
Prosthodontic Considerations for Customized Subperiosteal Implants: A Consensus Report

 , ,
, ,  , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- Prosthodontic planning
- Provisionalization protocols
- Prosthetic design
- Surgical considerations
- Supportive therapy protocols
- General recommendations and future perspectives
3. Results
3.1. Prosthodontic Planning
- Adequate preoperative prosthodontic planning is crucial. For this purpose, it is essential to have a high-resolution helical CT scan, an accurate impression of the soft tissues with the aid of an intraoral scan (Standard Tessellation Language (STL) file), information regarding the intermaxillary relationship and vertical dimension, intraoral and extraoral photographs and a digital wax-up of the final prosthesis [2]. Cone-beam computer tomography (CBCT) is not suitable to plan CSIs due to its suboptimal image quality [6]. All these steps provide valuable information that will allow us to correctly design the CSI and its prosthetic connections.
- All professionals involved in the treatment (prosthodontists, surgeons, CSI manufacturers and laboratory technicians) must have access to the patient data and should discuss the treatment plan before manufacturing the CSI (EO).
- The patient should be involved, together with the healthcare professionals, in the decision-making process regarding the rehabilitation options. Establishing an adequate dentist–patient relationship must be based on trust and patient-centered care, taking into account the patient’s personal motivations in order to choose the most appropriate treatment solution [9,10]. Active listening and empathetic communication concerning personal needs are encouraged to establish trust and improve patients’ adherence to clinical recommendations and future follow-ups [11].
3.2. Provisionalization Protocols
- CSIs can be loaded immediately, on the same day of the surgical procedure [7].
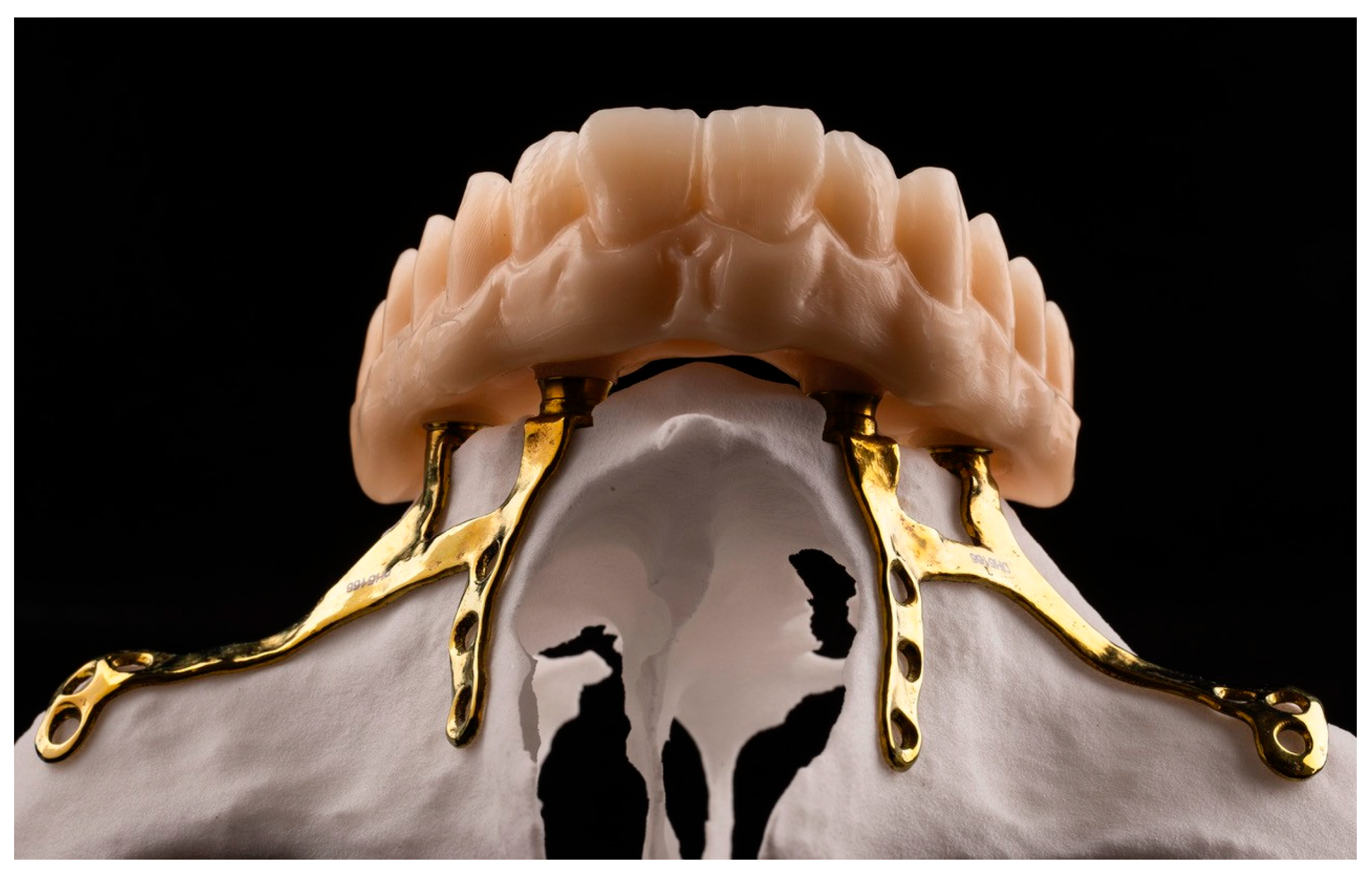
- It is essential to avoid pressure over the soft tissues with the provisional prosthesis. If possible, clinicians should consider leaving a visible space between the mucosa and the prosthesis to avoid pressure during healing and to facilitate oral hygiene (EO) (Figure 1).
- The provisional prosthesis must allow adequate access for oral hygiene (EO).
- The use of intermediate transepithelial abutments is recommended, and the emergence profile of the prosthesis should be straight (EO).
