
The Effects of Nutritional Education and School-Based Exercise Intervention Programs on Preschool and Primary School Children’s Cardiometabolic Biomarkers: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Information Sources
2.3. Search Strategy
(“early childhood” OR preschool OR kindergarten OR school* OR “primary education” OR “elementary education”) AND (Nutrient* OR nutrition OR food* OR DIET*) AND (exercise OR “Physical activity” OR “physical education” OR sport OR fitness OR aerobic OR movement) AND (program* OR intervention) AND (blood) AND (“randomized controlled trial*”)
2.4. Eligibility Criteria
2.5. Data Extraction
2.6. Assessment of Study Methodology and Risk of Bias
3. Results
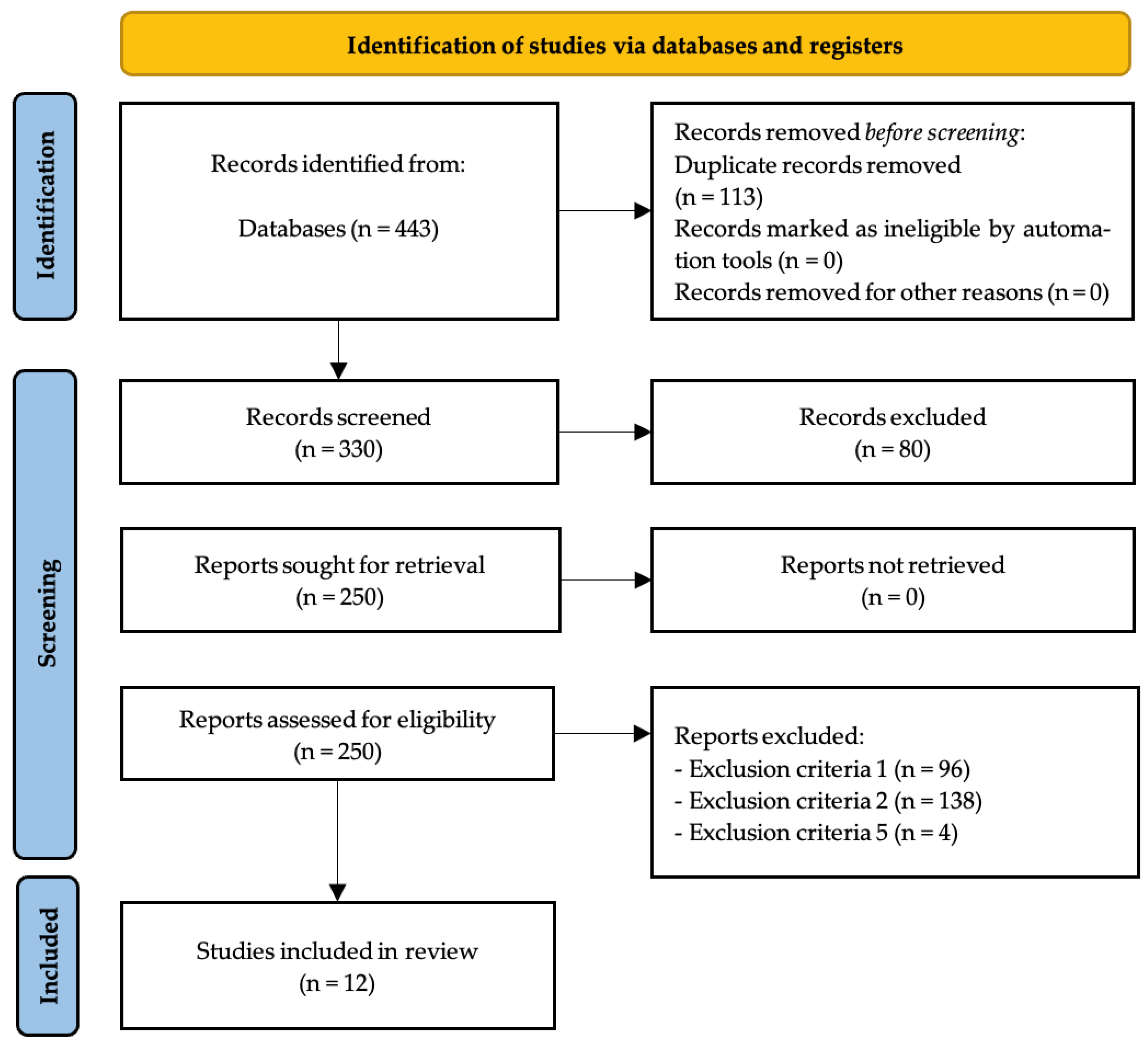
3.1. Study Selection and Inclusion Process
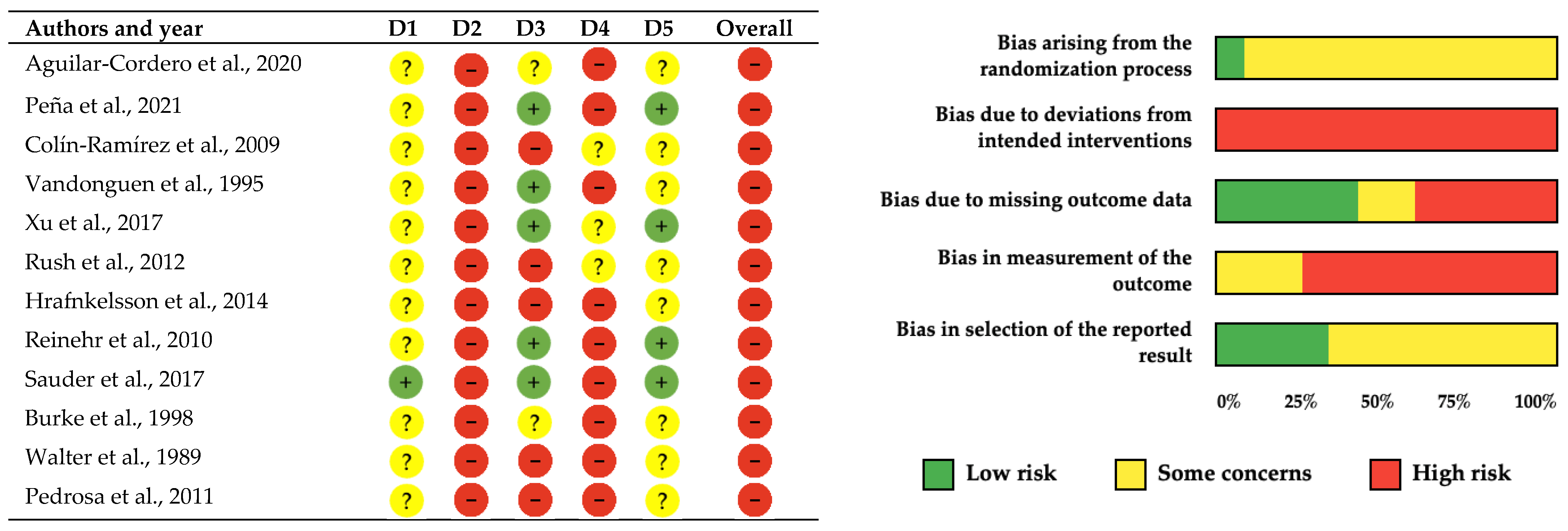
3.2. Methodological Quality and Risk of Bias Assessment
3.3. Study Characteristics
3.3.1. Quantitative Synthesis
3.3.2. Qualitative Synthesis
4. Discussion
4.1. Main Findings and Clinical Relevance
4.2. Intervention Characteristics and Effectiveness
4.3. Mechanistic Considerations
4.4. Sex and Geographic Context Considerations
4.5. Public Health Implications
4.6. Limitations and Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Garrido-Miguel, M.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Rodríguez-Artalejo, F.; Moreno, L.A.; Ruiz, J.R.; Ahrens, W.; Martínez-Vizcaíno, V. Prevalence and Trends of Overweight and Obesity in European Children from 1999 to 2016: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2019, 173, e192430. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, J.; Ni, Y.; Yi, C.; Fang, Y.; Ning, Q.; Shen, B.; Zhang, K.; Liu, Y.; Yang, L.; et al. Global Prevalence of Overweight and Obesity in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2024, 178, 800. [Google Scholar] [CrossRef]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to Prevent Global Childhood Overweight and Obesity: A Systematic Review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef]
- Liu, Z.; Xu, H.-M.; Wen, L.-M.; Peng, Y.-Z.; Lin, L.-Z.; Zhou, S.; Li, W.-H.; Wang, H.-J. A Systematic Review and Meta-Analysis of the Overall Effects of School-Based Obesity Prevention Interventions and Effect Differences by Intervention Components. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 95. [Google Scholar] [CrossRef]
- World Health Organization Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 July 2025).
