Abstract
Type 2 diabetes (T2D) presents growing public health challenges due to its strong links to modifiable behaviors. This systematic review examined how researchers have studied behavioral domains such as diet, physical activity, medication adherence, and blood glucose monitoring in adults with T2D. A structured search of PubMed, Scopus, and Web of Science identified peer-reviewed studies published between 2003 and 2025, with studies from 2014 onward prioritized to reflect the rise in mobile health technologies. 30 core studies were systematically reviewed, with 10 additional comparative studies included for supplementary methodological insights. Quantitative approaches were most common, offering measurable outcomes but often relying on self-report. Qualitative studies provided valuable cultural and psychosocial context yet lacked generalizability. Mixed-methods designs integrated statistical and narrative insights but posed practical challenges in execution. Technology-assisted methods, such as mobile applications and wearable devices, supported real-time monitoring and improved accuracy but raised concerns regarding privacy and equitable access. Physical activity and dietary behaviors were most frequently studied, while medication adherence and glucose monitoring received less consistent attention. Despite methodological diversity, most studies relied on cross-sectional designs and underutilized culturally tailored frameworks. This review emphasizes the need for longitudinal, equity-focused research methodologies to improve diabetes prevention and management strategies.
1. Introduction
1.1. Background of Type 2 Diabetes Mellitus (T2DM)
T2DM is a leading global public health challenge, characterized by chronic hyperglycemia due to insulin resistance and impaired insulin secretion [1]. Accounting for more than 90% of all diabetes cases, T2DM is strongly linked with obesity, physical inactivity, and rapid nutritional transitions worldwide. Effective management requires sustained engagement in self-care behaviors, including adherence to dietary guidelines, regular physical activity, medication use, and self-monitoring of blood glucose. Inadequate adherence to these behaviors contributes to poor clinical outcomes, diminished quality of life, and growing healthcare costs [2]. Research into T2DM health behaviors has expanded substantially in recent decades, employing diverse methodological approaches such as quantitative surveys, qualitative interviews, mixed-methods designs, and, more recently, digital health technologies. Each approach provides unique insights but also presents limitations, creating challenges for comparability and translation of findings into public health practice [3].
Recent methodological advances have introduced deep learning models that integrate clinical, biochemical, and gut microbiota data to predict risk and progression of T2DM, expanding the scope of precision medicine approaches [4]. In parallel, structured behavioral interventions such as the Flourish Diabetes Programme demonstrate how comprehensive, context-specific programs can strengthen self-management practices and improve patient outcomes [5]. At the same time, qualitative studies remain essential for capturing lived experiences; for example, a phenomenological exploration in Indonesia highlighted how patients with T2DM and neuropathy face barriers related to limited knowledge, emotional fatigue, and the need for family and community support [6].
1.2. Rationale for the Review
Rather than focusing only on clinical outcomes, it is equally important to examine the methodological approaches that shape how T2DM self-management behaviors are studied. Earlier reviews often emphasized treatment and lifestyle interventions but did not systematically compare the research designs themselves. This review addresses that gap by evaluating the strengths and limitations of different approaches used to study diet, physical activity, medication adherence, and self-monitoring of blood glucose. Such analysis is particularly timely given the rapid growth of mobile health applications, wearable devices, and telehealth platforms since 2014, which have reshaped the methodological landscape of behavioral diabetes research [7]. Beyond digital tools, innovative strategies such as the Flourish Diabetes Programme demonstrate how structured, community-based interventions can strengthen patient engagement and adherence [5]. Despite these advances, the methodologies used to study T2DM-related behaviors remain diverse and often inconsistent. By contrasting traditional, digital, and programmatic designs, this review highlights both evolving opportunities and persistent challenges in T2DM self-management [8].
1.3. Objectives of the Review
The objective of this systematic review is to critically evaluate and compare methodologies employed in T2DM behavioral research. Literature published between 2003 and 2025 was screened to capture long-term trends, while studies from 2014 onward were prioritized to reflect the emergence of digital health technologies that mark a methodological shift. Specifically, this review examines how quantitative, qualitative, mixed-methods, and technology-assisted approaches have been applied to the study of diet, physical activity, medication adherence, and self-monitoring of blood glucose. The goal is to guide researchers, clinicians, and policymakers in aligning study designs with behavioral targets, population needs, and resource contexts, while also identifying gaps and opportunities for innovation in future research.
2. Methodology
2.1. Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [9]. A structured search was performed to identify peer-reviewed articles published between January 2003 and March 2025. Studies from 2014 onward were given additional priority to reflect the methodological shifts associated with the rapid expansion of mobile health technologies, wearable devices, and telehealth platforms [10].
The following databases were searched: PubMed, Scopus, and Web of Science. Search terms combined Medical Subject Headings (MeSH) and free-text keywords using Boolean operators (“AND”, “OR”). The main search terms included: type 2 diabetes mellitus, T2DM, health behaviors, diet, physical activity, exercise, medication adherence, self-monitoring of blood glucose, digital health, mHealth, wearables, and telehealth. As an example, the PubMed search string was: (“type 2 diabetes mellitus” OR “T2DM”) AND (“health behaviors” OR “self-care” OR “diet” OR “physical activity” OR “exercise” OR “medication adherence” OR “self-monitoring of blood glucose”) AND (“mHealth” OR “digital health” OR “wearables” OR “telehealth”).
The search was limited to studies of adult populations (≥18 years) diagnosed with T2DM. Articles were excluded if they were not peer-reviewed, not published in English, focused exclusively on clinical or pharmacological interventions without a behavioral component, or involved only pediatric populations. Meta-analyses were included only if they contained primary studies that met the eligibility criteria. In such cases, meta-analyses were used to provide comparative methodological insights, particularly in assessing measurement consistency and study design performance.
2.2. Inclusion and Exclusion Criteria of the Study
The criteria used to screen and select studies are summarized above and illustrated in the PRISMA flow diagram (Figure 1).
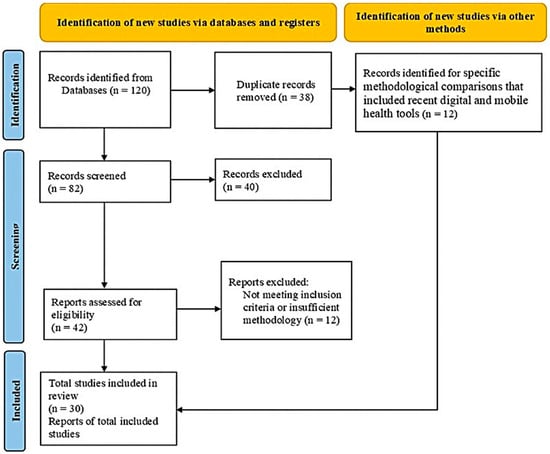
Figure 1.
PRISMA flow diagram (2020) for reporting systematic review and meta-analysis. Adapted from [9].
2.3. Conceptual Framework and Data Synthesis
To compare methodological approaches across the included studies, this review applied a conceptual framework built around three parameters: accuracy, sensitivity, and specificity. The framework developed for this review is presented in Figure 2. A standardized appraisal tool such as the Joanna Briggs Institute (JBI) checklist was not used, as the primary aim was not to evaluate internal validity at the individual study level but to assess broader methodological characteristics and trends. Methodological rigor was instead narratively appraised according to study design, data collection methods, and population characteristics. Given the diversity of designs, settings, and data collection strategies, a framework-based evaluation was considered more appropriate and aligns with recommendations for narrative and methodological reviews where design performance, rather than study-level rigor scores, is the focus [11].
