
The Use of Ibuprofen Arginate in Pain Management Following Third Molar Surgery—A Scoping Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
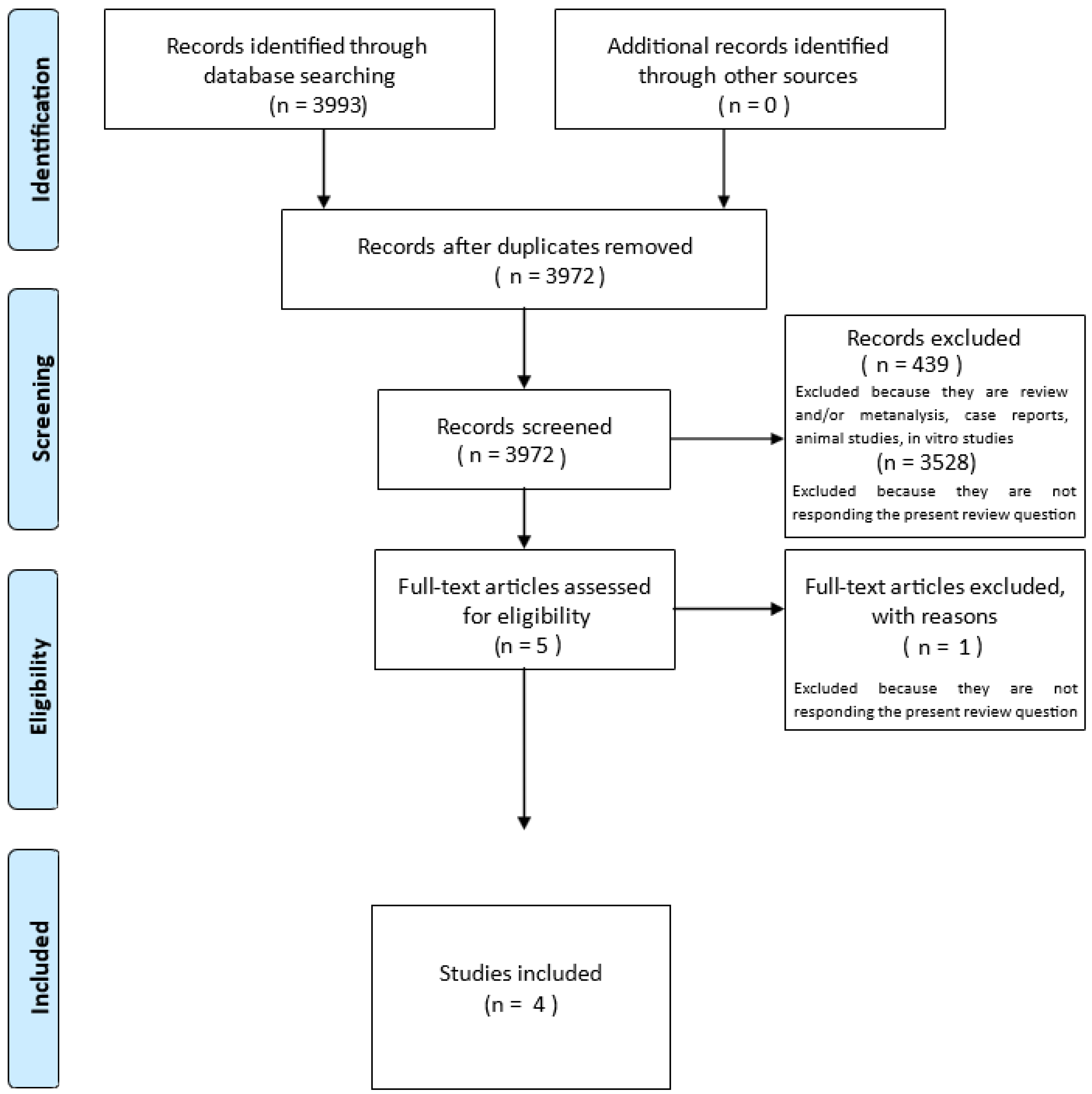
2.3. Selection of Sources of Evidence
2.4. Data Charting Process
2.5. Data Items
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Degirmenci, A.; Yalcin, E. The effect of pregabalin and ibuprofen combination for pain after third molar surgery. Niger. J. Clin. Pract. 2019, 22, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-C.; Choi, S.-S.; Wang, S.-J.; Kim, S.-G. Minor complications after mandibular third molar surgery: Type, incidence, and possible prevention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 102, e4–e11. [Google Scholar] [CrossRef] [PubMed]
- Mehlisch, D.R. Review of the comparative analgesic efficacy of salicylates, acetaminophen, and pyrazolones. Am. J. Med. 1983, 75, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Mehlisch, D.R.; Sollecito, W.A.; Heffrick, J.F.; Leibold, D.G.; Markowitz, R.; Schow, C.E.; Shultz, R.; Waite, D.E. Multicenter clinical trial of ibuprofen and acetaminophen in the treatment of postoperative dental pain. J. Am. Dent. Assoc. 1990, 121, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.A.; Moore, E.M.; Allen, H.W.; Beaver, W.T. Evaluation of an Ibuprofen Controlled-Release Tablet and Placebo in Postoperative Oral Surgery Pain. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1991, 11, 242–248. [Google Scholar] [CrossRef]
- Hersh, E.V.; Desjardin, P.J.; Trummel, C.L. Nonopioid analgesics, nonsteroidal anti-inflammatory drugs. In Pharmacology and Therapeutics for Dentistry, 6th ed.; Mosby Elsevier: St. Louis, MO, USA, 2011; pp. 346–348. [Google Scholar]
- Vane, J.R. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nat. New Biol. 1971, 231, 232–235. [Google Scholar] [CrossRef]
- Moore, P.A.; Hersh, E.V. Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions: Translating clinical research to dental practice. J. Am. Dent. Assoc. 2013, 144, 898–908. [Google Scholar] [CrossRef]
- Adams, S.S.; Bresloff, P.; Mason, C.G. Pharmacological differences between the optical isomers of ibuprofen: Evidence for metabolic inversion of the (-)-isomer. J. Pharm. Pharmacol. 1976, 28, 256–257. [Google Scholar] [CrossRef]
- Gaut, Z.N.; Baruth, H.; Randall, L.O.; Ashley, C.; Paulsrud, J.R. Stereoisomeric relationships among anti-inflammatory activity, inhibition of platelet aggregation, and inhibition of prostaglandin synthetase. Prostaglandins 1975, 10, 59–66. [Google Scholar] [CrossRef]
- Evans, A.M.; Nation, R.L.; Sansom, L.N.; Bochner, F.; Somogyi, A.A. Effect of racemic ibuprofen dose on the magnitude and duration of platelet cyclo-oxygenase inhibition: Relationship between inhibition of thromboxane production and the plasma unbound concentration of S(+)-ibuprofen. Br. J. Clin. Pharmacol. 1991, 31, 131–138. [Google Scholar] [CrossRef]
