



A Comparison Between the Mézières Method and Isostretching Postures for Frontal Stand Curvatures and Functionality in Elite Female Rhythmic Gymnasts with Low Back Pain: A Randomized Controlled Trial


Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
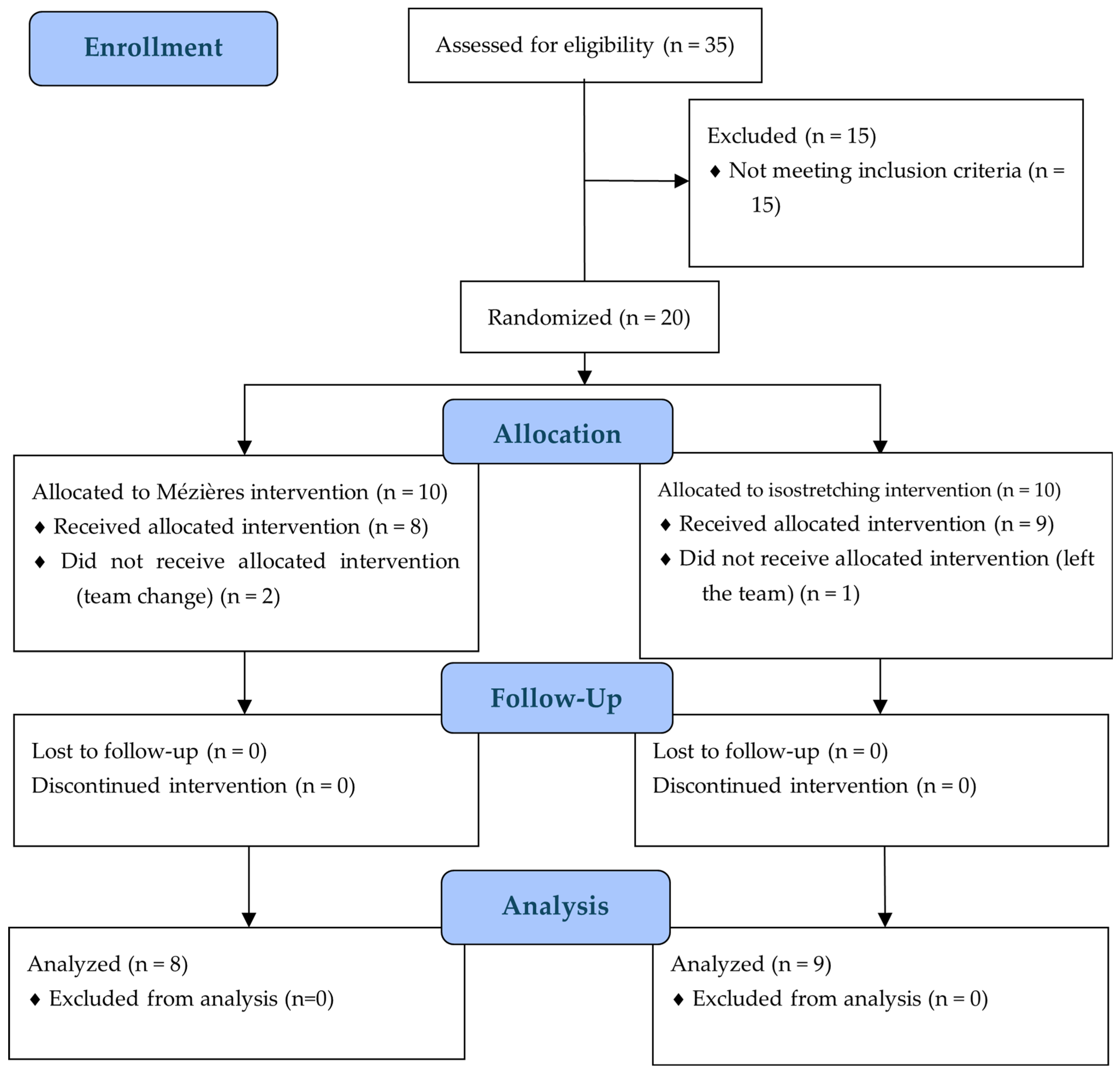
2.1. Trial Design
Recruitment
2.2. Study Setting
2.3. Participants
2.4. Outcomes
Athlete Observations and Physical Exploration Phase
2.5. Intervention
2.5.1. Mézières Method Experimental Group
2.5.2. Isostretching Posture Control Treatment Group
2.6. Statistical Analysis
2.6.1. Power Analysis and Rationale for Sample Size
2.6.2. Statistics
3. Results
3.1. Participant Baseline Characteristics
3.2. Multifactorial Analysis of NRS
3.3. Frontal Stand Upright Position Results
3.4. Frontal Standing Left Position Results
3.5. Frontal Standing Right Position Results
3.6. Frontal Standing Upright–Left Difference Position Results
3.7. Frontal Stand Upright–Right Difference Position Results
3.8. Frontal Stand Left–Right Difference Position
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LBP | Low back pain |
| RCT | Randomized controlled trial |
| NRS | Numeric Rating Scale |
| C7 | Cervical region 7 |
| TH1-12 | Thoracic region 1-12 |
| THSp | Thoracic spine vertebrae |
| L1-5 | Lumbar region 1-5 |
| LSp | Lumbar spine vertebrae |
| S1 | Sacrum region 1 |
| Sac/Hip | Sacrum–hip |
References
- Machado, G.F.; Bigolin, S.E. Comparative case study between neural mobilization and a muscle stretching program in chronic low back pain. Fisioter. Mov. 2010, 23, 545–554. [Google Scholar] [CrossRef]
- Soares, P.; Cabral, V.; Mendes, M.; Vieira, R.; Avolio, G.; Gomes de Souza Vale, R. Effects of the Posture School Program and Global Postural Reeducation on range of motion and pain levels in patients with chronic low back pain. Rev. Andal. Med. Dep. 2016, 9, 23–28. [Google Scholar] [CrossRef]
- Sahin, N.; Albayrak, I.; Durmus, B.; Ugurlu, H. Effectiveness of back school for pain and functional disability in chronic low back pain: A randomized controlled trial. J. Rehabil. Med. 2011, 43, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Roios, E.; Paredes, A.C.; Alves, A.F.; Pereira, M.G. Cognitive representations in low back pain in patients receiving chiropractic versus physiotherapy treatment. J. Health Psychol. 2017, 22, 1012–1024. [Google Scholar] [CrossRef]
- Hangai, M.; Kaneoka, K.; Okubo, Y.; Miyakawa, S.; Hinotsu, S.; Mukai, N.; Sakane, M.; Ochiai, N. Relationship between low back pain and competitive sports activities during youth. Am. J. Sports Med. 2010, 38, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.P.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal pain in gymnasts: A retrospective analysis on a cohort of professional athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef]
- Benjamin, H.J.; Engel, S.C.; Chudzik, D. Wrist pain in gymnasts: A review of common overuse wrist pathology in gymnastics athletes. Curr. Sports Med. Rep. 2017, 16, 322–329. [Google Scholar] [CrossRef]
