

Enhancing Clinical Assessment of Skin Ulcers with Automated and Objective Convolutional Neural Network-Based Segmentation and 3D Analysis

 , , ,
, , ,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Automatic Skin Ulcer Segmentation
2.2. Skin Ulcer Parameter Extraction
2.3. XR Environment for Skin Ulcer Visualization
3. Results
3.1. Segmentation Assessment
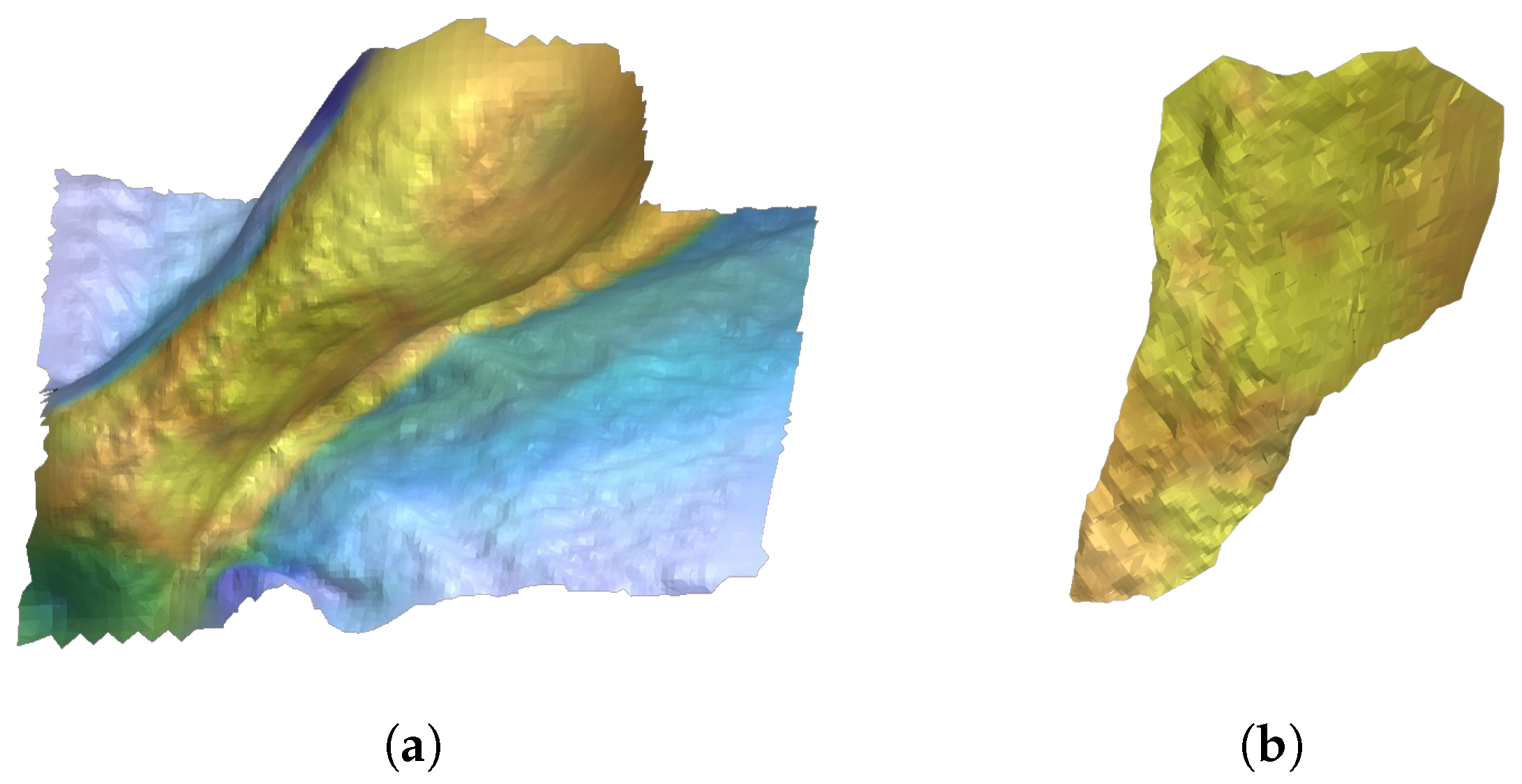
3.2. Surface Segmentation and Parameter Evaluation
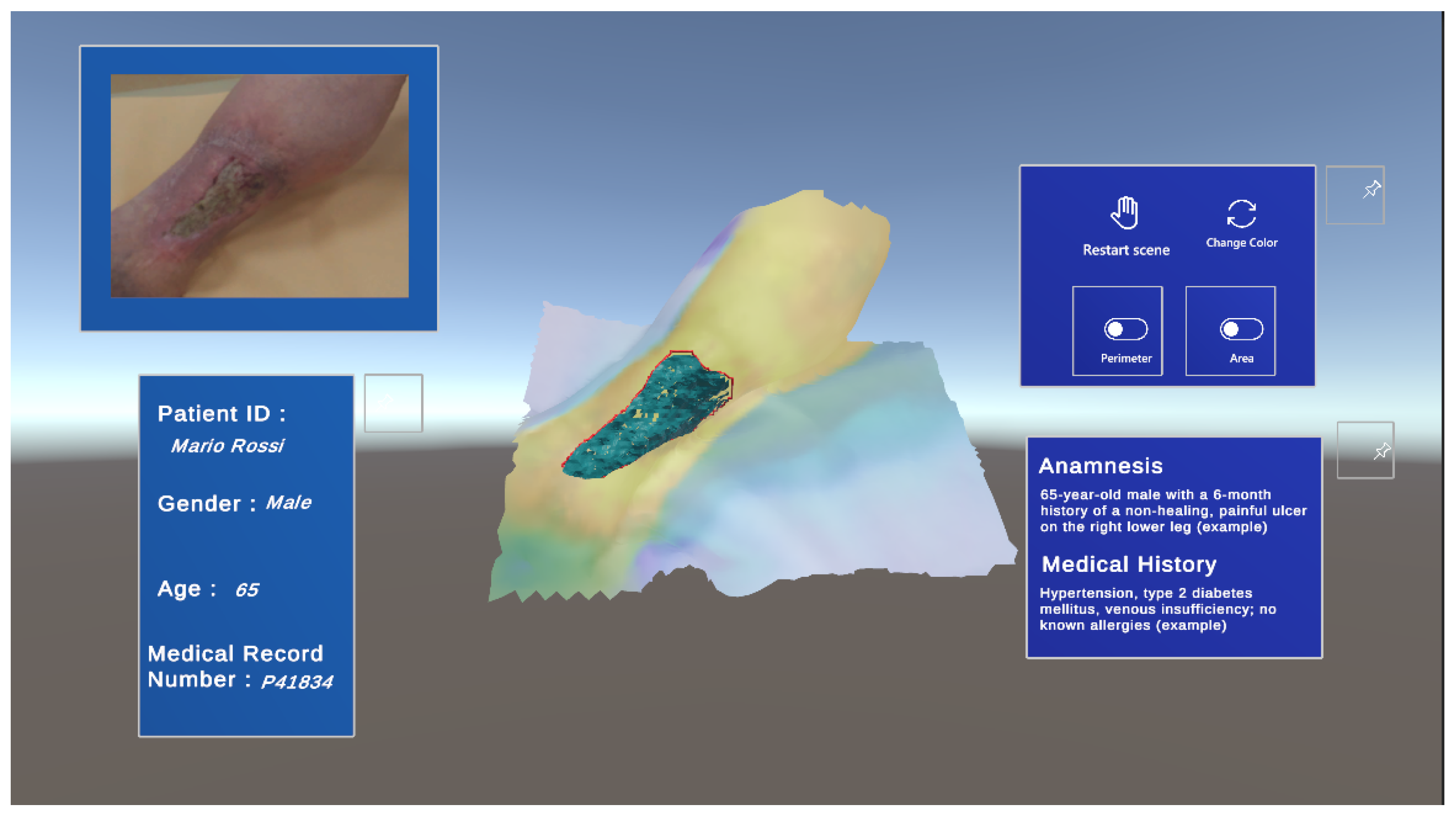
3.3. XR Environment Setup
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garcia, F.R.; da Silva Olanda, D.E.; Filgueiras, M.F.; de Pontes, A.T.A.; dos Santos, M.C.S.; do Nascimento, N.C.; Ferreira, J.A.G.; Silva, T.C.S.; Sousa, K.S. Multiprofessional Care in Chronic Wounds. Health Soc. 2022, 2, 31–36. [Google Scholar] [CrossRef]
- Iversen, A.K.S.; Lichtenberg, M.; Fritz, B.G.; Cort, I.D.P.; Al-Zoubaidi, D.F.; Gottlieb, H.; Kirketerp-Møller, K.; Bjarnsholt, T.; Jakobsen, T.H. The chronic wound characterisation study and biobank: A study protocol for a prospective observational cohort investigation of bacterial community composition, inflammatory responses and wound-healing trajectories in non-healing wounds. BMJ Open 2024, 14, e084081. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Shankar, R.; Yadav, A.K.; Pratap, A.; Ansari, M.A.; Srivastava, V. Burden of Chronic Nonhealing Wounds: An Overview of the Worldwide Humanistic and Economic Burden to the Healthcare System. Int. J. Low. Extrem. Wounds 2024. [Google Scholar] [CrossRef] [PubMed]
- Suksawat, T.; Panichayupakaranant, P. Skin Ulcers as a Painful Disorder with Limited Therapeutic Protocols. In Natural Products for Treatment of Skin and Soft Tissue Disorders; Bentham Science Publishers: Potomac, MD, USA, 2023; 209p. [Google Scholar]
- Markova, A.; Mostow, E.N. US skin disease assessment: Ulcer and wound care. Dermatol. Clin. 2012, 30, 107. [Google Scholar] [CrossRef]
- Laucirica, I.; Iglesias, P.G.; Calvet, X. Peptic ulcer. Med. Clín. (Engl. Ed.) 2023, 161, 260–266. [Google Scholar] [CrossRef]
- Secco, J. Imaging and Measurement. In Pearls and Pitfalls in Skin Ulcer Management; Springer: Berlin/Heidelberg, Germany, 2024; pp. 317–338. [Google Scholar]