- Rainsford, K.D. Discovery, mechanisms of action and safety of ibuprofen. Int. J. Clin. Pract. Suppl. 2003, 3–8. [Google Scholar] [PubMed]
- Jamali, F.; Mehvar, R.; Russell, A.S.; Sattari, S.; Yakimets, W.W.; Koo, J. Human pharmacokinetics of ibuprofen enantiomers following different doses and formulations: Intestinal chiral inversion. J. Pharm. Sci. 1992, 81, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Carosi, P.; Gallucci, G.O.; Nagy, K.; Nardi, A.; Arcuri, L. Accuracy of complete-arch digital implant impression with intraoral optical scanning and stereophotogrammetry: An in vivo prospective comparative study. Clin. Oral Implant. Res. 2023, 34, 1106–1117. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, K.; Abbott, P.V. Drugs for pain management in dentistry. Aust. Dent. J. 2005, 50 (Suppl. 2), S14–S22. [Google Scholar] [CrossRef]
- La Monaca, G.; Pranno, N.; Annibali, S.; Polimeni, A.; Pompa, G.; Cristalli, M.P. Effects of ibuprofen administration timing on oral surgery pain: A randomized clinical trial. Oral Dis. 2022, 28, 796–804. [Google Scholar] [CrossRef]
- Davies, N.M. Clinical pharmacokinetics of ibuprofen. The first 30 years. Clin. Pharmacokinet. 1998, 34, 101–154. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.A. The relative efficacy of ibuprofen in dental pain. Compend. Contin. Educ. Dent. 1986, 7, 578. [Google Scholar]
- Forbes, J.A.; Barkaszi, B.A.; Ragland, R.N.; Hankle, J.J. Analgesic effect of fendosal, ibuprofen and aspirin in postoperative oral surgery pain. Pharmacotherapy 1984, 4, 385–391. [Google Scholar] [CrossRef]
- Cooper, S.A. Five studies on ibuprofen for postsurgical dental pain. Am. J. Med. 1984, 77, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Sádaba, B.; Campanero, M.A.; Muñoz-Juarez, M.J.; Gil-Aldea, I.; García-Quetglas, E.; Esteras, A.; Azanza, J.R. A comparative study of the pharmacokinetics of ibuprofen arginate versus dexibuprofen in healthy volunteers. Eur. J. Clin. Pharmacol. 2006, 62, 849–854. [Google Scholar] [CrossRef]
- Fini, A.; Fazio, G.; Feroci, G. Solubility and solubilization properties of non-steroidal anti-inflammatory drugs. Int. J. Pharm. 1995, 126, 95–102. [Google Scholar] [CrossRef]
- Carosi, P.; Lorenzi, C.; Di Gianfilippo, R.; Papi, P.; Laureti, A.; Wang, H.L.; Arcuri, C. Immediate vs. Delayed Placement of Immediately Provisionalized Self-Tapping Implants: A Non-Randomized Controlled Clinical Trial with 1 Year of Follow-Up. J. Clin. Med. 2023, 12, 489. [Google Scholar] [CrossRef]
- De Palma, C.; Di Paola, R.; Perrotta, C.; Mazzon, E.; Cattaneo, D.; Trabucchi, E.; Cuzzocrea, S.; Clementi, E. Ibuprofen–arginine generates nitric oxide and has enhanced anti-inflammatory effects. Pharmacol. Res. 2009, 60, 221–228. [Google Scholar] [CrossRef]