- DiFiori, J.P. Overuse injury and the young athlete: The case of chronic wrist pain in gymnasts. Curr. Sports Med. Rep. 2006, 5, 165–167. [Google Scholar] [CrossRef]
- Cugusi, L.; Manca, A.; Sarritzu, S.; Bergamin, M.; Gobbo, S.; Di Blasio, A.; Massidda, M.; Cupisti, A.; Bandiera, P.; Deriu, F. Risk factors associated with low back pain in competitive female gymnasts: A meta-analytic approach. J. Sports Sci. 2020, 38, 2543–2552. [Google Scholar] [CrossRef]
- Zetaruk, M.; Violan, M.; Zurakowski, D.; Mitchell, W.A., Jr.; Micheli, L.J. Recommendations for training and injury prevention in elite rhythmic gymnasts. Apunt. Med. Esport 2006, 41, 100–106. [Google Scholar] [CrossRef]
- Hutchinson, M.R. Low back pain in elite rhythmic gymnasts. Med. Sci. Sports Exerc. 1999, 31, 1686–1688. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Evangelisti, I.; Piazza, M.; Galetta, F.; Morelli, E. Low back pain in competitive rhythmic gymnasts. J. Sports Med. Phys. Fit. 2004, 44, 49–53. [Google Scholar]
- Lena, O.; Todri, J.; Todri, A.; Martinez Gil, J.L.; Gomez Gallego, M. The effectiveness of the Mézières Method in elite rhythmic gymnastics athletes with low back pain: A randomized controlled trial. J. Sport Rehabil. 2019, 29, 913–919. [Google Scholar] [CrossRef]
- Wyatt, H.E.; Gittoes, M.J.R.; Irwin, G. Sport-specific musculoskeletal growth and postural control in female artistic gymnasts: A 12-month cohort study. Sports Biomech. 2020, 19, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Heitkamp, H.C.; Horstmann, T. Discomforts and injuries of the spine and medical examinations in young talented female gymnasts. Sportverletz. Sportschaden 2005, 19, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K. Spine injuries in rhythmic gymnastics. Sport Health 2009, 27, 27–29. [Google Scholar]
- Lena, O.; Qorri, E.; Martínez-Fuentes, J.; Todri, J. Evaluation of trunk mobility in spanish high-level national rhythmic gymnastics athletes with low back pain: A randomized controlled trial comparing the Mézières method and isostretching postures. J. Clin. Med. 2025, 14, 2584. [Google Scholar] [CrossRef]
- Todri, J.; Qorri, E.; Martínez-Fuentes, J.; Lena, O. A double-blind randomized controlled trial comparing the effects of the Mézières method and isostretching postures in sagittal stand position evaluated through the Spinal Mouse® in elite rhythmic gymnasts with low back pain. Arch. Med. Sci. 2025, 21, 327–338. [Google Scholar] [CrossRef]
- Lena, O.; Qorri, E.; Martínez-Fuentes, J.; Todri, J. Mézières method vs. isostretching postures on countermovement jump performance in elite rhythmic gymnasts with low back pain: A randomized controlled trial. Appl. Sci. 2025, 15, 3477. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G.; CONSORT. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomized trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Lawand, P.; Lombardi Júnior, I.; Jones, A.; Sardim, C.; Ribeiro, L.H.; Natour, J. Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: A randomized controlled trial. Jt. Bone Spine 2015, 82, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Guastala, F.A.M.; Guerini, M.H.; Klein, P.F.; Leite, V.C.; Cappellazzo, R.; Facci, L.M. Effect of global postural re-education and isostretching in patients with nonspecific chronic low back pain: A randomized clinical trial. Fisioter. Mov. 2016, 29, 515–525. [Google Scholar] [CrossRef]