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Childhood Adiposity, Adult Adiposity, and Cardiovascular Risk Factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar] [CrossRef]
- Takehara, K.; Togoobaatar, G.; Kikuchi, A.; Lkhagvasuren, G.; Lkhagvasuren, A.; Aoki, A.; Fukuie, T.; Shagdar, B.-E.; Suwabe, K.; Mikami, M.; et al. Exercise Intervention for Academic Achievement Among Children: A Randomized Controlled Trial. Pediatrics 2021, 148, e2021052808. [Google Scholar] [CrossRef]
- Fan, B.; Zhang, T.; Li, S.; Yan, Y.; Fan, L.; Bazzano, L.; He, J.; Chen, W. Differential Roles of Life-Course Cumulative Burden of Cardiovascular Risk Factors in Arterial Stiffness and Thickness. Can. J. Cardiol. 2022, 38, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizar, F.; Voortman, T. Arterial Stiffness in Childhood: A Predictor for Later Cardiovascular Disease? J. Cardiovasc. Risk 2018, 25, 100–102. [Google Scholar] [CrossRef]
- Murray, E.T.; Hardy, R.; Hughes, A.; Wills, A.; Sattar, N.; Deanfield, J.; Kuh, D.; Whincup, P. Overweight across the Life Course and Adipokines, Inflammatory and Endothelial Markers at Age 60–64 Years: Evidence from the 1946 Birth Cohort. Int. J. Obes. 2015, 39, 1010–1018. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of Physical Activity from Early Childhood through Youth into Adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef]
- Tapia-Serrano, M.A.; Sevil-Serrano, J.; Sánchez-Oliva, D.; Vaquero-Solís, M.; Sánchez-Miguel, P.A. Effects of a School-Based Intervention on Physical Activity, Sleep Duration, Screen Time, and Diet in Children. Rev. Psicodidáct. Engl. Ed 2022, 27, 56–65. [Google Scholar] [CrossRef]
- Evans, C.E.L.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic Review and Meta-Analysis of School-Based Interventions to Improve Daily Fruit and Vegetable Intake in Children Aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef]
- Nikooyeh, B.; Yari, Z.; Hariri, Z.; Baghdadi, G.; Yazdani, H.; Motlagh, M.E.; Neyestani, T.R. Which School-Based Interventions Work Better to Combat Obesity in Children? A Network Meta-Analysis. Syst. Rev. 2025, 14, 125. [Google Scholar] [CrossRef]
- Bustos, N.; Olivares, S.; Leyton, B.; Cano, M.; Albala, C. Impact of a School-Based Intervention on Nutritional Education and Physical Activity in Primary Public Schools in Chile (KIND) Programme Study Protocol: Cluster Randomised Controlled Trial. BMC Public Health 2016, 16, 1217. [Google Scholar] [CrossRef]
- Monsalves-Alvarez, M. Motor Skills and Nutritional Status Outcomes from a Physical Activity Intervention in Short Breaks on Preschool Children Conducted by Their Educators: A Pilot Study. Nutr. Hosp. 2015, 32, 1576–1581. [Google Scholar] [CrossRef] [PubMed]
- Hilger-Kolb, J.; Bosle, C.; Motoc, I.; Hoffmann, K. Associations between Dietary Factors and Obesity-Related Biomarkers in Healthy Children and Adolescents—A Systematic Review. Nutr. J. 2017, 16, 85. [Google Scholar] [CrossRef] [PubMed]
- Zafarmand, M.H.; Spanjer, M.; Nicolaou, M.; Wijnhoven, H.A.H.; van Schaik, B.D.C.; Uitterlinden, A.G.; Snieder, H.; Vrijkotte, T.G.M. Influence of Dietary Approaches to Stop Hypertension-Type Diet, Known Genetic Variants and Their Interplay on Blood Pressure in Early Childhood: ABCD Study. Hypertension 2020, 75, 59–70. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; García-Hermoso, A.; Martínez-González, M.Á.; Rodríguez-Artalejo, F. Mediterranean Diet and Cardiometabolic Biomarkers in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2024, 7, e2421976. [Google Scholar] [CrossRef]
- Obarzanek, E.; Kimm, S.Y.; Barton, B.A.; Van Horn, L.; Kwiterovich, P.O.; Simons-Morton, D.G.; Hunsberger, S.A.; Lasser, N.L.; Robson, A.M.; Franklin, F.A.; et al. Long-Term Safety and Efficacy of a Cholesterol-Lowering Diet in Children with Elevated Low-Density Lipoprotein Cholesterol: Seven-Year Results of the Dietary Intervention Study in Children (DISC). Pediatrics 2001, 107, 256–264. [Google Scholar] [CrossRef]
- Visuthranukul, C.; Sirimongkol, P.; Prachansuwan, A.; Pruksananonda, C.; Chomtho, S. Low-Glycemic Index Diet May Improve Insulin Sensitivity in Obese Children. Pediatr. Res. 2015, 78, 567–573. [Google Scholar] [CrossRef]
- Laitinen, T.T.; Nuotio, J.; Niinikoski, H.; Juonala, M.; Rovio, S.P.; Viikari, J.S.A.; Rönnemaa, T.; Magnussen, C.G.; Sabin, M.; Burgner, D.; et al. Attainment of Targets of the 20-Year Infancy-Onset Dietary Intervention and Blood Pressure Across Childhood and Young Adulthood: The Special Turku Coronary Risk Factor Intervention Project (STRIP). Hypertension 2020, 76, 1572–1579. [Google Scholar] [CrossRef]
- Wang, H.; Cheng, R.; Xie, L.; Hu, F. Comparative Efficacy of Exercise Training Modes on Systemic Metabolic Health in Adults with Overweight and Obesity: A Network Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2023, 14, 1294362. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Effects of Exercise on BMI Z-Score in Overweight and Obese Children and Adolescents: A Systematic Review with Meta-Analysis. BMC Pediatr. 2014, 14, 225. [Google Scholar] [CrossRef]
- Chen, L.; Liu, Q.; Xu, F.; Wang, F.; Luo, S.; An, X.; Chen, J.; Tang, N.; Jiang, X.; Liang, X. Effect of Physical Activity on Anxiety, Depression and Obesity Index in Children and Adolescents with Obesity: A Meta-Analysis. J. Affect. Disord. 2024, 354, 275–285. [Google Scholar] [CrossRef]
- Ameryoun, A.; Sanaeinasab, H.; Saffari, M.; Koenig, H.G. Impact of Game-Based Health Promotion Programs on Body Mass Index in Overweight/Obese Children and Adolescents: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Child. Obes. 2018, 14, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Q.; Lu, F.; Zhu, D. Effects of Aerobic Exercise Combined with Resistance Training on Body Composition and Metabolic Health in Children and Adolescents with Overweight or Obesity: Systematic Review and Meta-Analysis. Front. Public Health 2024, 12, 1409660. [Google Scholar] [CrossRef]