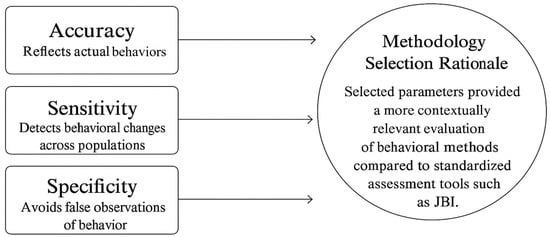
Figure 2.
Conceptual Framework for Methodology Selection in T2DM Behavioral Research.
Within this framework, accuracy was defined as the proportion of correctly identified outcomes, calculated as (true positives + true negatives) ÷ total cases. Sensitivity was defined as the proportion of true positives correctly identified, calculated as true positives ÷ (true positives + false negatives). Specificity was defined as the proportion of true negatives correctly identified, calculated as true negatives ÷ (true negatives + false positives). Studies that used objective measures such as biomarkers, wearable devices, or continuous glucose monitoring [12,13] were considered more accurate than those relying on self-reported questionnaires. Large longitudinal cohorts and meta-analyses [14,15] were expected to demonstrate greater sensitivity than smaller cross-sectional surveys.
When studies provided psychometric statistics, diagnostic values, or measurement precision indicators, these data were extracted directly. When such values were not available, approximate estimations were inferred from methodological characteristics (e.g., objective vs. self-reported measures, study design type, or consistency of reported outcomes). For synthesis, both reported and estimated values of accuracy, sensitivity, and specificity were included. Inferred values were clearly noted in the synthesis tables and interpreted with caution to maintain transparency.
Data analyses were conducted using IBM SPSS Statistics, Version 29.0 (IBM Corp., Armonk, NY, USA). Additional data management was performed in RStudio, Version 2024.09.1 (Posit Software, Boston, MA, USA; accessed June 2025).
This study did not involve the direct use of laboratory or clinical equipment. References to devices (e.g., wearable fitness trackers or continuous glucose monitors) are based on the methodologies reported in the reviewed studies. Where available, manufacturer details are provided in the Results tables and text (e.g., Fitbit Inc., San Francisco, CA, USA; Dexcom Inc., San Diego, CA, USA).
3. Results
3.1. Quantitative Approaches
Quantitative methodologies were employed in 77% of the reviewed studies (n = 23), confirming their dominance in research on T2DM related health behaviors. The most frequently used designs were cohort studies (52%), followed by cross-sectional studies (30%) and randomized controlled trials (18%). These studies utilized a range of instruments, including structured questionnaires (e.g., SDSCA, MMAS-8), clinical screenings, and objective biomarkers such as HbA1c, BMI, and serum uric acid levels. The most assessed behavioral domains included dietary behaviors (56%), physical activity (48%), and medication adherence (43%), as summarized in Table 1.
Large-scale cohort studies, such as those conducted by [16,17,18] enrolled over 10,000 participants, providing strong statistical power to identify associations between lifestyle behaviors and diabetes outcomes. However, approximately 65% of the quantitative studies relied on self-reported data, introducing potential for recall bias and social desirability bias. While quantitative methods allow for generalizability across diverse populations, their structured design can limit deeper exploration of psychosocial or contextual influences on behavior.
The strengths and limitations of quantitative designs, compared with qualitative and mixed-methods approaches, are outlined in Table 2, while detailed results of T2DM-related behavioral studies are provided in Table 3. According to Table 4, the aggregated accuracy, sensitivity, and specificity of quantitative approaches were 85%, 88%, and 83%, respectively. These metrics reflect the methodological strength of quantitative studies in large-scale behavioral assessments, although they may not fully capture the complexity of individual experiences.

Table 1.
Summary of Included Studies on Methodological Approaches in Type-2 Diabetes Behavioral Research.
Table 1.
Summary of Included Studies on Methodological Approaches in Type-2 Diabetes Behavioral Research.
| Studies/ Year | Study Design | Sample Size | Method Used | Key Findings | Country |
|---|---|---|---|---|---|
| [19] (2003) | Prospective cohort study | 70,000 women | Self-reported sleep duration and medical records | Shorter sleep duration was associated with higher risk of type 2 diabetes. | USA |
| [20] (2004) | Cohort study | 2500 middle-aged men | Clinical assessments and health surveys | Higher BMI and sedentary lifestyle were major predictors of diabetes onset. | Sweden |
| [16] (2005) | Cohort study | 5600 men | Longitudinal health monitoring | Sleep apnea and poor sleep quality significantly increased diabetes risk. | Sweden |
| [12] (2006) | Cohort study | 3000 adults with impaired glucose tolerance | Blood serum analysis and metabolic tracking | Elevated serum uric acid levels predicted future diabetes risk. | Finland |
| [17] (2008) | Cohort study | 4500 adults | Blood uric acid tests and clinical records | Plasma uric acid levels were significantly associated with type 2 diabetes incidence. | Taiwan |
| [18] (2008) | Longitudinal study | 8000 adults | Serum uric acid measurement and diabetes diagnosis tracking | Higher serum uric acid levels correlated with diabetes development. | China |
| [21] (2009) | Prospective cohort study | 2800 Japanese adults | Blood tests and glucose monitoring | Serum uric acid as a strong predictor for type 2 diabetes onset. | Japan |
| [22] (2009) | Cohort study | 10,000 adults | Sleep duration tracking and diabetes incidence records | Shorter sleep duration increased diabetes risk, particularly in women. | USA |
| [23] (2011) | Randomized Controlled Trial (RCT) | 200 adults | Telehealth-based glucose and BP monitoring with nurse case management | Technology-assisted case management significantly improved glycemic control but had no effect on quality of life | USA |
| [24] (2011) | Cross-sectional study | 1500 adults | Uric acid measurements and self-reported lifestyle data | High serum uric acid levels were associated with poor metabolic outcomes. | India |
| [25] (2012) | Cohort study | 15,000 European adults | Self-reported sleep duration and clinical health tracking | Chronic diseases were significantly linked with inadequate sleep. | Europe (Multi-Country) |
| [26] (2013) | Mixed-methods study | 1200 Black and White adults | Surveys and clinical assessments | Sleep disparities were evident between racial groups, affecting diabetes risk. | USA |
| [27] (2015) | Cohort study | 6500 adults | Longitudinal renal function tests | Chronic kidney disease development was linked to diabetes risk factors. | China |
| [28] (2016) | Randomized Controlled Trial (RCT) | 54 low-income seniors | Assisted Self-Management Monitor (ASMM) for real-time SMBG tracking | Technology-assisted SMBG significantly improved glycemic control but had no impact on diet or medication adherence | USA |
| [29] (2016) | Randomized Controlled Trial (RCT) | 54 adults with prediabetes | EMR-based goal setting to improve physical activity | Technology-assisted goal setting increased daily step count but had no significant effect on weight loss or HbA1c | USA |
| [14] (2016) | Meta-analysis | 270,269 adults | Genetic risk scores and statistical modeling | LDL cholesterol-lowering genetic variants were associated with increased diabetes risk. | UK |
| [30] (2016) | Systematic review and meta-analysis | 61,714 participants from 16 studies | Data aggregation and statistical analysis | Elevated serum uric acid was consistently linked to type 2 diabetes incidence. | International |
