1. Introduction
Sport-related injuries are prevalent across all levels of sports, from recreational to professional sports [
1]. These injuries carry a considerable public health burden, often leading to decreased participation in sports activities, possible long-term health consequences, and an increased strain on healthcare systems. At professional levels of sports, once a potential injury is observed and the athlete is removed from activity, medical personnel typically administer the appropriate assessments to confirm the presence of injury and the severity of the specific injury [
2].
At the sub-elite levels of sport, injury reporting can be less structured and is often carried out by individuals without formal training, such as coaches, parents, spectators, or the athletes themselves [
3]. In many of these settings, traditional injury identification methods, such as athlete self-reporting [
4,
5], or observer-based assessments [
6], are prone to human error, underreporting [
5], and subjective interpretation. Such limitations can delay injury management, or formal diagnosis and appropriate interventions, particularly in field-based settings. The dynamic nature of sports further complicates timely and accurate detection using conventional methods, especially when medical professionals may not be immediately available at sub-elite levels of sport [
7].
One of the many issues with the self-reporting of injury is the lack of education regarding the identification and severity of certain injuries, for example, sport-related concussion (SRC). In a study involving collegiate athletes who had experienced an SRC, less than 50% reported the injury, with 65% not reporting their injury, believing the injury was not serious enough to warrant medical attention [
5].
As injury management modalities advance, emerging technologies are being developed which offer greater accuracy and accessibility in injury detection. These technologies are increasingly capable of identifying and detecting injury events as they occur, even in field-based settings. There is a burgeoning interest in objective tools which aim to detect injuries and reduce human error. Although sports injuries are inherently unpredictable [
8], the development of tools to aid in detection and identification may be useful.
These tools aim to overcome the limitations of traditional detection approaches by providing objective, accessible data that can assist practitioners in making timely decisions.
The existing reviews focus on injury prevention, rehabilitation, or predictive models, rather than the real-time identification of injury events. This systematic review aims to identify and evaluate peer-reviewed studies published in the last decade which utilise emerging technologies for the detection of sport-related injuries in field or competition environments. By assessing their methodologies, implementation contexts, and practical utility, this review seeks to inform the development, validation, and broader application of injury detection tools at all levels of sport [
9,
10,
11]. This paper provides a novel contribution by critically assessing current tools used for the direct detection of sport-related injuries within their real-world contexts, rather than focusing on retrospective analyses or predictive models. This approach aims to inform both current discourse and the direction of future research.
2. Materials and Methods
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [
12]. The review was registered on the International Prospective Register of Systematic Reviews (PROSPERO) before beginning the literature search on 16 November 2024 (Ref No. CRD42024608964).
Search Strategy
Preliminary searches were conducted in November 2024 using EndNote (V21.5, Philadelphia, USA) on five databases (Sport Discus, ScienceDirect, Web of Science, PubMed, and Google Scholar). This initial process aided in identifying key search terms used in later stages. The search process was conducted over four stages: (1) Initial preliminary search terms with synonyms and timeline. (2) Agreement and refinement of search term protocol in an attempt to improve results. (3) Final search terms, databases, and timeline agreed by LCD, ED, LR, and MM (November 2024). (4) Recorded database search on the agreed databases. The search terms consisted of: Technology AND Sport injury AND Detection OR Identification, from 2014 until the end of 2024, see
Table 1 for sample search terms.
Inclusion and Exclusion Criteria
Papers were included in the review if they: (1) were written in English, (2) were conducted on humans of any age, (3) involved an injury in a sport context, or (4) involved an injury identified over the course of the study using the method described.
Papers were excluded from this review if they: (1) were not written in English, (2) were not conducted on humans, (3) did not involve an injury during sport participation, (4) retrospectively analysed data to restructure and produce more positive outcomes, (5) did not directly detect injury, but identified risk, load, fatigue, or impact, (6) comprised a review (literature or systematic), or (7) involved a study conducted before 2014.
Studies identifying risk factors, conducted prospectively with the intention of identifying risk factors, meaning that the studies were designed with preliminary screening using existing tools, with surveillance, and confirmatory analysis to identify risk factors, were also excluded. Predictive models were excluded as they did not involve direct, real-time detection or confirmatory surveillance of injuries; instead, they estimated risk based on proxy measures (e.g., load, fatigue, impact) without verified injury outcomes, which did not align with the review’s focus on confirmed injury detection tools Studies conducted before 2014 were excluded to focus on the rapid development of emerging technologies in the past decade.
Study Selection
The study selection process was completed by the research team over three phases. After the initial search protocols were agreed upon, in phase one, LCD screened titles and abstracts. From the initially included papers, a random, numerically selected sample of papers (n = 20) was sent to the research team (LR, ED, MM) for review and quality control protocols. No disagreements were found on the search protocol, and adherence to the set criteria was met.
In phase two, LCD screened the full texts of included articles for the inclusion and exclusion criteria. Upon agreement from the team, a decision was made to further refine the criteria of inclusion to remove papers which were retrospective in design and those that did not directly measure injury detection as an outcome, such as protocols which measured athlete load, fatigue, or impact. This decision was made after careful review of initially included studies, where it was found that numerous studies used the term “injury” and did not directly address which muscle injury they were focusing on, such as algorithmic or predictive studies.
