
Assessment of the Physico-Chemical, Microbial, and Cytotoxic Characteristics of Zirconia Crowns Utilized in Pediatric Dentistry

 , ,
, ,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Physico-Chemical Assay
2.2. Microbiological Assay
2.3. Histology Assay
3. Results
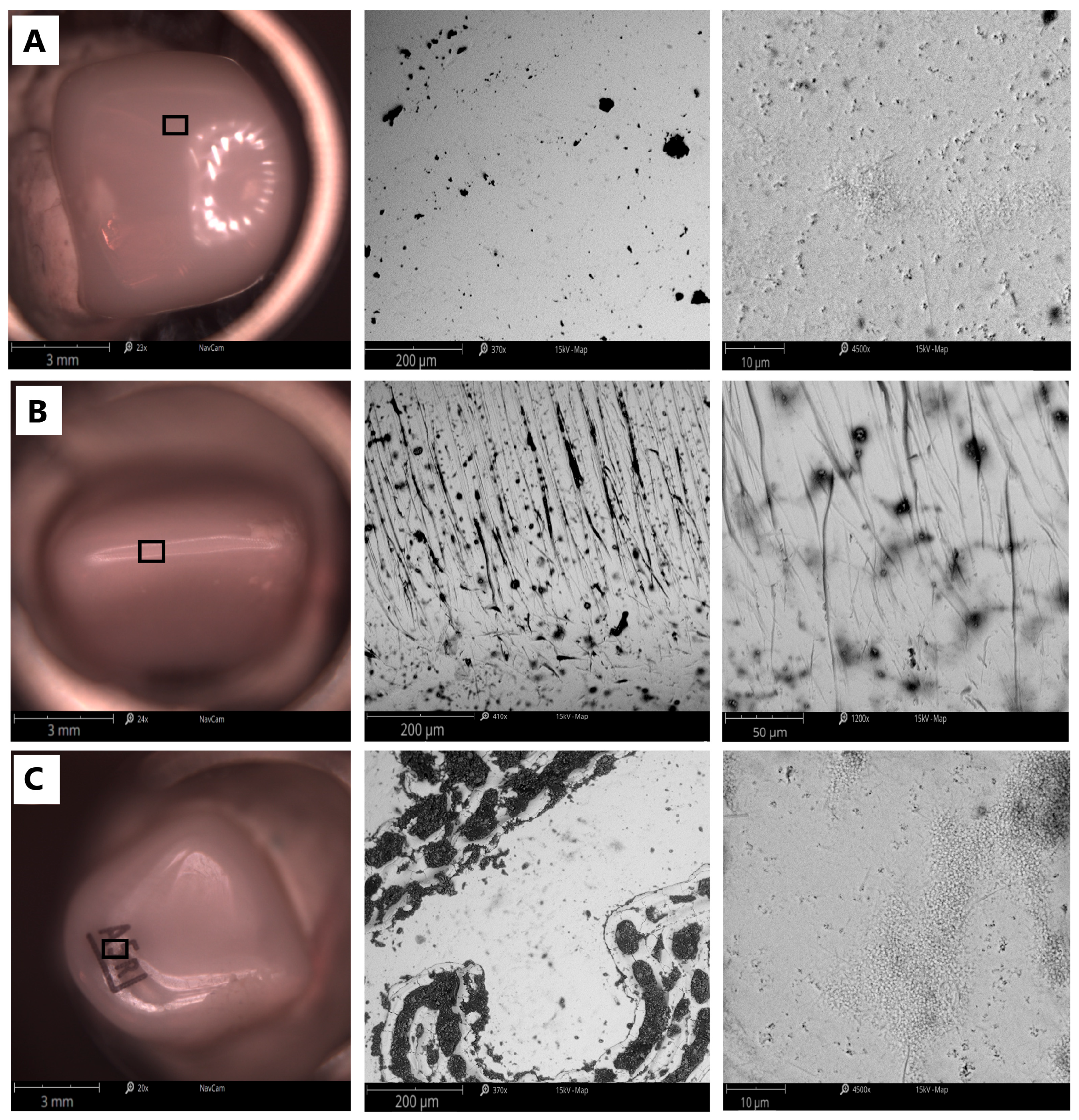
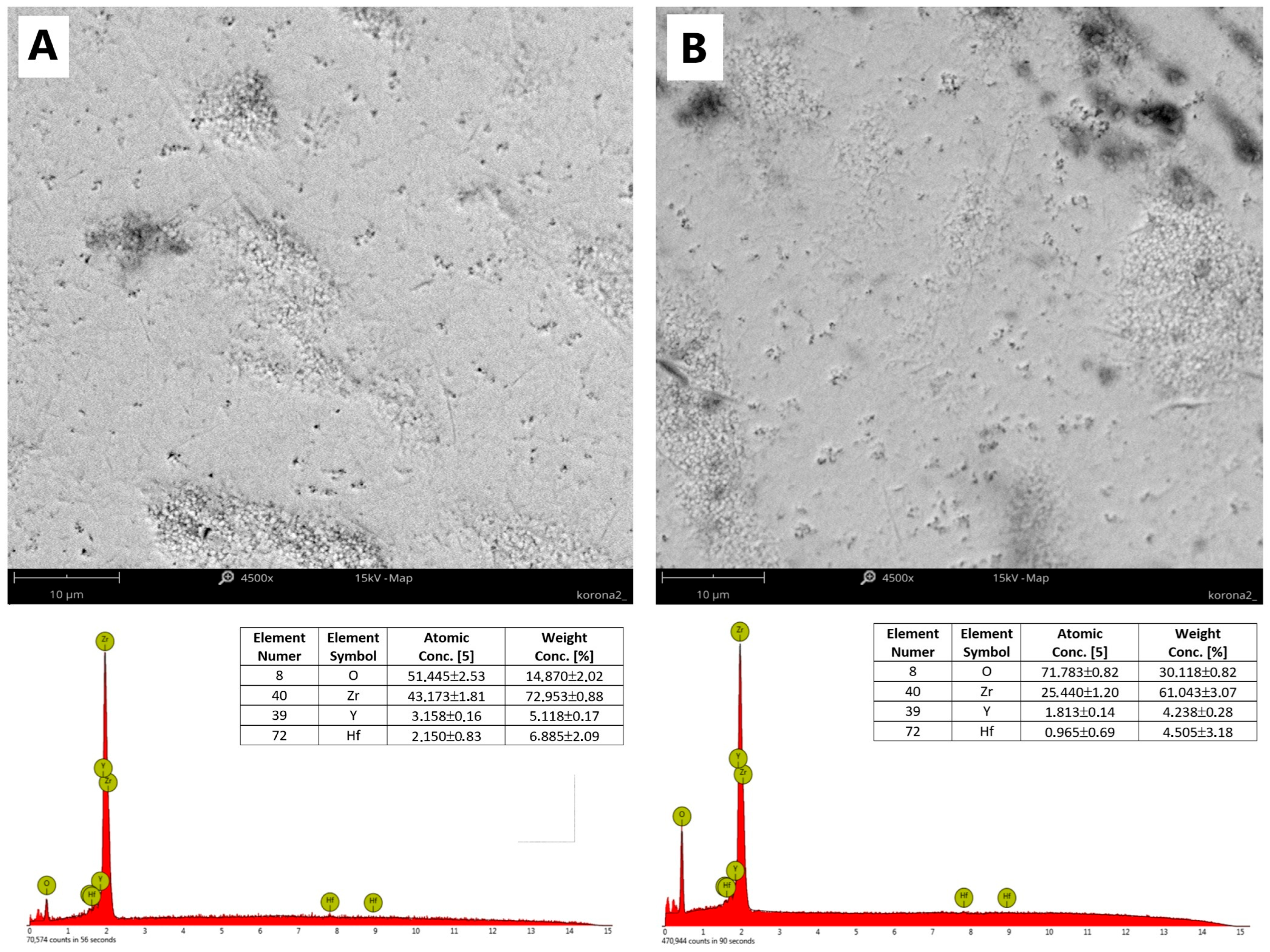
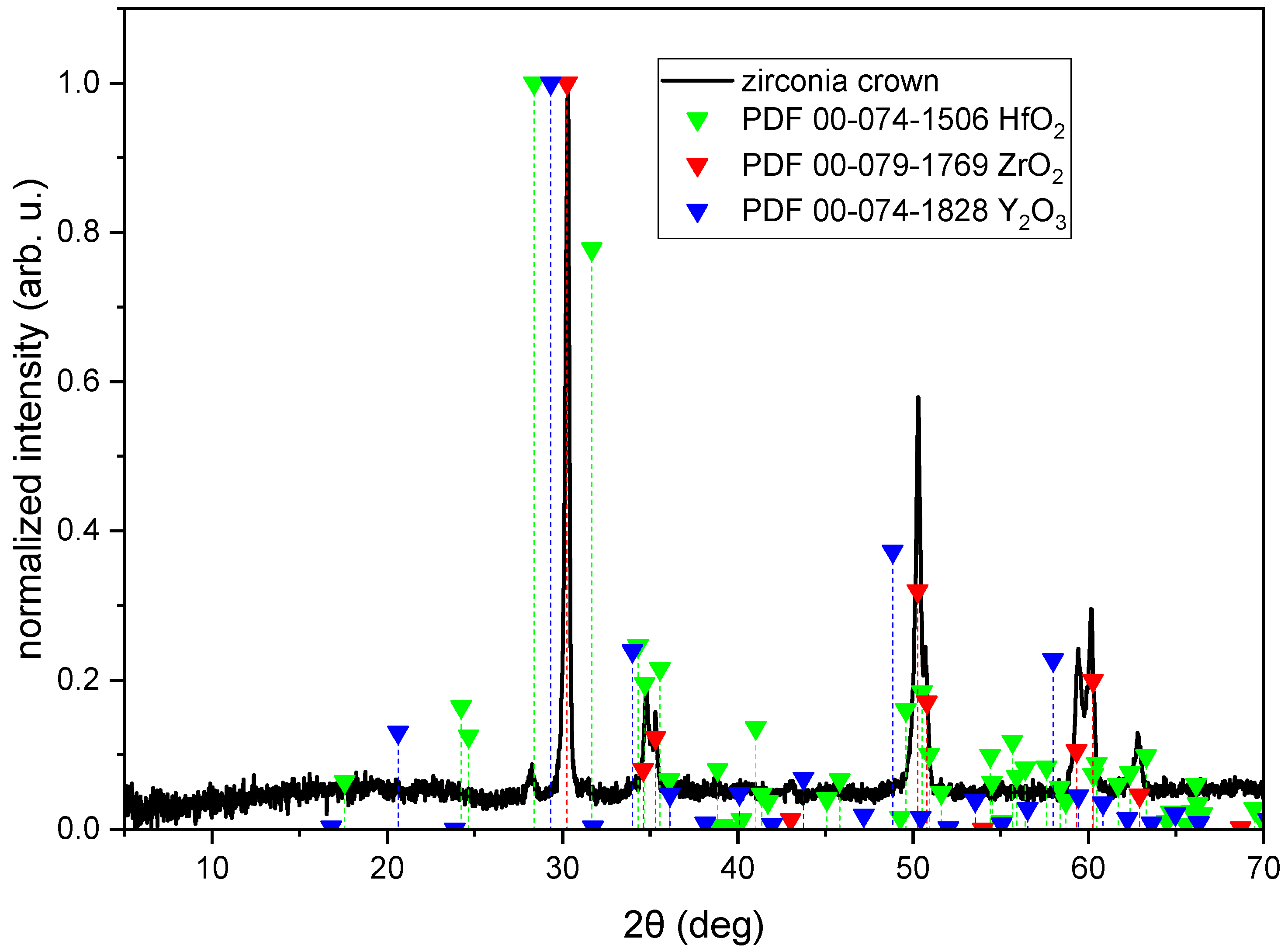
3.1. Physico-Chemical Assay Results
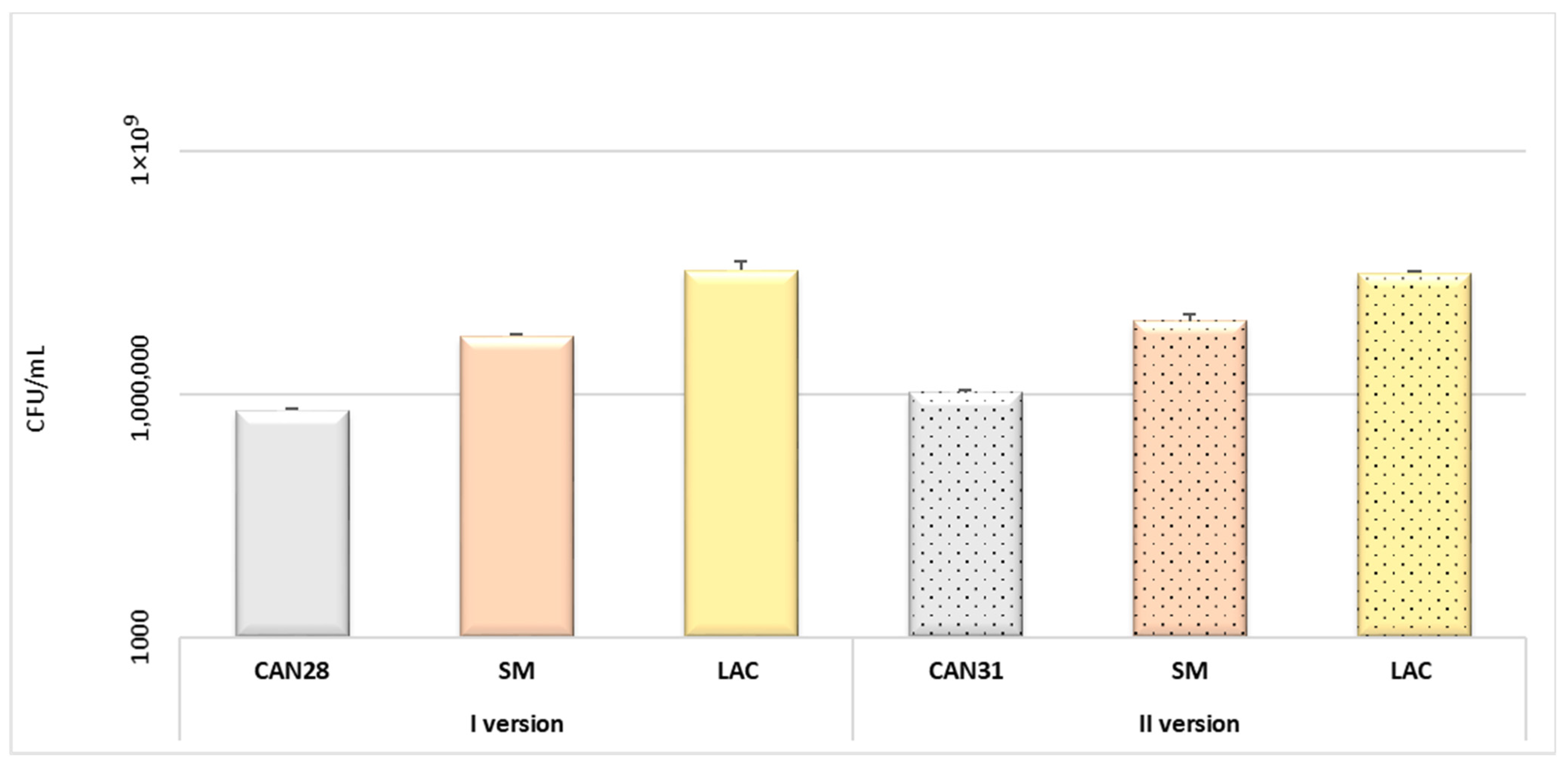
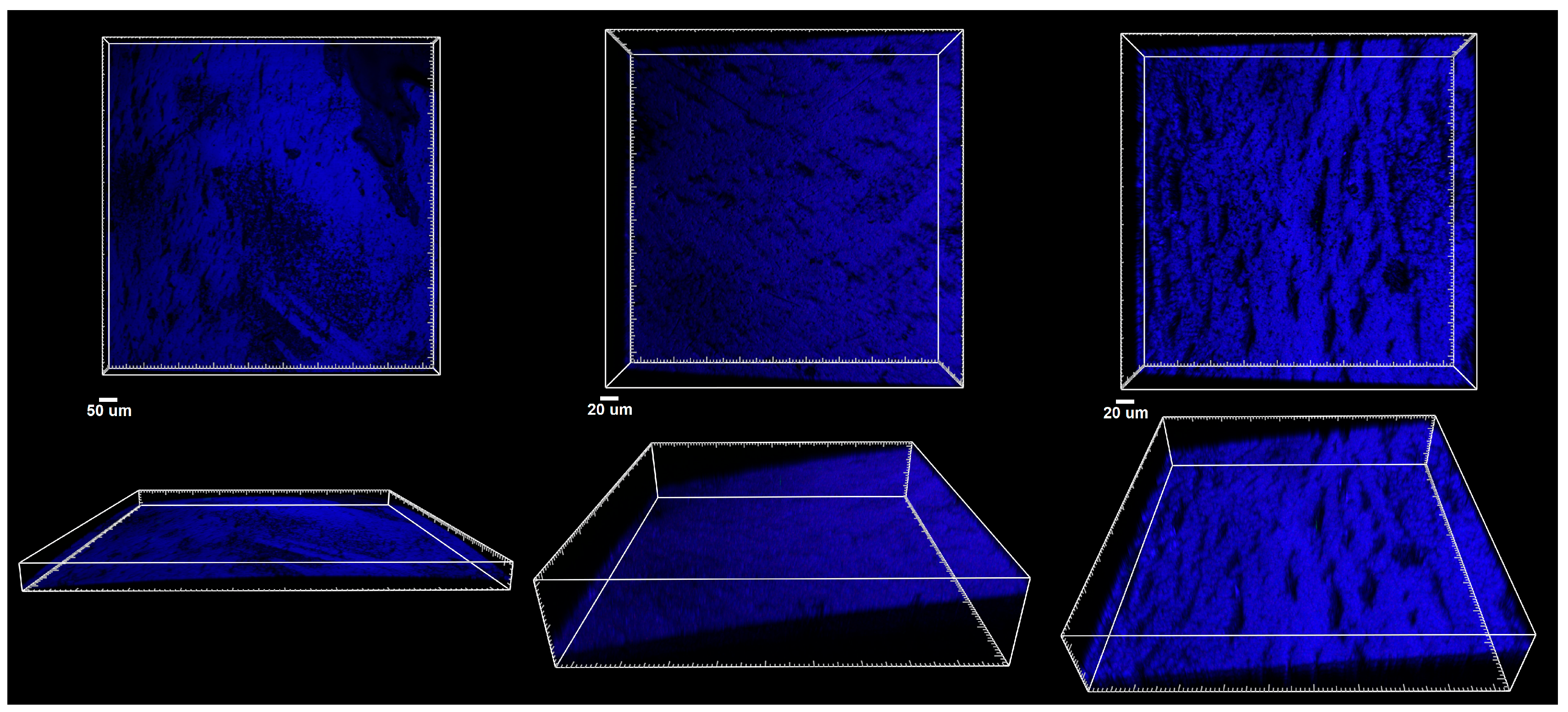
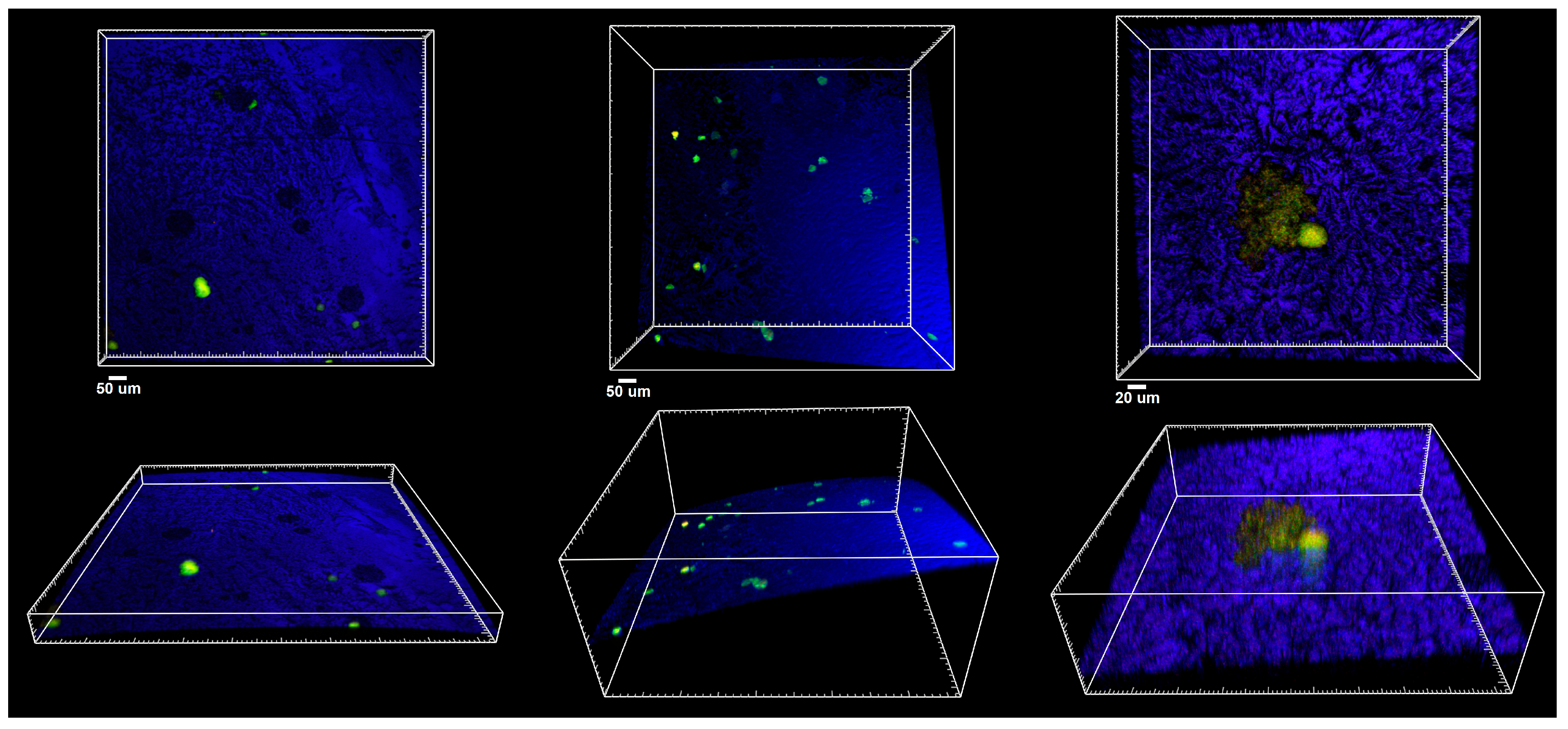
3.2. Microbiological Assay Results
3.3. Histology Assay Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ajayakumar, L.P.; Chowdhary, N.; Reddy, V.R.; Chowdhary, R. Use of Restorative Full Crowns Made with Zirconia in Children: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2020, 13, 551–558. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Planells Del Pozo, P.; Fuks, A. Zirconia crowns-an esthetic and resistant restorative alternative for ECC affected primary teeth. J. Clin. Pediatr. Dent. 2014, 38, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Salami, A.; Walia, T.; Bashiri, R. Comparison of parental satisfaction with three tooth-colored full-coronal restorations in primary maxillary incisors. J. Clin. Pediatr. Dent. 2015, 39, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Holsinger, D.M.; Wells, M.H.; Scarbecz, M.; Donaldson, M. Clinical evaluation and parental satisfaction with pediatric zirconia anterior crowns. Pediatr. Dent. 2016, 38, 192–198. [Google Scholar]
- Ashima, G.; Bhatia, S.K.; Gauba, K.; Mittal, H.C. Zirconia crowns for rehabilitation of decayed primary incisors: An Esthetic alternative. J. Clin. Pediatr. Dent. 2014, 39, 18–22. [Google Scholar] [CrossRef]
- Cohn, C. Zirconia-prefabricated crowns for pediatric patients with primary dentition: Technique and cementation for esthetic outcomes. Comp. Cont. Educ. Dent. 2016, 37, 554–558. [Google Scholar]
- Schmoeckel, J.; Gorseta, K.; Splieth, C.H.; Juric, H. How to intervene in the caries process: Early childhood caries—A systematic review. Caries Res. 2020, 54, 102–112. [Google Scholar] [CrossRef]
- An, S.Y.; Shim, Y.S.; Park, S.Y. Aesthetic rehabilitation in maxillary anterior tooth with early childhood caries using ZIRKIZ® crown: Long-term follow-up. Indian J. Sci. Technol. 2015, 8, 1–5. [Google Scholar] [CrossRef]
- Karaca, S.; Ozbay, G.; Kargul, B. Primary zirconia crown restorations for children with early childhood caries. Acta Stomatol. Croat. 2013, 47, 64–71. [Google Scholar] [CrossRef]