- Cattaneo, D.; Clementi, E. Clinical pharmacokinetics of ibuprofen arginine. Curr. Clin. Pharmacol. 2010, 5, 239–245. [Google Scholar] [CrossRef]
- Cajaraville, J.P. Ibuprofen arginate for rapid-onset pain relief in daily practice: A review of its use in different pain conditions. J. Pain Res. 2021, 14, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, P.; Black, P.; Papageorge, M.; Norwood, T.; Shen, D.D.; Norris, L.; Ardia, A. Ibuprofen arginate provides effective relief from postoperative dental pain with a more rapid onset of action than ibuprofen. Eur. J. Clin. Pharmacol. 2002, 58, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Black, P.; Max, M.B.; Desjardins, P.; Norwood, T.; Ardia, A.; Pallotta, T. A randomized, double-blind, placebo-controlled comparison of the analgesic efficacy, onset of action, and tolerability of ibuprofen arginate and ibuprofen in postoperative dental pain. Clin. Ther. 2002, 24, 1072–1089. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, SA, Australia, 2015. [Google Scholar]
- Ramos, E.U.; Benetti, L.P.; Oliveira, J.C.S.; Bassi, A.P.F. Single-Dose Ibuprofen-Arginine as a Preventive for Pain, Edema, and Trismus After Impacted Lower Third Molar Surgery: A Randomized Split-Mouth Clinical Trial. Eur. J. Dent. 2022, 16, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Mehlisch, D.R.; Ardia, A.; Pallotta, T. A controlled comparative study of ibuprofen arginate versus conventional ibuprofen in the treatment of postoperative dental pain. J. Clin. Pharmacol. 2002, 42, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi, C.; Lio, F.; Papi, P.; Mazzetti, V.; Laureti, A.; Arcuri, C. Clinical Reliability of Complete-Arch Fixed Prostheses Supported by Narrow-Diameter Implants to Support Complete-Arch Restorations. Appl. Sci. 2023, 13, 538. [Google Scholar] [CrossRef]
- Lau, S.L.; Chow, R.L.K.; Yeung, R.W.K.; Samman, N. Pre-emptive ibuprofen arginate in third molar surgery: A double-blind randomized controlled crossover clinical trial. Aust. Dent. J. 2009, 54, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, C. Nitric oxide and the immune response. Nat. Immunol. 2001, 2, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.L.; Vong, L. NSAID-induced gastrointestinal damage and the design of GI-sparing NSAIDs. Curr. Opin. Investig. Drugs 2008, 9, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- De Nadai, C.; Sestili, P.; Cantoni, O.; Lièvremont, J.-P.; Sciorati, C.; Barsacchi, R.; Moncada, S.; Meldolesi, J.; Clementi, E. Nitric oxide inhibits tumor necrosis factor-alpha-induced apoptosis by reducing the generation of ceramide. Proc. Natl. Acad. Sci. USA 2000, 97, 5480–5485. [Google Scholar] [CrossRef]
- Bulotta, S.; Barsacchi, R.; Rotiroti, D.; Borgese, N.; Clementi, E. Activation of the endothelial nitric-oxide synthase by tumor necrosis factor-alpha. A novel feedback mechanism regulating cell death. J. Biol. Chem. 2001, 276, 6529–6536. [Google Scholar] [CrossRef]