To maintain relevance and clarity in scope, the inclusion criteria were refined to focus solely on studies with direct injury detection as a primary outcome. In phase three, papers were separated and codified using EndNote. The codified papers were independently sent to the research team, which included or excluded papers. The research team had no disagreements on the included or excluded papers.
2.1. Extraction
The extraction process was completed by LCD using a tool developed in Excel; this can be found in the
Supplementary Files Section. The tool comprised standard sections including title, DOI, author, year of publication, sample size, population, results, and summary. The sections based on prior research comprised sport level (i.e., youth, university/intervarsity, elite, other), type of sport, duration of surveillance, and method of assessment in the study. The section specific to this review comprised research gaps exposed (stated in the paper or found by design of study), future research (stated in the paper or found by design of study), and rationale of the CASP scoring. No subgroup analysis was performed.
2.2. Risk of Bias Assessment
The CASP checklist tools for cohort studies [
12] and cross-sectional studies [
13] were used to assess the quality of the studies included in the full text review. The papers were assessed by LCD. The studies were assessed based on subjective qualities that are cross-compared. Scoring is dependent on which tool is used, based on the study design (cohort, case–control, or cross-sectional). Each individual tool has subsections specific to the type of study, but overall scoring is out of 11 points. There are prompts for the reviewer to score “Yes” (1 point), “No” (0 point), or “Unclear/NA” (0.5 point). A general score is then given based on the study’s individual criteria checklist. From the included papers in this review, 12 studies were of “Good” standard (scoring 8–9/11), and the remaining 9 studies were “Excellent” (scoring 10+).
3. Results
3.1. Result Extraction Process
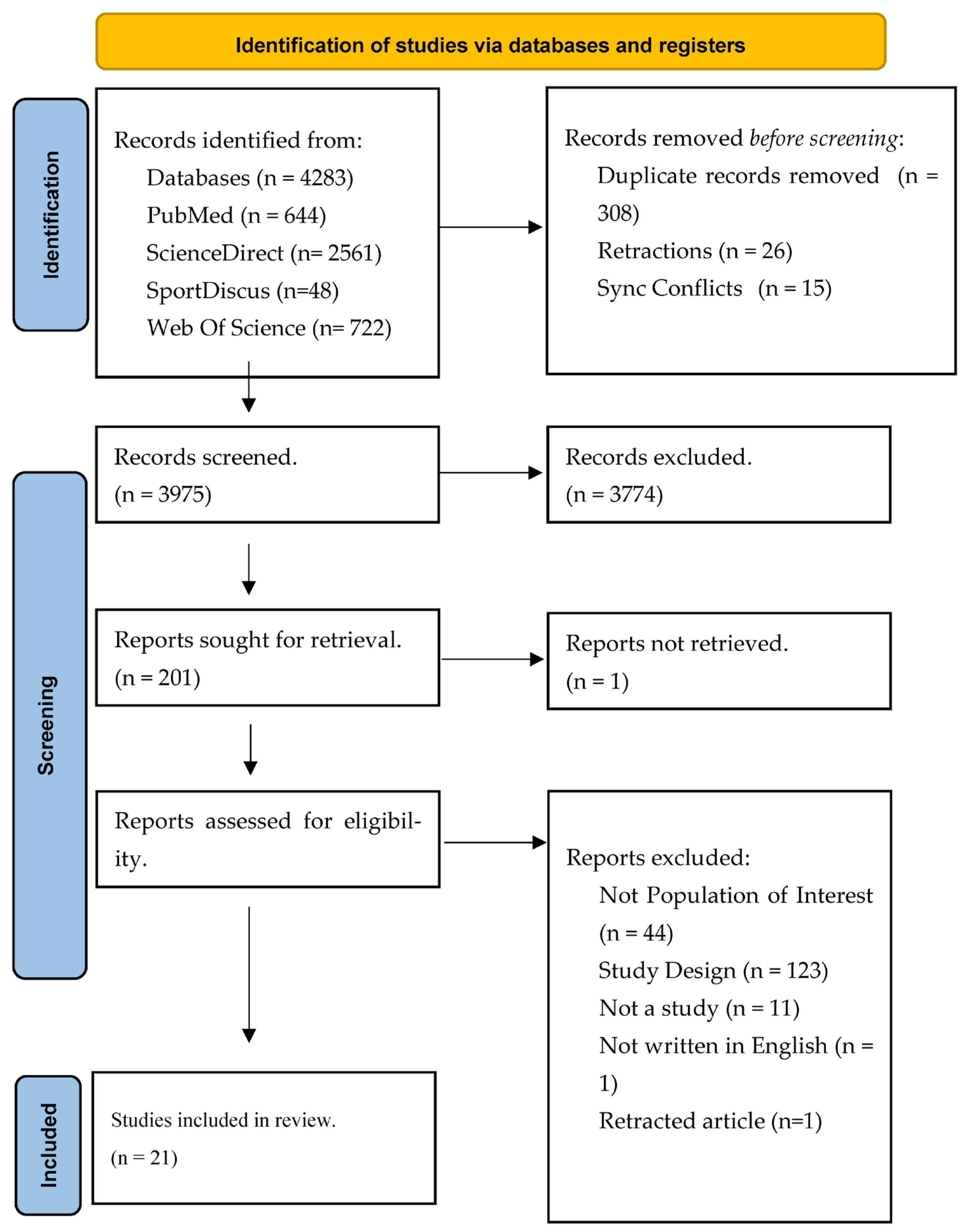
The database search resulted in 4283 papers initially being included, with 510 duplicates and retracted papers removed automatically by EndNote (Clarivate, PA, USA). The PRISMA diagram can be seen in
Figure 1. The 21 studies involved 1973 participants (95.14% male, n = 1877; 4.86% female, n = 96), with sample sizes ranging from 17 to 515. There was a considerable loss of participants in the included studies, with 468 participants removing themselves from the studies for various reasons, reducing the total to 1505 (23.72% loss). Seventeen studies focused on sport-related concussion (SRC) and/or mild traumatic brain injury (mTBI), two on persistent post-concussive symptoms (PPCS), and one study on both hamstring strain injuries (HIS) and osteochondritis dissecans (OCD).