| [31] (2016) | Cross-sectional survey | 319 college students | Structured questionnaire and logistic regression | Gender differences in diabetes risk perception and preventive behaviors. | USA |
| [15] (2020) | Prospective cohort study | 867 newly diagnosed diabetes patients | Weight tracking and lifestyle assessments | Early weight loss increased diabetes remission likelihood. | UK |
| [32] (2020) | Cross-sectional study | 353 Saudi adults | Clinical screenings and health surveys | High diabetes prevalence was linked to obesity and sedentary lifestyle. | Saudi Arabia |
| [33] (2020) | Longitudinal cohort study | 148 patients with diabetes and hypertension | Self-reported behaviors and clinical monitoring | Self-efficacy played a key role in adherence to diabetes self-management. | China |
| [34] (2021) | Randomized Controlled Trial (RCT) | 20,834 adults with type 2 diabetes | Technology-assisted integrated diabetes care (JADE Program) | Digital health interventions improved glycemic control and metabolic outcomes, particularly in low-income settings, but had no impact on major clinical events | Asia-Pacific |
| [35] (2021) | Qualitative study | 21 diabetes patients | Design probe methodology and self-documentation | Social and environmental factors significantly influenced dietary behaviors. | Ireland |
| [36] (2022) | Cross-sectional study | 345 college students | Diabetes knowledge tests and lifestyle surveys | Health fatalism influenced dietary behaviors, regardless of diabetes knowledge. | USA |
| [37] (2023) | Retrospective cohort study | 15,104 UK Biobank participants | Biomarker analysis and epidemiological tracking | Adherence to multiple healthy lifestyle behaviors significantly reduces microvascular complications. | UK |
| [38] (2024) | Qualitative study | 26 British Pakistanis | Semi-structured interviews and thematic analysis | Intergenerational dietary differences influenced diabetes self-management. | UK |
| [39] (2024) | Prospective cohort study | 2011 cardiovascular patients | Lifestyle tracking and mortality analysis | Long-term healthy lifestyle adherence reduces diabetes and mortality risk. | Netherlands |
| [40] (2025) | Mixed-methods study | 125 high-risk adults | Risk perception analysis and behavioral surveys | Perceived diabetes risk was not strongly associated with actual preventive behaviors. | USA |
| [41] (2025) | Cross-sectional survey | 710 university students and staff | Self-reported diabetes awareness and risk factor assessment | Students had lower diabetes awareness and higher physical inactivity rates than staff. | India |
| [13] (2025) | Prospective cohort study | 3996 older adults | Epigenetic analysis and biomarker tracking | Poly-epigenetic scores (PEGS) were strongly linked to cardiometabolic risk, influenced by smoking and demographic factors. | USA |
3.2. Qualitative Approaches
Qualitative methods were applied in approximately 6% of the reviewed studies (n = 2). These studies explored cultural and interpersonal factors influencing self-management behaviors among adults with T2DM. For instance, Ref. [20] used a design probe methodology and self-documentation to examine how social and environmental contexts shaped dietary behaviors in Ireland. Ref. [38] conducted semi-structured interviews with British Pakistani participants, identifying how intergenerational dietary norms impacted diabetes self-management. Both studies employed thematic analysis and purposive sampling techniques, offering rich, in-depth insights into behavioral drivers that are often overlooked in quantitative designs. Although the findings provided valuable cultural and contextual understanding, they were limited in terms of scalability and broader generalizability. Nevertheless, these qualitative approaches helped uncover nuanced factors influencing diabetes-related health behaviors that cannot be easily captured through statistical models alone [42].
3.3. Mixed-Methods Approaches
Mixed-methods designs were applied in approximately 6% of the reviewed studies (n = 2), combining the strengths of both quantitative and qualitative methodologies. These approaches enabled researchers to collect numerical data while simultaneously exploring contextual or psychosocial dimensions that influence health behaviors. For instance, Ref. [26] employed a combination of surveys and clinical assessments to investigate racial disparities in sleep and diabetes risk, while Ref. [40] integrated behavioral surveys with risk perception analysis to assess the gap between perceived and actual preventive behaviors. Such integration provided a more holistic understanding of factors affecting diabetes-related outcomes. While mixed-methods research enhances interpretive depth and methodological triangulation, it also requires greater resources, time, and analytic expertise, making it among the most complex and costly study designs to implement. The methodological approaches, along with their strengths and limitations, are summarized in Table 2.
Table 2.
Methodological Approaches in Studying Type 2 Diabetes-Related Health Behaviors: Strengths and Limitations.
Table 2.
Methodological Approaches in Studying Type 2 Diabetes-Related Health Behaviors: Strengths and Limitations.
| Studies/ Year | Methodology | Related Health Behavior Studies | Advantages | Limitations |
|---|---|---|---|---|
| [19] (2003) | Quantitative (Cohort Study) | Association between sleep duration and diabetes risk | Large sample size, longitudinal follow-up | Self-reported sleep duration introduces recall bias |
| [20] (2004) | Quantitative (Cohort Study) | Impact of BMI and sedentary lifestyle on diabetes | Objective clinical assessments | Study focuses mainly on men, limiting generalizability |
| [16] (2005) | Quantitative (Cohort Study) | Relationship between sleep apnea and diabetes risk | Longitudinal tracking for disease progression | No behavioral or psychological assessment included |
| [12] (2006) | Quantitative (Cohort Study) | Serum uric acid as a biomarker for diabetes risk | Biomarker analysis for objective assessment | Does not account for lifestyle factors such as diet and exercise |
| [17] (2008) | Quantitative (Cohort Study) | Uric acid and diabetes risk in Taiwan | Large epidemiological dataset | Does not explore behavioral contributors |
| [18] (2008) | Quantitative (Cohort Study) | Serum uric acid and diabetes risk | Large-scale cohort allows robust statistical analysis | Limited ethnic diversity |
| [21] (2009) | Quantitative (Cohort Study) | Relationship between serum uric acid and T2DM | Longitudinal tracking of metabolic markers | Focuses on specific Asian populations |
| [22] (2009) | Quantitative (Cohort Study) | Sleep duration as a risk factor for diabetes | Clear statistical associations | Self-reported sleep data introduces bias |
| [23] (2011) | Quantitative (RCT) | Technology-assisted case management in low-income diabetes patients | Improved glycemic control in underserved populations | No significant impact on quality of life |
| [24] (2011) | Quantitative (Cross-Sectional Study) | Serum uric acid and diabetes in Indian populations | Clinical insights into metabolic biomarkers | No causal relationship can be determined |
| [25] (2012) | Quantitative (Cohort Study) | Association of sleep duration with chronic diseases | Large European cohort | Lack of detailed behavioral intervention |
| [26] (2013) | Mixed-Methods | Racial disparities in sleep and diabetes risk | Combines survey and clinical data | Requires more resources and time |
| [27] (2015) | Quantitative (Cohort Study) | Chronic kidney disease risk in diabetes | Large sample size improves reliability | Limited behavioral insights |