- Jaganathan, Y.; Sanober, S.; Aldossary, S.M.A.; Aldosari, H. Validating wound severity assessment via region-anchored convolutional neural network model for mobile image-based size and tissue classification. Diagnostics 2023, 13, 2866. [Google Scholar] [CrossRef]
- Sánchez-Jiménez, C.L.; Verdesoto, E.S.B. State of the art of the automatized characterization of chronic wound patterns. In Proceedings of the 2024 IEEE Eighth Ecuador Technical Chapters Meeting (ETCM), Virtual, 15–18 October 2024; pp. 1–6. [Google Scholar]
- Sarp, S.; Kuzlu, M.; Zhao, Y.; Gueler, O. Digital twin in healthcare: A study for chronic wound management. IEEE J. Biomed. Health Inform. 2023, 27, 5634–5643. [Google Scholar] [CrossRef]
- Dini, V.; Granieri, G. Wound Measurement. In Pearls and Pitfalls in Skin Ulcer Management; Springer: Berlin/Heidelberg, Germany, 2024; pp. 339–346. [Google Scholar]
- Innocente, C.; Piazzolla, P.; Ulrich, L.; Moos, S.; Tornincasa, S.; Vezzetti, E. Mixed reality-based support for total hip arthroplasty assessment. In Proceedings of the International Joint Conference on Mechanics, Design Engineering & Advanced Manufacturing, Ischia, Italy, 1–3 June 2022; pp. 159–169. [Google Scholar]
- Biagioni, R.B.; Carvalho, B.V.; Manzioni, R.; Matielo, M.F.; Neto, F.C.B.; Sacilotto, R. Smartphone application for wound area measurement in clinical practice. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 258–261. [Google Scholar] [CrossRef]
- Fauzi, M.F.A.; Khansa, I.; Catignani, K.; Gordillo, G.; Sen, C.K.; Gurcan, M.N. Computerized segmentation and measurement of chronic wound images. Comput. Biol. Med. 2015, 60, 74–85. [Google Scholar] [CrossRef]
- Smith-Strøm, H.; Igland, J.; Østbye, T.; Tell, G.S.; Hausken, M.F.; Graue, M.; Skeie, S.; Cooper, J.G.; Iversen, M.M. The effect of telemedicine follow-up care on diabetes-related foot ulcers: A cluster-randomized controlled noninferiority trial. Diabetes Care 2018, 41, 96–103. [Google Scholar] [CrossRef]
- Bolton, L. Telemedicine Improves Chronic Ulcer Outcomes. Wounds A Compend. Clin. Res. Pract. 2019, 31, 114–116. [Google Scholar]
- Dabas, M.; Schwartz, D.; Beeckman, D.; Gefen, A. Application of artificial intelligence methodologies to chronic wound care and management: A scoping review. Adv. Wound Care 2023, 12, 205–240. [Google Scholar] [CrossRef] [PubMed]