Section 3.3,
Section 3.4,
Section 3.5,
Section 3.6 and
Section 3.7 synthesise the findings of the included studies based on the methodology of injury detection. In our review, seven studies used field-based testing, six studies used biomarkers, three studies used sensor-based wearables, and five studies used advanced imaging techniques for identifying sports injuries. Below, in
Figure 1, we have included a PRISMA flow diagram to illustrate the exclusion process for papers.
3.2. Study Characteristics
Table 2 provides a breakdown of the key characteristics of the extracted data from the studies that met the final inclusion criteria. Key metrics were sample size, duration of intervention, sport context, injury in focus, and intervention method. Abbreviations for the injuries under focus can be found in the table at the end of this paper.
3.3. Field-Based Identification
Field-based tests, primarily targeting SRC, provide accessible sideline tools for rapid injury detection. Seven studies [
8,
17,
18,
20,
22,
24,
26,
27,
28] evaluated tools such as the King–Devick Test (KD-T), Immediate Post-concussion Assessment and Cognitive Testing (ImPACT), and Display Enhanced Testing for Cognitive Impairment and mTBI (DETECT) in rugby, American football, ice hockey, soccer, and cheerleading. The KD-T demonstrated high reliability (ICC: 0.79–0.97), identifying 52 SRC cases over three years in rugby (incidence: 44 per 1000 match hours, 95% CI: 32–56) and seven unrecognised concussions in juniors [
22,
27,
28]. ImPACT detected significant cognitive declines over a season (
p < 0.05), with correlations between rotational velocity (>80 g) and performance decline (R = 0.69,
p = 0.028) [
18,
24]. DETECT showed strong sensitivity (86.7%, 95% CI: 59.5–98.3%, AUC: 0.778,
p = 0.02) for SRC [
20]. Video analysis (VA) had good inter-rater reliability for motor incoordination (81% positive predictive value) but lower specificity [
26] in identifying concussive symptoms in Australian Football League (AFL) players. KD-T and DETECT outperformed VA and KD-Eye Tracking, which showed limited sensitivity [
17], highlighting varied diagnostic precision. Applied during games or immediately post-event, these tools support rapid assessment but require further development for enhanced integration with ET and adoption by teams and organisations.
3.4. Biomarker-Based Solutions
Biomarkers offer consistent diagnostic accuracy for SRC and PPCS by detecting neurological changes and stress. Six studies [
11,
14,
16,
19,
21,
23,
25] investigated NfL, GFAP, Cerebrospinal Fluid (CSF), and salivary markers in boxing, rugby, and diving. NfL levels rose significantly post-SRC (
p < 0.0001), correlating with impact severity and distinguishing rapid versus prolonged symptoms [
21,
25]. GFAP peaked within one hour post-injury (
p = 0.017), normalising by 10 days, unlike non-mTBI controls (
p > 0.999) [
21]. CSF markers, including IL-2 and TNFα, were elevated in athletes with PPCS (
p < 0.05), indicating an ongoing inflammatory process [
11,
14]. Salivary microRNAs (e.g., miR-27b-3p) showed upregulation post-SRC (
p = 0.016) [
23]. NfL and GFAP provided superior sensitivity compared to salivary markers, but all required laboratory analysis, severely limiting their sideline use. Conducted post-injury by clinicians, these biomarkers excel in controlled diagnostics and could complement sensors’ real-time potential following an integration of the two methodologies.