- Kara, N.B.; Yilmaz, Y. Assessment of oral hygiene and periodontal health around posterior primary molars after their restoration with various crown types. Int. J. Paediatr. Dent. 2013, 24, 303–313. [Google Scholar] [CrossRef]
- Manicone, P.F.; Iommetti, P.R.; Raffaelli, L. An overview of zirconia ceramics: Basic properties and clinical applications. J. Dent. 2007, 35, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Son, Y.H.; Han, C.H.; Kim, S. Influence of internal-gap width and cement type on the retentive force of zirconia copings in pullout testing. J. Dent. 2012, 40, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A. Esthetic zirconia crown in pedodontics. Int. J. Pedod. Rehabil. 2017, 2, 31–33. [Google Scholar] [CrossRef]
- Seminario, A.L.; Garcia, M.; Spiekerman, C.; Rajanbabu, P.; Donly, K.J.; Harbert, P. Survival of zirconia crowns in primary maxillary incisors at 12-, 24- and 36-month follow-up. Pediatr. Dent. 2019, 41, 385–390. [Google Scholar]
- Yanover, L.; Tickotsky, N.; Waggoner, W.; Kupietzky, A.; Moskovitz, M. Zirconia crown performance in primary maxillary anterior teeth: A retrospective photographic and radiographic cohort study. Eur. Arch. Paediatr. Dent. 2020, 22, 417–423. [Google Scholar] [CrossRef]
- Donly, K.J.; Sasa, I.; Contreras, C.I.; Mendez, M.J.C. Prospective randomized clinical trial of primary molar crowns: 36-month results. Am. J. Dent. 2020, 33, 165–168. [Google Scholar]
