
Marginal Bone Loss Around Bone-Level and Tissue-Level Implants: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. PICO Question
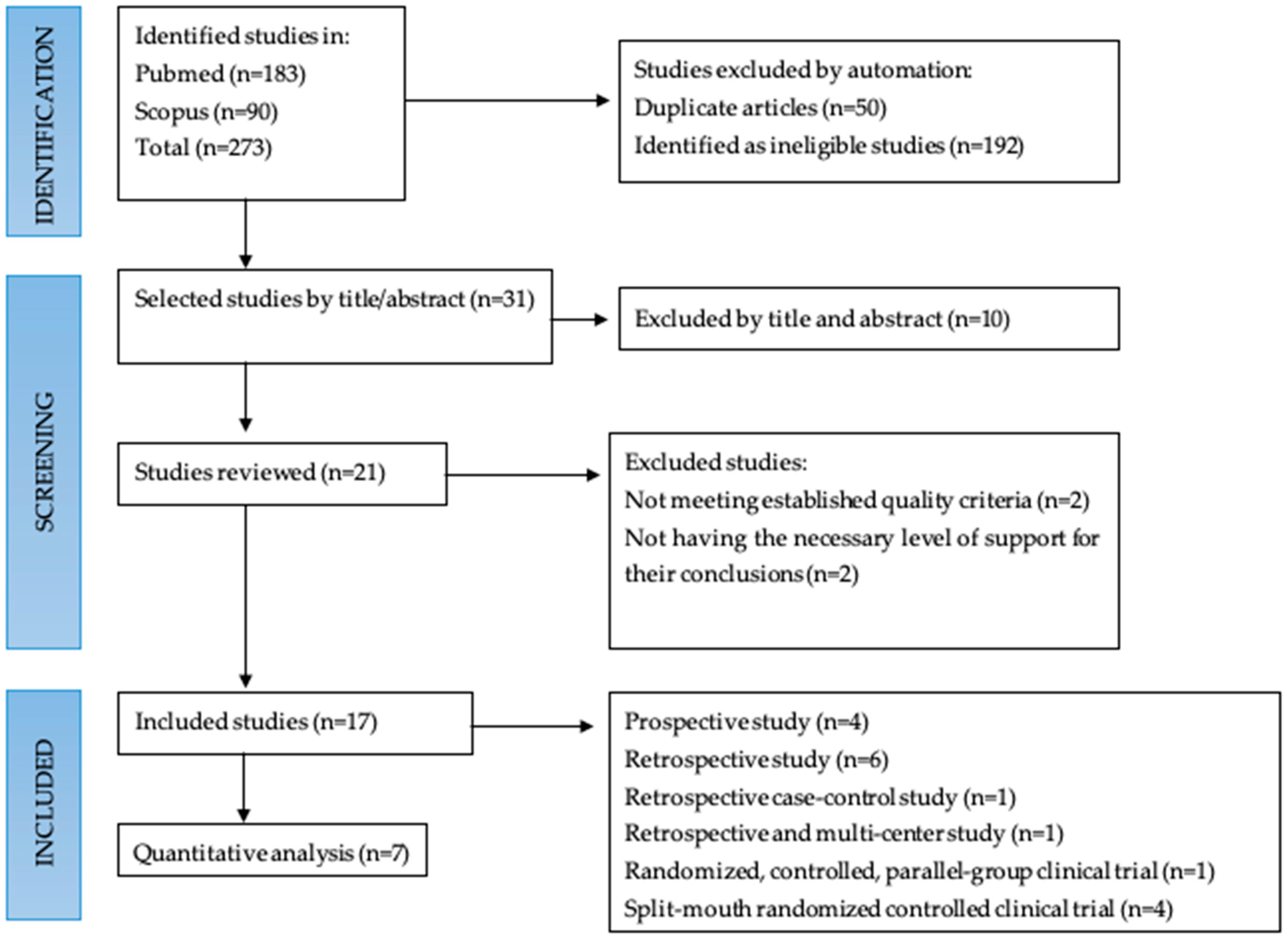
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Quality Assessment
2.6. Data Extraction
2.7. Data Synthesis
3. Results
3.1. Bias Analysis
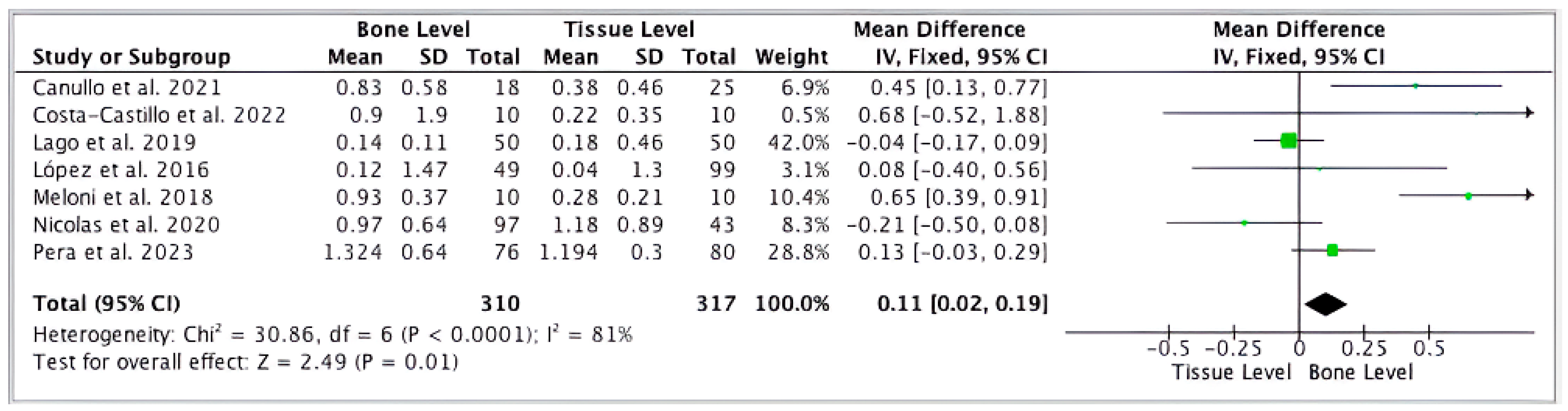
3.2. Comparative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alghamdi, H.S.; Jansen, J.A. The development and future of dental implants. Dent. Mater. J. 2020, 39, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Sargozaie, N.; Moeintaghavi, A.; Shojaie, H. Comparing the Quality of Life of Patients Requesting Dental Implants Before an After Implant. Open Dent. J. 2017, 11, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef]
- Heydecke, G.; Locker, D.; Awad, M.A.; Lund, J.P.; Feine, J.S. Oral and general health-related quality of life with conventional and implant dentures. Community Dent. Oral Epidemiol. 2003, 31, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar]
- Zarb, G.A.; Albrektsson, T. Osseointegration: A requiem for the periodontal ligament? Int. J. Periodontics Restor. Dent. 1991, 11, 88–91. [Google Scholar]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- French, D.; Ofec, R.; Levin, L. Long term clinical performance of 10 871 dental implants with up to 22 years of follow-up: A cohort study in 4247 patients. Clin. Implant Dent. Relat. Res. 2021, 23, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Raikar, S.; Talukdar, P.; Kumari, S.; Panda, S.K.; Oommen, V.M.; Prasad, A. Factors Affecting the Survival Rate of Dental Implants: A Retrospective Study. J. Int. Soc. Prev. Community Dent. 2017, 7, 351–355. [Google Scholar] [CrossRef] [PubMed]
- French, D.; Clark-Perry, D.; Ofec, R.; Levin, L. Radiographic bone loss around dental implants: A large-cohort, long-term follow-up revealing prevalence and predictive factors. Quintessence Int. 2024, 55, 296–303. [Google Scholar] [PubMed]
- Hermann, J.S.; Cochran, D.L.; Nummikoski, P.V.; Buser, D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded non-submerged and submerged implants in the canine mandible. J. Periodontol. 1997, 68, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Mantena, S.R.; Sivagami, G.; Gottumukkala, S.N. Evaluation of crestal bone loss and stability of immediate functional loading versus immediate non-functional loading of single-mandibular posterior implants: A pilot randomized controlled clinical trial. Dent. Res. J. 2014, 11, 585–591. [Google Scholar]