3.5. Sensor-Based Solutions
Sensor-based technologies enable real-time injury event monitoring in sports settings. Three studies [
13,
15,
20] assessed iMGs and Head Impact Telemetry (HIT) in rugby and American football. iMGs with machine learning achieved high accuracy (CatBoost AUROC: 0.900) in classifying head impacts [
13], surpassing HIT, which showed weaker correlations (Spearman’s r = 0.254–0.262,
p = 0.02–0.03) [
20]. Helmet-based HIT detected impacts but lacked robust validation [
15]. When worn during games, iMGs offer practical field data, though further standardisation for comparability between devices is needed. These real-time solutions are more aligned with the sports industry’s need for real-time injury detection. With the correct supervision and further development, these technologies may deliver insights for real-time, sport injury detection.
3.6. Advanced Imaging-Based Solutions
Advanced imaging reveals microstructural changes in SRC, PPCS, HSI, and OCD. Five studies [
9,
10,
11,
12,
15] used 7T Diffusion Kurtosis Imaging (DKI), Quantitative Susceptibility Mapping (QSM), Resting-State Functional MRI (Rs-fMRI), and ultrasound in ice hockey, baseball, and Australian football. The 7T DKI detected PPCS white matter abnormalities correlating with CSF markers (
p < 0.05) [
11], outperforming 3T MRI, which showed increased frontoparietal connectivity (
p = 0.016) [
15] but was limited without cross-comparability of CSF biomarkers. QSM/Rs-fMRI identified mTBI signal changes (days 3–7 post SRC) [
9]. Ultrasound-supported HSI predictive algorithms and OCD screening with high sensitivity [
10,
12] imaging require clinical settings, limiting field applicability. This level of diagnostic insight informs the broader synthesis of technological applications but is limited in its area of impact.
3.7. Synthesis of Findings
Emerging technologies demonstrate potential for sports injury detection, with field-based tools offering sideline practicality, biomarkers providing high precision, sensors enabling real-time monitoring, and imaging delivering detailed diagnostics.
4. Discussion
This systematic review aimed to identify and evaluate emerging technologies for injury detection in active sports settings. The review highlighted twenty-one studies in this context, which identified an array of field-applicable tools and tests. With heterogeneity in results, it is difficult to compare and suggest the most appropriate tool(s) to be utilised across various sporting contexts.
Biomarker-based solutions, NfL, GFAP, CSF markers, and salivary microRNAs, showed high diagnostic accuracy for SRC and PPCS by detecting specific neurological changes [
11,
14,
16,
19,
21,
23,
25]. NfL and GFAP demonstrated greater sensitivity and correlation with injury severity. While these markers offer precise insights into subclinical injuries, their requirement for laboratory analysis leads to a delay in diagnosis delivery, which significantly limits their applicability to sideline utilisation, where point-of-care diagnosis is often needed. Relying on medical professionals with specialised equipment and their accompanying sophisticated results interpretation often deters a more widespread adoption of these tools [
35,
36]. The limited frequent use of biomarkers for direct injury detection in sports settings stems from several key challenges.
A lack of specificity in results, as found with creatine kinase or other inflammatory cytokines, can be elevated due to normal exercise-induced muscle damage or general physiological stress, rather than a specific injury occurrence, making it difficult to differentiate between physiological adaptation and a muscular injury [
29,
30]. The inter-individual variability in biomarker levels, specifically in athletes, who all have unique confounding variables such as nutrition, hydration, and training status, complicates the “norm” ranges, as highlighted in Shahim’s study using inflammatory biomarker S100B [
25,
29]. The current body of literature necessitates a universally accepted range of athlete-specific biomarkers. The practicality of such an approach poses significant logistical and resource challenges for many sports organisations [
35,
36,
37].
Sensor-based technologies such as iMGs and HIT systems offer promising avenues for real-time injury event monitoring in contact sports [
13,
15,
20]. However, further standardisation is required to ensure unbiased comparability and widespread adoption.
Advanced imaging techniques, including 7T DKI, QSM, Rs-fMRI, and ultrasound, provided detailed insights into microstructural changes associated with SRC, PPCS, HIS, and OCD [
9,
10,
11,
12,
15]. These methods are limited in field applicability, similar to biomarkers, requiring clinical settings with trained professionals. Recent studies have investigated field-based ultrasound tools for the assessment of HSI [
38], which could be a middle ground between field-based applications and medical-level insights, but further investigation is required.
The current review highlighted a considerable reduction in the number of participants (23.72%) who were retained for the duration of the included studies, which may limit the generalisability and reliability of findings. Additionally, gender imbalance was highly prevalent (95.14% male, 4.86% female *reported) and may affect implications for practitioners who work in female sports. Female athletes have different physiologies, different prevalences of injuries, for example, with HSI and knee ligament injuries [
39]. This lack of developed female athlete research, specifically injury surveillance, was highlighted by a recent systematic review by Beech [
40] in 2024. A recent review clarified [
41] that female athlete injury pathophysiology and biomechanical properties have a different make-up and thus require specific academic research. The underrepresentation of female athletes in these studies is notable and warrants further investigation, which may further help develop robust methodologies such as AI, giving broader scope to injury mechanisms and broader datasets. The need for larger samples, standardised protocols, and tool validation was frequently identified, particularly for sensors and predictive models.
