. The Effect of Growth and Body Surface Area on Cardiopulmonary Exercise Testing: A Cohort Study in Preadolescent Female Swimmers. Children 2023, 10, 1608. [Google Scholar] [CrossRef]
- Scholkmann, F.; Wolf, U. The Pulse-Respiration Quotient: A Powerful but Untapped Parameter for Modern Studies About Human Physiology and Pathophysiology. Front. Physiol. 2019, 10, 371. [Google Scholar] [CrossRef]
- Stavrou, V.; Vavougios, G.D.; Bardaka, F.; Karetsi, E.; Daniil, Z.; Gourgoulianis, K.I. The effect of exercise training on the quality of sleep in national-level adolescent finswimmers. Sports Med. Open 2019, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699, Erratum in J. Am. Geriatr. Soc. 2019, 67, 1991. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, K.; Baril, A.A.; Gagnon, J.F.; Fortin, M.; Décary, A.; Lafond, C.; Desautels, A.; Montplaisir, J.; Gosselin, N. Cognitive impairment in obstructive sleep apnea. Pathol. Biol. 2014, 62, 233–240. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Papayianni, E.; Astara, K.; Vavougios, G.D.; Kontogianni, M.D.; Bargiota, A.; Pastaka, C.; Daniil, Z.; Gourgoulianis, K.I. Tele-Pulmonary Rehabilitation and Mediterranean-like Lifestyle, Adjunctively to Continuous Positive Airway Pressure in Obstructive Sleep Apnea Patients: Effects in Fitness and Oxidative Indicators. Appl. Sci. 2024, 14, 8424. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Griziotis, M.; Vavougios, G.D.; Raptis, D.G.; Bardaka, F.; Karetsi, E.; Kyritsis, A.; Daniil, Z.; Tsarouhas, K.; Triposkiadis, F.; et al. Supervised Versus Unsupervised Pulmonary Rehabilitation in Patients with Pulmonary Embolism: A Valuable Alternative in COVID Era. J. Funct. Morphol. Kinesiol. 2021, 6, 98. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Tourlakopoulos, K.N.; Vavougios, G.D.; Papayianni, E.; Kiribesi, K.; Maggoutas, S.; Nikolaidis, K.; Fradelos, E.C.; Dimeas, I.; Daniil, Z.; et al. Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 806. [Google Scholar] [CrossRef]
- Somers, V.K.; Dyken, M.E.; Mark, A.L.; Abboud, F.M. Sympathetic-nerve activity during sleep in normal subjects. N. Engl. J. Med. 1993, 328, 303–307. [Google Scholar] [CrossRef]
- de Abreu, R.M.; Rehder-Santos, P.; Minatel, V.; Dos Santos, G.L.; Catai, A.M. Effects of inspiratory muscle training on cardiovascular autonomic control: A systematic review. Auton. Neurosci. 2017, 208, 29–35. [Google Scholar] [CrossRef]
- Stavrou, V.; Voutselas, V.; Karetsi, E.; Gourgoulianis, K.I. Acute responses of breathing techniques in maximal inspiratory pressure. Sport Sci. Health 2018, 14, 91–95. [Google Scholar] [CrossRef]
- Matić, Z.; Kalauzi, A.; Moser, M.; Platiša, M.M.; Lazarević, M.; Bojić, T. Pulse respiration quotient as a measure sensitive to changes in dynamic behavior of cardiorespiratory coupling such as body posture and breathing regime. Front. Physiol. 2022, 13, 946613. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, R.J.S.; Band, G.P.H. Breath of Life: The Respiratory Vagal Stimulation Model of Contemplative Activity. Front. Hum. Neurosci. 2018, 12, 397. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.D.; Dal Lago, P.; da Silva Soares, P.P. Inspiratory muscle training improves breathing pattern and sympatho-vagal balance but not spontaneous baroreflex sensitivity in older women. Respir. Physiol. Neurobiol. 