- Wikström, L.; Nilsson, M.; Broström, A. Patients’ self-reported nausea: Validation of the numerical rating scale and a daily summary of repeated numerical rating scale scores. J. Clin. Nurs. 2019, 28, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.R.; Lopez, M. Neck and back pain-specific outcome assessment questionnaires in the Spanish language: A systematic literature review. Spine J. 2013, 13, 1667–1674. [Google Scholar] [CrossRef]
- Livanelioglu, A.; Kaya, F.; Nabiyev, V.; Demirkiran, G.; Firat, T. The validity and reliability of the “Spinal Mouse” assessment of spinal curvatures in the frontal plane in pediatric adolescent idiopathic thoraco-lumbar curves. Eur. Spine J. 2016, 25, 476–482. [Google Scholar] [CrossRef]
- Mannion, A.F.; Knecht, K.; Balaban, G.; Dvorak, J.; Grob, D. A new skin-surface device for measuring the curvature and global and segmental ranges of motion of the spine: Reliability of measurements and comparison with data reviewed from the literature. Eur. Spine J. 2004, 13, 122–136. [Google Scholar] [CrossRef]
- Porsnok, D.; Mutlu, A.; Livanelioğlu, A. Assessment of spinal alignment in children with unilateral cerebral palsy. Clin. Biomech. 2022, 100, 105800. [Google Scholar] [CrossRef] [PubMed]
- Lena, O.; Todri, J.; Todri, A.; Papajorgji, P.; Martinez Fuentes, J. A randomized controlled trial concerning the implementation of the postural Mézières treatment in elite athletes with low back pain. Postgrad. Med. 2022, 134, 559–572. [Google Scholar] [CrossRef]
- Lena, O.; Todri, J.; Todri, A.; Azorín, L.F.; Fuentes, J.M.; Papajorgji, P.; Sanchez, S.H.; Castejon, M.C.; Garzón, M.C.L.; Gil, J.L.M. The Mézières Method as a novel treatment for elite Spanish second-division soccer league players with low back pain: A randomized controlled trial. J. Sport Rehabil. 2022, 31, 398–413. [Google Scholar] [CrossRef]
- Prado, É.R.A.; Meireles, S.M.; Carvalho, A.C.A.; Mazoca, M.F.; Neto, A.D.M.M.; Da Silva, R.B.; Trindade Filho, E.M.; Júnior, I.L.; Natour, J. Influence of isostretching on patients with chronic low back pain: A randomized controlled trial. Physiother. Theory Pract. 2021, 37, 287–294. [Google Scholar] [CrossRef]
- Mann, L.; Kleinpaul, J.F.; Weber, P.; Bolli Mota, C.; Pivetta Carpes, F. Effect of isostretching training on chronic low back pain: A case study. Motriz 2009, 15, 50–60. [Google Scholar]
- Cools, A.M.; Geerooms, E.; Van den Berghe, D.F.; Cambier, D.C.; Witvrouw, E.E. Isokinetic scapular muscle performance in young elite gymnasts. J. Athl. Train. 2007, 42, 458–463. [Google Scholar] [PubMed]

{kind=link}