4.1. Key Findings
These findings highlight opportunities in research for developing integrated, accessible tools to enhance injury detection across sports. CSF and the KD test were two of the most studied identifiers of SRC. Where accessible, this review highlights that these tools should be first used in the identification of SRC in practice. For sports bodies with limited access to expensive tools such as CSF biomarker testing, field-based testing such as KD is highly applicable. Sensor-based solutions appear to offer promising developments in the ET space, being applicable to both practitioners and researchers with adequate development; iMGs are a strong candidate for the identification of SRC and head impact load in contact sports, but further research is needed before a full recommendation can be made. Female-specific research is further warranted in the domain of sport injury, specifically in AI, with computer vision models being under-explored, and lacking depth in research in female-based models being developed.
4.2. Limitations
There were limitations associated with the study, notably, the heterogeneity amongst findings and methodologies between studies, making them unfeasible for meta-analysis. This review is limited to emerging technologies that are currently being used—or have already been tested in a sporting context—in a sporting population. This excludes studies that have predictive models, tools and methods to identify injuries that may potentially impact the industry. The search criteria used in the process of this review were narrow and may have limited what areas could be explored in the review, namely with the methodology of reviews, and the search criteria have a potential language exclusion bias, concentrating on English language-only studies. This process has highlighted that various studies initially included may have the potential to identify injuries or sicknesses in sports settings. However, the study design meant they were excluded for numerous reasons, such as retrospective design, improper validation of devices/tools, or the participant cohort. The findings are limited in generalizability to female athletes, as under 5% of participants included across the studies were female.
4.3. Implications
This review has direct practical implications for sports bodies, clubs, and organisations as a guide for what current tools, techniques and emerging technologies may be used in a sports setting to identify injuries accurately and reliably. The review also highlighted the level at which a tool may be more accessible. Although there were noticeably low numbers of female participants in the studies included, it must be clarified that these tools and methods were not reported as gender-specific in these studies. Following the evidence-informed approaches for the implementation of tools included in this review, it must be known that both sexes can benefit from these tools. For researchers, it is evident that there is a lack of high-quality research with ET in the domain that is developed enough to be applicable and designed for the end user—sports bodies, organisations, and athletes at any level.
4.4. Future Directions for Innovation
Future research should address the most prominent predictive and risk-identifying tools for possible future investigations to address context-specific, relevant research questions. A tool could be developed to assist in this process and ensure that future studies may adhere to a homogeneous protocol.
No study in our review assisted sports officials, such as referees, during a game in identifying a possible injury event. Further investigation into these “unnoticed” injuries is needed. There are video surveillance systems for supporting officials in sports; by extension, these may be utilised for injury detection. It has been previously noted by [
42] that video surveillance is time-consuming, delayed, and not perfectly accurate; however, an automated video surveillance system, which tags possible injury events, quantifies impact load, and can observe joint angles, may prove useful.
Existing models, such as graphical neural networks (GNN), may be an avenue for exploration. GNNs are a form of AI used in the creation of relationships between graphical inputs, for example, photos of games, streamed from live video, captured frame by frame. These methods may be able to model biomechanical systems, providing real-time injury detection.
5. Conclusions
This systematic review highlights the potential of ET, including biomarkers, wearable sensors, and sideline assessments, for real-time sports injury detection. Biomarkers like NfL and GFAP excel in detecting subclinical injuries, while iMGs and HIT sensors offer practical field applications for identifying head impact loads during sport. The KD test for sideline concussion assessment has excellent reliability and accuracy, with extensive testing across gender, age, and sports disciplines. For practitioners, this review highlights the use of field-based testing, such as the KD test, and field-based sensors such as iMGs or HIT systems for immediate practical insights into identifying sports injuries. Other methods identified in this review are notable but provide a significant gap in practicality for sporting bodies.
Future developments should focus on standardising study protocols, increasing female representation, and developing transdisciplinary tools adaptable across sports. The development of a robust, ergonomic tool designed for the end user that matches the accuracy of biomarkers included in this review would require a strong point-of-care tool for injuries that otherwise take many hours to diagnose.
Alternatively, further development of the sensors included, such as iMGs integrated with GNNs, would deliver a tool amalgamating the current best detection methods for sports injuries—VA, sensors, and AI. These findings direct future research to include samples representative of all people who play sports, with refined research protocols that are time-sensitive, to reduce athlete drop-out, which in turn would increase research output quality through reliable results.
Author Contributions
Conceptualisation, L.C.D., L.R., and E.D.; methodology, L.C.D.; formal analysis, L.C.D.; investigation, L.C.D.; data curation, L.C.D., L.R., and E.D.; writing—original draft preparation, L.C.D.; writing—review and editing, L.R., E.D., and M.M.; visualisation, L.C.D., L.R., E.D., and M.M.; supervision, M.M., L.R., and E.D. All authors have read and agreed to the published version of the manuscript.
Funding
TU RISE is co-funded by the Government of Ireland and the European Union through the ERDF Southern, Eastern & Midland Regional Programme 2021–2027 and the Northern & Western Regional Programme 2021–2027.
Data Availability Statement
Data will be available on reasonable request to the corresponding author.
Conflicts of Interest
There are no conflicts of interest declared.