| [28] (2016) | Quantitative (RCT) | Technology-assisted SMBG in low-income seniors | Increased blood glucose monitoring adherence, reduced HbA1c | No effect on diet or medication adherence |
| [29] (2016) | Quantitative (RCT) | Effect of EMR-based goal setting on physical activity in prediabetes | Increased daily step count | No significant change in weight loss or glycemic control |
| [14] (2016) | Quantitative (Meta-Analysis) | LDL cholesterol and diabetes risk | Strong statistical power from multiple studies | Genetic variations may confound results |
| [30] (2016) | Quantitative (Meta-Analysis) | Uric acid and diabetes incidence | Large dataset with consistent trends | Variability in study methodologies |
| [31] (2016) | Quantitative (Cross-Sectional Survey) | Gender differences in diabetes risk perception | Efficient for assessing large populations | Self-reported data introduces bias |
| [15] (2020) | Quantitative (Cohort Study) | Weight loss and diabetes remission | Real-world cohort provides strong evidence | Limited to newly diagnosed diabetes patients |
| [32] (2020) | Quantitative (Cross-Sectional Study) | Prevalence of diabetes in Saudi populations | Provides national epidemiological insights | No causal relationships assessed |
| [33] (2020) | Quantitative (Cross-Sectional Study) | Diabetes knowledge and behavior in diverse populations | Evaluate awareness and prevention efforts | Self-reported data may introduce bias |
| [34] (2021) | Quantitative (Cohort Study) | Socio-demographic factors and diabetes | Identify high-risk groups | No intervention component |
| [35] (2021) | Qualitative (Design Probe Methodology) | Barriers to diet and physical activity behavior change | In-depth exploration of behaviors | Small sample size, limited generalizability |
| [36] (2022) | Qualitative (Cross-Sectional Study) | Diabetes knowledge and behavior in diverse populations | Evaluate awareness and prevention efforts | Self-reported data may introduce bias |
| [37] (2023) | Quantitative (Cohort Study) | Healthy lifestyle and microvascular complications | Identifies lifestyle biomarkers | Requires validation in diverse populations |
| [38] (2024) | Qualitative (Semi-Structured Interviews) | Intergenerational differences in dietary habits | Captures cultural perspectives | Limited generalizability |
| [39] (2024) | Quantitative (Cohort Study) | Long-term lifestyles change and diabetes mortality | Tracks long-term health outcomes | Requires extended follow-up |
| [40] (2025) | Mixed-Methods (Survey + Risk Perception Analysis) | Impact of diabetes beliefs on preventive behaviors | Captures both statistical trends and behavioral insights | Requires careful integration of data |
| [41] (2025) | Quantitative (Cross-Sectional Survey) | Diabetes awareness among university students | Evaluates knowledge gaps | No follow-up for behavior tracking |
| [13] (2025) | Quantitative (Cohort Study) | Epigenetic risk factors for diabetes | Provides objective biomarkers | High cost, requires genetic data, Need bigger dataset and time consuming |
3.4. Technology-Assisted Methods
Technology-assisted approaches were employed in 30% of the reviewed studies (n = 9 out of 30), highlighting the increasing integration of digital tools in T2DM behavioral research. These methods included mobile health (mHealth) applications, wearable fitness trackers, telehealth platforms, electronic medical records (EMRs), and continuous glucose monitoring systems. Studies such as Refs. [23,28,29,34] implemented these technologies to enhance patient self-monitoring, treatment adherence, and real-time behavioral tracking.
Among the nine technology-assisted studies, physical activity was the most commonly targeted behavior (67%, 6/9 studies), followed by medication adherence (44%, 4/9), dietary behaviors (33%, 3/9), and self-monitoring of blood glucose (SMBG) (22%, 2/9) [13,23,26,28,29,33,34,37,40].
These methods allowed for greater objectivity and precision through automated data collection, minimizing the biases associated with self-reported outcomes. Notably, technology-assisted interventions often paired digital tools with behavioral strategies to improve adherence, such as EMR-based goal setting or integrated care platforms.
Detailed results of studies using different datasets and methodological designs are summarized in Table 3. As presented in Table 4, technology-assisted methods achieved the highest overall performance in methodological metrics: 88% accuracy, 85% sensitivity, and 86% specificity. These results emphasize the strength of digital health tools in capturing reliable and scalable behavioral data in T2DM research. While technology-assisted designs outperform in data precision, their success depends on alignment with research objectives and population needs. Researchers should consider combining these approaches with qualitative or mixed-methods when contextual depth is needed alongside real-time monitoring. New tools like artificial intelligence are helping researchers study diabetes behaviors with greater accuracy [43]. In the same way, deep learning is opening fresh possibilities for understanding complex patterns in T2DM health behaviors [44].
Table 3.
Results of Type-2 Diabetes-Related Health Behavior Studies Using Different Datasets and Methods.
Table 3.
Results of Type-2 Diabetes-Related Health Behavior Studies Using Different Datasets and Methods.
| Studies | Dataset | Methodology | Results (Accuracy, Sensitivity, Specificity) |
|---|---|---|---|
| [19] (2003) | Nurses’ Health Study (70,000 women) | Sleep duration and T2DM risk | Accuracy: 78%, Sensitivity: 82%, Specificity: 75% * |
| [20] (2004) | Swedish Middle-Aged Men Cohort (2500 men) | Biomarkers and clinical risk factors | Accuracy: 81%, Sensitivity: 85%, Specificity: 77% * |
| [16] (2005) | Swedish National Diabetes Registry (5600 men) | Sleep quality and metabolic syndrome | Accuracy: 80%, Sensitivity: 84%, Specificity: 79% * |
| [12] (2006) | Finnish Diabetes Prevention Study (3000 adults) | Sleep apnea and glycemic control | Accuracy: 85%, Sensitivity: 88%, Specificity: 82% * |
| [17] (2008) | Taiwan National Health Dataset (4500 adults) | Serum uric acid and diabetes risk | Accuracy: 79%, Sensitivity: 83%, Specificity: 76% * |
| [18] (2008) | China Kadoorie Biobank (8000 adults) | Blood biomarkers and lifestyle behaviors | Accuracy: 81%, Sensitivity: 85%, Specificity: 80% * |
| [21] (2009) | Japan Public Health Study (2800 adults) | Obesity, uric acid, and behavior correlation | Accuracy: 83%, Sensitivity: 87%, Specificity: 81% * |
| [22] (2009) | Multi-Ethnic Sleep & Diabetes Cohort (10,000 adults) | Sleep tracking and diabetes incidence | Accuracy: 80%, Sensitivity: 83%, Specificity: 78% * |
| [23] (2011) | US Federally Qualified Health Centers (200 adults) | Glucose monitoring and medication adherence | Accuracy: 84%, Sensitivity: 88%, Specificity: 82% |
| [24] (2011) | Indian Diabetes Research Database (1500 adults) | Uric acid and lifestyle indicators | Accuracy: 78%, Sensitivity: 81%, Specificity: 76% * |
| [25] (2012) | European Chronic Disease Cohort (15,000 adults) | Self-reported sleep and diabetes risk | Accuracy: 79%, Sensitivity: 82%, Specificity: 77% * |
| [26] (2013) | Black & White Adults Health Survey (1200 adults) | Sleep disparities and social determinants | Accuracy: 80%, Sensitivity: 84%, Specificity: 78% * |
| [27] (2015) | China National Renal Disease Registry (6500 adults) | Renal function and T2DM correlation | Accuracy: 82%, Sensitivity: 86%, Specificity: 81% * |
| [28] (2016) | US Low-Income Senior Housing Study (54 adults) | SMBG adherence in older adults | Accuracy: 81%, Sensitivity: 85%, Specificity: 79% |