- Lee, J.H. Guided tooth preparation for a pediatric zirconia crown. J. Am. Dent. Assoc. 2018, 149, 202–208. [Google Scholar] [CrossRef]
- Sztyler, K.; Wiglusz, R.J.; Dobrzynski, M. Review on Preformed Crowns in Pediatric Dentistry—The Composition and Application. Materials 2022, 15, 2081. [Google Scholar] [CrossRef]
- Lee, J.-H. Case Report Guided tooth preparation for a pediatric zirconia crown. Orig. Contrib. Case Rep. 2018, 149, P202–P208.E2. [Google Scholar] [CrossRef]
- Ayad, M.F.; Maghrabi, A.A.; Rosenstiel, S.F. Assessment of convergence angles of tooth preparations for complete crowns among dental students. J. Dent. 2005, 33, 633–638. [Google Scholar] [CrossRef]
- Alrashdi, M.; Ardoin, J.; Liu, J.A. Zirconia crowns for children: A systematic review. Int. J. Paediatr. Dent. 2021, 66–81. [Google Scholar] [CrossRef] [PubMed]
- Walia, T.; Salami, A.A.; Bashiri, R.; Hamoodi, O.M.; Rashid, F. A randomised controlled trial of three aesthetic full-coronal restorations in primary maxillary teeth. Eur. J. Paediatr. Dent. 2014, 15, 113–118. [Google Scholar] [PubMed]
- Alhissan, A.S.; Pani, S.C. Factors Influencing the Survival of Preformed Zirconia Crowns in Children Treated under General Anesthesia. Int. J. Dent. 2021, 2021, 5515383. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef]