- García-Hermoso, A.; López-Gil, J.F.; Izquierdo, M.; Ramírez-Vélez, R.; Ezzatvar, Y. Exercise and Insulin Resistance Markers in Children and Adolescents with Excess Weight: A Systematic Review and Network Meta-Analysis. JAMA Pediatr. 2023, 177, 1276–1284. [Google Scholar] [CrossRef]
- Jiménez-Peláez, C.C.; Fernández-Aparicio, Á.; Montero-Alonso, M.A.; González-Jiménez, E. Effect of Dietary and Physical Activity Interventions Combined with Psychological and Behavioral Strategies on Preventing Metabolic Syndrome in Adolescents with Obesity: A Meta-Analysis of Clinical Trials. Nutrients 2025, 17, 2051. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Gao, X.; Chen, M.; van Dam, R.M. Long-Term Effectiveness of Diet-plus-Exercise Interventions vs. Diet-Only Interventions for Weight Loss: A Meta-Analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2009, 10, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Racey, M.; Ali, M.U.; Sherifali, D.; Fitzpatrick-Lewis, D.; Lewis, R.; Jovkovic, M.; Gramlich, L.; Keller, H.; Holroyd-Leduc, J.; Giguère, A.; et al. Effectiveness of Nutrition Interventions and Combined Nutrition and Physical Activity Interventions in Older Adults with Frailty or Prefrailty: A Systematic Review and Meta-Analysis. CMAJ Open 2021, 9, E744–E756. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Caldwell, H.; Dobbins, M. School-Based Physical Activity Programs for Promoting Physical Activity and Fitness in Children and Adolescents Aged 6 to 18. Cochrane Database Syst. Rev. 2021, 9, CD007651. [Google Scholar] [CrossRef]
- Rico-González, M. The Effect of Primary School-Based Physical Education Programs: A Systematic Review of Randomized Controlled Trials. J. Phys. Act. Health 2023, 20, 317–347. [Google Scholar] [CrossRef]
- Armstrong, N. Paediatric Exercise Physiology: Advances in Sport and Exercise, 1st ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2006; ISBN 978-0-7020-3492-3. [Google Scholar]
- Gao, S.; Yang, L.; Li, Y.; Liu, S.; Zhang, H.; Arens, E.; Zhai, Y. Metabolic Rate in Children and Adolescents: Tabulate Values for Common Activities and Comparisons with Standards and Adult Values. Build. Environ. 2023, 244, 110804. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Rico-González, M.; Pino-Ortega, J.; Clemente, F.M.; Los Arcos, A. Guidelines for Performing Systematic Reviews in Sports Science. Biol. Sport 2022, 39, 463–471. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Colín Ramírez, E.; Castillo Martínez, L.; Orea Tejeda, A.; Vergara, A.; Villa, A.R. Efecto de una intervención escolar basada en actividad física y dieta para la prevención de factores de riesgo cardiovascular (RESCATE). Rev. Esp. Nutr. Comunitaria Span. J. Community Nutr. 2009, 15, 71–80. [Google Scholar]
- Xu, H.; Li, Y.; Zhang, Q.; Hu, X.; Liu, A.; Du, S.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Comprehensive School-Based Intervention to Control Overweight and Obesity in China: A Cluster Randomized Controlled Trial. Asia Pac. J. Clin. Nutr. 2017, 26, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Walter, H.J. Primary Prevention of Chronic Disease among Children: The School-Based “Know Your Body” Intervention Trials. Health Educ. Q. 1989, 16, 201–214. [Google Scholar] [CrossRef]
- Vandongen, R.; Jenner, D.A.; Thompson, C.; Taggart, A.C.; Spickett, E.E.; Burke, V.; Beilin, L.J.; Milligan, R.A.; Dunbar, D.L. A Controlled Evaluation of a Fitness and Nutrition Intervention Program on Cardiovascular Health in 10-Year-Old to 12-Year-Old Children. Prev. Med. 1995, 24, 9–22. [Google Scholar] [CrossRef]
- Rush, E.; Reed, P.; McLennan, S.; Coppinger, T.; Simmons, D.; Graham, D. A School-Based Obesity Control Programme: Project Energize. Two-Year Outcomes. Br. J. Nutr. 2012, 107, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Sauder, K.A.; Dabelea, D.; Bailey-Callahan, R.; Kanott Lambert, S.; Powell, J.; James, R.; Percy, C.; Jenks, B.F.; Testaverde, L.; Thomas, J.M.; et al. Targeting Risk Factors for Type 2 Diabetes in American Indian Youth: The Tribal Turning Point Pilot Study. Pediatr. Obes. 2018, 13, 321–329. [Google Scholar] [CrossRef]
- Burke, V.; Milligan, R.A.; Thompson, C.; Taggart, A.C.; Dunbar, D.L.; Spencer, M.J.; Medland, A.; Gracey, M.P.; Vandongen, R.; Beilin, L.J. A Controlled Trial of Health Promotion Programs in 11-Year-Olds Using Physical Activity “Enrichment” for Higher Risk Children. J. Pediatr. 1998, 132, 840–848. [Google Scholar] [CrossRef]
- Aguilar-Cordero, M.J.; Rodríguez-Blanque, R.; Leon-Ríos, X.; Expósito Ruiz, M.; García García, I.; Sánchez-López, A.M. Influence of Physical Activity on Blood Pressure in Children with Overweight/Obesity: A Randomized Clinical Trial. Am. J. Hypertens. 2020, 33, 131–136. [Google Scholar] [CrossRef]
- Peña, S.; Carranza, M.; Cuadrado, C.; Parra, D.C.; Villalobos Dintrans, P.; Castillo, C.; Cortinez-O’Ryan, A.; Espinoza, P.; Müller, V.; Rivera, C.; et al. Effectiveness of a Gamification Strategy to Prevent Childhood Obesity in Schools: A Cluster Controlled Trial. Obesity 2021, 29, 1825–1834. [Google Scholar] [CrossRef]
- Hrafnkelsson, H.; Magnusson, K.T.; Thorsdottir, I.; Johannsson, E.; Sigurdsson, E.L. Result of School-Based Intervention on Cardiovascular Risk Factors. Scand. J. Prim. Health Care 2014, 32, 149–155. [Google Scholar] [CrossRef]
- Reinehr, T.; Schaefer, A.; Winkel, K.; Finne, E.; Toschke, A.M.; Kolip, P. An Effective Lifestyle Intervention in Overweight Children: Findings from a Randomized Controlled Trial on “Obeldicks Light”. Clin. Nutr. 2010, 29, 331–336. [Google Scholar] [CrossRef]
- Pedrosa, C.; Oliveira, B.M.P.M.; Albuquerque, I.; Simões-Pereira, C.; Vaz-de-Almeida, M.D.; Correia, F. Metabolic Syndrome, Adipokines and Ghrelin in Overweight and Obese Schoolchildren: Results of a 1-Year Lifestyle Intervention Programme. Eur. J. Pediatr. 2011, 170, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for Preventing Obesity in Children. Cochrane Database Syst. Rev. 2019, 7, CD001871. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Sulek, K.; Stinson, S.E.; Holm, L.A.; Kim, M.; Trost, K.; Hooshmand, K.; Lund, M.A.V.; Fonvig, C.E.; Juel, H.B.; et al. Lipid Profiling Identifies Modifiable Signatures of Cardiometabolic Risk in Children and Adolescents with Obesity. Nat. Med. 2025, 31, 294–305. [Google Scholar] [CrossRef]