- CSI provisional prostheses can be made with the same materials used in the fabrication process for provisionals placed over conventional endosseous dental implants. The working group recommends the use of any CAD-CAM milled titanium-based material such as milled PMMA or acetal [7]. Additionally, 3D-printed resin prosthetic restorations can be considered but clinicians should be aware that the available evidence to support their use as a provisional prosthesis to be placed over a CSI is very scarce (EO).
- Although immediate placement of the provisional prosthesis using an intraoperative check bar is feasible, most authors recommend a delayed approach based on an impression made after CSI placement. This method ensures optimal accuracy, reduces discrepancies and favors the stability of the implant (EO).
- The final position of the CSI should not be jeopardized by the need to adapt the provisional prosthesis (EO).
3.3. Prosthetic Design
- At least four prosthetic connections are required. However, the number of connections should be adapted according to the patient’s characteristics, taking into account the risk factors associated with mechanical complications or CSI exposure. A greater number of connections seems to increase the incidence of exposures [2].
- Prosthetic connections should be placed with adequate spacing, leaving at least one tooth (pontic) between the connections, to ensure the correct distribution of functional loads and to minimize the risk of soft tissue dehiscences (EO).
- The working group recommends the use of removable intermediate transepithelial abutments (EO) (Figure 2).
- The materials used to fabricate definite prostheses over conventional endosseous dental implants can also be used in CSI prostheses [3,7,12]. New CAD-CAM materials (titanium or PEEK) with PMMA or composite resin coatings can be considered in order to reduce the weight of the prosthesis and/or to minimize overload on the CSI (EO) (Figure 3).
- The prosthetic screws should be placed with the recommended torques to avoid mechanical complications such as screw loosening (EO).
3.4. Surgical Considerations
- Buccal fat pad flaps may be an interesting approach to treat complications and exposures of CSIs. However, their routine use to prevent soft tissue dehiscences is not recommended, since these complications are associated with the CSI design and the amount of keratinized mucosa, rather than with the thickness of the buccal flap [4].
- Dental extractions should be done prior to CSI placement to allow proper tissue healing. If this is not feasible, basic periodontal therapy should be applied to the remaining teeth to remove biofilm and reduce inflammation (EO).