- Lee, J.H.; Jung, E.H.; Jeong, S.N. Profilometric, volumetric, and esthetic analysis of guided bone regeneration with L-shaped collagenated bone substitute and connective tissue graft in the maxillary esthetic zone: A case series with 1-year observational study. Clin. Implant Dent. Relat. Res. 2022, 24, 655–663. [Google Scholar] [CrossRef]
- van Eekeren, P.; Tahmaseb, A.; Wismeijer, D. Crestal bone changes in macrogeometrically similar implants with the implant-abutment connection at the crestal bone level or 2.5 mm above: A prospective randomized clinical trial. Clin. Oral Implants Res. 2016, 27, 1479–1484. [Google Scholar] [CrossRef]
- Lombardo, G.; Signoriello, A.; Marincola, M.; Liboni, P.; Bonfante, E.A.; Nocini, P.F. Survival rates of ultra-short (<6 mm) compared with short locking-taper implants supporting single crowns in posterior areas: A 5-year retrospective study. Clin. Implant Dent. Relat. Res. 2021, 23, 904–919. [Google Scholar] [PubMed]
- Canullo, L.; Micarelli, C.; Lembo-Fazio, L.; Iannello, G.; Clementini, M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures. Clin. Oral Implant Res. 2014, 25, 328–336. [Google Scholar] [CrossRef]
- Gil, J.; Pérez, R.; Herrero-Climent, M.; Rizo-Gorrita, M.; Torres-Lagares, D.; Gutierrez, J.L. Benefits of residual aluminium oxide for sand blasting titanium dental implants: Osseointegration and bactericidal effects. Materials 2022, 15, 178. [Google Scholar] [CrossRef]
- Herrero-Climent, M.; López-Jarana, P.; Lemos, B.F.; Gil, F.J.; Falcao, C.; Rios-Santos, J.V.; Rios-Carrasco, B. Relevant design aspects to improve the stability of titanium dental implants. Materials 2020, 13, 1910. [Google Scholar] [CrossRef]
- Nicolas-Silvente, A.I.; Velasco-Ortega, E.; Ortiz-García, I.; Monsalve-Guil, L.; Gil, F.J.; Jimenez-Guerra, A. Influence of the Titanium implants surface treatment on the surface roughness and chemical composition. Materials 2020, 13, 314. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ciurana, X.; Vela-Nebot, X.; Segalà-Torres, M.; Calvo-Guirado, J.L.; Camba, J.; Méndez-Blando, V. The effect of interimplant distance on the height of the interimplant bone crest when using platform-switched implants. Int. J. Periodontics Restor. Dent. 2009, 29, 141–151. [Google Scholar]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. Th influence of soft tissue thickness on crestal bone changes around implants: A 1-year prospective controlled clinical trial. Int. J. Oral Maxillofac. Implant 2009, 24, 712–719. [Google Scholar]