- A Townsend, J.; Knoell, P.; Yu, Q.; Zhang, J.-F.; Wang, Y.; Zhu, H.; Beattie, S.; Xu, X. In vitro fracture resistance of three commercially available zirconia crowns for primary molars. Pediatr. Dent. 2014, 36, 125–129. [Google Scholar]
- Choi, J.-W.; Bae, I.-H.; Noh, T.-H.; Ju, S.-W.; Lee, T.-K.; Ahn, J.-S.; Jeong, T.-S.; Huh, J.-B. Wear of primary teeth caused by opposed all ceramic or stainless steel crowns. J. Adv. Prosthodont. 2016, 8, 43–52. [Google Scholar] [CrossRef]
- Donly, K.J.; Sasa, I.; Contreras, C.I.; Mendez, M.J.C. Prospective randomized clinical trial of primary molar crowns: 24-month results. Pediatr. Dent. 2018, 40, 253–258. [Google Scholar]
- Mathew, M.G.; Samuel, S.R.; Soni, A.J.; Roopa, K.B. Evaluation of adhesion of Streptococcus mutans, plaque accumulation on zirconia and stainless steel crowns, and surrounding gingival inflammation in primary molars: Randomized controlled trial. Clin. Oral Investig. 2020, 24, 3275–3280. [Google Scholar] [CrossRef]
- EN 13060; Small Steam Sterilizers. Available online: https://standards.iteh.ai/catalog/standards/cen/c427dd54-2927-4833-a160-f6730b5cec2f/en-13060-2014a1-2018?srsltid=AfmBOoqfWSU1pH5dZi1m8ivPxxVW8xUGsm7PekWTdO805w_MbbNdMUHq (accessed on 7 May 2025).