- Lièvremont, J.-P.; Sciorati, C.; Morandi, E.; Paolucci, C.; Bunone, G.; Della Valle, G.; Meldolesi, J.; Clementi, E. The p75(NTR)-induced apoptotic program develops through a ceramide-caspase pathway negatively regulated by nitric oxide. J. Biol. Chem. 1999, 274, 15466–15472. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Carosi, P.; Laureti, A.; Mattheos, N.; Pimkhaokham, A.; Chow, J.; Arcuri, L. Accuracy of navigation guided implant surgery for immediate loading complete arch restorations: Prospective clinical trial. Clin. Implant. Dent. Relat. Res. 2024, 26, 954–971. [Google Scholar] [CrossRef]
- De Palma, C.; Falcone, S.; Panzeri, C.; Radice, S.; Bassi, M.T.; Clementi, E. Endothelial nitric oxide synthase overexpression by neuronal cells in neurodegeneration: A link between inflammation and neuroprotection. J. Neurochem. 2008, 106, 193–204. [Google Scholar] [CrossRef]
- Lorenzi, C.; Leggeri, A.; Cammarota, I.; Carosi, P.; Mazzetti, V.; Arcuri, C. Hyaluronic Acid in Bone Regeneration: Systematic Review and Meta-Analysis. Dent. J. 2024, 12, 263. [Google Scholar] [CrossRef] [PubMed]
- Leggeri, A.; Carosi, P.; Mazzetti, V.; Arcuri, C.; Lorenzi, C. Techniques to Improve the Accuracy of Intraoral Digital Impression in Complete Edentulous Arches: A Narrative Review. Appl. Sci. 2023, 13, 7068. [Google Scholar] [CrossRef]
- Franco, L.; Doria, D. Nitric oxide enhances prostaglandin production in ethanol-induced gastric mucosal injury in rats. Eur. J. Pharmacol. 1998, 348, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Konturek, J.W.; Fischer, H.; Gromotka, P.M.; Konturek, S.J.; Domschke, W. Endogenous nitric oxide in the regulation of gastric secretory and motor activity in humans. Aliment. Pharmacol. Ther. 1999, 13, 1683–1691. [Google Scholar] [CrossRef]
- Carosi, P.; Ottria, L.; Lio, F.; Laureti, A.; Papi, P. The health of soft tissues around four dental implants loaded immediately supporting a 4-year-old fixed screw-retained prosthesis. J. Biol. Regul. Homeost. Agents 2021, 35 (Suppl. 1), 57–66. [Google Scholar] [CrossRef] [PubMed]
- Mollace, V.; Muscoli, C.; Masini, E.; Cuzzocrea, S.; Salvemini, D. Modulation of prostaglandin biosynthesis by nitric oxide and nitric oxide donors. Pharmacol. Rev. 2005, 57, 217–252. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi, C.; Lio, F.; Mazzetti, V.; Carosi, P.; Lamelza, S.; Pistoia, E.S.; Pica, F.; Gaziano, R. Synergistic Effect of Metronidazole and Chlorhexidine against Porphyromonas gingivalis Growth: An In Vitro Study. Dent. J. 2024, 12, 307. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.L. Prostaglandins, NSAIDs, and gastric mucosal protection: Why doesn’t the stomach digest itself? Physiol. Rev. 2008, 88, 1547–1565. [Google Scholar] [CrossRef] [PubMed]