- Naert, I.; Duyck, J.; Vandamme, K. Occlusal overload and bone/implant loss. Clin. Oral Implant Res. 2012, 23, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Prosper, L.; Redaelli, S.; Pasi, M.; Zarone, F.; Radaelli, G.; Gherlone, E.F. A randomized prospective multicenter trial evaluating the platform-switching technique for the prevention of postrestorative crestal bone loss. Int. J. Oral Maxillofac. Implant 2009, 24, 299–308. [Google Scholar]
- Canullo, L.; Fedele, G.R.; Iannello, G.; Jepsen, S. Platform switching and marginal bone-level alterations: The results of a randomized-controlled trial. Clin. Oral Implant Res. 2010, 21, 115–121. [Google Scholar] [CrossRef]
- Romanos, G.E. Wound healing in immediately loaded implants. Periodontology 2000 2015, 68, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Hoyos, M.; Velasco, F.; Ginebra, M.P.; Manero, J.M.; Gil, F.J.; Mas-Moruno, C. Regenerating bone via multifunctional coatings: The blending of cell integration and bacterial inhibition properties on the Surface of biomaterials. ACS Appl. Mater. Interfaces 2019, 11, 36449–36457. [Google Scholar]
- Hoyos-Nogués, M.; Buxadera-Palomero, J.; Ginebra, M.P.; Manero, J.M.; Gil, F.J.; Mas-Moruno, C. All-in-One trifunctional strategy: A cell adhesive, bacteriostatic and bactericidal coating for titanium implants. Colloids Surf. B Biointerfaces 2018, 169, 30–40. [Google Scholar] [CrossRef]
- Sodnom-Ish, B.; Eo, M.Y.; Kim, M.J.; Kim, S.M. A 10-year survival rate of tapered self-tapping bone-level implants from medically compromised Korean patients at a maxillofacial surgical unit. Maxillofac. Plast. Reconstr. Surg. 2023, 45, 35. [Google Scholar] [CrossRef]
- Spinelli, A.; Zamparini, F.; Romanos, G.; Gandolfi, M.G.; Prati, C. Tissue-Level Laser-Lok Implants Placed with a Flapless Technique: A 4-Year Clinical Study. Materials 2023, 16, 1293. [Google Scholar] [CrossRef] [PubMed]
- Chacun, D.; Laforest, L.; Langlois-Jacques, C.; Dard, M.; Gritsch, K.; Grosgogeat, B. A Multicenter Cohort Study on 301 Tissue-Level Implants: Cumulative Implant Survival Rate and Marginal Bone Level Change up to 4.5 Years. Int. J. Oral Maxillofac. Implants. 2024, 39, 224–234. [Google Scholar] [CrossRef]
- Menini, M.; Dellepiane, E.; Deiana, T.; Fulcheri, E.; Pera, P.; Pesce, P. Comparison of Bone-Level and Tissue-Level Implants: A Pilot Study with a Histologic Analysis and a 4-Year Follow-up. Int. J. Periodontics Restor. Dent. 2022, 42, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. 2013. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 June 2020).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Lopez, M.A.; Andreasi, B.M.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. Clinical outcome of 215 transmucosal implants with a conical connection: A retrospective study after 5-year follow-up. J. Biol. Regul. Homeost. Agents 2016, 30, 55–60. [Google Scholar] [PubMed]