- Poon, E.T.-C.; Sum, W.M.-K.; Lubans, D.; Wong, S.H.-S.; Ho, R.S.-T. High-Intensity Interval Training for Improving Cardiometabolic Health in Children and Adolescents: An Umbrella Review of Systematic Reviews. J. Sports Sci. 2024, 42, 2199–2215. [Google Scholar] [CrossRef]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-Based Childhood Obesity Prevention Interventions: A Systematic Review and Quantitative Content Analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Obita, G.; Alkhatib, A. Effectiveness of Lifestyle Nutrition and Physical Activity Interventions for Childhood Obesity and Associated Comorbidities among Children from Minority Ethnic Groups: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2524. [Google Scholar] [CrossRef]
- Verma, R.; Bisen, P.S.; Bulló, M. Integrated Review of Cardiometabolic Biomarkers and Dietary Nutrients. J. Food Bioact. 2024, 27, 44–57. [Google Scholar] [CrossRef]
- Spiga, F.; Davies, A.L.; Tomlinson, E.; Moore, T.H.; Dawson, S.; Breheny, K.; Savović, J.; Gao, Y.; Phillips, S.M.; Hillier-Brown, F.; et al. Interventions to Prevent Obesity in Children Aged 5 to 11 Years Old. Cochrane Database Syst. Rev. 2024, 5, CD015328. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.C.; Davies, A.L.; Spiga, F.; Heitmann, B.L.; Jago, R.; Summerbell, C.D.; Higgins, J.P.T.; Inequity in Obesity Prevention Trialists Collaborative Group. Do the Effects of Interventions Aimed at the Prevention of Childhood Obesity Reduce Inequities? A Re-Analysis of Randomized Trial Data from Two Cochrane Reviews. EClinicalMedicine 2025, 81, 103130. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.H.; Mohamoud, I.; Olanisa, O.O.; Parab, P.; Chaudhary, P.; Mukhtar, S.; Moradi, A.; Kodali, A.; Okoye, C.; Arcia Franchini, A.P. Impact of School-Based Interventions on Pediatric Obesity: A Systematic Review. Cureus 2023, 15, e43153. [Google Scholar] [CrossRef]
- Vilchis-Gil, J.; Klünder-Klünder, M.; Flores-Huerta, S. Effect on the Metabolic Biomarkers in Schoolchildren After a Comprehensive Intervention Using Electronic Media and In-Person Sessions to Change Lifestyles: Community Trial. J. Med. Internet Res. 2018, 20, e44. [Google Scholar] [CrossRef]
- Pratapwar, M.P.; Sheth, H.J.; Ravi, A.K.; Block, M.L.; Korber, K.A.; Kepsel, A.; Leimanis-Laurens, M.; Comstock, S.S. Use of Biomarkers in Nutrition Intervention Studies of Children: A Scoping Review. Nutrients 2024, 16, 3584. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Criterion | Inclusion | Exclusion | Search Coherence |
|---|---|---|---|
| (1) Population | Preschool and school-aged children | Children out of preschool or school age Children under medical treatment | “early childhood” OR preschool OR kindergarten OR school* OR “primary education” OR “elementary education” |
| (2) Intervention or Exposure | Children in schools involved in a multifaceted (nutrition and exercise) intervention program (exercise should be in school) | Children out of school doing physical activity program (nutrition intervention could be at home) Children not involved in a multifaceted program Children involved in programs with supplementation (e.g., vitamins) Study protocols | (nutrient* OR nutrition OR food* OR DIET*) AND (exercise OR “Physical activity” OR “physical education” OR sport OR fitness OR aerobic OR movement) AND (program* OR intervention) |
| (3) Comparation | - | - | - |
| (4) Outcome[s] | Outcomes extracted from children`s blood analysis | Outcomes not related to blood | blood |
| (5) Design | Randomized controlled trial | Non randomized controlled trials | “randomized controlled trial*” |
| (6) Other criteria | Peer-reviewed full-text studies published in original journal articles, without language restrictions. | Non-peer reviewed journal articles. Non original full-text studies (conference papers…). |
| Colín-Ramírez et al., 2009 [40] | Xu et al., 2017 [41] | Walter et al., 1989 [42] | Vandonguen et al., 1995 [43] | Rush et al., 2012 [44] | Sauder et al., 2017 [45] | Burke et al., 1998 [46] | Aguilar-Cordero et al., 2020 [47] | Peña et al., 2021 [48] | Hrafnkelsson et al., 2014 [49] | Reinehr et al., 2010 [50] | Pedrosa et al., 2011 [51] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Random allocation | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Concealed allocation | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Baseline comparability | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 |
| Blinding of subjects | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Blinding of therapists | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Blinding of assessors | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Adequate follow-up (>85%) | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 |
| Intention-to-treat analysis | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 |
| Between-group statistical comparisons | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Point estimates and measures of variability for at least one key outcome | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Score | 5 | 7 | 4 | 6 | 5 | 7 | 4 | 5 | 6 | 4 | 6 | 4 |
| Cut-off points | Fair | Good | Fair | Good | Fair | Good | Fair | Fair | Good | Fair | Good | Fair |
| Authors | Sample Characteristics and Dropouts | NutritionalIntervention | Physical ExerciseIntervention | Outcomes | Main Results |
|---|---|---|---|---|---|