- Dobrzynski, M.; Pajaczkowska, M.; Nowicka, J.; Jaworski, A.; Kosior, P.; Szymonowicz, M.; Kuropka, P.; Rybak, Z.; Bogucki, Z.A.; Filipiak, J.; et al. Study of Surface Structure Changes for Selected Ceramics Used in the CAD/CAM System on the Degree of Microbial Colonization. Vitr. Tests BioMed Res. Int. 2019, 2019, 9130806. [Google Scholar] [CrossRef]
- Sztyler, K.; Pajączkowska, M.; Nowicka, J.; Rusak, A.; Chodaczek, G.; Nikodem, A.; Wiglusz, R.J.; Watras, A.; Dobrzyński, M. Evaluation of the microbial, cytotoxic and physico-chemical properties of the stainless steel crowns used in pediatric dentistry. Acta Bioeng. Biomech. 2022, 24, 127–137. [Google Scholar] [CrossRef]
- Reśliński, A.; Mikucka, A.; Szmytkowski, J.; Głowacka, K.; Szczęsny, W.; Gospodarek, E.; Dąbrowiecki, S. Biofilm Detection on the Surface of Hernia Mesh Implants. Adv. Clin. Exp. Med. 2010, 19, 685–690. [Google Scholar]
- ISO 10993-12; Biological Evaluation of Medical Devices—Part 12: Sample Preparation and Reference Materials. ISO: Geneva, Switzerland, 2021.
- ISO 10993-5; Biological Evaluation of Medical Devices—Part 5: Tests for In Vitro Cytotoxicity. ISO: Geneva, Switzerland, 2009.
- Solis-Velazquez, O.A.; Gutiérrez-Lomelí, M.; Guerreo-Medina, P.J.; Rosas-García, M.L.; Iñiguez-Moreno, M.; Avila-Novoa, M.G. Nosocomial pathogen biofilms on biomaterials: Different growth medium conditions and components of biofilms produced in vitro. J. Microbiol. Immunol. Infect. 2020, 54, 1038–1047. [Google Scholar] [CrossRef]
- El Aouame, A.; El Quars, F.; Bentahar, Z.; Zerouali, K.; Sidqui, M. In Vitro Evaluation of Bacterial Adhesion to Dental and Stainless-Steel Surfaces. Open J. Med. Microbiol. 2021, 11, 176–197. [Google Scholar] [CrossRef]
- Gheorghe, D.C.; Niculescu, A.G.; Bîrcă, A.C.; Grumezescu, A.M. Biomaterials for the Prevention of Oral Candidiasis Development. Pharmaceutics 2021, 13, 803. [Google Scholar] [CrossRef] [PubMed]
- Sterzenbach, T.; Helbig, R.; Hannig, C.; Hannig, M. Bioadhesion in the oral cavity and approaches for biofilm management by surface modifications. Clin. Oral Investig. 2020, 24, 4237–4260. [Google Scholar] [CrossRef]
- Bigos, P.; Czerwińska, R.; Pajączkowska, M.; JNowicka, J. Mixed Oral Biofilm. Postępy Mikrobiol. Adv. Microbiol. 2021, 60, 47–58. [Google Scholar] [CrossRef]
- Marsh, P.D.; Zaura, E. Dental biofilm: Ecological interactions in health and disease. J. Clin. Periodontol. 2017, 44, S12–S22. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, S.B. Oral Biofilms. Int. J. Curr. Microbiol. Appl. Sci. 2018, 7, 643–652. [Google Scholar] [CrossRef]
- Cavalcanti, I.M.; Cury, A.A.D.B.; Jenkinson, H.F.; Nobbs, A.H. Interactions between Streptococcus oralis, Actinomyces oris, and Candida albicans in the development of multispecies oral microbial biofilms on salivary pellicle. Mol. Oral Microbiol. 2017, 32, 60–73. [Google Scholar] [CrossRef]
- Larsen, T.; Fiehn, N.E. Dental biofilm infections—An update. APMIS 2017, 125, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Deng, S.; Wang, Y.; Lin, X.; Yang, Z. Adhesive Ability of Different Oral Pathogens to Various Dental Materials: An In Vitro Study. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 9595067. [Google Scholar] [CrossRef]
- Huffines, J.T.; Scoffield, J.A. Disruption of Streptococcus mutans and Candida albicans synergy by a commensal streptococcus. Sci. Rep. 2020, 10, 19661. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Huang, X.; Zhou, X.; Li, M.; Ren, B.; Peng, X.; Cheng, L. Influence of Dental Prosthesis and Restorative Materials Interface on Oral Biofilms. Int. J. Mol. Sci. 2018, 19, 3157. [Google Scholar] [CrossRef]
- Kreth, J.; Merritt, J.; Pfeifer, C.S.; Khajotia, S.; Ferracane, J.L. Interaction between the Oral Microbiome and Dental Composite Biomaterials: Where We Are and Where We Should Go. J. Dent. Res. 2020, 99, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Cenci, T.; Deng, D.M.; Kraneveld, E.A.; Manders, E.M.M.; Cury, A.A.D.B.; Cate, J.M.T.; Crielaard, W. The effect of Streptococcus mutans and Candida glabrata on Candida albicans biofilms formed on different surfaces. Arch. Oral Biol. 2008, 53, 755–764. [Google Scholar] [CrossRef]