2021, 290, 103672. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.T.; Vavougios, G.D.; Hadjigeorgiou, G.M.; Bargiotas, P. The Effect of Physical Exercise on Patients With Mild Cognitive Impairment: A Scoping Review. Cureus 2024, 16, e73265. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, V.T.; Kyriaki, A.; Vavougios, G.D.; Fatouros, I.G.; Metsios, G.S.; Kalabakas, K.; Karagiannis, D.; Daniil, Z.; IGourgoulianis, K.; Βasdekis, G. Athletes with mild post-COVID-19 symptoms experience increased respiratory and metabolic demands: A cross-sectional study. Sports Med. Health Sci. 2023, 5, 106–111. [Google Scholar] [CrossRef]
- Zhang, H.; Guo, Z.; Qu, Y.; Zhao, Y.; Yang, Y.; Du, J.; Yang, C. Cognitive function and brain activation before and after transcutaneous cervical vagus nerve stimulation in healthy adults: A concurrent tcVNS-fMRI study. Front. Psychol. 2022, 13, 1003411. [Google Scholar] [CrossRef] [PubMed]
- Magnon, V.; Dutheil, F.; Vallet, G.T. Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Sci. Rep. 2021, 11, 19267. [Google Scholar] [CrossRef]
- Hughes, C.M.; McCullough, C.A.; Bradbury, I.; Boyde, C.; Hume, D.; Yuan, J.; Quinn, F.; McDonough, S.M. Acupuncture and reflexology for insomnia: A feasibility study. Acupunct. Med. 2009, 4, 163–168. [Google Scholar] [CrossRef]
- Silva de Sousa, A.; Pereira da Rocha, A.; Brandão Tavares, D.R.; Frazão Okazaki, J.É.; de Andrade Santana, M.V.; Fernandes Moça Trevisani, V.; Pereira Nunes Pinto, A.C. Respiratory muscle training for obstructive sleep apnea: Systematic review and meta-analysis. J. Sleep Res. 2024, 33, e13941. [Google Scholar] [CrossRef]
- Stavrou, V.; Bardaka, F.; Karetsi, E.; Daniil, Z.; Gourgoulianis, K.I. Brief Review: Ergospirometry in Patients with Obstructive Sleep Apnea Syndrome. J. Clin. Med. 2018, 7, 191. [Google Scholar] [CrossRef]
- Wang, W.; Li, R.; Li, C.; Liang, Q.; Gao, X. Advances in VNS efficiency and mechanisms of action on cognitive functions. Front. Physiol. 2024, 15, 1452490. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Song, L.; Wang, X.; Li, N.; Zhan, S.; Rong, P.; Wang, Y.; Liu, A. Transcutaneous Vagus Nerve Stimulation Could Improve the Effective Rate on the Quality of Sleep in the Treatment of Primary Insomnia: A Randomized Control Trial. Brain Sci. 2022, 12, 1296. [Google Scholar] [CrossRef] [PubMed]
- Vranish, J.R.; Bailey, E.F. Inspiratory Muscle Training Improves Sleep and Mitigates Cardiovascular Dysfunction in Obstructive Sleep Apnea. Sleep 2016, 39, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Hsu, B.; Emperumal, C.P.; Grbach, V.X.; Padilla, M.; Enciso, R. Effects of respiratory muscle therapy on obstructive sleep apnea: A systematic review and meta-analysis. J. Clin. Sleep Med. 2020, 16, 785–801. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Tanuma, T. The effect of nasal and oral breathing on airway collapsibility in patients with obstructive sleep apnea: Computational fluid dynamics analyses. PLoS ONE 2020, 15, e0231262. [Google Scholar] [CrossRef]
 Baseline RMTgroup;
Baseline RMTgroup;  After 4-week RMTgroup;
After 4-week RMTgroup;  Baseline CPAPgroup;
Baseline CPAPgroup;  After 4-week CPAPgroup. # p < 0.001, * p < 0.05 between baseline and after 4-week, ^ p < 0.001, ‡ p < 0.05 between groups.