| Aguilar-Cordero et al., 2020 [47] | N = 98 (EG: 49; CG: 49) Sex: 52 male, 46 female Age: 10.43 ± 1.35 y BMI: 28.28 ± 3.84 kg/m2 Weight: 65.60 ± 16.07 kg Height: 1.50 ± 0.10 m Country: Spain Pathologies: Overweight/obesity Dropouts: n = 10 (9.2%) IG: 5, CG: 5 | Duration: 9 months EG + CG: Theoretical-practical sessions on nutritional advice twice monthly for children and families. | Duration: 9 months EG: Games-based PA program (90 min, 4 days/week, 9 months, 144 total sessions). Activities: warm-up, main activity (games and sports with largely aerobic component), cool-down. Playful, non-competitive sessions. CG: No physical exercise intervention | Blood pressure SBP (mmHg) DBP (mmHg) SBP percentiles DBP percentiles Hypertension prevalence Body composition Body fat (%) | Intra-group (p < 0.05) EG ↓ SBP (128 ± 9.19 vs. 124.69 ± 5.72 mmHg) ↓ DBP (77.26 ± 7.67 vs. 72.77 ± 4.97 mmHg) ↓ Body fat (41.91 ± 6.24 vs. 38.50 ± 6.62%); ↓ SBP percentiles (95.86 ± 6.50 vs. 79.71 ± 10.77); ↓ DBP percentiles (90.86 ± 7.65 vs. 76.92 ± 11.09) ↓ Hypertension prevalence (85.7% to 16.3%) CG ↑ SBP (129.72 ± 12.78 vs. 131.16 ± 12.24 mmHg) ↑ DBP (77.00 ± 9.62 vs. 78.41 ± 8.70 mmHg) ↑ Body fat (38.64 ± 5.82 vs. 41.25 ± 4.93%) ↑ Hypertension prevalence (77.6% to 81.6%) Inter-group (p < 0.05) EG vs. CG ↓ SBP ↓ DBP ↓ Body fat ↓ SBP percentiles ↓ DBP percentiles ↓ Hypertension prevalence |
| Peña et al., 2021 [48] | N = 2197 (EG: 1544; CG: 653) Sex: 1398 male, 799 female Age: EG: 11.08 ± 0.75; CG: 11.15 ± 0.79 y BMI: EG: 20.3 ± 3.6; CG: 20.7 ± 3.9 kg/m2 Weight: EG: 42.9 ± 10.0; CG: 44.0 ± 11.0 kg Height: EG: 144.8 ± 7.7; CG: 145.3 ± 7.7 cm Country: Chile Pathologies: No. Dropouts: n = 123 (5.3%) IG: 67, CG: 56 | Duration: 7 months. EG: Healthy Snacks Challenge: Points for bringing healthy snacks (NOVA classification-based scoring system), gamification strategy with leaderboards and rewards CG: Standard education provision + access to online platform with educational materials | Duration: 7 months. EG: Multicomponent gamification strategy: Steps Challenge 13,000 steps/day target, Healthy Activity Challenge by family-based activities with photo uploads, Structural rewards (climbing walls, sports infrastructure improvements) CG: Standard curricula | Blood pressure SBP (mmHg) DBP (mmHg) Body composition Zbmi BMI (kg/m2) WC (cm) | Inter-group (7 months, p < 0.05) EG vs. CG ↓ SBP: adjusted mean difference −1.41 mmHg (95% CI: −2.44 to −0.38) ↓ BMI z-score: adjusted mean difference −0.133 (95% CI: −0.25 to −0.01) ↓ BMI: adjusted mean difference −0.42 kg/m2 (95% CI: −0.78 to −0.05) |
| Vandonguen et al., 1995 [43] | N = 869 (F: 150; SN: 148; SN + HN: 119; HN: 161; F + SN: 149; CG: 126) Sex: 423 males, 446 females Age: 10–12 years old BMI: Males: 18.0, Females: 17.8 kg/m2 Weight: NR Height: NR Country: Australia Pathologies: No Dropouts: 193 (15.5%) | Duration: 9 months. EG: School nutrition (SN): 10 × 1-h lessons to improve knowledge, attitudes, and eating habits. Program guide and resources including videos. School + home nutrition (SN + HN): School nutrition + home-based nutrition messages using comics delivered through schools. Educational material for children and parents. Fitness + school nutrition (FIT + SN): Combined fitness and school nutrition interventions. CG Fitness (FIT) Home nutrition only (HN) Control (C): Standard school curricula | Duration: 9 months. EG: Fitness (FIT): 6 × 30-min classroom sessions providing rational basis for activity programs. Physical fitness education with increasing intensity and duration. Fitness + school nutrition (FIT + SN): Combined fitness and nutrition interventions. CG School nutrition (SN) School + home nutrition (SN + HN) Home nutrition only (HN), Control (C): Standard school curricula | Blood pressure SBP (mmHg) DBP (mmHg) Blood lipid Total cholesterol (mmol/L) Dietary intake Total and saturated fat (%) Polyunsaturated fat (%) Monounsaturated fat (%) Protein (%) Fiber intake (g/day) Sodium (g/day) Energy (MJ/day) Sugar (% energy) Anthropometrics BMI (kg/m2) Triceps skinfold (mm) Subscapular skinfold (mm) Body fat (%) Physical fitness Leger score (laps) Run time (min) | Inter-group (p < 0.05) Dietary intake parameters ↓ Total fat (%): boys (FIT + SN) ↓ Saturated fat (%): girls (SN, SN + HN) ↑ Protein intake: boys (FIT + SN, SN, SN + HN) ↑ Fiber intake: Girls in FIT and SN + HN ↓ Sugar intake: Negative correlations in SN, SN + HN and FIT + SN. Sodium intake: ↑ girls (FIT, FIT + SN, SN), ↓ boys (SN) Blood pressure parameters ↓ DBP: Girls in fitness programs (FIT and FIT + SN) Anthropometric parameters ↓ Triceps skinfold: boys and girls (FIT + SN) Blood lipid parameters ↑ Total cholesterol: boys (FIT), girls (all groups). Physical fitness parameters ↑ Leger score: FIT and FIT + SN. ↓ Run time: FIT and FIT + SN. |
| Colín-Ramírez et al., 2009 [40] | N = 498 (EG: 245; CG: 253) Sex: 52.9% male, 47.1% female Age: 8–10 years, mean: 9.5 ± 0.7 years BMI: NR Weight: NR Height: NR Country: Mexico Pathologies: No Dropouts: n = 130 (20.7%) EG: 59; CG: 62 | Duration: 12 months. EG: Nutrition education classes (20–30 min/session) weekly for 10 weeks/year, fun activities, healthy talks for parents, homework assignments, menu suggestions and healthy snacks and lifestyle recommendations CG: Standard school curricula | Duration: 12 months. EG: Physical education classes (30 min/session) twice weekly, moderate to vigorous PA, exercise breaks during classes (2–10 min), benefits of exercise education CG: Standard school curricula | Blood pressure SBP (mmHg) DBP (mmHg) Dietary intake Energy intake (kcal) Fiber (g) Carbohydrates (%) Protein (%) Total fat (%) Saturated fat (%) Monounsaturated fat (%) Polyunsaturated fat (%) Cholesterol (mg) Calcium (mg) Iron (mg) Magnesium (mg) Sodium (mg) Potassium (mg) Vitamin C (mg) Folic acid (μg) Healthy habits Nutrition and health knowledge scores PA attitudes | Intra-group (12 months, p < 0.05) EG ↓ Energy intake (1895 ± 227 vs. 1827 ± 216 kcal) ↓ Fiber intake (6 ± 1 vs. 3 ± 1 g) ↓ Saturated fat (12 ± 2 vs. 11 ± 1%) ↓ Polyunsaturated fat (6 ± 1 vs. 8 ± 1%) ↓ Calcium (957 ± 131 vs. 914 ± 132 mg) ↓ Iron (12 ± 3 vs. 11 ± 2 mg) ↓ Magnesium (145 ± 22 vs. 134 ± 17 mg) ↓ Sodium (1631 ± 371 vs. 847 ± 292 mg) ↓ Potassium (2092 ± 316 vs. 1465 ± 326 mg) ↓ Vitamin C (80 ± 34 vs. 46 ± 42 mg) ↓ Folic acid (113 ± 27 vs. 98 ± 24 μg) ↑ Knowledge attitudes scores (46.2 to 49.7 points) CG ↑ Energy intake (1998 ± 265 vs. 2298 ± 436 kcal) ↓ Fiber intake (6 ± 1 vs. 5 ± 2 g) ↑ Carbohydrates (50 ± 4 vs. 53 ± 5%) ↓ Protein (13 ± 1 vs. 12 ± 2%) ↓ Total fat (37 ± 3 vs. 36 ± 4%) ↓ Cholesterol (258 ± 93 vs. 234 ± 84 mg) ↑ Monounsaturated fat (12 ± 2 vs. 13 ± 2%) ↓ Polyunsaturated fat (6 ± 1 vs. 5 ± 2%) ↑ Calcium (1040 ± 161 vs. 1223 ± 265 mg) ↑ Iron (10 ± 2 vs. 13 ± 4 mg) ↓ Magnesium (131 ± 20 vs. 119 ± 39 mg) ↑ Sodium (1309 ± 440 vs. 1626 ± 544 mg) ↑ Potassium (1891 ± 400 vs. 2297 ± 662 mg) Inter-group (12 months, p < 0.05) Blood pressure parameters ↓ SBP: EG showed greater reduction in SBP to CG (adjusted for baseline obesity prevalence) Cardiovascular risk factors prevalence EG showed significant reduction in overall cardiovascular risk factors prevalence compared to CG, particularly in elevated saturated fat, abdominal fat and, overweight. |