- Sarp, S.; Kuzlu, M.; Wilson, E.; Cali, U.; Guler, O. The enlightening role of explainable artificial intelligence in chronic wound classification. Electronics 2021, 10, 1406. [Google Scholar] [CrossRef]
- Anisuzzaman, D.; Patel, Y.; Rostami, B.; Niezgoda, J.; Gopalakrishnan, S.; Yu, Z. Multi-modal wound classification using wound image and location by deep neural network. Sci. Rep. 2022, 12, 20057. [Google Scholar] [CrossRef]
- Secco, J.; Pittarello, M.; Begarani, F.; Sartori, F.; Corinto, F.; Ricci, E. Memristor Based Integrated System for the Long-Term Analysis of Chronic Wounds: Design and Clinical Trial. In Proceedings of the 2022 29th IEEE International Conference on Electronics, Circuits and Systems (ICECS), Glasgow, UK, 24–26 October 2022; pp. 1–4. [Google Scholar]
- Zoppo, G.; Marrone, F.; Pittarello, M.; Farina, M.; Uberti, A.; Demarchi, D.; Secco, J.; Corinto, F.; Ricci, E. AI technology for remote clinical assessment and monitoring. J. Wound Care 2020, 29, 692–706. [Google Scholar] [CrossRef]
- Kręcichwost, M.; Czajkowska, J.; Wijata, A.; Juszczyk, J.; Pyciński, B.; Biesok, M.; Rudzki, M.; Majewski, J.; Kostecki, J.; Pietka, E. Chronic wounds multimodal image database. Comput. Med. Imaging Graph. 2021, 88, 101844. [Google Scholar] [CrossRef]
- Ahmed, A.; Imran, A.S.; Manaf, A.; Kastrati, Z.; Daudpota, S.M. Enhancing wrist abnormality detection with yolo: Analysis of state-of-the-art single-stage detection models. Biomed. Signal Process. Control 2024, 93, 106144. [Google Scholar] [CrossRef]
- Al-Masni, M.A.; Al-Antari, M.A.; Park, J.M.; Gi, G.; Kim, T.Y.; Rivera, P.; Valarezo, E.; Choi, M.T.; Han, S.M.; Kim, T.S. Simultaneous detection and classification of breast masses in digital mammograms via a deep learning YOLO-based CAD system. Comput. Methods Programs Biomed. 2018, 157, 85–94. [Google Scholar] [CrossRef]
- Nie, Y.; Sommella, P.; O’Nils, M.; Liguori, C.; Lundgren, J. Automatic detection of melanoma with yolo deep convolutional neural networks. In Proceedings of the 2019 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 21–23 November 2019; pp. 1–4. [Google Scholar]