Abbreviations
The following abbreviations are used in this manuscript:
| KD | King–Devick |
| VA | Video Assessment |
| NfL | Neurofilament Light |
| VMT | Visuomotor Racking |
| GFAP | Glial Fibrillary Acidic Protein |
| MiRN | Micro-Ribonucleic Acid |
| HIT | Head Impact Telemetry |
| ONSD | Optic Nerve Sheath Diameter |
| KD-ET | King–Devick Eye Tracking |
| FT | Field Test |
| CSF | Cerebrospinal Fluid |
| TTG | Timed Tandem Gate |
| MBESS | Multiple Balance Error Scoring System |
| QSM | Quantitative Susceptibility Mapping |
| RsfMRI | Resting-State Functional Magnetic Resonance Imaging |
| SAC | Standard Assessment of Concussion |
| U | Ultrasound |
| SRC | Sport-Related Concussion |
| MTBI | Mild Traumatic Brain Injury |
| PPCS | Persistent Post-Concussive Symptoms |
| HSI | Hamstring Strain Injury |
| OCD | Osteochondritis Dissecans |
| PC | Prospective Cohort Study |
| CSO | Cross-Sectional Study |
| O | Observational Study |
| PCC | Prospective Case–Control |
| C | Contact Sport Not Specified |
| CH | Cheerleading |
| LCD | Luke Canavan Dignam |
| LR | Lisa Ryan |
| MM | Michael McCann |
| ED | Ed Daly |
| iMg | Instrumented Mouth Guard |
| DKI | Diffusion Kurtosis |
| GNN | Graphical Neural Network |
| CASP | Critical Appraisal Skills Programme |
References
- Sprouse, B.; Chandran, A.; Rao, N.; Boltz, A.J.; Johnson, M.; Hennis, P.; Varley, I. Injury and illness surveillance monitoring in team sports: A framework for all. Inj. Epidemiol. 2024, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Albicini, M.; McKinlay, A. A review of sideline assessment measures for identifying sports-related concussion. J. Concussion 2018, 2, 205970021878482. [Google Scholar] [CrossRef]
- Ferdinand Pennock, K.; McKenzie, B.; McClemont Steacy, L.; Mainwaring, L. Under-reporting of sport-related concussions by adolescent athletes: A systematic review. Int. Rev. Sport Exerc. Psychol. 2020, 16, 66–92. [Google Scholar] [CrossRef]
- Kroshus, E.; Garnett, B.; Hawrilenko, M.; Baugh, C.M.; Calzo, J.P. Concussion under-reporting and pressure from coaches, teammates, fans, and parents. Social. Sci. Med. 2015, 134, 66–75. [Google Scholar] [CrossRef]
- McCrea, M.; Hammeke, T.; Olsen, G.; Leo, P.; Guskiewicz, K. Unreported concussion in high school football players: Implications for prevention. Clin. J. Sport. Med. 2004, 14, 13–17. [Google Scholar] [CrossRef]
- Mihalik, J.P.; Bell, D.R.; Marshall, S.W.; Guskiewicz, K.M. Measurement of head impacts in collegiate football players: An investigation of positional and event-type differences. Neurosurgery 2007, 61, 1229–1235; discussion 1235. [Google Scholar] [CrossRef]
- Patricios, J.; Fuller, G.W.; Ellenbogen, R.; Herring, S.; Kutcher, J.S.; Loosemore, M.; Makdissi, M.; McCrea, M.; Putukian, M.; Schneider, K.J. What are the critical elements of sideline screening that can be used to establish the diagnosis of concussion? A systematic review. Br. J. Sports Med. 2017, 51, 888–894. [Google Scholar] [CrossRef]
- Thisani, S.K. Developing a High-Performance Sports Results Prediction Artificial Neural Network: Case Study on World Championship Boxing. Int. J. Comput. Sci. Sport 2024, 23, 1–21. [Google Scholar] [CrossRef]
- Bullock, G.S.; Mylott, J.; Hughes, T.; Nicholson, K.F.; Riley, R.D.; Collins, G.S. Just How Confident Can We Be in Predicting Sports Injuries? A Systematic Review of the Methodological Conduct and Performance of Existing Musculoskeletal Injury Prediction Models in Sport. Sports Med. 2022, 52, 2469–2482. [Google Scholar] [CrossRef]
- Stephenson, S.D.; Kocan, J.W.; Vinod, A.V.; Kluczynski, M.A.; Bisson, L.J. A comprehensive summary of systematic reviews on sports injury prevention strategies. Orthop. J. Sports Med. 2021, 9, 23259671211035776. [Google Scholar] [CrossRef]
- Van Eetvelde, H.; Mendonça, L.D.; Ley, C.; Seil, R.; Tischer, T. Machine learning methods in sport injury prediction and prevention: A systematic review. J. Exp. Orthop. 2021, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J. CASP Checklist: CASP Cohort Study Checklist. Available online: https://casp-uk.net/casp-tools-checklists/cohort-study-checklist/ (accessed on 12 May 2025).