| Groups | Mean | SD | Median | W Statistic | Test Used | t/U | p | |
|---|---|---|---|---|---|---|---|---|
| Age | Isostretch | 13.00 | 0.4895 | Mann–Whitney U | 15 | 0.032 | ||
| Mézières | 13.50 | |||||||
| Height | Isostretch | 153.78 | 10.895 | 0.9657 | Shapiro–Wilk | −1.051 | 0.7398 | |
| Mézières | 158.75 | 8.225 | ||||||
| Weight | Isostretch | 40.56 | 6.56 | 0.955 | Shapiro–Wilk | −1.765 | 0.5404 | |
| Mézières | 47.06 | 8.612 | ||||||
| Body Temperature | Isostretch | 36.656 | 0.3432 | 0.9035 | Shapiro-Wilk | 0.803 | 0.0777 | |
| Mézières | 36.5 | 0.4536 | ||||||
| Training hours per weak | Isostretch | 15.00 | 0.7859 | Mann–Whitney U | 33.5 | 0.838 | ||
| Mézières | 15.00 | |||||||
| NRS | Isostretch | 5.722 | 1.4814 | 0.9339 | Shapiro-Wilk | 1.187 | 0.254 | |
| Mézières | 4.938 | 1.2082 | ||||||
 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Frontal Standing Left | Frontal Standing Upright | Frontal Standing Right | ||||||||||||
| Vertebral Scanning | Mean | SD | t | p | Mean | SD | t | p | Mean | SD | t | p | ||
| Regional | Sac/Hip | Isostretch | 1.22 | 9.667 | −0.867 | 0.400 | 17.00 | 7.246 | 2.324 | 0.035 | 14.44 | 7.844 | −0.557 | 0.586 |
| Mézières | 5.25 | 9.438 | 9.63 | 5.605 | 17.25 | 12.658 | ||||||||
| THSpTH12 | Isostretch | −2.56 | 7.502 | 1.638 | 0.122 | 2.22 | 6.667 | 0.802 | 0.435 | 3.56 | 10.113 | −2.348 | 0.033 | |
| Mézières | −8.63 | 7.763 | −23.75 | 97.341 | 17.13 | 13.643 | ||||||||
| LSpTH12 | Isostretch | −30.22 | 11.563 | −0.613 | 0.549 | −15.89 | 9.239 | −0.819 | 0.425 | 15.33 | 11.203 | 0.636 | 0.535 | |
| Mézières | −27.00 | 9.885 | −12.50 | 7.597 | 10.50 | 19.523 | ||||||||
| Inclination | Isostretch | −22.67 | 3.354 | −1.763 | 0.098 | 3.33 | 1.732 | 1.227 | 0.239 | 29.22 | 8.599 | −0.255 | 0.802 | |
| Mézières | −18.75 | 5.651 | 2.25 | 1.909 | 30.25 | 7.924 | ||||||||
| Length | Isostretch | 410.89 | 46.145 | −1.312 | 0.209 | 442.00 | 22.383 | −0.867 | 0.400 | 429.89 | 37.605 | −0.675 | 0.510 | |
| Mézières | 445.00 | 60.814 | 463.00 | 68.962 | 446.88 | 64.295 | ||||||||
| Frontal Plan | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trial Groups | Repeated-Measures ANOVA | ||||||||||||||
| Isostretching | Mézières | ||||||||||||||
| Pre | Post 3 Months | Pre Treatment | Post 3 Months | Groups | Time | Time*Groups | |||||||||
| Pain Intensity | Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | p | η2 | p | η2 | p | η2 | |
| NRS | 5.722 | 1.4814 | 3.722 | 1.5434 | 4.938 | 1.2082 | 1.625 | 1.0607 | 0.005 | 0.416 | 0.000 | 0.813 | 0.108 | 0.445 | |
| Regional vertebral evaluation | |||||||||||||||
| Frontal standing upright | Sac/Hip | 17.00 | 7.246 | 6.440 | 3.909 | 9.630 | 5.605 | 6.750 | 1.488 | 0.357 | 0.057 | 0.000 | 0.861 | 0.001 | 0.761 |
| THSpTH12 | 2.220 | 6.667 | 4.000 | 5.937 | −23.750 | 97.341 | 1.630 | 1.408 | 0.428 | 0.042 | 0.161 | 0.398 | 0.442 | 0.251 | |
| LSpTH12 | −15.890 | 9.239 | −6.110 | 6.274 | −12.500 | 7.597 | −5.380 | 2.669 | 0.879 | 0.002 | 0.021 | 0.591 | 0.037 | 0.546 | |