- Ünver, H.M.; Ayan, E. Skin lesion segmentation in dermoscopic images with combination of YOLO and grabcut algorithm. Diagnostics 2019, 9, 72. [Google Scholar] [CrossRef]
- Tan, L.; Huangfu, T.; Wu, L.; Chen, W. Comparison of RetinaNet, SSD, and YOLO v3 for real-time pill identification. BMC Med. Inform. Decis. Mak. 2021, 21, 324. [Google Scholar] [CrossRef]
- Kazhdan, M.; Hoppe, H. Screened poisson surface reconstruction. ACM Trans. Graph. (ToG) 2013, 32, 1–13. [Google Scholar] [CrossRef]
- Bernardini, F.; Mittleman, J.; Rushmeier, H.; Silva, C.; Taubin, G. The ball-pivoting algorithm for surface reconstruction. IEEE Trans. Vis. Comput. Graph. 1999, 5, 349–359. [Google Scholar] [CrossRef]
- Lee, D.T.; Schachter, B.J. Two algorithms for constructing a Delaunay triangulation. Int. J. Comput. Inf. Sci. 1980, 9, 219–242. [Google Scholar] [CrossRef]
- Ulrich, L.; Salerno, F.; Moos, S.; Vezzetti, E. How to exploit Augmented Reality (AR) technology in patient customized surgical tools: A focus on osteotomies. Multimed. Tools Appl. 2024, 83, 70257–70288. [Google Scholar] [CrossRef]
- Monroy, B.; Sanchez, K.; Arguello, P.; Estupiñán, J.; Bacca, J.; Correa, C.V.; Valencia, L.; Castillo, J.C.; Mieles, O.; Arguello, H.; et al. Automated chronic wounds medical assessment and tracking framework based on deep learning. Comput. Biol. Med. 2023, 165, 107335. [Google Scholar] [CrossRef]
- Jørgensen, L.B.; Halekoh, U.; Jemec, G.B.; Sørensen, J.A.; Yderstræde, K.B. Monitoring wound healing of diabetic foot ulcers using two-dimensional and three-dimensional wound measurement techniques: A prospective cohort study. Adv. Wound Care 2020, 9, 553–563. [Google Scholar] [CrossRef]
- Liu, C.; Fan, X.; Guo, Z.; Mo, Z.; Chang, E.I.C.; Xu, Y. Wound area measurement with 3D transformation and smartphone images. BMC Bioinform. 2019, 20, 724. [Google Scholar] [CrossRef]
- Souto, J.R.; Barbosa, F.M.; Carvalho, B.M. Three-Dimensional Wound Reconstruction using Point Descriptors: A Comparative Study. In Proceedings of the 2023 IEEE 36th International Symposium on Computer-Based Medical Systems (CBMS), L’Aquila, Italy, 22–24 June 2023; pp. 41–46. [Google Scholar]
- Gutierrez, E.; Castañeda, B.; Treuillet, S.; Lucas, Y. Combined thermal and color 3D model for wound evaluation from handheld devices. In Proceedings of the Medical Imaging 2021: Imaging Informatics for Healthcare, Research, and Applications, San Diego, CA, USA, 20–24 February 2021; Volume 11601, pp. 27–34. [Google Scholar]