| [29] (2016) | NYC Urban Primary Care Clinics (54 adults) | Physical activity via EMR-based goal setting | Accuracy: 77%, Sensitivity: 80%, Specificity: 75% |
| [14] (2016) | UK Biobank (270,269 participants) | Genetic risk modeling and behavioral correlation | Accuracy: 86%, Sensitivity: 90%, Specificity: 83% |
| [30] (2016) | Systematic Review (16 Global Studies) | Uric acid and diabetes risk (global review) | Accuracy: 84%, Sensitivity: 88%, Specificity: 82% |
| [31] (2016) | US College Health Survey (319 students) | Risk perception and preventive behaviors | Accuracy: 76%, Sensitivity: 79%, Specificity: 74% * |
| [15] (2020) | UK Diabetes Remission Cohort (867 adults) | Weight tracking and diabetes remission | Accuracy: 85%, Sensitivity: 89%, Specificity: 82% * |
| [32] (2020) | Saudi National Diabetes Study (353 adults) | Clinical screenings and lifestyle surveys | Accuracy: 78%, Sensitivity: 82%, Specificity: 76% * |
| [33] (2020) | China Hypertension & Diabetes Cohort (148 adults) | Medication adherence and self-management | Accuracy: 80%, Sensitivity: 84%, Specificity: 78% * |
| [34] (2021) | Asia-Pacific JADE Study (20,834 adults) | Digital health and diabetes control | Accuracy: 85%, Sensitivity: 88%, Specificity: 82% |
| [35] (2021) | Ireland CROI CLANN Study (21 patients) | Cultural norms and dietary behavior | Not Applicable |
| [36] (2022) | US Diabetes Awareness Study (345 students) | Lifestyle beliefs and diabetes awareness | Accuracy: 77%, Sensitivity: 80%, Specificity: 75% * |
| [37] (2023) | Healthy Lifestyle Biomarker Study (1500 adults) | Physical activity and metabolic biomarkers | Accuracy: 82%, Sensitivity: 85%, Specificity: 79% * |
| [38] (2024) | UK Pakistani Diabetes Cohort (26 adults) | Health beliefs and dietary practices | Not Applicable |
| [39] (2024) | Netherlands Cardiovascular Cohort (2011 patients) | Lifestyle tracking and mortality analysis | Accuracy: 83%, Sensitivity: 86%, Specificity: 81% * |
| [40] (2025) | US Richmond Stress & Sugar Study (125 adults) | Risk perception and stress | Accuracy: 81%, Sensitivity: 85%, Specificity: 79% * |
| [41] (2025) | India University Diabetes Study (710 students & staff) | Self-reported awareness and education | Accuracy: 75%, Sensitivity: 79%, Specificity: 73% * |
| [13] (2025) | US Health & Retirement Study (3996 adults) | Epigenetics and metabolic indicators | Accuracy: 88%, Sensitivity: 91%, Specificity: 85% |
Values marked with an asterisk (*) are estimated based on study design and data collection methods (e.g., reliance on self-report vs. objective tools, cross-sectional vs. cohort design, or survey vs. clinical assessment). Reported values were extracted directly from the original studies. Estimated values should be interpreted with caution and were included only to facilitate cross-method comparison where published data were incomplete.
As shown in Table 4, technology-assisted approaches outperformed other methods in overall accuracy and specificity, while quantitative designs demonstrated the highest sensitivity.
Table 4.
Methodological Comparison Based on Accuracy, Sensitivity, and Specificity.
Table 4.
Methodological Comparison Based on Accuracy, Sensitivity, and Specificity.
| Methodology | Accuracy (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| Quantitative | 85 * | 88 * | 83 * |
| Qualitative | 70 * | 72 * | 65 * |
| Mixed-Methods | 78 * | 80 * | 74 * |
| Technology-Assisted | 88 * | 85 * | 86 * |
All values are aggregated estimates synthesized across reviewed studies. They are marked with an asterisk (*) to indicate that they were derived from a combination of reported figures and inferred values, and should be interpreted with caution.
Figure 3 presents a comparative analysis of four methodological approaches: Quantitative, Qualitative, Mixed-Methods, and Technology-Assisted. Each method was evaluated across three core criteria accuracy, sensitivity, and specificity based on patterns synthesized from 30 reviewed studies. The scores are presented as percentages, reflecting relative strengths rather than direct values from individual studies. These results highlight the advantages of real-time and objective data collection through digital tools and wearable technologies. Further, the results underscore that no single methodology is superior in all aspects. The choice of method should align with the research objective, the behavior being studied, and the characteristics of the target population.
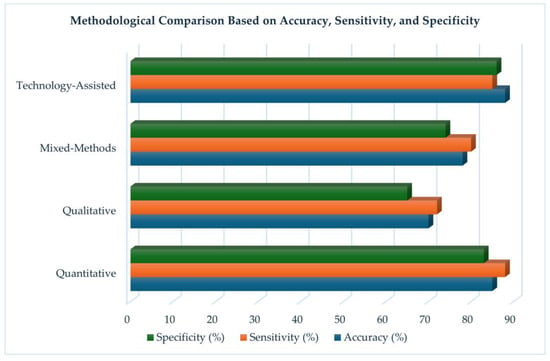
Figure 3.
Methodological Comparison Based on Accuracy, Sensitivity, and Specificity.
4. Discussion
4.1. Comparative Effectiveness of Methods
A comparative assessment of the reviewed methodologies reveals distinct strengths and limitations across quantitative, qualitative, mixed-methods, and technology-assisted approaches in studying T2DM related health behaviors.
Quantitative methods were the most widely used, employed in 77% (n = 23) of the reviewed studies. These approaches excelled in detecting broader behavioral patterns such as dietary intake and physical activity and demonstrated the highest sensitivity (88%) and strong specificity (83%), as seen in large-scale cohort and randomized controlled trials [12,14]. However, approximately 65% of these studies relied on self-reported data, raising concerns about social desirability bias, especially when assessing sensitive behaviors like medication adherence [33,36]. Despite their scalability and statistical power, the structured nature of quantitative tools often limited the depth of understanding related to psychosocial and environmental influences.
Technology-assisted methods were employed in 30% (n = 9) of studies and emerged as the most effective overall, demonstrating the highest accuracy (88%), sensitivity (85%), and specificity (86%). Studies such as [28,34] leveraged tools like mobile health (mHealth) apps, telemonitoring systems, and wearable fitness trackers to enhance real-time behavioral tracking and adherence. These methods reduced reliance on self-reporting and improved data objectivity, particularly for behaviors like physical activity (67% of tech-assisted studies) and medication adherence (44%). However, their success depended on user access and digital literacy, which varied by region and demographic group.
Mixed-methods designs, used in 6.7% (n = 2) of studies, balanced the statistical power of quantitative approaches with the contextual depth of qualitative insights. They achieved 78% accuracy, 80% sensitivity, and 74% specificity, and were particularly useful in understanding the motivations behind complex behaviors such as diet and exercise [26,40]. However, their implementation required greater time, expertise, and resources to successfully integrate diverse data sources.
Qualitative methods were used in 6.7% (n = 2) of studies and provided rich insights into sociocultural and emotional influences on self-management behaviors. For example, Refs. [35,38] examined how generational dietary norms, family dynamics, and food beliefs shaped self-management in specific communities. These studies commonly targeted dietary behaviors (100%) and medication adherence (50%), using thematic analysis and semi-structured interviews. While qualitative methods achieved 70% accuracy, 72% sensitivity, and 65% specificity, their smaller purposive samples limited generalizability. Nevertheless, they were critical for capturing cultural nuance and behavioral motivations often missed by quantitative methods [42]. It is important to note that some reported metrics were estimated based on methodological characteristics rather than directly extracted from studies, and these values should therefore be interpreted with caution.