- Gyires, K. Gastric mucosal protection: From prostaglandins to gene-therapy. Curr. Med. Chem. 2005, 12, 203–215. [Google Scholar] [CrossRef]
- Duda, D.G.; Fukumura, D.; Jain, R.K. Role of eNOS in neovascularization: NO for endothelial progenitor cells. Trends Mol. Med. 2004, 10, 143–145. [Google Scholar] [CrossRef]
- Moore, A.R.; Derry, S.; Straube, S.; Ireson-Paine, J.; Wiffen, P.J. Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain 2014, 155, 14–21. [Google Scholar] [CrossRef]
- Uzeda, M.J.; Silva, A.M.; Costa, L.N.; Brito, F.S.; Fernandes, G.V.; Resende, R.F. Evaluating the effectiveness of low-level laser therapy in patients undergoing lower third molar extraction: A double-blinded randomized controlled trial. Med. Oral Patol. Oral. Cir. Bucal. 2025, 30, e129–e134. [Google Scholar] [CrossRef]
- Monteiro, R.J.S.V.; Moura-Netto, C.; Veiga, N.J.; Amaral, S.A.; Fernandes, G.V.D.O. Periodontal regeneration after third molar extraction causing attachment loss in distal and furcation sites of the second molar: A case report with 12 months follow-up. J. Clin. Rev. Case Rep. 2022, 7, 128–132. [Google Scholar]

{kind=link}
| PCC | |
|---|---|
| (P) Population | Patients undergoing third molar extraction |
| (C) Concept | Ibuprofen arginate compared to conventional ibuprofen |
| (C) Context | All settings considered |
| Database | MeSH Terms and Search Terms |
|---|---|
| MEDLINE/PubMed | (((“ibuprofen arginine” [Supplementary Concept] OR “ibuprofen arginine” [All Fields] OR “ibuprofen arginate” [All Fields] OR (“ibuprofen arginine” [Supplementary Concept] OR “ibuprofen arginine” [All Fields])) AND ((“molar, third” [MeSH Terms] OR (“molar” [All Fields] AND “third” [All Fields]) OR “third molar” [All Fields] OR (“third” [All Fields] AND “molar” [All Fields])) AND (“surgery” [MeSH Subheading] OR “surgery” [All Fields] OR “surgical procedures, operative” [MeSH Terms] OR (“surgical” [All Fields] AND “procedures” [All Fields] AND “operative” [All Fields]) OR “operative surgical procedures” [All Fields] OR “general surgery” [MeSH Terms] OR (“general” [All Fields] AND “surgery” [All Fields]) OR “general surgery” [All Fields] OR “surgery s” [All Fields] OR “surgerys” [All Fields] OR “surgeries” [All Fields]))) OR ((“postoperative period” [MeSH Terms] OR (“postoperative” [All Fields] AND “period” [All Fields]) OR “postoperative period” [All Fields] OR “postop” [All Fields] OR “postoperative” [All Fields] OR “postoperatively” [All Fields] OR “postoperatives” [All Fields]) AND (“toothache” [MeSH Terms] OR “toothache” [All Fields] OR (“dental” [All Fields] AND “pain” [All Fields]) OR “dental pain” [All Fields]))) AND (2002:2024 [pdat]) |
| First Author | Date | Sample Size | Medications | Timing | Pain Test 6 h After Surgery (Mean and SD) | Pain Control Test 6 h After Surgery (Mean and SD) | Conclusion |
|---|---|---|---|---|---|---|---|