- Lopez, M.A.; Andreasi Bassi, M.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. Retrospective study on bone-level and soft-tissue-level cylindrical implants. Regul. Homeost Agents 2016, 30 (Suppl. S1), 43–48. [Google Scholar]
- Andreasi Bassi, M.; Lopez, M.A.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. Clinical outcome of a two-piece implant system with an internal hexagonal connection: A prospective study. J. Biol. Regul. Homeost. Agents 2016, 30, 7–12. [Google Scholar]
- Lopez, M.A.; Andreasi, B.M.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. The influence of “conical plus octagonal” internal connection on implant survival and success rate: A retrospective study of 66 fixtures. J. Biol. Regul. Homeost. Agents 2016, 30, 49–54. [Google Scholar] [PubMed]
- Souza, A.B.; Sukekava, F.; Tolentino, L.; César-Neto, J.B.; Garcez-Filho, J.; Araújo, M.G. Narrow- and regular-diameter implants in the posterior region of the jaws to support single crowns: A 3-year split-mouth randomized clinical trial. Clin. Oral Implants Res. 2017, 28, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, J.; Naaman, B.A.N.; Nohra, J.; Chaaya, B.M. Marginal bone stability around bone level versus tissue level implants in non-compliant patients with healthy or reduced periodontium: A 10-year retrospective study. Int. Arab. J. Dent. 2020, 11, 75–85. [Google Scholar] [CrossRef]
- Bienz, S.P.; Ruales, C.E.; Hüsler, J.; Roccuzzo, A.; Jung, R.E.; Thoma, D.S. Soft tissue contour changes at implant sites with or without soft tissue grafting in the esthetic zone: A retrospective case–control study with a 12-year follow-up. Clin. Oral Implants Res. 2023, 34, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Catena, A.; Pérez-Sayáns, M.; Fernández-Barbero, J.E.; O’Valle, F.; Padial-Molina, M. Early marginal bone loss around dental implants to define success in implant dentistry: A retrospective study. Clin. Implant Dent. Relat. Res. 2022, 24, 630–642. [Google Scholar] [CrossRef] [PubMed]
- Sui, H.; Tang, Z.; Zhang, X.; Wei, D.; Wang, F.; Zhao, Y. A prospective, multicenter study of 6-mm short implants in posterior alveolar bone supporting splinted crowns: A 5-year follow-up study. J. Clin. Periodontol. 2022, 49, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Aloy-Prosper, A.; Sanchis-Gonzalez, J.C.; Peñarrocha-Diago, M.A.; Peñarrocha-Diago, M. Comparison of peri-implant bone loss between conventional drilling with irrigation versus low-speed drilling without irrigation. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e730–e736. [Google Scholar] [CrossRef] [PubMed]