- The flap design should maximize the keratinized mucosa (EO). Distal vertical releasing incisions improve surgical access but should be placed far away from the posterior connections of the CSI [14].
- The prosthetic connection areas should have adequate keratinized mucosa to prevent possible exposures of the CSI (EO).
- The fixation screw protocol should be adapted according to the bone type involved. The fixation screw direction and primary stability are critical surgical factors (EO).
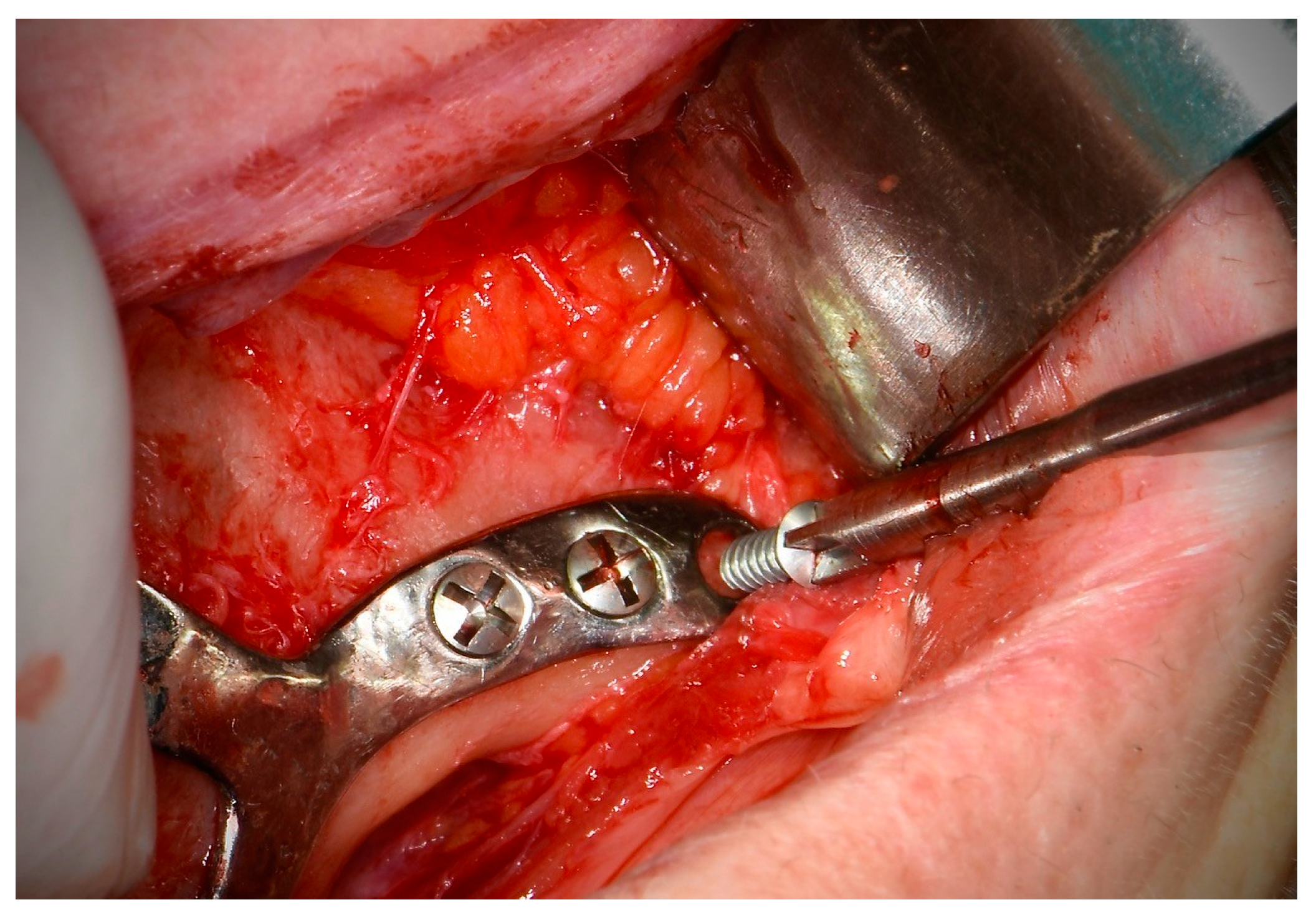
- Fixation screws should be placed perpendicular to the bone and in the center of the CSI insertion hole, maintaining the planned direction (EO) (Figure 4).