- Monshipouri, M.; Aliahmad, B.; Ogrin, R.; Elder, K.; Anderson, J.; Polus, B.; Kumar, D. Thermal imaging potential and limitations to predict healing of venous leg ulcers. Sci. Rep. 2021, 11, 13239. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Learning Rate | Batch | Image Size | Epochs | Patience |
|---|---|---|---|---|
| 0.01 | 16 | 640 | 150 | 30 |
| Blur | Median Blur | ToGray | CLAHE |
|---|---|---|---|
| p = 0.01 blur_limit = (3, 7) | p = 0.01 blur_limit = (3, 7) | p = 0.01 | p = 0.01 clip_limit = (1, 4) |
| Area [cm2] Delaunay | Perimeter [cm] | |
|---|---|---|
| 2D | 67.9 | 39.5 |
| 3D | 123.1 | 66.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavazzana, R.; Faccia, A.; Cavallaro, A.; Giuranno, M.; Becchi, S.; Innocente, C.; Marullo, G.; Ricci, E.; Secco, J.; Vezzetti, E.; et al. Enhancing Clinical Assessment of Skin Ulcers with Automated and Objective Convolutional Neural Network-Based Segmentation and 3D Analysis. Appl. Sci. 2025, 15, 833. https://doi.org/10.3390/app15020833
Cavazzana R, Faccia A, Cavallaro A, Giuranno M, Becchi S, Innocente C, Marullo G, Ricci E, Secco J, Vezzetti E, et al. Enhancing Clinical Assessment of Skin Ulcers with Automated and Objective Convolutional Neural Network-Based Segmentation and 3D Analysis. Applied Sciences. 2025; 15(2):833. https://doi.org/10.3390/app15020833
Chicago/Turabian StyleCavazzana, Rosanna, Angelo Faccia, Aurora Cavallaro, Marco Giuranno, Sara Becchi, Chiara Innocente, Giorgia Marullo, Elia Ricci, Jacopo Secco, Enrico Vezzetti, and et al. 2025. "Enhancing Clinical Assessment of Skin Ulcers with Automated and Objective Convolutional Neural Network-Based Segmentation and 3D Analysis" Applied Sciences 15, no. 2: 833. https://doi.org/10.3390/app15020833
APA StyleCavazzana, R., Faccia, A., Cavallaro, A., Giuranno, M., Becchi, S., Innocente, C., Marullo, G., Ricci, E., Secco, J., Vezzetti, E., & Ulrich, L. (2025). Enhancing Clinical Assessment of Skin Ulcers with Automated and Objective Convolutional Neural Network-Based Segmentation and 3D Analysis. Applied Sciences, 15(2), 833. https://doi.org/10.3390/app15020833