Baseline RMTgroup; After 4-week RMTgroup; Baseline CPAPgroup; After 4-week CPAPgroup. # p < 0.001, * p < 0.05 between baseline and after 4-week, ^ p < 0.001, ‡ p < 0.05 between groups.
After 4-week CPAPgroup. # p < 0.001, * p < 0.05 between baseline and after 4-week, ^ p < 0.001, ‡ p < 0.05 between groups.
Baseline RMTgroup; After 4-week RMTgroup; Baseline CPAPgroup; After 4-week CPAPgroup. # p < 0.001, * p < 0.05 between baseline and after 4-week, ^ p < 0.001, ‡ p < 0.05 between groups.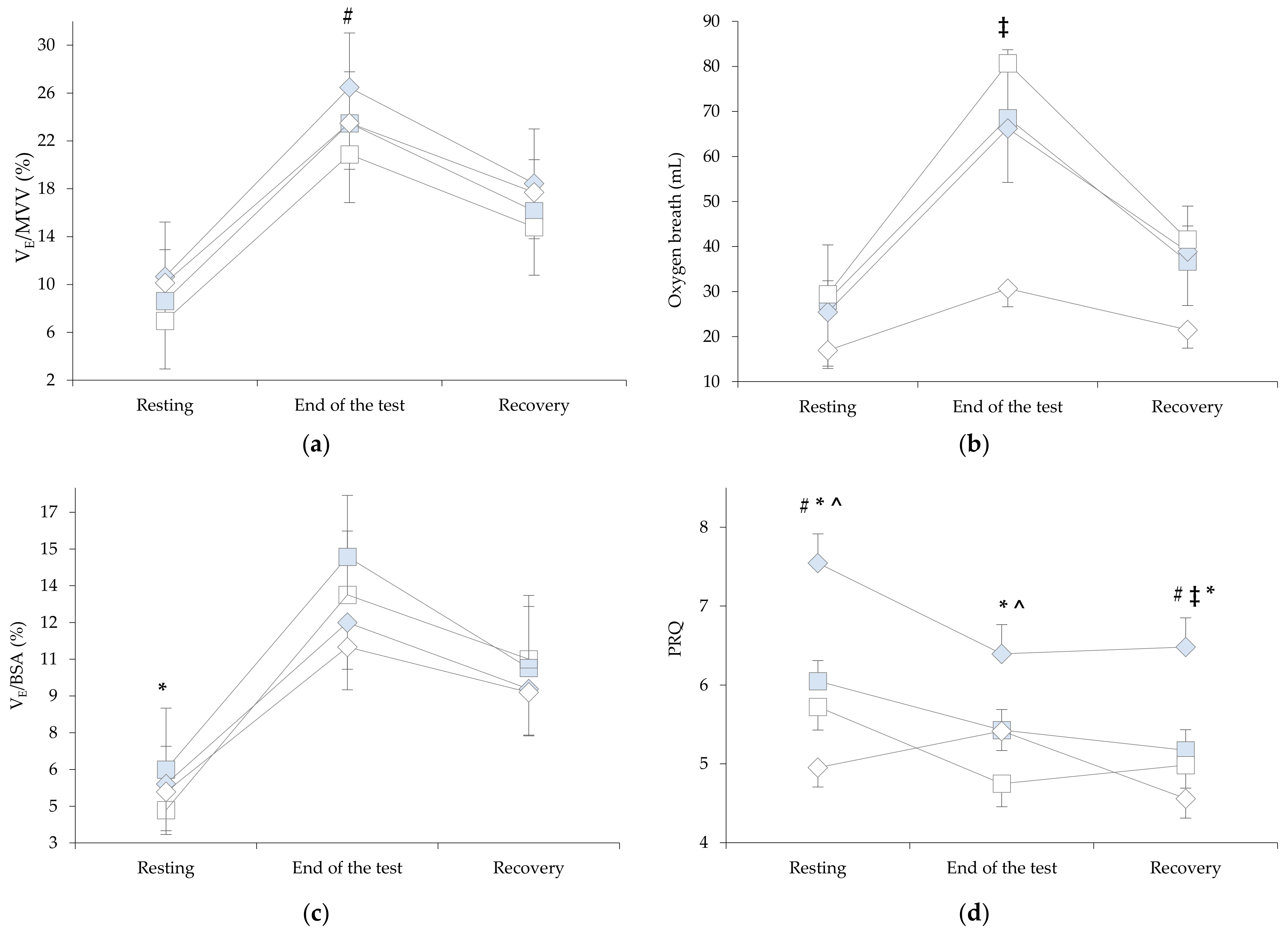
 Baseline RMTgroup;
Baseline RMTgroup;  After 4-week RMTgroup;
After 4-week RMTgroup;  Baseline CPAPgroup;
Baseline CPAPgroup;  After 4-week CPAPgroup. * p < 0.05 between baseline and after 4-week.