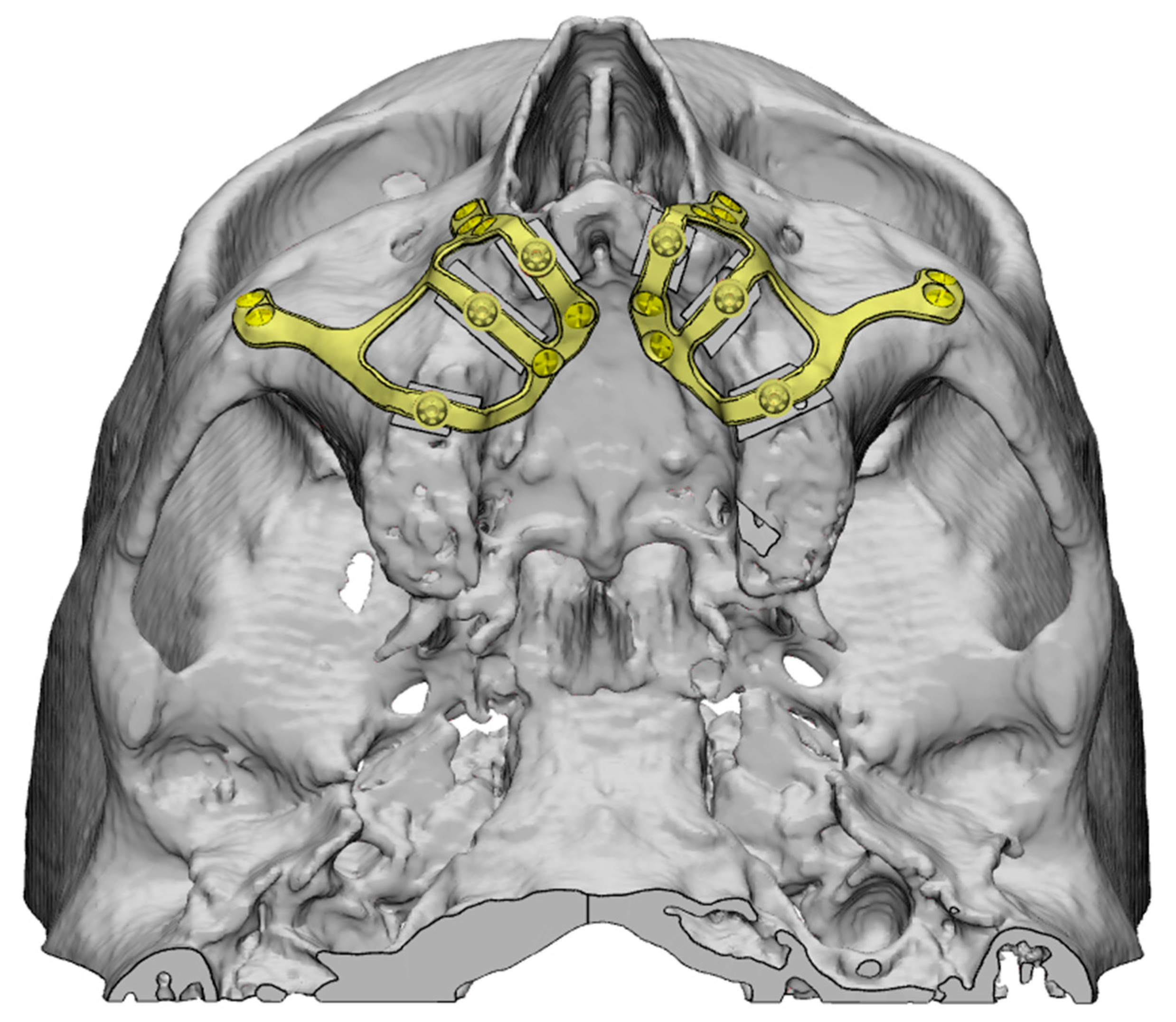
- The working group recommends the use of self-drilling screws to avoid the use of drills, which may compromise screw stability in areas of alveolar bone in cases of grade V atrophy. In cortical bone areas, such as the nasal buttress and zygomatic bone, drilling prior to screw placement is recommended in order to avoid excessive insertion torque, screw head deformation and/or screw fracture. Depending on the surgeon’s experience, the use of drills may be omitted in certain areas [2] (Figure 5).