| Rush et al., 2012 [44] | N = 1352 (EG: 692; CG: 660) Sex: 686 boys, 666 girls Age: 5–7 years (926 children) and 10–12 years (426 children) BMI: NR Weight: NR Height: NR Country: New Zealand Pathologies: No Dropouts: 20% 5–7 y, 43% 10–12 y | Duration: 2 years EG: Assigned an “Energizer” (trained nutrition and PA agent). Interventions: canteen makeovers removing pies/cookies, adding healthy options; healthy fundraising; curriculum-based nutrition material; weekly nutrition “nuggets” in newsletters; home-school link program with parent sessions; integrated nutrition lessons. CG: Maintain school activity | Duration: 2 years EG: Assigned an “Energizer” (trained nutrition and PA agent). Interventions: modeling classes for fundamental movement skills, fitness activities, modified games; promotion of active transport, lunchtime games, bike days; student leadership training. CG: Maintain school activity | Anthropometrics BMI (standard deviation score, SDS) % Body fat (SDS) Blood pressure SBP (SDS) DBP (SDS) | Intra-group (p < 0.05) 5–7-year sample EG: ↑ BMI (0.59) ↑ %BF (0.65) ↓ SBP (−0.38) ↑ DBP (0.90) CG: ↑ BMI (0.60) ↑ %BF (0.79) ↓ SBP (−0.41) ↑ DBP (0.87) 10–12-year sample EG: ↑ BMI (0.81) ↑ %BF(1.10) ↑ DBP (1.26) CG: ↑ BMI (0.76) ↑ %BF (1.06) ↑ DBP (1.40) Inter-group (p < 0.05) EG vs. CG 5–7-year age group ↓ %BF: intervention effect −0.14 (95% CI: −0.26, −0.01) 10–12-year age group ↓ SBP: intervention effect −0.23 (95% CI: −0.43, −0.02) |
| Xu et al., 2017 [41] | N = 8573 (EG: 5343, CG: 4574) Sex: 4205 females, 4368 males Age: 9.0 ± 1.4 years BMI: EG: 17.1 ± 3.2, CG: 7.0 ± 3.1 kg/m2 Weight: NR Height: NR Country: China Pathologies: Childhood obesity focus Dropouts: 1294 (13.1%) EG: 633, CG: 661 | Duration: 12 months. EG: Cartoon-style nutrition education handbook distributed to students, 6 nutrition lectures for students (minimum 40 min each), 2 lectures for parents, 4 lectures for teachers and health workers. Contents included healthy eating proportions, beverage and snack choices, reducing fast food consumption. CG: Standard school curricula | Duration: 12 months. EG: “Happy 10” program–classroom-based PA intervention, 10 min of moderate intensity, age- and space-appropriate PA twice daily at school. Activities included games, dance, rhythmic gymnastics. Average energy expenditure: 25.0–35.1 kcal per 10-min session. CG: Standard school curricula | Anthropometrics BMI (kg/m2) Zbmi Body fat (%) WC (cm) Overweight prevalence Blood biomarkers Glucose (mmol/L) Insulin (mU/mL) Total cholesterol (mmol/L) Triglycerides (mmol/L) HDL cholesterol (mmol/L) LDL cholesterol (mmol/L) Physical activity level PA time (minutes/week) Healthy habits Nutrition knowledge, attitudes, and practices scores | Intra-group (p < 0.05) EG ↑ BMI (17.0 ± 3.3 vs. 17.6 ± 3.5 kg/m2) ↓ BMI z-scores (0.23 ± 1.37 vs. 0.12 ± 1.40) ↑ Body fat (26.9 ± 7.1 vs. 28.0 ± 7.0%) ↑ WC (57.9 ± 8.8 vs. 61.0 ± 9.9 cm) ↓ Glucose (4.58 ± 0.54 vs. 4.53 ± 0.43 mmol/L) ↓ Total cholesterol (4.24 ± 0.77 vs. 4.10 ± 0.79 mmol/L) ↑ PA time (815.9 ± 420.6 vs. 855.1 ± 405.6 min/week) CG ↑ BMI (17.1 ± 3.2 vs. 17.9 ± 3.6 kg/m2) ↑ BMI z-scores (0.19 ± 1.30 vs. 0.22 ± 1.39) ↑ Body fat (26.8 ± 7.2 vs. 28.6 ± 6.8%) ↑ WC (57.5 ± 8.9 vs. 61.1 ± 10.1 cm) ↑ Glucose (4.53 ± 0.51 vs. 4.68 ± 0.49 mmol/L) ↑ Total cholesterol (4.00 ± 0.82 vs. 4.18 ± 0.74 mmol/L) ↑ Overweight/obesity prevalence (22.7% vs. 24.2%) Inter-group (p < 0.05) EG vs. CG ↓ BMI: −0.3 kg/m2 (95% CI: −0.4, −0.2) ↓ BMI z-scores: −0.14 (95% CI: −0.18, −0.11) ↓ Body fat: −0.8% (95% CI: −0.9, −0.6) ↓ WC: −0.5 cm (95% CI: −0.6, −0.3) ↓ Glucose: −0.20 mmol/L (95% CI: −0.24, −0.16) ↓ Total cholesterol: −0.32 mmol/L (95% CI: −0.34, −0.30) ↓ HDL cholesterol: −0.09 mmol/L (95% CI: −0.11, −0.07) ↑ PA time: +46.0 min/week |
| Hrafnkelsson et al., 2014 [49] | N = 267 (EG: 128; CG: 139) Sex: NR Age: 7.3 ± 0.3 years BMI: NR Weight: 26.3 ± 4.4 kg Height: 127.0 ± 5.2 cm Country: Iceland (Reykjavik) Pathologies: No Dropouts: 45 (16.8%) EG: 17, CG: 28 | Duration: 2 years EG: General nutrition education focusing on increasing fruit and vegetable intake, with educational material and homework assignments. Food-based dietary guidelines on fish, fish liver oil and milk intake. Parents, teachers, and school food service staff involved in intervention. CG: Standard school curricula | Duration: 2 years EG: Progressive PA program starting with approximately 30 min/day at study start, increasing to approximately 60 min/day in the second year. Teachers integrated PA into daily school routine using various strategies. Extra PE lesson per week introduced in autumn 2007 (discontinued in autumn 2008). CG: Standard PA program at school | Blood pressure SBP (mmHg) DBP (mmHg) Body composition Body fat (%) Weight (kg) BMI (kg/m2) Sum of five skinfolds (mm) Metabolic markers Total cholesterol (mmol/L) HDL-cholesterol (mmol/L) LDL-cholesterol (mmol/L) Triglycerides (mmol/L) Fasting glucose, (mmol/L) HbA1c (%) S-Insulin (mU/L) Physical fitness Fitness (watts/kg) Dietary intake Fruit and vegetable intake Fiber intake | Intra-group (p < 0.05) EG ↑ Fruit and vegetable intake (+47%) ↑ Fiber intake (+17%) CG ↓ Fruit and vegetable intake (−27%) Inter-group (p < 0.05) EG vs. CG Not observed |