Baseline RMTgroup; After 4-week RMTgroup; Baseline CPAPgroup; After 4-week CPAPgroup. * p < 0.05 between baseline and after 4-week.
After 4-week CPAPgroup. * p < 0.05 between baseline and after 4-week.
Baseline RMTgroup; After 4-week RMTgroup; Baseline CPAPgroup; After 4-week CPAPgroup. * p < 0.05 between baseline and after 4-week.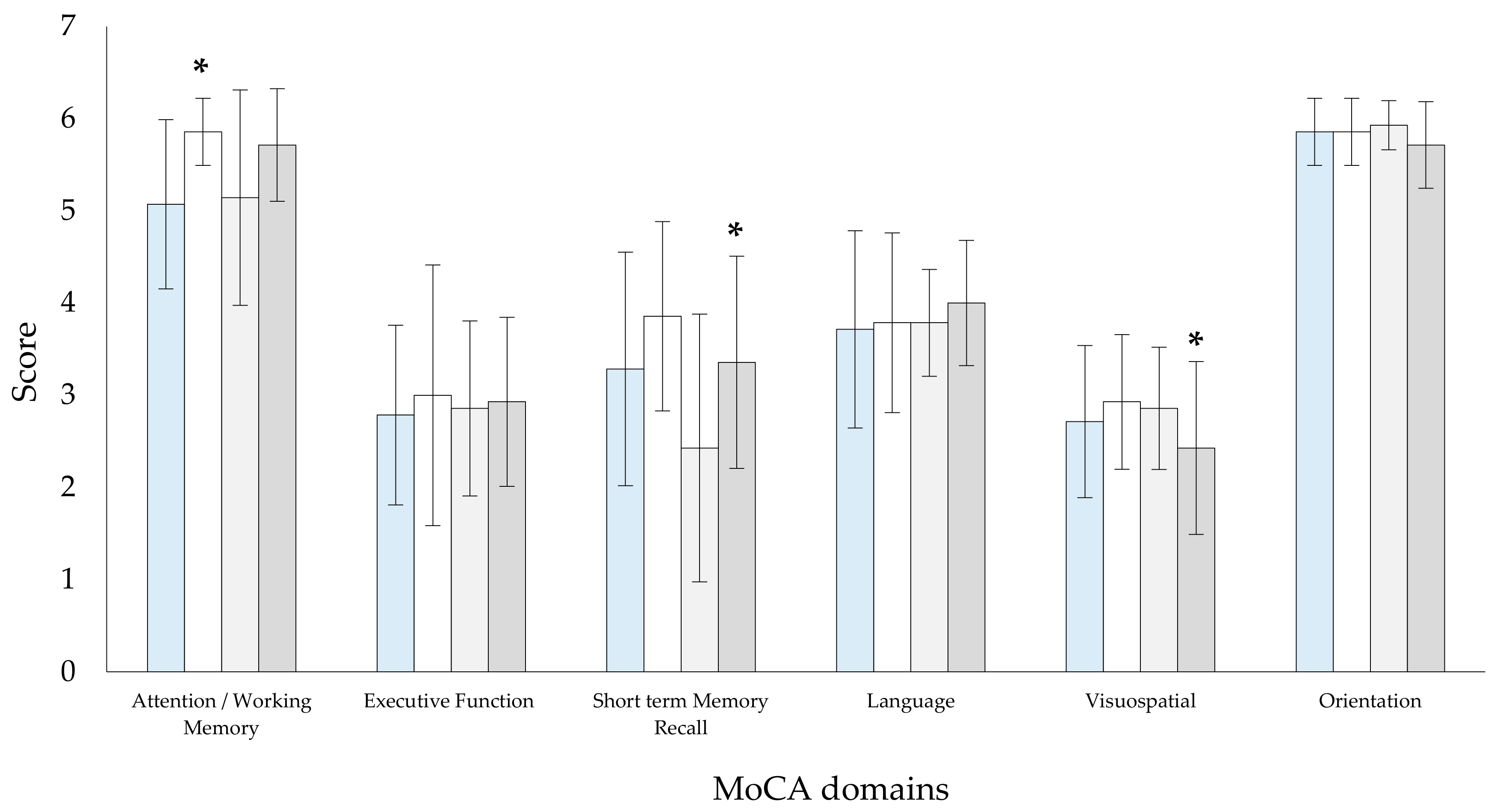

{kind=link}
{kind=link}
{kind=link}
| RMTgroup | CPAPgroup | p-Value Between Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Unit | Baseline | After 4 Weeks | p-Value | 95% CI | Baseline | After 4-Week | p-Value | 95% CI | Baseline | After 4 Weeks |
| Age | years | 51.3 ± 9.6 | - | - | - | 56.2 ± 5.9 | - | - | - | 0.114 | - |
| Apnea hypopnea index | events/h | 22.4 ± 7.0 | - | - | - | 26.5 ± 5.5 | - | - | - | 0.056 | - |
| Desaturation index | % | 16.1 ± 9.9 | - | - | - | 18.5 ± 4.7 | - | - | - | 0.205 | - |
| Body mass index | kg/m2 | 30.0 ± 7.4 | 29.9 ± 7.6 | 0.709 | −0.425 to 0.625 | 32.5 ± 6.1 | 32.5 ± 6.0 | 0.472 | −0.335 to 0.724 | 0.337 | 0.336 |
| Body surface area | m2 | 2.2 ± 0.6 | 2.2 ± 0.6 | 0.336 | −0.400 to 0.588 | 2.4 ± 0.4 | 2.4 ± 0.3 | 0.165 | −0.158 to 0.931 | 0.350 | 0.348 |
| Fat mass index | kg/m2 | 10.7 ± 7.0 | 10.2 ± 6.5 | 0.656 | −0.271 to 0.796 | 10.9 ± 5.9 | 11.7 ± 6.3 | 0.197 | −0.899 to 0.185 | 0.940 | 0.556 |
| Muscle mass index | kg/m2 | 8.8 ± 4.4 | 8.9 ± 3.2 | 0.669 | −0.255 to 0.749 | 10.3 ± 3.5 | 10.3 ± 3.5 | 0.446 | −0.324 to 0.736 | 0.330 | 0.328 |
| Basic metabolic rate | kcal | 1814.6 ± 216.4 | 1812.4 ± 219.7 | 0.684 | −0.410 to 0.642 | 1805.1 ± 157.2 | 1802.3 ± 149.0 | 0.414 | −0.309 to 0.752 | 0.895 | 0.887 |
| Total body water | % | 50.1 ± 6.0 | 50.2 ± 6.1 | 0.681 | −0.386 to 0.604 | 49.0 ± 4.4 | 49.0 ± 4.4 | 0.466 | −0.726 to 0.333 | 0.554 | 0.557 |