- The number of fixation screws should ensure adequate mechanical stability of the CSI. A minimum of two screws per fixation area (palatal, zygomatic or nasal) is recommended [14]. Since the stability of the CSI depends on the number and length of the screws, their placement in the fixation areas should be maximized. Fixation screws in areas close to the alveolar ridge may increase the risk of CSI exposure, since they affect the design of the implant [2] (Figure 6).
- The use of a surgical cutting guide is essential in patients with grade V atrophy [5]. Placement of the CSI over the alveolar ridge should be avoided in order to minimize the presence of abrupt transitions, which are often associated with implant exposures. Titanium surgical cutting guides are rigid, thus providing greater precision and reducing the risk of particle release during the procedure. Other materials, such as a semirigid polyamide can be used, but further research is required to conduct a correct cost-effectiveness analysis (EO).
3.5. Supportive Therapy Protocols
- Clinicians should consider indicating an occlusal splint in all patients (EO).
- After placement of the CSI provisional prosthesis, patients should be followed-up on regularly (1, 3 and 6 months). At these appointments, clinicians should reassess both occlusion and proper access to oral hygiene (EO).
- All patients should undergo lifelong regular supportive therapy appointments at least every 6 months. However, patients considered to be at high risk of developing complications and peri-implant diseases (i.e., history of periodontal disease or poor oral hygiene) should have more frequent appointments (every 3–4 months). Follow-up controls should be primarily clinical. In the event of any complications (such as implant exposures or mobility), a cone-beam CT would be indicated (EO).
- Removal of the prosthesis is advisable in patients with inadequate biofilm control or when inflammation around the CSI connection areas is observed (EO).
- The main objective of regular supportive therapy appointments is to remove biofilm and calculus without changing the surface of the transepithelial abutment. For this purpose, mechanical debridement should be performed and may be complemented with the use of an antiseptic agent [12].
3.6. General Recommendations and Future Perspectives
3.6.1. General Recommendations
3.6.2. Future Perspectives
- The literature clearly provides limited long-term information on the occurrence of mechanical and/or biological complications. There are also few data regarding the use of CSIs in partial edentulous patients.
- Additional biomechanical approaches such as finite element studies or other experimental methods like strain-gauge analysis are required to compare the mechanical behavior of different CSIs and prosthesis designs.
- Bruxism could be a risk factor for complications in patients with CSIs. Further clinical data are needed to assess the risks, as its effects remain uncertain [15].