- Page, M.J. CASP Checklist: CASP Cross-Sectional Studies Checklist. Available online: https://casp-uk.net/casp-tools-checklists/cross-sectional-studies-checklist/ (accessed on 12 May 2025).
- Wethe, J.V.; Bogle, J.; Dodick, D.W.; Howard, M.D.; Gould, A.R.; Butterfield, R.J.; Buras, M.R.; Adler, J.; Talaber, A.; Soma, D.; et al. Baseline Normative and Test-Retest Reliability Data for Sideline Concussion Assessment Measures in Youth. Diagnostics 2024, 14, 1661. [Google Scholar] [CrossRef] [PubMed]
- To, X.V.; Cumming, P.; Nasrallah, F. From impact to recovery: Tracking mild traumatic brain injury with MRI-a pilot study and case series. BMJ Open Sport. Exerc. Med. 2024, 10, e002010. [Google Scholar] [CrossRef]
- Sim, A.; Timmins, R.G.; Ruddy, J.D.; Shen, H.; Liao, K.; Maniar, N.; Hickey, J.T.; Williams, M.D.; Opar, D.A. Hamstring Strain Injury Risk Factors in Australian Football Change over the Course of the Season. Med. Sci. Sports Exerc. 2024, 56, 297–306. [Google Scholar] [CrossRef]
- Gard, A.; Kornaropoulos, E.N.; Portonova Wernersson, M.; Rorsman, I.; Blennow, K.; Zetterberg, H.; Tegner, Y.; De Maio, A.; Markenroth Bloch, K.; Bjorkman-Burtscher, I.; et al. Widespread White Matter Abnormalities in Concussed Athletes Detected by 7T Diffusion Magnetic Resonance Imaging. J. Neurotrauma 2024, 41, 1533–1549. [Google Scholar] [CrossRef]
- Teruya, S.; Ogawa, T.; Yamada, H.; Tsuge, H.; Michinobu, R.; Ikeda, K.; Hara, Y.; Kamada, H.; Yamazaki, M.; Yoshii, Y. Detection of Factors Related to the Development of Osteochondritis Dissecans in Youth Baseball Players Screening. Diagnostics 2023, 13, 3589. [Google Scholar] [CrossRef]
- Powell, D.R.L.; Petrie, F.J.; Docherty, P.D.; Arora, H.; Williams, E.M.P. Development of a Head Acceleration Event Classification Algorithm for Female Rugby Union. Ann. Biomed. Eng. 2023, 51, 1322–1330. [Google Scholar] [CrossRef]
- Gard, A.; Vedung, F.; Piehl, F.; Khademi, M.; Wernersson, M.P.; Rorsman, I.; Tegner, Y.; Pessah-Rasmussen, H.; Ruscher, K.; Marklund, N. Cerebrospinal fluid levels of neuroinflammatory biomarkers are increased in athletes with persistent post-concussive symptoms following sports-related concussion. J. Neuroinflamm. 2023, 20, 189. [Google Scholar] [CrossRef]
- DiFabio, M.S.; Smith, D.R.; Breedlove, K.M.; Pohlig, R.T.; Buckley, T.A.; Johnson, C.L. Altered brain functional connectivity in the frontoparietal network following an ice hockey season. Eur. J. Sport. Sci. 2023, 23, 684–692. [Google Scholar] [CrossRef]
- Rosén, A.; Gennser, M.; Oscarsson, N.; Kvarnström, A.; Sandström, G.; Seeman-Lodding, H.; Simrén, J.; Zetterberg, H. Protein tau concentration in blood increases after SCUBA diving: An observational study. Eur. J. Appl. Physiol. 2022, 122, 993–1005. [Google Scholar] [CrossRef]
- Hecimovich, M.; Murphy, M.; Chivers, P.; Stock, P. Evaluation and Utility of the King-Devick With Integrated Eye Tracking as a Diagnostic Tool for Sport-Related Concussion. Orthop. J. Sports Med. 2022, 10, 23259671221142255. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.M.; Yuditskaya, S.; Williamson, J.R.; Vian, T.R.; Lacirignola, J.J.; Shenk, T.E.; Talavage, T.M.; Heaton, K.J.; Quatieri, T.F. Using Oculomotor Features to Predict Changes in Optic Nerve Sheath Diameter and ImPACT Scores From Contact-Sport Athletes. Front. Neurol. 2021, 12, 584684. [Google Scholar] [CrossRef] [PubMed]
- Pin, E.; Petricoin, E., III; Cortes, N.; Bowman, T.G.; Andersson, E.; Uhlen, M.; Nilsson, P.; Caswell, S.V. Immunoglobulin A Autoreactivity toward Brain Enriched and Apoptosis-Regulating Proteins in Saliva of Athletes after Acute Concussion and Subconcussive Impacts. J. Neurotrauma 2021, 38, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, T.R.; Hendershot, K.A.; Liu, B.; Knezevic, A.; Jacobs, B.B.; Gore, R.K.; Guskiewicz, K.M.; Bazarian, J.J.; Phelps, S.E.; Wright, D.W.; et al. A Novel Neuropsychological Tool for Immersive Assessment of Concussion and Correlation with Subclinical Head Impacts. Neurotrauma Rep. 2021, 2, 232–244. [Google Scholar] [CrossRef]