| Neck circumference | cm | 38.4 ± 4.7 | 38.5 ± 4.2 | 0.807 | −0.410 to 0.642 | 39.6 ± 3.3 | 39.9 ± 3.0 | 0.770 | −0.603 to 0.446 | 0.464 | 0.335 |
| Waist—hip ratio | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.488 | −0.386 to 0.604 | 1.0 ± 0.1 | 1.0 ± 0.1 | 0.870 | −0.568 to 0.480 | 0.166 | 0.057 | |
| Δchest | cm | 6.3 ± 2.6 | 6.5 ± 1.7 | 0.684 | −0.416 to 0.635 | 6.1 ± 3.5 | 5.4 ± 1.8 | 0.418 | −0.311 to 0.750 | 0.565 | 0.094 |
| FEV1 | % predicted | 99.2 ± 14.6 | 97.0 ± 14.5 | 0.197 | −0.185 to 0.899 | 91.8 ± 13.8 | 93.7 ± 13.6 | 0.615 | −0.662 to 0.391 | 0.181 | 0.306 |
| DLCO | % predicted | 107.1 ± 16.9 | 106.1 ± 18.7 | 0.679 | −0.415 to 0.636 | 111.6 ± 13.8 | 109.1 ± 17.0 | 0.135 | −0.130 to 0.966 | 0.454 | 0.534 |
| TLC | % predicted | 84.2 ± 9.7 | 90.4 ± 11.8 | 0.087 | −1.043 to 0.071 | 83.1 ± 11.4 | 84.0 ± 14.9 | 0.752 | −0.610 to 0.440 | 0.793 | 0.169 |
| MIP | % predicted | 95.1 ± 23.1 | 105.9 ± 31.0 | 0.028 | −1.232 to −0.070 | 107.1 ± 24.2 | 104.5 ± 25.7 | 0.575 | −0.376 to 0.678 | 0.196 | 0.969 |
| MEP | % predicted | 108.7 ± 31.4 | 127.9 ± 46.7 | 0.022 | −1.268 to −0.095 | 111.9 ± 24.6 | 105.7 ± 27.2 | 0.465 | −0.332 to 0.727 | 0.781 | 0.151 |
| PSQI | score | 11.1 ± 5.8 | 9.1 ± 5.1 | 0.013 | 0.082 to 1.248 | 6.1 ± 4.6 | 7.0 ± 5.9 | 0.122 | −0.859 to 0.271 | 0.018 | 0.331 |
| MoCA | score | 23.4 ± 3.0 | 25.3 ± 2.4 | <0.001 | −2.033 to −0.582 | 23.0 ± 2.9 | 24.1 ± 2.3 | 0.054 | −1.006 to 0.099 | 0.708 | 0.211 |
| RMTgroup | CPAPgroup | p-Value Between Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Stage | Variable | Unit | Baseline | After 4-Week | p-Value | 95% CI | Baseline | After 4 Weeks | p-Value | 95% CI | Baseline | After 4 Weeks |