| Ramos et al. [29] | 2022 | 21 | Group 1: ibuprofen (600 mg) + arginine (500 mg); Group 2: ibuprofen (600 mg) | 1 h before surgery | 2.6 ± 1 * | 5.0 ± 1 * | Ibuprofen arginate, compared to conventional ibuprofen, is notably more effective in managing pain and swelling. |
| Black et al. [28] | 2002 | 498 | Group 1: ibuprofen arginate (200 or 400 mg); Group 2: ibuprofen (200 or 400 mg); and Group 3: placebo | When pain had reached a moderate-to-severe intensity | 200 mg = 0.6 ± 0.8 ** 400 mg = 0.8 ± 0.9 ** | 200 mg = 0.7 ± 0.9 ** 400 mg = 1.0 ± 1.0 ** Placebo = 0.1 ± 1.0 ** | In this patient population, ibuprofen arginate was as effective as traditional ibuprofen in pain control but provided a faster onset of action. |
| Mehlisch et al. [30] | 2002 | 500 | Group 1: ibuprofen arginate (200 or 400 mg); Group 2: ibuprofen (200 or 400 mg); and Group 3: placebo | When pain had reached a moderate-to-severe intensity | 200 mg= 1.9 ± 1.4 ** 400 mg = 1.8 ± 1.5 ** | 200 mg= 1.5 ± 1.4 ** 400 mg = 2.0 ± 1.5 ** Placebo = 0.7 ± 1.7 ** | Ibuprofen arginate was equally effective as a pain reliever compared to conventional ibuprofen, but with a quicker onset of action. |
| Desjardins et al. [31] | 2002 | 226 | Group 1: ibuprofen arginate (200 or 400 mg); Group 2: ibuprofen (200 or 400 mg); and Group 3: placebo | When pain had reached a moderate-to-severe intensity | 200 mg = −0.5 ± 0.8 ** 400 mg = −0.3 ± 0.9 ** | 200 mg = −0.4 ± 0.8 ** 400 mg = −0.3 ± 1.0 ** Placebo = −0.8 ± 0.4 ** | Ibuprofen arginate provided pain relief that was either comparable to or better than that of conventional ibuprofen, depending on the dose, with a faster onset of action. Patients receiving 400 mg of ibuprofen arginate experienced significant pain relief in half the time compared to those treated with 400 mg of standard ibuprofen. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzi, C.; Cammarota, I.; Mazzetti, V.; Arcuri, C.; Carosi, P.; Pujia, A.M. The Use of Ibuprofen Arginate in Pain Management Following Third Molar Surgery—A Scoping Review. Appl. Sci. 2025, 15, 662. https://doi.org/10.3390/app15020662
Lorenzi C, Cammarota I, Mazzetti V, Arcuri C, Carosi P, Pujia AM. The Use of Ibuprofen Arginate in Pain Management Following Third Molar Surgery—A Scoping Review. Applied Sciences. 2025; 15(2):662. https://doi.org/10.3390/app15020662
Chicago/Turabian StyleLorenzi, Claudia, Ilaria Cammarota, Vincenzo Mazzetti, Claudio Arcuri, Paolo Carosi, and Alberto Maria Pujia. 2025. "The Use of Ibuprofen Arginate in Pain Management Following Third Molar Surgery—A Scoping Review" Applied Sciences 15, no. 2: 662. https://doi.org/10.3390/app15020662
APA StyleLorenzi, C., Cammarota, I., Mazzetti, V., Arcuri, C., Carosi, P., & Pujia, A. M. (2025). The Use of Ibuprofen Arginate in Pain Management Following Third Molar Surgery—A Scoping Review. Applied Sciences, 15(2), 662. https://doi.org/10.3390/app15020662