- The use of CSIs in systemically compromised patients and patients under antiresorptive or antiangiogenic treatment is controversial. Further research on this topic is required.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CSIs | Customized subperiosteal implants |
| CT | Computed tomography |
| CAD-CAM | Computer-aided design/Computed-aided manufacture |
| EO | Expert opinion |
| PMMA | Polymethyl methacrylate |
| PEEK | Polyether ether ketone |
| QoL | Quality of life |
| OHIP | Oral health impact profile |
| VAS | Visual analogue scale |
References
- Łoginoff, J.; Majos, A.; Elgalal, M. The evolution of custom subperiosteal implants for treatment of partial or complete edentulism in patients with severe alveolar ridge atrophy. J. Clin. Med. 2024, 13, 3582. [Google Scholar] [CrossRef] [PubMed]
- Onică, N.; Budală, D.G.; Baciu, E.R.; Onică, C.A.; Gelețu, G.L.; Murariu, A.; Balan, M.; Pertea, M.; Stelea, C. Long-term clinical outcomes of 3d-printed subperiosteal titanium implants: A 6-year follow-up. J. Pers. Med. 2024, 14, 541. [Google Scholar] [CrossRef]
- Chamorro-Pons, M.; Arias-Gallo, J.; Margarit-Pérez, L.; Demaría-Martínez, G.; Cidad-Vicario, A. Implantes subperiósticos personalizados para la rehabilitación completa del maxilar superior atrófico. Revisión de una serie clínica de 8 casos. Rev. Esp. Cir. Oral Maxilofac. 2021, 43, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Tofé-Povedano, Á.; Parras-Hernández, J.; Herce-López, J.; Matute-García, D.; Astolfi-González-Moguena, V.; Rollón-Mayordomo, Á. Design modifications in subperiosteal implants to avoid complications. Presentation of a case series study and literature review. Rev. Esp. Cir. Oral Maxilofac. 2023, 45, 57–63. [Google Scholar]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef]
- Herce-López, J.; Pingarrón, M.D.C.; Tofé-Povedano, Á.; García-Arana, L.; Espino-Segura-Illa, M.; Sieira-Gil, R.; Rodado-Alonso, C.; Sánchez-Torres, A.; Figueiredo, R. Customized subperiosteal implants for the rehabilitation of atrophic jaws: A consensus report and literature review. Biomimetics 2024, 9, 61. [Google Scholar] [CrossRef]
- Vatteroni, E.; Covani, U.; Menchini Fabris, G.B. The new generation of subperiosteal implants for patient-specific treatment of atrophic dental arches: Literature review and two case reports. Int. J. Periodontics Restor. Dent. 2023, 43, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Mommaerts, M.Y. Management of adverse effects following additively manufactured subperiosteal jaw implantation in the maxilla. J. Stomatol. Oral Maxillofac. Surg. 2024; 102206, in press. [Google Scholar] [CrossRef]
- Yuan, S.; Freeman, R.; Hill, K.; Newton, T.; Humphris, G. Communication, trust and dental anxiety: A person-centred approach for dental attendance behaviours. Dent. J. 2020, 8, 118. [Google Scholar] [CrossRef]
- Yamalik, N. Dentist-patient relationship and quality care 1. Introduction. Int. Dent. J. 2005, 55, 110–112. [Google Scholar] [CrossRef]
- Sánchez-Torres, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E. Validity and reliability of the Spanish version of the consultation and relational empathy measure in dental students (Sp-Dent-CARE): A cross-sectional study. Eur. J. Dent. Educ. 2024, 28, 267–274. [Google Scholar] [CrossRef]
- Van den Borre, C.; De Neef, B.; Loomans, N.A.J.; Rinaldi, M.; Nout, E.; Bouvry, P.; Naert, I.; Van Stralen, K.J.; Mommaerts, M.Y. Soft tissue response and determination of underlying risk drivers for recession and mucositis after AMSJI implantation in the maxilla. Int. J. Oral Maxillofac. Implant. 2024, 39, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, M.; Ozturk Muhtar, M.; Kundakcioglu, A.; Kucukcakir, O.; Cansiz, E. Evaluation of clinical success of the 3D-printed custom-made subperiosteal implants. J. Craniofac. Surg. 2024, 35, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Biglio, A.; Roy, M.; Salzano, G.; Troise, S.; Abbate, V.; Mayo-Yanez, M.; Lechien, J.R.; Piombino, P.; De Riu, G. Full-arch rehabilitation of severely atrophic maxilla with additively manufactured custom-made subperiosteal implants: A multicenter retrospective study. J. Cranio-Maxillofac. Surg. 2024, 52, 991–998. [Google Scholar] [CrossRef]