| Resting | VO2 | mL/min | 359.7 ± 134.3 | 316.6 ± 135.8 | 0.042 | −0.066 to 1.048 | 346.4 ± 121.6 | 331.4 ± 75.9 | 0.328 | −0.406 to 0.645 | 0.786 | 0.726 |
| VCO2 | mL/min | 294.4 ± 101.8 | 262.4 ± 105.2 | 0.087 | −0.167 to 0.920 | 318.5 ± 130.5 | 303.4 ± 81.9 | 0.338 | −0.414 to 0.638 | 0.591 | 0.260 | |
| Tidal volume | L | 0.7 ± 0.3 | 0.7 ± 0.1 | 0.391 | −0.450 to 0.599 | 0.7 ± 0.3 | 0.7 ± 0.2 | 0.168 | −0.795 to 0.272 | 0.324 | 0.629 | |
| Breath frequency | 1/min | 14.6 ± 4.3 | 10.9 ± 2.2 | <0.001 | 0.477 to 1.857 | 14.5 ± 3.4 | 15.6 ± 2.7 | 0.056 | −1.000 to 0.104 | 0.923 | <0.001 | |
| PETCO2 | mmHg | 33.7 ± 5.3 | 33.6 ± 5.4 | 0.476 | −0.508 to 0.540 | 32.3 ± 5.1 | 32.6 ± 3.3 | 0.401 | −0.592 to 0.457 | 0.471 | 0.532 | |
| PETO2 | mmHg | 106.6 ± 9.1 | 105.6 ± 10.3 | 0.500 | −0.524 to 0.524 | 111.6 ± 7.4 | 111.9 ± 7.0 | 0.445 | −0.561 to 0.487 | 0.117 | 0.124 | |
| Heart rate | % predicted | 43.0 ± 8.2 | 43.1 ± 4.6 | 0.166 | −0.270 to 0.798 | 45.0 ± 5.5 | 45.0 ± 6.1 | 0.933 | −0.546 to 0.501 | 0.462 | 0.171 | |
| MAP | mmHg | 95.3 ± 7.9 | 91.3 ± 7.7 | 0.131 | −0.230 to 0.844 | 94.1 ± 7.5 | 93.7 ± 8.6 | 0.875 | −0.482 to 0.566 | 0.717 | 0.211 | |
| End test | VO2 | mL/min | 1356.0 ± 453.1 | 1355.6 ± 453.0 | 0.497 | −0.522 to 0.526 | 1392.1 ± 494.2 | 1312.5 ± 310.3 | 0.163 | −0.266 to 0.802 | 0.842 | 0.771 |
| % predicted | 53.3 ± 18.6 | 52.1 ± 17.8 | 0.205 | −0.755 to 0.307 | 58.3 ± 15.1 | 55.7 ± 10.9 | 0.410 | −0.307 to 0.754 | 0.456 | 0.343 | ||
| VCO2 | mL/min | 1071.0 ± 363.3 | 1121.8 ± 376.1 | 0.234 | −0.726 to 0.333 | 1089.6 ± 386.7 | 1038.1 ± 273.7 | 0.145 | −0.246 to 0.825 | 0.896 | 0.507 | |
| Tidal volume | L | 1.7 ± 0.7 | 1.6 ± 0.6 | 0.321 | −0.401 to 0.651 | 1.7 ± 0.6 | 1.7 ± 0.5 | 0.466 | −0.547 to 0.501 | 0.883 | 0.611 | |