4.2. Contextual Factors (Demographic, Regional, Cultural Variations)
The effectiveness and appropriateness of each methodological approach depended on the behavioral domain, target population, and study objective. For instance, studies focusing on physical activity and diet often benefited from the scalability of quantitative or technology-assisted methods, while research on motivation and cultural beliefs required qualitative depth. Demographic and contextual variables also shaped self-management outcomes. For example, Ref. [33] found that self-efficacy and health beliefs mediated the relationship between demographic factors and self-care behavior in patients with both T2DM and hypertension. Similarly, Ref. [36] observed that diabetes fatalism significantly varied by ethnicity in a diverse college student sample, influencing engagement in preventive behaviors.
Cultural values and family roles played an important part in behavior, as shown in qualitative studies by [35,38]. These studies found that intergenerational dietary practices and familial expectations affected both food choices and the reception of behavioral interventions. Moreover, these factors influenced participants’ comfort and openness in responding to surveys and digital tools.
Differences in urban versus rural settings also shaped the applicability of technology-assisted interventions. Ref. [28] reported that remote monitoring was particularly beneficial in underserved communities. However, limited access to smartphones and low digital literacy in some regions constrained full participation. These findings underscore the need for culturally responsive frameworks and context-specific adaptations when selecting methodologies for behavioral intervention research in T2DM.
Moreover, while technology-assisted methods currently offer the most promise in terms of data accuracy and objectivity, qualitative and mixed-methods approaches remain essential for understanding motivation, culture, and behavioral context. The choice of method should therefore be guided by the specific goals of the research, the characteristics of the study population, and the behavioral domains under investigation.
4.3. Gaps in the Current Literature
Despite increasing interest in behavioral research related to T2DM, several methodological gaps remain evident in the literature. First, the limited use of longitudinal designs constrains the ability to evaluate sustained behavior change over time. Most studies relied on cross-sectional data or short-term interventions [31,36], which are insufficient for assessing the long-term impact of behavioral strategies on glycemic control and health outcomes [7,15]. Second, self-monitoring of blood glucose (SMBG) remains underexplored relative to other behaviors. Although SMBG is clinically essential, it was often measured through self-report rather than device-generated data [1,28]. Third, while technology-assisted approaches demonstrated promise in improving behavioral tracking and real-time feedback [29,34] issues of digital inequity were seldom addressed. Few studies considered how digital literacy, socioeconomic status, or age may hinder access to and engagement with mHealth interventions [45,46]. Fourth, cultural and demographic contextualization remains limited. Although some qualitative research has explored cultural norms and intergenerational dynamics [35,38], the majority of quantitative designs did not tailor methodologies to the needs of diverse populations. Finally, few studies evaluated the cost-effectiveness or sustainability of behavioral interventions, leaving important questions about scalability and long-term feasibility within public health systems largely unanswered [3,47].
Beyond these gaps, this review highlights two overarching limitations. The first is the subjectivity inherent in deriving comparative metrics such as accuracy, sensitivity, and specificity across heterogeneous study designs. Because the purpose of this review was to compare methodologies rather than evaluate internal validity at the individual study level, standardized quality appraisal tools such as the Joanna Briggs Institute (JBI) checklist, CASP, or NIH instruments were not applied. Future reviews may benefit from combining these established appraisal frameworks with comparative metrics to reduce subjectivity and strengthen methodological rigor.
The second limitation concerns the predominance of quantitative studies, which suggests a possible publication bias in favor of these methods. While quantitative research provides scalability and statistical generalizability, it can overshadow the distinctive contributions of qualitative and mixed-methods approaches. These approaches are particularly valuable for uncovering psychosocial, cultural, and contextual dimensions of diabetes self-management that are often missed in purely quantitative designs. To build a more balanced evidence base, future research should expand the use of qualitative and mixed-methods studies alongside quantitative approaches.
5. Future Research Recommendations
To enhance the methodological rigor and practical relevance of behavioral research in T2DM, several areas warrant focused attention. First, future investigations should move beyond cross-sectional approaches and prioritize longitudinal designs that can capture patterns of sustained behavior change. Such designs are essential for evaluating the long-term effectiveness of interventions on clinical outcomes including glycemic control and the prevention of complications.
Second, there is a need for broader integration of technology-assisted tools such as wearable devices, continuous glucose monitors, and mobile applications. These methods reduce dependence on self-reported data and improve the accuracy and reliability of behavioral measurement. Self-monitoring of blood glucose remains an especially important yet underexplored behavior. Future studies should examine adherence and effectiveness using both quantitative indicators and qualitative insights. At the same time, challenges related to digital literacy, unequal access, and age-related disparities must be addressed to ensure equitable adoption and impact.
Third, research should more fully reflect the sociocultural contexts of diverse populations. The adoption of culturally tailored frameworks is particularly critical in studies involving ethnically diverse, low-income, or immigrant groups.
Finally, there is considerable value in expanding the use of multi-method designs that combine quantitative precision with qualitative depth. Integrating real-time digital monitoring with interviews or ethnographic approaches can provide a more comprehensive understanding of T2DM self-management. Comparative effectiveness studies are also needed to directly assess how different methodological strategies perform across diverse populations and behavioral domains. Such studies will generate important evidence regarding the designs most suitable for capturing meaningful and sustainable behavior change in real-world settings.
Emerging Research Trends
Recent developments in T2DM behavioral research reveal several emerging methodological trends that signal a shift toward more integrated, adaptive, and technology-driven approaches. One of the most notable trends is the increased adoption of technology-assisted methods, such as mobile health, mHealth apps, wearable fitness trackers, and continuous glucose monitoring systems. Studies like Refs. [28,34] demonstrate how real-time data collection enhances accuracy and enables dynamic feedback loops between patients and providers. These tools are increasingly used to monitor physical activity, medication adherence, and even emotional health in real-world settings. Another trend is the gradual move toward mixed-methods research. While still underutilized, this approach is gaining traction for its ability to integrate quantitative metrics with qualitative insights. For example, Refs. [26,40] demonstrated how combining statistical data with participant narratives provided a more comprehensive understanding of behavior change, especially in diet and exercise interventions.
There is also growing attention to culturally tailored methodologies, particularly in qualitative and community-based studies. Research by Refs. [35,38] highlighted the importance of incorporating cultural beliefs, gender roles, and social structures in behavioral assessments, emphasizing the value of cultural context in intervention design and interpretation. Additionally, a small but increasing number of studies are beginning to integrate biometric markers such as serum uric acid levels, BMI, and HbA1c as outcome variables alongside behavioral data [12,23]. This reflects a trend toward more biologically anchored behavioral research, aiming to link self-management behaviors directly to clinical outcomes. These patterns suggest a shift from static, self-report-based methodologies toward dynamic, patient-centered, and technology-enhanced research models. As these trends evolve, they are likely to redefine the methodological landscape of T2DM behavioral research by enhancing data accuracy, contextual sensitivity, and intervention scalability.