- De Moor, E.; Huys, S.E.F.; van Lenthe, G.H.; Mommaerts, M.Y.; Vander Sloten, J. Mechanical evaluation of a patient-specific additively manufactured subperiosteal jaw implant (AMSJI) using finite-element analysis. Int. J. Oral Maxillofac. Surg. 2022, 51, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.R.G.R.; Grillo, R. Maxillary rehabilitation after zygomatic implant sequelae using custom subperiosteal implants: A case study. J. Stomatol. Oral Maxillofac. Surg. 2024, 126, 102154. [Google Scholar] [CrossRef]
- Cebrián-Carretero, J.L.; Del Castillo-Pardo de Vera, J.L.; Montesdeoca-García, N.; Garrido-Martínez, P.; Pampín-Martínez, M.M.; Aragón-Niño, I.; Navarro-Cuéllar, I.; Navarro-Cuéllar, C. Virtual surgical planning and customized subperiosteal titanium maxillary implant (CSTMI) for three dimensional reconstruction and dental implants of maxillary defects after oncological resection: Case series. J. Clin. Med. 2022, 11, 4594. [Google Scholar] [CrossRef]
- Anitua, E.; Eguia, A.; Staudigl, C.; Alkhraisat, M.H. Clinical performance of additively manufactured subperiosteal implants: A systematic review. Int. J. Implant. Dent. 2024, 10, 4. [Google Scholar] [CrossRef]
- Van den Borre, C.; De Neef, B.; Loomans, N.A.J.; Rinaldi, M.; Nout, E.; Bouvry, P.; Naert, I.; Mommaerts, M.Y. Patient satisfaction and impact on oral health after maxillary rehabilitation using a personalized additively manufactured subperiosteal jaw implant (AMSJI). J. Pers. Med. 2023, 13, 297. [Google Scholar] [CrossRef]
- Van den Borre, C.; Rinaldi, M.; De Neef, B.; Loomans, N.A.J.; Nout, E.; Van Doorne, L.; Naert, I.; Politis, C.; Schouten, H.; Klomp, G.; et al. Radiographic evaluation of bone remodeling after additively manufactured subperiosteal jaw implantation (AMSJI) in the maxilla: A one-year follow-up study. J. Clin. Med. 2021, 10, 3542. [Google Scholar] [CrossRef]
- Kundakcioglu, A.; Ayhan, M. Evaluation of different subperiosteal implant thicknesses on mechanical strength and stress on bone by finite element analysis. Int. J. Med. Sci. 2024, 21, 1672–1680. [Google Scholar] [CrossRef]
- Dalkey, N.; Helmer, O. An experimental application of the Delphi method to the use of experts. Manag. Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tofé-Povedano, Á.; Herce-López, J.; del Canto-Pingarrón, M.; Sieira-Gil, R.; Rodado-Alonso, C.; Garrido-Martínez, P.; Reyes-Minguillán, J.; Camps-Font, O.; Sánchez-Torres, A.; Figueiredo, R. Prosthodontic Considerations for Customized Subperiosteal Implants: A Consensus Report. Appl. Sci. 2025, 15, 7633. https://doi.org/10.3390/app15147633
Tofé-Povedano Á, Herce-López J, del Canto-Pingarrón M, Sieira-Gil R, Rodado-Alonso C, Garrido-Martínez P, Reyes-Minguillán J, Camps-Font O, Sánchez-Torres A, Figueiredo R. Prosthodontic Considerations for Customized Subperiosteal Implants: A Consensus Report. Applied Sciences. 2025; 15(14):7633. https://doi.org/10.3390/app15147633
Chicago/Turabian StyleTofé-Povedano, Álvaro, Javier Herce-López, Mariano del Canto-Pingarrón, Ramón Sieira-Gil, Carlos Rodado-Alonso, Pablo Garrido-Martínez, Jorge Reyes-Minguillán, Octavi Camps-Font, Alba Sánchez-Torres, and Rui Figueiredo. 2025. "Prosthodontic Considerations for Customized Subperiosteal Implants: A Consensus Report" Applied Sciences 15, no. 14: 7633. https://doi.org/10.3390/app15147633
APA StyleTofé-Povedano, Á., Herce-López, J., del Canto-Pingarrón, M., Sieira-Gil, R., Rodado-Alonso, C., Garrido-Martínez, P., Reyes-Minguillán, J., Camps-Font, O., Sánchez-Torres, A., & Figueiredo, R. (2025). Prosthodontic Considerations for Customized Subperiosteal Implants: A Consensus Report. Applied Sciences, 15(14), 7633. https://doi.org/10.3390/app15147633