| Breath frequency | 1/min | 20.5 ± 4.1 | 16.9 ± 2.3 | 0.001 | 0.365 to 1.675 | 21.4 ± 5.6 | 19.7 ± 5.4 | 0.144 | −0.245 to 0.827 | 0.621 | 0.089 | |
| PETCO2 | mmHg | 40.9 ± 5.6 | 41.9 ± 6.7 | 0.191 | −0.770 to 0.294 | 41.2 ± 6.0 | 41.8 ± 4.3 | 0.198 | −0.762 to 0.301 | 0.974 | 0.973 | |
| PETO2 | mmHg | 96.9 ± 7.8 | 97.9 ± 8.8 | 0.266 | −0.696 to 0.360 | 96.6 ± 7.4 | 95.5 ± 8.4 | 0.276 | −0.367 to 0.688 | 0.941 | 0.463 | |
| Heart rate | % predicted | 56.4 ± 8.9 | 57.6 ± 15.7 | 0.148 | −0.820 to 0.250 | 54.3 ± 6.8 | 55.7 ± 6.7 | 0.295 | −0.822 to 0.249 | 0.467 | 0.246 | |
| MAP | mmHg | 100.7 ± 4.9 | 91.9 ± 15.7 | 0.035 | −0.042 to 1.081 | 95.4 ± 6.9 | 101.9 ± 8.0 | 0.032 | −1.211 to −0.055 | 0.030 | 0.022 | |
| Recovery | VO2 | mL/min | 613.1 ± 249.9 | 590.7 ± 253.0 | 0.239 | −0.338 to 0.720 | 650.9 ± 235.3 | 648.4 ± 177.7 | 0.474 | −0.506 to 0.541 | 0.680 | 0.492 |
| VCO2 | mL/min | 715.3 ± 286.9 | 731.5 ± 253.0 | 0.378 | −0.608 to 0.442 | 729.2 ± 345.8 | 713.9 ± 267.0 | 0.374 | −0.439 to 0.611 | 0.909 | 0.872 | |
| Tidal volume | L | 1.2 ± 0.6 | 1.2 ± 0.4 | 0.169 | −0.273 to 0.794 | 1.3 ± 0.6 | 1.1 ± 0.4 | 0.172 | −0.791 to 0.276 | 0.193 | 0.911 | |
| Breath frequency | 1/min | 18.5 ± 4.8 | 14.4 ± 2.3 | 0.001 | 0.327 to 1.614 | 17.4 ± 4.3 | 19.4 ± 4.5 | 0.045 | −1.039 to 0.074 | 0.537 | 0.001 | |
| PETCO2 | mmHg | 38.4 ± 5.9 | 37.1 ± 7.1 | 0.500 | −0.524 to 0.524 | 38.4 ± 2.8 | 37.9 ± 4.2 | 0.500 | −0.524 to 0.524 | 0.989 | 0.991 | |
| PETO2 | mmHg | 111.4 ± 5.4 | 113.6 ± 6.2 | 0.054 | −1.045 to 0.069 | 109.9 ± 6.7 | 110.3 ± 7.3 | 0.348 | −0.630 to 0.421 | 0.519 | 0.200 | |
| Heart rate | % predicted | 46.6 ± 9.0 | 48.9 ± 6.8 | 0.173 | −0.277 to 0.790 | 46.0 ± 4.9 | 48.3 ± 7.0 | 0.130 | −0.973 to 0.125 | 0.835 | 0.425 | |
| MAP | mmHg | 94.7 ± 7.1 | 92.8 ± 8.2 | 0.163 | −0.266 to 0.802 | 90.7 ± 7.7 | 98.4 ± 7.8 | 0.011 | −1.378 to −0.172 | 0.177 | 0.035 | |