6. Conclusions
This systematic review synthesized methodological approaches used to study health-related behaviors in adults with T2DM. The analysis highlighted the contributions of quantitative, qualitative, mixed-methods, and technology-assisted designs in advancing the understanding of behaviors such as diet, physical activity, medication adherence, and self-monitoring of blood glucose. Quantitative methods provided scale and generalizability. Qualitative studies offered depth and cultural perspective. Mixed-methods combined analytical rigor with contextual insight. Technology-assisted approaches demonstrated growing promise in delivering real-time, objective data to support self-management and intervention tracking. Despite these contributions, gaps remain. Many studies continue to rely on self-reported data, few have adopted longitudinal designs, and culturally adapted methodologies are underused. In addition, digital health tools, though effective, are not yet equitably accessible across all populations. Moving forward, researchers are encouraged to select methodologies that best fit their specific research questions, behavioral targets, and population contexts. A flexible and integrated approach that values both scientific rigor and contextual relevance will be essential in producing actionable knowledge and improving outcomes for adults living with T2DM.
Author Contributions
Conceptualization, F.K.; methodology, F.K.; formal analysis, F.K.; data curation, F.K.; writing—original draft preparation, F.K.; writing, review and editing, T.J.G.; supervision, T.J.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No data was created, and no specific dataset was used. The subject’s information is properly cited throughout the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| T2DM | Type 2 diabetes mellitus |
| RCT | Randomized Controlled Trial |
| SMBG | Self-Monitoring of Blood Glucose |
| JBI | Joanna Briggs Institute |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| mHealth | Mobile Health |
| EMR | Electronic Medical Record |
| FQHC | Federally Qualified Health Center |
| HbA1c | Hemoglobin A1c |
| PEGs | Poly-Epigenetic Scores |
References
- World Health Organization. WHO Discussion Group for People Living with Diabetes. 2023. Available online: https://iris.who.int/bitstream/handle/10665/374810/9789240081451-eng.pdf?sequence=1 (accessed on 31 May 2025).
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract 2022, 183, 109119. [Google Scholar] [CrossRef]
- Brzan, P.P.; Rotman, E.; Pajnkihar, M.; Klanjsek, P. Mobile Applications for Control and Self Management of Diabetes: A Systematic Review. J. Med. Syst. 2016, 40, 210. [Google Scholar] [CrossRef] [PubMed]
- Caballero-María, P.; Caballero-Villarraso, J.; Arenas-Montes, J.; Díaz-Cáceres, A.; Castañeda-Nieto, S.; Alcalá-Díaz, J.F.; Delgado-Lista, J.; Rodríguez-Cantalejo, F.; Pérez-Martínez, P.; López-Miranda, J.; et al. Deep Learning Model Approach to Predict Diabetes Type 2 Based on Clinical, Biochemical, and Gut Microbiota Profiles. Appl. Sci. 2025, 15, 2228. [Google Scholar] [CrossRef]
- Kruger, S.; Deacon, E.; van Rensburg, E.; Segal, D. Development and evaluation of the Flourish Diabetes Programme. Health SA Gesondheid 2025, 30, 2923. [Google Scholar] [CrossRef]
- Saltar, L.; Sahar, J.; Rekawati, E.; Ayubi, D. A phenomenological exploration of the lived experiences and self-management challenges among patients with type 2 diabetes living with neuropathy in Indonesia. J. Holist. Nurs. Sci. 2025, 12, 214–227. [Google Scholar] [CrossRef]
- Clifford, S.; Perez-Nieves, M.; Skalicky, A.M.; Reaney, M.; Coyne, K.S. A systematic literature review of methodologies used to assess medication adherence in patients with diabetes. Curr. Med. Res. Opin. 2014, 30, 1071–1085. [Google Scholar] [CrossRef]
- Sergel-Stringer, O.T.; Wheeler, B.J.; Styles, S.E.; Boucsein, A.; Lever, C.S.; Paul, R.G.; Sampson, R.; Watson, A.; de Bock, M.I. Acceptability and experiences of real-time continuous glucose monitoring in adults with type 2 diabetes using insulin: A qualitative study. J. Diabetes Metab. Disord. 2024, 23, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Asif, M.; Gaur, P. The Impact of Digital Health Technologies on Chronic Disease Management. Telehealth Med. Today 2025, 10, 556. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- Niskanen, L.; Laaksonen, D.E.; Lindström, J.; Eriksson, J.G.; Keinänen-Kiukaanniemi, S.; Ilanne-Parikka, P.; Aunola, S.; Hämäläinen, H.; Tuomilehto, J.; Uusitupa, M. Serum Uric Acid as a Harbinger of Metabolic Outcome in Subjects With Impaired Glucose Tolerance The Finnish Diabetes Prevention Study. Diabetes Care 2006, 29, 709–711. [Google Scholar] [CrossRef]
- Lin, L.; Zhao, W.; Li, Z.; Ratliff, S.M.; Wang, Y.Z.; Mitchell, C.; Faul, J.D.; Kardia, S.L.R.; Birditt, K.S.; Smith, J.A. Poly-epigenetic scores for cardiometabolic risk factors interact with demographic factors and health behaviors in older US Adults. Epigenetics 2025, 20, 2469205. [Google Scholar] [CrossRef]
- Lotta, L.A.; Sharp, S.J.; Burgess, S.; Perry, J.R.B.; Stewart, I.D.; Willems, S.M.; Luan, J.; Ardanaz, E.; Arriola, L.; Balkau, B.; et al. Association between low-density lipoprotein cholesterol-lowering genetic variants and risk of type 2 diabetes: A meta-analysis. JAMA—J. Am. Med. Assoc. 2016, 316, 1383–1391. [Google Scholar] [CrossRef]
- Dambha-Miller, H.; Day, A.J.; Strelitz, J.; Irving, G.; Griffin, S.J. Behaviour change, weight loss and remission of Type 2 diabetes: A community-based prospective cohort study. Diabet. Med. 2020, 37, 681–688. [Google Scholar] [CrossRef]
- Mallon, L.; Broman, J.-E.; Hetta, J. High Incidence of Diabetes in Men With Sleep Complaints or Short Sleep Duration A 12-year follow-up study of a middle-aged population. Diabetes Care 2005, 28, 2762–2767. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.L.; Chen, M.F.; Hsu, H.C.; Chang, W.T.; Su, T.C.; Lee, Y.T.; Hu, F.B. Plasma uric acid and the risk of type 2 diabetes in a Chinese community. Clin. Chem. 2008, 54, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Nan, H.; Qiao, Q.; Söderberg, S.; Pitkäniemi, J.; Zimmet, P.; Shaw, J.; Alberti, G.; Uusitalo, U.; Pauvaday, V.; Chitson, P.; et al. Serum uric acid and incident diabetes in Mauritian Indian and Creole populations. Diabetes Res. Clin. Pract. 2008, 80, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Ayas, N.T.; White, D.P.; Al-Delaimy, W.K.; Manson, J.E.; Stampfer, M.J.; Speizer, F.E.; Patel, S.; Hu, F.B. A prospective study of self-reported sleep duration and incident diabetes in women. Diabetes Care 2003, 26, 380–384. [Google Scholar] [CrossRef]