- Prati, C.; Zamparini, F.; Pirani, C.; Montebugnoli, L.; Canullo, L.; Gandolfi, M.G. A multilevel analysis of platform-switching flapless implants placed at tissue level: 4-year prospective cohort study. Int. J. Oral Maxillofac. Implants. 2020, 35, 330–341. [Google Scholar] [CrossRef]
- Costa Castillo, M.; Martos, L.M.; Pitarch, M.R.; Selva, G.M.; Rodríguez, C.S.; Fons-Badal, C. Analysis of Peri-Implant Bone Loss with a Convergent Transmucosal Morphology: Retrospective Clinical Study. Int. J. Environ. Res. Public Health 2022, 19, 3443. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, J.; Chen, K.; Li, Z.; Chen, Z.; Huang, B. Clinical and radiographic results of crestal vs. subcrestal placement of implants in posterior areas: A split-mouth randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2023, 25, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Meloni, S.M.; Baldoni, E.; Pisano, M.; Tullio, A.; De Riu, G.; Tallarico, M. 1-year results from a split-mouth randomised controlled pilot trial comparing implants with 0.75 mm of machined collar placed at bone level or supracrestally. Eur. J. Oral Implantol. 2018, 11, 353–359. [Google Scholar] [PubMed]
- Canullo, L.; Menini, M.; Bagnasco, F.; Di Tullio, N.; Pesce, P. Tissue-level versus bone-level single implants in the anterior area rehabilitated with feather-edge crowns on conical implant abutments: An up to 5-year retrospective study. J. Prosthet. Dent. 2022, 128, 936–941. [Google Scholar] [CrossRef]
- Pera, F.; Carossa, M.; Bagnasco, F.; Crupi, A.; Ambrogio, G.; Isola, G.; Menini, M.; Pesce, P. Comparison between Bone-Level and Tissue-Level Implants in Immediate-Loading Full-Arch Rehabilitations: A Retrospective Multi-Center 1-Year Follow-Up Study. Prosthesis 2023, 5, 1301–1311. [Google Scholar] [CrossRef]
- Lago, L.; Da Silva, L.; Martinez-Silva, I.; Rilo, B. Radiographic Assessment of Crestal Bone Loss in Tissue-Level Implants Restored by Platform Matching Compared with Bone-Level Implants Restored by Platform Switching: A Randomized, Controlled, Split-Mouth Trial with 3-Year Follow-Up. Int. J. Oral Maxillofac. Implants 2019, 34, 179–186. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Authors | Study Design | Sample | Implant System, Brand and Number | Implant Length and Diameter (mm) | Surgery | [Follow-Up] Methods of Measurements | Survival Rate & Success Rate | Results (mean MBL, CBL, HBL OR PIL) in mm. | Covariates |
|---|---|---|---|---|---|---|---|---|---|