| Inclination | 3.330 | 1.732 | 2.890 | 2.421 | 2.250 | 1.909 | 2.750 | 2.121 | 0.000 | 0.828 | 0.122 | 0.431 | 0.413 | 0.263 | |
| Length | 442.000 | 22.383 | 438.780 | 26.076 | 463.000 | 68.962 | 500.000 | 70.593 | 0.082 | 0.189 | 0.017 | 0.179 | 0.213 | 0.101 | |
| Frontal standing left | Sac/Hip | 1.220 | 9.667 | −3.220 | 5.805 | 5.250 | 9.438 | −0.380 | 3.739 | 0.227 | 0.096 | 0.009 | 0.643 | 0.432 | 0.255 |
| THSpTH12 | −2.560 | 7.502 | −6.440 | 8.890 | −8.630 | 7.763 | −14.880 | 7.140 | 0.008 | 0.387 | 0.017 | 0.178 | 0.987 | 0.006 | |
| LSpTH12 | −30.220 | 11.563 | −26.890 | 8.253 | −27.000 | 9.885 | −23.250 | 8.860 | 0.952 | 0.000 | 0.060 | 0.502 | 0.299 | 0.315 | |
| Inclination | −22.670 | 3.354 | −27.330 | 4.690 | −18.750 | 5.651 | −22.630 | 7.891 | 0.544 | 0.025 | 0.006 | 0.207 | 0.069 | 0.133 | |
| Length | 410.89 | 46.145 | 425.670 | 31.325 | 445.000 | 60.814 | 495.880 | 71.742 | 0.034 | 0.267 | 0.001 | 0.264 | 0.442 | 0.060 | |
| Frontal standing right | Sac/Hip | 14.44 | 7.844 | 8.890 | 4.314 | 17.250 | 12.658 | 8.750 | 5.946 | 0.830 | 0.003 | 0.028 | 0.163 | 0.300 | 0.077 |
| THSpTH12 | 3.560 | 10.113 | 26.330 | 12.410 | 17.130 | 13.643 | 28.130 | 9.463 | 0.071 | 0.201 | 0.000 | 0.440 | 0.010 | 0.196 | |
| LSpTH12 | 15.330 | 11.203 | 19.78 | 7.067 | 10.500 | 19.523 | 14.880 | 5.866 | 0.379 | 0.052 | 0.548 | 0.049 | 0.682 | 0.037 | |
| Inclination | 29.220 | 8.599 | 29.440 | 7.073 | 30.250 | 7.924 | 27.880 | 7.882 | 0.750 | 0.007 | 0.959 | 0.010 | 0.615 | 0.043 | |
| Length | 429.890 | 37.605 | 435.330 | 40.872 | 446.880 | 64.295 | 491.880 | 63.831 | 0.106 | 0.165 | 0.001 | 0.253 | 0.317 | 0.074 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todri, J.; Qorri, E.; Martínez-Fuentes, J.; Lena, O. A Comparison Between the Mézières Method and Isostretching Postures for Frontal Stand Curvatures and Functionality in Elite Female Rhythmic Gymnasts with Low Back Pain: A Randomized Controlled Trial. Appl. Sci. 2025, 15, 5932. https://doi.org/10.3390/app15115932
Todri J, Qorri E, Martínez-Fuentes J, Lena O. A Comparison Between the Mézières Method and Isostretching Postures for Frontal Stand Curvatures and Functionality in Elite Female Rhythmic Gymnasts with Low Back Pain: A Randomized Controlled Trial. Applied Sciences. 2025; 15(11):5932. https://doi.org/10.3390/app15115932
Chicago/Turabian StyleTodri, Jasemin, Erda Qorri, Juan Martínez-Fuentes, and Orges Lena. 2025. "A Comparison Between the Mézières Method and Isostretching Postures for Frontal Stand Curvatures and Functionality in Elite Female Rhythmic Gymnasts with Low Back Pain: A Randomized Controlled Trial" Applied Sciences 15, no. 11: 5932. https://doi.org/10.3390/app15115932
APA StyleTodri, J., Qorri, E., Martínez-Fuentes, J., & Lena, O. (2025). A Comparison Between the Mézières Method and Isostretching Postures for Frontal Stand Curvatures and Functionality in Elite Female Rhythmic Gymnasts with Low Back Pain: A Randomized Controlled Trial. Applied Sciences, 15(11), 5932. https://doi.org/10.3390/app15115932