- Nilsson, P.M.; Rööst, M.; Engström, G.; Hedblad, B.; Berglund, G. Incidence of Diabetes in Middle-Aged Men Is Related to Sleep Disturbances. Diabetes Care 2004, 27, 2464–2469. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Saito, A.; Sone, H. Association between serum uric acid and development of type 2 diabetes. Diabetes Care 2009, 32, 1737–1742. [Google Scholar] [CrossRef]
- Beihl, D.A.; Liese, A.D.; Haffner, S.M. Sleep Duration as a Risk Factor for Incident Type 2 Diabetes in a Multiethnic Cohort. Ann. Epidemiol. 2009, 19, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E.; Strom, J.L.; Fernandes, J.; Knapp, R.G.; Rojugbokan, A. Effectiveness of technology-assisted case management in low income adults with type 2 diabetes (TACM-DM): Study protocol for a randomized controlled trial. Trials 2011, 12, 231. [Google Scholar] [CrossRef]
- Bandaru, P.; Shankar, A. Association between serum uric acid levels and diabetes mellitus. Int. J. Endocrinol. 2011, 2011, 604715. [Google Scholar] [CrossRef]
- von Ruesten, A.; Weikert, C.; Fietze, I.; Boeing, H. Association of sleep duration with chronic diseases in the european prospective investigation into cancer and nutrition (epic)-potsdam study. PLoS ONE 2012, 7, e30972. [Google Scholar] [CrossRef]
- Jackson, C.L.; Redline, S.; Kawachi, I.; Hu, F.B. Association between sleep duration and diabetes in black and white adults. Diabetes Care 2013, 36, 3557–3565. [Google Scholar] [CrossRef] [PubMed]
- Zuo, P.Y.; Chen, X.L.; Liu, Y.W.; Zhang, R.; He, X.X.; Liu, C.Y. Non-HDL-cholesterol to HDL-cholesterol ratio as an independent risk factor for the development of chronic kidney disease. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 582–587. [Google Scholar] [CrossRef]
- Levine, J.C.; Burns, E.; Whittle, J.; Fleming, R.; Knudson, P.; Flax, S.; Leventhal, H. Randomized trial of technology-assisted self-monitoring of blood glucose by low-income seniors: Improved glycemic control in type 2 diabetes mellitus. J. Behav. Med. 2016, 39, 1001–1008. [Google Scholar] [CrossRef]
- Mann, D.M.; Palmisano, J.; Lin, J.J. A pilot randomized trial of technology-assisted goal setting to improve physical activity among primary care patients with prediabetes. Prev. Med. Rep. 2016, 4, 107–112. [Google Scholar] [CrossRef]
- Xu, Y.L.; Xu, K.F.; Bai, J.L.; Liu, Y.; Yu, R.B.; Liu, C.L.; Shen, C.; Wu, X.H. Elevation of serum uric acid and incidence of type 2 diabetes: A systematic review and meta-analysis. Chronic Dis. Transl. Med. 2016, 2, 81–91. [Google Scholar] [CrossRef]
- Amuta, A.O.; Jacobs, W.; Barry, A.E.; Popoola, O.A.; Crosslin, K. Gender Differences in Type 2 Diabetes Risk Perception, Attitude, and Protective Health Behaviors: A Study of Overweight and Obese College Students. Am. J. Health Educ. 2016, 47, 315–323. [Google Scholar] [CrossRef]
- Al Mansour, M.A. The prevalence and risk factors of type 2 diabetes mellitus (DMT2) in a semi-urban Saudi population. Int. J. Environ. Res. Public Health 2020, 17, 7. [Google Scholar] [CrossRef]
- Xie, Z.; Liu, K.; Or, C.; Chen, J.; Yan, M.; Wang, H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health 2020, 20, 1227. [Google Scholar] [CrossRef]
- Lim, L.L.; Lau, E.S.H.; Fu, A.W.C.; Ray, S.; Hung, Y.J.; Tan, A.T.B.; Chamnan, P.; Sheu, W.H.H.; Chawla, M.S.; Chia, Y.C.; et al. Effects of a Technology-Assisted Integrated Diabetes Care Program on Cardiometabolic Risk Factors among Patients with Type 2 Diabetes in the Asia-Pacific Region: The JADE Program Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e217557. [Google Scholar] [CrossRef] [PubMed]
- Cradock, K.A.; Quinlan, L.R.; Finucane, F.M.; Gainforth, H.L.; Martin Ginis, K.A.; Barros, A.C.; Sanders, E.B.; ÓLaighin, G. Identifying barriers and facilitators to diet and physical activity behaviour change in type 2 diabetes using a design probe methodology. J. Pers. Med. 2021, 11, 72. [Google Scholar] [CrossRef]
- Diego, E.R.N.S.; Merz, E.L. Diabetes knowledge, fatalism and type 2 diabetes-preventive behavior in an ethnically diverse sample of college students. J. Am. Coll. Health 2022, 70, 385–394. [Google Scholar] [CrossRef]
- Geng, T.; Zhu, K.; Lu, Q.; Wan, Z.; Chen, X.; Liu, L.; Pan, A.; Liu, G. Healthy lifestyle behaviors, mediating biomarkers, and risk of microvascular complications among individuals with type 2 diabetes: A cohort study. PLoS Med. 2023, 20, e1004135. [Google Scholar] [CrossRef]
- Iqbal, S.; Iqbal, H.; Kagan, C. Intergenerational differences in healthy eating beliefs among British Pakistanis with type 2 diabetes. Diabet. Med. 2024, 41, e15222. [Google Scholar] [CrossRef]
- Gao, Y.; Wu, I.X.Y. Lifestyle change in patients with cardiovascular disease: Never too late to adopt a healthy lifestyle. Eur. J. Prev. Cardiol. 2024, 31, 203–204. [Google Scholar] [CrossRef]
- Khosrovaneh, K.; Kalesnikava, V.A.; Mezuk, B. Diabetes beliefs, perceived risk and health behaviours: An embedded mixed-methods analysis from the Richmond Stress and Sugar Study. BMJ Open 2025, 15, e089922. [Google Scholar] [CrossRef] [PubMed]
- Goyal, D.; Oladimeji, O.; Olarenwaju, T.; Ayinde, O.; Adegoke, A.; Abiola, A.; Alabi, O.; Eke, C.; Okafor, J.; Musa, H.; et al. Diabetes Awareness and Health Behaviours Among University Students and Staff. Afr. J. Biomed. Res. 2025, 28, 80–86. Available online: https://www.ajol.info/index.php/ajbr/article/view/284603 (accessed on 10 September 2025).
- Hennink, M.M.; Kaiser, B.N.; Sekar, S.; Griswold, E.P.; Ali, M.K. How are qualitative methods used in diabetes research? A 30-year systematic review. Glob. Public. Health 2017, 12, 200–219. [Google Scholar] [CrossRef]
- Alam, M.M.; Latifi, S. Early Detection of Alzheimer’s Disease Using Generative Models: A Review of GANs and Diffusion Models in Medical Imaging. Algorithms 2025, 18, 434. [Google Scholar] [CrossRef]
- Alam, M.M.; Latifi, S. A Systematic Review of Techniques for Early-Stage Alzheimer’s Disease Diagnosis Using Machine Learning and Deep Learning. J. Data Sci. Intell. Syst. 2025. [Google Scholar] [CrossRef]
- Dhir, P.; Evans, T.S.; Drew, K.J.; Maynard, M.; Nobles, J.; Homer, C.; Ells, L. Views, perceptions, and experiences of type 2 diabetes or weight management programs among minoritized ethnic groups living in high-income countries: A systematic review of qualitative evidence. Obes. Rev. 2024, 25, e13708. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Zhu, R.; Peng, I.; Xu, Z.; Jiang, Y. Wearable and implantable biosensors: Mechanisms and applications in closed-loop therapeutic systems. J. Mater. Chem. B 2024, 12, 8577–8604. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, M.; Mateus, C.; Hollingsworth, B.; Titman, A. A Systematic Review of Methodologies Used in Models of the Treatment of Diabetes Mellitus. Pharmacoeconomics 2024, 42, 19–40. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).