| Reinehr et al., 2010 [50] | N = 66 (EG: 34; CG: 32) Sex: 28 male, 38 female Age: 11.5 ± 1.6 years BMI: 23.4 ± 1.5 kg/m2 Weight: NR Height: NR Country: Germany Pathologies: Overweight (BMI >90th to <97th percentile) Dropouts: 6 (9%) EG: 1; CG: 5 | Duration: 6 months EG: Nutritional course based on “Optimized mixed diet” with traffic-light system for food selection (30% fat, 15% protein, 55% carbohydrates including 5% sugar vs. typical German diet of 38% fat, 13% protein, 49% carbohydrates including 14% sugar). Six group sessions (1.5 h each) in intensive phase plus individual nutrition counseling sessions. CG: No intervention | Duration: 6 months IG: PA training once weekly (1.5 h per session) including ball games, jogging, trampoline jumping, dancing for girls, wrestling for boys, and instructions for daily life PA and reducing TV/computer time. CG: No intervention | Blood pressure SBP (mmHg) DBP (mmHg) Body composition BMI-(SDS) BMI (kg/m2) WC (cm) Triceps and Subscapular skinfold (cm) Fat mass (%) Lean body mass (kg) Dietary intake Energy intake (kcal/day) Fat (E%) Protein (E%) Carbohydrate (E%) Sugar (E%) Healthy habits Sports activity (survey) TV consumption (h/week) Computer use (h/week) | Intra-group (p < 0.05) EG ↓ BMI-SDS (−0.26 ± 0.22) ↓ BMI (−0.85 ± 1.02 kg/m2) ↓ WC (−6 ± 8 cm) ↓ Triceps skinfold (−5 ± 7 cm) ↓ Subscapular skinfold (−4 ± 8 cm) ↓ Fat mass (−6 ± 8% skinfold; −2.7 ± 4.9% bioimpedance) ↑ Lean body mass (+6.0 ± 9.9 kg) ↓ SBP (−7 ± 4 mmHg) ↓ DBP (−6 ± 4 mmHg) ↓ Energy intake (1651 ± 433 vs. 1372 ± 341 kcal/day) ↓ Fat intake (35 ± 6 vs. 32 ± 5 E%) ↑ Protein intake (14 ± 2 vs. 16 ± 3 E%) ↓ Sugar intake (13 ± 5 vs. 9 ± 4 E%) ↑ Sports activity (2.6 ± 0.9 vs. 2.9 ± 0.9) CG ↑ BMI (+0.76 ± 0.99 kg/m2) Inter-group (p < 0.05) EG vs. CG ↓ BMI-SDS: −0.31 (CG: +0.05 ± 0.19; EG: −0.26 ± 0.22) ↓ BMI: −1.61 kg/m2 (CG: +0.76 ± 0.99; EG: −0.85 ± 1.02) ↓ WC: −6.0 cm (CG: 0.0 ± 1; EG: −6 ± 8) ↓ Triceps skinfold: −7.0 cm (CG: +2 ± 6; EG: −5 ± 7) ↓ Subscapular skinfold: −7.0 cm (CG: +3 ± 8; EG: −4 ± 8) ↓ Fat mass (skinfold): −8.6% (CG: +2.6 ± 7.8; EG: −6 ± 8) ↓ Fat mass (bioimpedance): −2.9 kg (CG: +0.2 ± 2.6; EG: −2.7 ± 4.6) ↓ SBP: −6.0 mmHg (CG: −1 ± 5; EG: −7 ± 4) ↓ DBP: −4.0 mmHg (CG: −2 ± 7; EG: −6 ± 4) |
| Sauder et al., 2017 [45] | N = 62 (EG: 29; CG: 33) Sex: 32 male, 30 female Age: EG: 9.3 ± 1.0, CG: 9.1 ± 1.1 years BMI: EG: 26.4 ± 4.7, CG: 26.1 ± 4.5 kg/m2 Weight: NR Height: NR Country: United States Pathologies: Overweight/obese American Indian children (BMI ≥85th percentile) Dropouts: n = 2 | Duration: 8 months (4 months intensive + 4 months maintenance) EG: Tribal Turning Point program with “5−2-1-0” messaging (≥5 servings fruits/vegetables, ≤2 h screen time, ≥1 h PA, 0 sugary beverages daily). Traffic Light Diet system for food selection. 10 group classes (2 h each) over 4 months + 2 booster classes in spring. Individual motivational interviewing sessions and resource toolbox. CG: Three 1-h health and safety group sessions (bullying, drug/alcohol prevention, first aid, fire safety, bike safety) with healthy group meals. | Duration: 8 months EG: PA component integrated into group classes (10–20 min per session). Optional 60-min “Kids Work-Out” before each session with games and activities. PA education and goal-setting. CG: No structured PA intervention. | Blood pressure SBP (mmHg) DBP (mmHg) Body composition BMI (kg/m2) Zbmi WC (cm) Metabolic markers Fasting insulin (uU/mL) Fasting glucose (mg/dL) HbA1c (%) HOMA-IR Healthy habits PACER fitness test (laps) MVPA (30-min blocks) Screen time (30-min blocks) PA self-efficacy Dietary self-efficacy | Intra-group (p < 0.05) IG ↓ BMI z-score (−0.17) ↑ PACER laps (+1.8) ↑ MVPA (+4.2) ↑ PA self-efficacy (+0.6) CG: ↑ BMI (+1.0) ↑ WC (+3.7) ↑ PACER laps (+1.9) ↑ MVPA (+6.1) Inter-group (p < 0.05) EG vs. CG ↓ BMI z-score: −0.18 (IG: −0.17 vs. CG: +0.01) ↓ WC: −2.5 cm (IG: +1.2 vs. CG: +3.7 cm) |
| Burke et al., 1998 [46] | N = 800 (Distribution by groups: NR) Sex: 409 male, 391 female Age: 11 years old BMI: 16.8 kg/m2 (lower risk boys), 21.1 kg/m2 (higher risk boys), 17.5 kg/m2 (lower risk girls), 19.2 kg/m2 (higher risk girls) Weight: NR Height: NR Country: Australia Pathologies: 29% identified as higher cardiovascular risk Dropouts: 80 | Duration: 2 school terms (20 weeks) EG: Updated WASPAN nutrition program including comic books featuring space creatures learning human dietary habits, teachers’ handbook, home-based mission booklet, class activities, incentives, and recipe booklet. Focus on reducing fat, sugar, and salt intake while increasing fiber intake. 1 h per week nutrition classes. CG: Standard school curriculum only | Duration: 2 school terms (20 weeks) EG: Six classroom lessons plus innovative 20-min fitness sessions daily (4 sessions/week) using small group activities allowing for individual fitness levels. 37% sessions lasted 15 min, 55% lasted 20 min, 8% lasted 25 min. CG: Standard school curriculum only | Blood pressure SBP (mmHg) DBP (mmHg) Body composition BMI (kg/m2) Weight-for-height-for-age (WHA) Subscapular skinfold (mm) Triceps skinfold (mm) Body fat (%) Metabolic markers Total cholesterol (mmol/L) Physical fitness Leger shuttle run (laps) 1.6 km run time (min) Healthy habits Leisure-time PA (h/week) Television watch (h/week) Intake (sodium, fat, fiber) | Intra-group (p < 0.05) All program groups ↑ Physical fitness in both boys and girls at WASPAN and enrichment schools ↑ BMI and WHA in boys at WASPAN schools only Higher risk boys in enrichment schools Greatest improvement in fitness ↓ Time for 1.6 km run Inter-group (p < 0.05) EG vs. CG ↑ Shuttle run laps: Greatest improvement in higher risk boys in enrichment schools vs. other groups ↑ Fitness improvements in girls from program schools vs. controls ↓ Subscapular skinfolds: Girls in enrichment schools vs. other groups ↓ Triceps skinfolds: Enrichment vs. control groups ↓ Cholesterol: Higher risk girls and boys in enrichment schools ↓ Sodium intake: Both boys and girls in enrichment schools ↓ TV watching: Boys in enrichment schools |