- Laverse, E.; Guo, T.; Zimmerman, K.; Foiani, M.S.; Velani, B.; Morrow, P.; Adejuwon, A.; Bamford, R.; Underwood, N.; George, J.; et al. Plasma glial fibrillary acidic protein and neurofilament light chain, but not tau, are biomarkers of sports-related mild traumatic brain injury. Brain Commun. 2020, 2, fcaa137. [Google Scholar] [CrossRef]
- King, D.; Hume, P.A.; Clark, T.N.; Pearce, A.J. Use of the King-Devick test for the identification of concussion in an amateur domestic women’s rugby union team over two competition seasons in New Zealand. J. Neurol. Sci. 2020, 418, 117162. [Google Scholar] [CrossRef]
- Di Pietro, V.; Porto, E.; Ragusa, M.; Barbagallo, C.; Davies, D.; Forcione, M.; Logan, A.; Di Pietro, C.; Purrello, M.; Grey, M.; et al. Salivary MicroRNAs: Diagnostic Markers of Mild Traumatic Brain Injury in Contact-Sport. Front. Mol. Neurosci. 2018, 11, 290. [Google Scholar] [CrossRef]
- Brokaw, E.B.; Fine, M.S.; Kindschi, K.E.; Santago Ii, A.C.; Lum, P.S.; Higgins, M. Cross-sectional evaluation of visuomotor tracking performance following subconcussive head impacts. Technol. Health Care 2018, 26, 109–118. [Google Scholar] [CrossRef]
- Shahim, P.; Zetterberg, H.; Tegner, Y.; Blennow, K. Serum neurofilament light as a biomarker for mild traumatic brain injury in contact sports. Neurology 2017, 88, 1788–1794. [Google Scholar] [CrossRef]
- Makdissi, M.; Davis, G. The reliability and validity of video analysis for the assessment of the clinical signs of concussion in Australian football. J. Sci. Med. Sport 2016, 19, 859–863. [Google Scholar] [CrossRef]
- King, D.; Hume, P.; Gissane, C.; Clark, T. Use of the King-Devick test for sideline concussion screening in junior rugby league. J. Neurol. Sci. 2015, 357, 75–79. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Gissane, C.; Hume, P.A.; Flaws, M. The King-Devick test was useful in management of concussion in amateur rugby union and rugby league in New Zealand. J. Neurol. Sci. 2015, 351, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.C.; Fragala, M.S.; Kavouras, S.A.; Queen, R.M.; Pryor, J.L.; Casa, D.J. Biomarkers in sports and exercise: Tracking health, performance, and recovery in athletes. J. Strength Cond. Res. 2017, 31, 2920–2937. [Google Scholar] [CrossRef]
- Haller, N.; Behringer, M.; Reichel, T.; Wahl, P.; Simon, P.; Krüger, K.; Zimmer, P.; Stöggl, T. Blood-Based Biomarkers for Managing Workload in Athletes: Considerations and Recommendations for Evidence-Based Use of Established Biomarkers. Sports Med. 2023, 53, 1315–1333. [Google Scholar] [CrossRef]
- Pedlar, C.R.; Newell, J.; Lewis, N.A. Blood Biomarker Profiling and Monitoring for High-Performance Physiology and Nutrition: Current Perspectives, Limitations and Recommendations. Sports Med. 2019, 49, 185–198. [Google Scholar] [CrossRef]
- Crawford, S.K.; Wille, C.M.; Stiffler-Joachim, M.R.; Lee, K.S.; Bashford, G.R.; Heiderscheit, B.C. Spatial frequency analysis detects altered tissue organization following hamstring strain injury at time of injury but not return to sport. BMC Med. Imaging 2021, 21, 190. [Google Scholar] [CrossRef]
- Mancino, F.; Kayani, B.; Gabr, A.; Fontalis, A.; Plastow, R.; Haddad, F.S. Anterior cruciate ligament injuries in female athletes: Risk factors and strategies for prevention. Bone Jt. Open 2024, 5, 94–100. [Google Scholar] [CrossRef]
- Beech, J.; Jones, B.; Hughes, T.; Emmonds, S. Injury Profile in Youth Female Athletes: A Systematic Review and Meta-Analysis. Sports Med. 2024, 54, 1207–1230. [Google Scholar] [CrossRef]
- Lin, C.Y.; Casey, E.; Herman, D.C.; Katz, N.; Tenforde, A.S. Sex Differences in Common Sports Injuries. PM&R 2018, 10, 1073–1082. [Google Scholar] [CrossRef]
- Hendricks, S.; Till, K.; den Hollander, S.; Savage, T.N.; Roberts, S.P.; Tierney, G.; Burger, N.; Kerr, H.; Kemp, S.; Cross, M.; et al. Consensus on a video analysis framework of descriptors and definitions by the Rugby Union Video Analysis Consensus group. Br. J. Sports Med. 2020, 54, 566–572. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}