- Diaz, P.I.; Strausbaugh, L.D.; Dongari-Bagtzoglou, A. Fungal-bacterial interactions and their relevance to oral health: Linking the clinic and the bench. Front. Cell. Infect. Microbiol. 2014, 4, 101. [Google Scholar] [CrossRef]
- Salehi, B.; Kregiel, D.; Mahady, G.; Sharifi-Rad, J.; Martins, N.; Rodrigues, C.F. Management of Streptococcus mutans-Candida spp. Oral Biofilms’ Infections: Paving the Way for Effective Clinical Interventions. J. Clin. Med. 2020, 9, 517. [Google Scholar] [CrossRef]
- Lin, Y.-T.J.; Chou, C.-C.; Hsu, C.-Y.S. Effects of Lactobacillus Casei Shirota Intake on Caries Risk in Children. J. Dent. Sci. 2017, 12, 179–184. [Google Scholar] [CrossRef]
- Schwendicke, F.; Dörfer, C.; Kneist, S.; Meyer-Lueckel, H.; Paris, S. Cariogenic effects of probiotic lactobacillus rhamnosus GG in a dental biofilm model. Caries Res. 2014, 48, 186–192. [Google Scholar] [CrossRef]
- Murali, G.; Mungara, J.; Vijayakumar, P.; Keerthi, T.; Kothimbakkam, S.S.K.; Priya, A.S. Clinical Evaluation of Pediatric Posterior Zirconia and Stainless Steel Crowns: A Comparative Study. Int. J. Clin. Pediatr. Dent. 2022, 15, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.I.; Hajwal, S.I.; Ab-Ghani, Z. Bacterial Adhesion on Zirconia, Lithium Desilicated and Gold Crowns-In Vivo Study. Adv. Dent. Oral Health 2016, 1, 555574. [Google Scholar] [CrossRef]
- Gupta, S.; Khanduja, R.; Agrawal, R.; Singhal, M.; Kaushik, M. Clinical Evaluation of Stainless Steel Crown versus Zirconia Crown in Primary Molars: An In Vivo Study. Int. J. Clin. Pediatr. Dent. 2022, 15, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Singh, A.; Sahoo, S.S.; Singh, C.; Mukhopadhyaya, I.; Joshi, A. Effect of pre-fabricated strip, zirconia and stainless steel crowns in primary molars. Bioinformation 2023, 19, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Nikhil, D.K.R.; H, K.S.; Savitha, S.; Allwin, A.; Nandan, S. Clinical Evaluation of Zirconia and Stainless-Steel crowns in Primary Molars—A Randomized Control Trial: Original Research. Int. J. Pedod. Rehabil. 2022, 7, 30–38. [Google Scholar] [CrossRef]
- Wakwak, M.A.; Bayoumy, S.Y.; Barakat, I.F.; Tawfik, A. Assessment of microbial adhesion to zirconia and stainless-steel crowns in primary molars. Al-Azhar J. Dent. Sci. 2019, 2, 165–169. [Google Scholar]
- Paulindraraj, S.; Ramkumar, H.; Jayakaran, T.G.; Dakshinamurthy, S.; Elizabeth, J.A.; Manoharan, R. Evaluation of Streptococcus mutans Colonization and Oral Hygiene Status in Primary Molars Restored with Two Different Crowns: A Randomized Clinical Trial. Int. J. Clin. Pediatr. Dent. 2023, 16 (Suppl. S2), S183–S189. [Google Scholar] [CrossRef]
- Alaki, S.M.; Abdulhadi, B.S.; AbdElBaki, M.A.; Alamoudi, N.M. Comparing zirconia to anterior strip crowns in primary anterior teeth in children: A randomized clinical trial. BMC Oral Health 2020, 20, 313. [Google Scholar] [CrossRef]
- Kaczmarek, K.; Konieczny, B.; Siarkiewicz, P.; Leniart, A.; Lukomska-Szymanska, M.; Skrzypek, S.; Lapinska, B. Surface Characterization of Current Dental Ceramics Using Scanning Electron Microscopic and Atomic Force Microscopic Techniques. Coatings 2022, 12, 1122. [Google Scholar] [CrossRef]
- Teughels, W.; Van Assche, N.; Sliepen, I.; Quirynen, M. Effect of material characteristics and/or surface topography on biofilm development. Clin. Oral Implants Res. 2006, 17, 68–81. [Google Scholar] [CrossRef]
- Rashid, H. The effect of surface roughness on ceramics used in dentistry: A review of literature. Eur. J. Dent. 2014, 08, 571–579. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rani, V.; Mittal, S.; Sukhija, U. An In vitro Evaluation to Compare the Surface Roughness of Glazed, Reglazed and Chair Side Polished Surfaces of Dental Porcelain. Contemp. Clin. Dent. 2021, 12, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Liber-Kneć, A.; Łagan, S. Surface Testing of Dental Biomaterials-Determination of Contact Angle and Surface Free Energy. Materials 2021, 14, 2716. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Cytotoxicity | Description of Colony Changes |