| Walter et al., 1989 [42] | N = 3388 (EG: 2075, CG: 1313) Sex: 1725 males, 1663 females Age: 8.9–9.1 years BMI: NR Weight: NR Height: NR Country: United States Pathologies: No Dropouts: Westchester: 911 (82.4%) participated at baseline, 593 (65.1%) eligible for 6-year analysis. Bronx: 1563 (68.5%) participated at baseline, 1036 (66.3%) qualified for 5-year analysis. | Duration: 5–6 years EG: “Know Your Body” (KYB) curriculum focusing on “prudent diet” with daily total fat <30% calories, saturated fat <10% calories, total carbohydrate >55% calories, cholesterol <300 mg, sodium <2 g, decreased refined sugar, increased complex carbohydrates and fiber, maintain ideal body weight. Approximately 2 h per week throughout each school year. Parent education component included newsletters, curriculum activities, and evening seminars. CG: Standard school curriculum only | Duration: 5–6 years EG: Physical fitness component promoting regular endurance exercise program to supplement skill/strength exercises. Integrated into KYB curriculum (~2 h per week). CG: Standard school curriculum only. | Blood pressure SBP (mmHg) DBP (mmHg) Body composition Ponderosity index (kg/m) Triceps skinfold (mm) Metabolic markers Total cholesterol (mg/dL) HDL cholesterol (mg/dL) Physical fitness Recovery index (score) Healthy habits 24-h dietary recall (total fat %, saturated and polyunsaturated fat %, carbohydrate %, cholesterol and sodium in mg) Knowledge test scores (prevention-related) Cigarette smoking initiation (biochemically verified) | Intra-group (p < 0.05) Westchester EG ↓ Total cholesterol (−8.5 mg/dL or 5.1% net decline) ↓ Total fat intake (−3.6%) ↑ Total carbohydrate intake (+4.5%) ↑ Knowledge test scores (+22.6% net increase) Bronx EG ↓ Total cholesterol (−5.0 mg/dL or 2.9% net decline) ↓ Saturated fat intake (−2.1%) ↑ Knowledge test scores (+18.8% net increase) Inter-group (p < 0.05) EG vs. CG Westchester ↓ Total cholesterol: −1.7 mg/dL per year (95% CI: −2.7 to −0.7) ↓ Total fat intake: −3.6% (95% CI: −7.1 to −0.1) ↑ Carbohydrate intake: +4.5% (95% CI: +0.1 to +8.9) ↑ Knowledge scores: +0.14 per year (95% CI: +0.06 to +0.22) ↓ Cigarette smoking initiation: 73.3% reduction (3.5% in intervention vs. 13.1% in control schools) Bronx ↓ Total cholesterol: −1.0 mg/dL per year (95% CI: −2.3 to +0.3) ↓ Saturated fat intake: −2.1% (95% CI: −4.7 to +0.5) ↑ Knowledge scores: +0.12 per year (95% CI: +0.03 to +0.21) |
| Pedrosa et al., 2011 [51] | N= 61 (EG: 42, CG: 19) Sex: 27 male, 34 female Age: 8.4–9.3 years BMI: 22.4–22.6 kg/m2 Weight: 40.9–44.2 kg Height: 134.1–137.5 cm Country: Portugal Pathologies: Overweight/obese children (≥85th BMI percentile), 51 obese (≥95th percentile), 10 overweight (85–95th percentile) Dropouts: n = 22, EG: 16, CG: 6. | Duration: 1 year EG: Individual healthy eating plan (~1800 kcal) prescribed and explained to children and parents. Nutritional counseling at follow-up visits (3, 6, and 12 months). CG: Four group-based nutrition education sessions (60 min each) distributed over first semester, conducted by nutritionist. Children and parents participated together. Sessions covered childhood obesity, healthy eating habits, cooking methods, portion control, food labeling. | Duration: 1 year EG: PA was encouraged and sedentary behaviors (TV watching, computer/video games) were discouraged. No structured exercise program described. CG: No intervention. | Blood pressure SBP (mmHg) DBP (mmHg) Body composition Zbmi WC (cm) WC/height ratio Metabolic markers Fasting glucose (mmol/L) Insulin (pmol/L) HOMA-IR HDL cholesterol (mmol/L) Triglycerides (mmol/L) Apolipoprotein A-I and B (g/L) Adipokines and hormones Leptin (ng/mL) Adiponectin (μg/mL) Ghrelin (pg/mL) C-reactive protein (mg/L) Homocysteine (μmol/L) MS prevalence Using modified NCEP ATP III criteria | Intra-group (p < 0.05) EG + CG (time effect) ↓ Zbmi: Significant decrease over time ↓ WC/height ratio: Significant decrease over time ↓ DBP: Improvement over time ↑ HDL cholesterol: Increase over time ↓ Triglycerides: Decrease over time ↑ Ghrelin: Increase over time Inter-group (p < 0.05) EG vs. CG ↓ BMI z-score: Greater decrease in CG vs. EG (p = 0.042) ↓ WC/height ratio: Greater improvement in CG vs. EG (p = 0.042) ↑ HDL: Greater increase in CG vs. EG (p = 0.042) ↑ Ghrelin: Different behavior between groups–increased in CG while decreased in EG (p = 0.039) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rico-González, M.; González-Devesa, D.; Gómez-Carmona, C.D.; Moreno-Villanueva, A. The Effects of Nutritional Education and School-Based Exercise Intervention Programs on Preschool and Primary School Children’s Cardiometabolic Biomarkers: A Systematic Review of Randomized Controlled Trials. Appl. Sci. 2025, 15, 8564. https://doi.org/10.3390/app15158564
Rico-González M, González-Devesa D, Gómez-Carmona CD, Moreno-Villanueva A. The Effects of Nutritional Education and School-Based Exercise Intervention Programs on Preschool and Primary School Children’s Cardiometabolic Biomarkers: A Systematic Review of Randomized Controlled Trials. Applied Sciences. 2025; 15(15):8564. https://doi.org/10.3390/app15158564
Chicago/Turabian StyleRico-González, Markel, Daniel González-Devesa, Carlos D. Gómez-Carmona, and Adrián Moreno-Villanueva. 2025. "The Effects of Nutritional Education and School-Based Exercise Intervention Programs on Preschool and Primary School Children’s Cardiometabolic Biomarkers: A Systematic Review of Randomized Controlled Trials" Applied Sciences 15, no. 15: 8564. https://doi.org/10.3390/app15158564
APA StyleRico-González, M., González-Devesa, D., Gómez-Carmona, C. D., & Moreno-Villanueva, A. (2025). The Effects of Nutritional Education and School-Based Exercise Intervention Programs on Preschool and Primary School Children’s Cardiometabolic Biomarkers: A Systematic Review of Randomized Controlled Trials. Applied Sciences, 15(15), 8564. https://doi.org/10.3390/app15158564