| Lopez et al., 2016 [38]. | Cohort | P = 65. F = 35. M = 30. | -Cylindrical tapered Shiner XT Implants (215). -FMD Falappa Medical Devices S.p.A. Rome, Italy) -BL = 215. | Length = >8, 10–14 & <14. Diameter = 3.4–4.8. | Technique A. | [5-year; 85 ± 44 m] Int, Pan. | SVR = 100% SCR = 92.6% | PIL = 01 ± 1.3. |
|
| Lopez et al., 2016 [39]. | Cohort | P = 150. F = 76. M = 74. | -Cylindrical tapered Implant. -FMD, Rome, Italy. -BL = 49 -STL = 99 | Length = 8–14. Diameter = 3.4,3.8, & <4.2. | Technique A. | [84 ± 47 m] Int, Pan. | SCR = 92% SVR = 98.7% | PIL = 0 ± 1.4. BL = 0.12 ± 1.47. STL = 0.04 ± 1.3. Only two implants were lost. |
|
| Andreasi Bassi et al., 2016 [40]. | Cohort | P = 52. F = 21. M = 31. | -Cylindrical and Conical tapered implants (52). -Elisir EVO Cylindrical & conical, FMD, Rome, Italy. -BL = 52. | Length = ≤10.5, 11.5, 13 & >13. Diameter = 3.4, 3.8 & >4.2. | Technique A. | [44.6 ± 34.4 m] Px. | SCR = 77%. SVR = 100%. | MBL = 0.9 ± 0.7. |
|
| López et al., 2016 [41]. | Cohort | P = 38. F = 18. M = 20. | -Cylindrical and Conical tapered implants. -I-Fix implants by FMD Falappa Medical Devices S.p.A. Rome, Italy. -BL= 66. | Lengths = 8, 10, 11.5, 13. Diameters = 3.5, 4.0, 4.5, 5.0. | Technique A. | [(12 to 36 M), with a mean of 24 months] Px. | SVR = 100% SCR = 82%. | MBL cylindrical I = 0.52 ± 0.21. MBL conical I = 0.48 ± 0.19. |
|
| Nicolas et al., 2020 [43]. | Cohort | P = 44. N.m. | -Straumann, Branemark & 3I Biomet. -BL = 97. -TL = 43. | Length = 8, 8.5, 10, 11.5, 12, 13, 15. Diameter = 3.25, 3.30, 3.75, 4.0, 4.10, 4.80, 5.0. | N.m | [10-year] Px. | N.m | Mean CBL: TL = 1.18 ± 0.89. BL = 0.97 ± 0.64. Mesial bone loss (MBL): 3i BL = 0.68 ± 0.74. Branemark BL = 0.61 ± 0.83. Straumann TL = 0.85 ± 1.25. Distal bone loss (DBL): 3i BL = 1.45 ± 0.74. Branemark BL = 1.10 ± 0.84. Straumann TL = 1.50 ± 0.80. Average bone loss (ABL): 3i BL = 1.07 ± 0.61. Branemark BL = 0.856 ± 0.67. Straumann TL = 1.18 ± 0.89. |
|
| Galindo-Moreno et al., 2022 [45]. | Cohort | P = 176. M = 89. F = 87. | -Conical internal connection. -Astra Tech TX implants. -BL = 590. | Length = 6, 9, 11, 13 & 15. Diameter = 3.5, 4.0, 4.5 &5. | Technique A. | [(6 & 18 m] Pan. | N.m | MBL BL = 0.64. |
|
| Sui et al., 2022 [46]. | Cohort | P = 45. M = 17. F = 28. | -Cylindrical dental implants -Osseo Speed TX, Dentsply Sirona, York, PA, USA). -BL = 68. | Length: 6. Diameter: 4. | Technique A. | [5-year] Px. | SCR = 88.4% | MBL = 0.04 ± 0.14. 4 I in 4 P were lost before loading. 1 I in 1 P was lost at the 5-year follow-up. 2 P were lost to follow-up. | N.m. |