|---|---|---|
| 0 | None | No changes in both the surroundings of the material and under the material |
| 1 | Low | Individual cells have become degenerated or deformed under the influence of the material |
| 2 | Average | The zone of affected cells is limited to the area under the material |
| 3 | Medium | The zone of affected cells is limited to 1 cm around the material |
| 4 | High | Zone of affected cells exceeds the limit of 1 cm around the material |
| Parameters of Linear Roughness | |||
| Anterior surface | Posterior surface | ||
| Ra [nm] | 50.66 ± 7.48 | Ra [nm] | 115.19 ± 20.31 |
| Rq [nm] | 68.23 ± 11.17 | Rq [nm] | 150.19 ± 27.79 |
| Rz [nm] | 366.73 ± 83.59 | Rz [nm] | 779.89 ± 146.97 |
| Parameters of Surface Roughness | |||
| Anterior surface | Posterior surface | ||
| Sa [nm] | 29.18 ± 5.95 | Sa [nm] | 66.05 ± 5.05 |
| Sq [nm] | 41.47 ± 8.45 | Sq [nm] | 86.23 ± 6.12 |
| Sz [nm] | 1407.65 ± 917.73 | Sz [nm] | 1319.87 ± 161.49 |
| Sp [nm] | 698.25 ± 540.04 | Sp [nm] | 568.91 ± 95.04 |
| Sv [nm] | 709.19 ± 390.53 | Sv [nm] | 750.96 ± 93.62 |
| Water Contact Angle | |||
| θC [°] | 66.575 ± 2.65 | 75.95 ± 3.64 | |
| Mixed Microbial Suspension | C. albicans 28 | S. mutans | L. rhamnosus | |||
|---|---|---|---|---|---|---|
| I | II | I | II | I | II | |
| CFU/mL | 5.99 × 105 | 6.51 × 105 | 5.40 × 106 | 5.10 × 106 | 4.1 × 107 | 2.7 × 107 |
| Mean ± SD | 6.25 × 105 ± 3.67 × 104 | 5.25 × 106 ± 3.45 × 107 | 3.4 × 107 ± 9.89 × 106 | |||
| Mixed microbial suspension | C. albicans 31 | S. mutans | L. rhamnosus | |||
| I | II | I | II | I | II | |
| CFU/mL | 1.0 × 106 | 1.1 × 106 | 6.8 × 106 | 9.2 × 106 | 3.05 × 107 | 3.25 × 107 |
| Mean ± SD | 1.05 × 106 ± 7.07 × 104 | 8 × 106 ± 1.69 × 106 | 3.15 × 107 ± 1.41 × 106 | |||
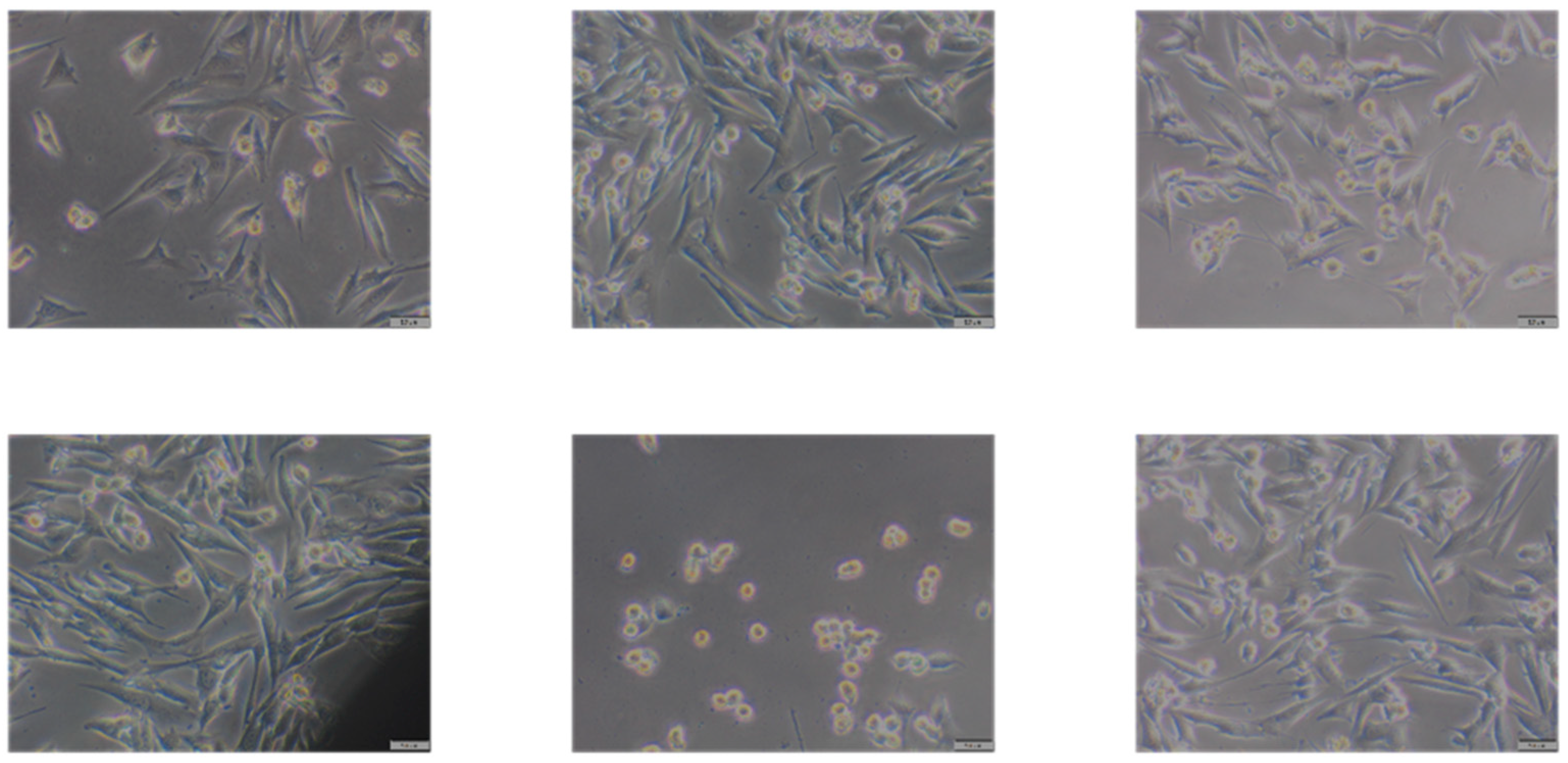
| Material | Sample Number | Description of Morphological Changes in Cell Culture | Evaluation of Changes in Cell Culture | Cytotoxicity |
|---|---|---|---|---|
| Zirconia Pediatric preformed crown | 1 | Changes in the morphology of the cells with the tested material (rounded cells, shrunken cells, stunted growth of the culture); near the sample up to 1 cm and in the rest of the culture, cell morphology normal | 2 | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sztyler, K.; Pajączkowska, M.; Nowicka, J.; Rusak, A.; Chodaczek, G.; Dubniański, Ł.; Nikodem, A.; Wiglusz, R.J.; Watras, A.; Dobrzyński, M. Assessment of the Physico-Chemical, Microbial, and Cytotoxic Characteristics of Zirconia Crowns Utilized in Pediatric Dentistry. Appl. Sci. 2025, 15, 5444. https://doi.org/10.3390/app15105444
Sztyler K, Pajączkowska M, Nowicka J, Rusak A, Chodaczek G, Dubniański Ł, Nikodem A, Wiglusz RJ, Watras A, Dobrzyński M. Assessment of the Physico-Chemical, Microbial, and Cytotoxic Characteristics of Zirconia Crowns Utilized in Pediatric Dentistry. Applied Sciences. 2025; 15(10):5444. https://doi.org/10.3390/app15105444
Chicago/Turabian StyleSztyler, Klaudia, Magdalena Pajączkowska, Joanna Nowicka, Agnieszka Rusak, Grzegorz Chodaczek, Łukasz Dubniański, Anna Nikodem, Rafal J. Wiglusz, Adam Watras, and Maciej Dobrzyński. 2025. "Assessment of the Physico-Chemical, Microbial, and Cytotoxic Characteristics of Zirconia Crowns Utilized in Pediatric Dentistry" Applied Sciences 15, no. 10: 5444. https://doi.org/10.3390/app15105444
APA StyleSztyler, K., Pajączkowska, M., Nowicka, J., Rusak, A., Chodaczek, G., Dubniański, Ł., Nikodem, A., Wiglusz, R. J., Watras, A., & Dobrzyński, M. (2025). Assessment of the Physico-Chemical, Microbial, and Cytotoxic Characteristics of Zirconia Crowns Utilized in Pediatric Dentistry. Applied Sciences, 15(10), 5444. https://doi.org/10.3390/app15105444