| 30 s StS test | repetitions | 17.4 ± 3.7 | 18.6 ± 3.8 | 0.064 | −0.977 to 0.122 | 14.2 ± 5.1 | 15.1 ± 4.4 | 0.097 | −1.025 to 0.084 | 0.073 | 0.018 | |
| Handgrip test | kg | 39.0 ± 14.1 | 39.8 ± 15.4 | 0.251 | −0.710 to 0.347 | 38.5 ± 13.5 | 37.7 ± 13.2 | 0.438 | −0.483 to 0.532 | 0.914 | 0.704 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stavrou, V.T.; Vavougyios, G.D.; Tsirimona, G.; Boutlas, S.; Santo, M.; Hadjigeorgiou, G.; Bargiotas, P.; Gourgoulianis, K.I. The Effects of 4-Week Respiratory Muscle Training on Cardiopulmonary Parameters and Cognitive Function in Male Patients with OSA. Appl. Sci. 2025, 15, 2532. https://doi.org/10.3390/app15052532
Stavrou VT, Vavougyios GD, Tsirimona G, Boutlas S, Santo M, Hadjigeorgiou G, Bargiotas P, Gourgoulianis KI. The Effects of 4-Week Respiratory Muscle Training on Cardiopulmonary Parameters and Cognitive Function in Male Patients with OSA. Applied Sciences. 2025; 15(5):2532. https://doi.org/10.3390/app15052532
Chicago/Turabian StyleStavrou, Vasileios T., George D. Vavougyios, Glykeria Tsirimona, Stylianos Boutlas, Marinela Santo, Georgios Hadjigeorgiou, Panagiotis Bargiotas, and Konstantinos I. Gourgoulianis. 2025. "The Effects of 4-Week Respiratory Muscle Training on Cardiopulmonary Parameters and Cognitive Function in Male Patients with OSA" Applied Sciences 15, no. 5: 2532. https://doi.org/10.3390/app15052532
APA StyleStavrou, V. T., Vavougyios, G. D., Tsirimona, G., Boutlas, S., Santo, M., Hadjigeorgiou, G., Bargiotas, P., & Gourgoulianis, K. I. (2025). The Effects of 4-Week Respiratory Muscle Training on Cardiopulmonary Parameters and Cognitive Function in Male Patients with OSA. Applied Sciences, 15(5), 2532. https://doi.org/10.3390/app15052532