| Prati et al., 2020 [48]. | Cohort | P = 76. M = 34. F = 42. | -Cylindrical Hexagonal internal connection implant. -Premium SP, Sweden & Martina. -TL = 128. | Length = 10 or 11.5. Diameter = 3.8, 4.25, or 5.0. | Technique A. | [48 M] Px. | SVR = 98.4% SCR = 98.4% | MBL = 0.99 ± 0.68. 2 implants were failed. |
|
| Pellicer-Chover et al., 2017 [47]. | Case-control | P = 25. M = 9. F = 16. | -Ticare® Inhex® implants. -Group A = High-speed drilling with irrigation. -Group B = Low-speed drilling with irrigation -BL = 30. | length = 10, 11.5, 13. Diameter = 3.75, 4.2, 5.0. | Technique C. | [12 m] Px. | SCR: Group A = 93.3%. Group B = 100%. | MBL: Group A = 0.83 ± 0.73. Group B = 0.70 ± 0.62. 1 I failed during osseointegration in Group A. | N.m. |
| Costa-Castillo et al., 2022 [49]. | Case-control | P = 30. N.r. | -Cylindrical & tapered. -Sweden & Martina (Prama, Shelta & Premium) (Padua, Italy). -Bl = 20. -TL = 10. | Length = 8.5, 10, 11.5, 13. Diameter = 3.30. 3.80, 4.25, 5.0. | N.r. | [1-year; prosthetic loading] Px. | N.r. | Mean PIL: BL = 1.04., 0.12. TL = 0.27. |
|
| Canullo L et al., 2022) [52] | Case-control | P = 43. M = 43. | -Conical connection. -Premium Kohno & Prama; Sweden & Martina. -BL = 18. -TL = 25. | Length = 11–13. Diameter = 3.8. | N.r. | [5-year; TLI = 3.97 Y BL = 4.71 Y] Px. | SVR = 100%. | MBL TL = 0.38 ± 0.46. BL = 0.83 ±0.58. | N.m |
| Pera F et al. 2020) [53] | Case-control | P = 38. N.r. | -Conical & cylindrical Tapered. -Syra or Shelta & Prama implants, Sweden & Martina Due Carrare, Padova, Italy. -BL = 76. -TL = 80. | Length = 10, 11.5,13,15. Diameter = 3.8, 4.25. | Technique A. | [1 y] Px. | BL SVR = 97.37%. TL SVR = 100%. | MBL BL = 1.324 ± 0.64. TL = 1.194 ± 0.30. Failure of 2 BL Implants. | N.m. |
| Souza et al., 2017 [42]. | RCT | P = 22. F = 12. M = 10. | - Straumann® Tissue Level Standard Plus implants with narrow and regular diameter. -Straumann® Dental Implant System, Basel, Switzerland. -TL = 44. | Length = 6–12. NDIs: 3.3. RDIs: 4.1. | N.m | [3-year] Px. | SCR = 95% NDIs = 95%. RDIs = 100% | MBL NDIs: 1Y = −0.49 ± 0.27. 3Y = −0.58 ± 0.39. MBL RDIs: 1Y = −0.42 ± 0.27. 3Y = −0.53 ± 0.46. |
|
| Yue Sun et al., 2023 [50]. | RCT | P = 19. F = 11. M = 8. | -Conical connection. -Straumann RC BL. -Bl = 21. -Tl = 21. | Length = 8 & 10. Diameter = 4.1 &4.8. | Technique A. | [12 ms] Px. | N.r. | MBL TL = 0.04 ± 0.08. BL = 0.17 ± 0.017. 4 Implants were lost for control. | N.m. |
| Meloni M.S et al., 2018) [51] | RCT | P = 10. M = 3. F = 7. | -Tapered connection. -Nobel Replace Tapered CC PMC, Nobel Biocare, Goteborg, Sweden. -Bl = 10. -SC = 10. | Length = 8 & 10. Diameter = 4.3. | Technique A. | [1-year] Px. | N.r. | MBL BL = 0.93 ± 0.37. SC = 0.28 ± 0.21. | N.m. |
| Lago L et al., 2018) [54] | RCT | P = 35. M = 15. F = 20. | -Straumann &Straumann Plus -BL = 50. -TL = 50. | N.r. | Technique A. | [3 y] Px. | SVR = 100% | CBL BL = 0.18 ± 0.46. TL = 0.14 ± 0.35. | N.m. |
| Randomized * | Double Blind * | Lost to Follow-Up and Removed from Study * | Correct Method of Randomization ** | Correct Method of Double Blind ** | Score | |
|---|---|---|---|---|---|---|
| Souza et al. [42] | 1 | 0 | 1 | 1 | −1 | 2 |
| Sun et al. [50] | 1 | 1 | 1 | 1 | 1 | 5 |
| Meloni et al. [51] | 1 | 0 | 1 | −1 | −1 | 0 |
| Lago et al. [54] | 1 | 0 | 1 | 1 | −1 | 2 |
| Selection | Comparability | Exposure | Score (0–9) | |
|---|---|---|---|---|
| Lopez et al. [38] | *** | * | ** | 6 |
| Lopez et al. [39] | *** | * | ** | 6 |
| Anndrea Bassi et al. [40] | *** | * | ** | 6 |
| Lopez et al. [41] | *** | * | ** | 6 |
| Nicolas et al. [43] | *** | * | ** | 6 |
| Bienz et al. [44] | **** | * | ** | 7 |
| Galindo-Moreno et al. [45] | *** | * | ** | 6 |
| Sui et al. [46] | **** | * | ** | 7 |
| Pellicer-Chover et al. [47] | *** | * | ** | 6 |
| Prati et al. [48] | *** | * | ** | 6 |
| Costa-Castillo et al. [49] | *** | * | *** | 7 |
| Canullo et al. [52] | *** | * | ** | 6 |
| Pera et al. [53] | **** | * | *** | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkattan, A.; Torres-Velázquez, N.; Blázquez-Hinarejos, M.; Egido-Moreno, S.; Ayuso-Montero, R.; Roselló-Llabrés, X.; López-López, J. Marginal Bone Loss Around Bone-Level and Tissue-Level Implants: A Systematic Review and Meta-Analysis. Appl. Sci. 2025, 15, 2286. https://doi.org/10.3390/app15052286
Elkattan A, Torres-Velázquez N, Blázquez-Hinarejos M, Egido-Moreno S, Ayuso-Montero R, Roselló-Llabrés X, López-López J. Marginal Bone Loss Around Bone-Level and Tissue-Level Implants: A Systematic Review and Meta-Analysis. Applied Sciences. 2025; 15(5):2286. https://doi.org/10.3390/app15052286
Chicago/Turabian StyleElkattan, Ahmed, Natalia Torres-Velázquez, Mónica Blázquez-Hinarejos, Sonia Egido-Moreno, Raúl Ayuso-Montero, Xavier Roselló-Llabrés, and José López-López. 2025. "Marginal Bone Loss Around Bone-Level and Tissue-Level Implants: A Systematic Review and Meta-Analysis" Applied Sciences 15, no. 5: 2286. https://doi.org/10.3390/app15052286
APA StyleElkattan, A., Torres-Velázquez, N., Blázquez-Hinarejos, M., Egido-Moreno, S., Ayuso-Montero, R., Roselló-Llabrés, X., & López-López, J. (2025). Marginal Bone Loss Around Bone-Level and Tissue-Level Implants: A Systematic Review and Meta-Analysis. Applied Sciences, 15(5), 2286. https://doi.org/10.3390/app15052286