
Effects of Systemic and Local Vibration Therapies on the Functional Capacity of Knee Osteoarthritis Individuals: A Systematic Review of Randomized Clinical Trials

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Material and Methods
2.1. Protocol and Registration
2.2. Research Question
2.3. Eligibility Criteria
2.4. Search Strategies
2.5. Data Extraction
2.6. Methodological Quality and Risk of Bias
3. Results
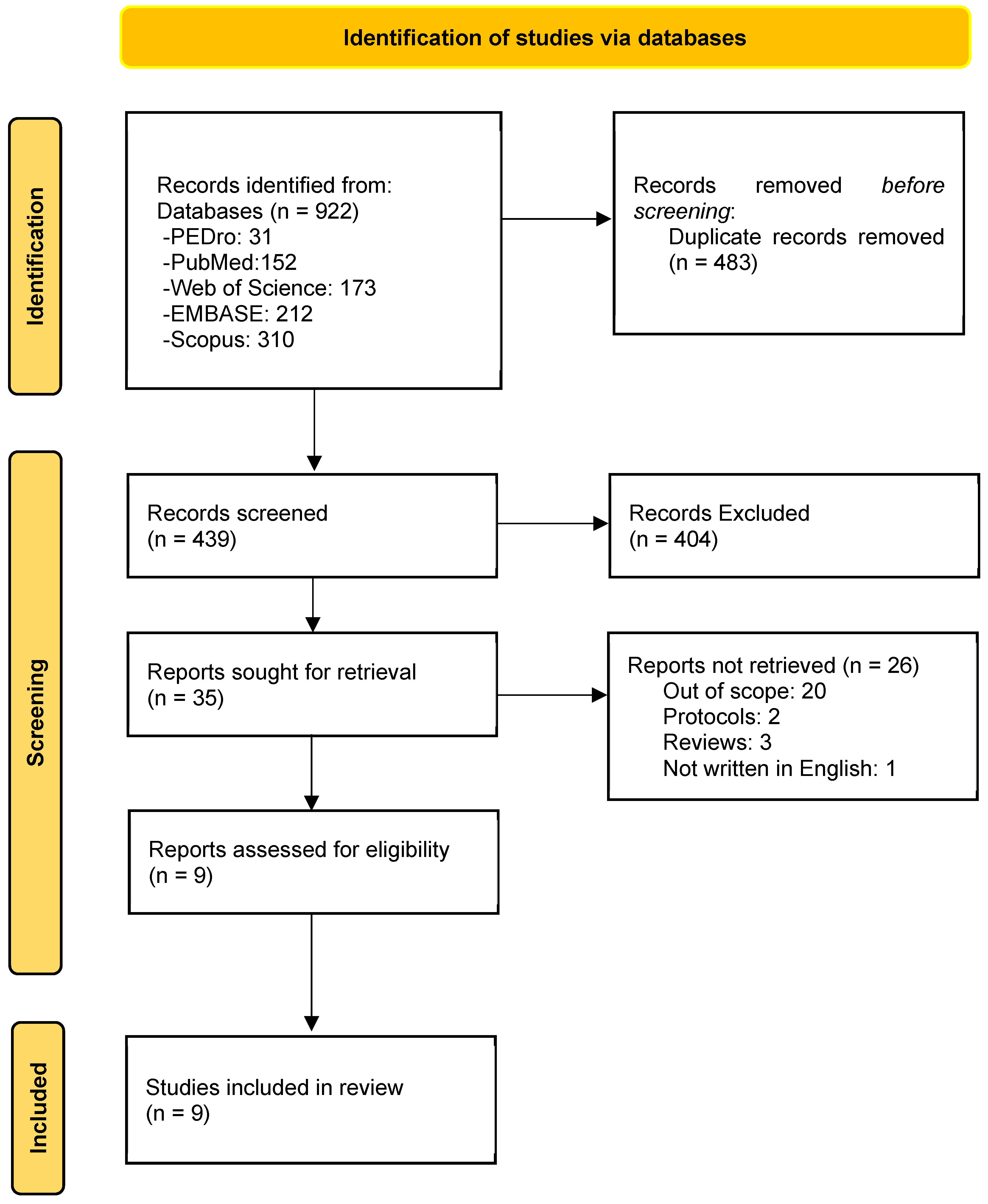
3.1. Search Results
3.2. Studies Characteristics

{kind=link}
{kind=link}
{kind=link}
| Authors/Year/Country | Participants/Groups/Mean Age (Years) | BMI (kg/m2–Mean ± SD) | Aim | Vibration Device | Exposure Variable | Period (Days) Bouts/Rest Time | Tools Used to Assess the Functional Capacity |
|---|---|---|---|---|---|---|---|
| Trans et al., 2009. [31] Denmark. | N: 52 Female WBVG: 61.5 ± 9.2 WBVBG: 58.7 ± 11 CG: 61.1 ± 8.5 | WBVG 29.2 ± 6.1 WBVBG 29.1 ± 5.8 CG 30.2 ± 5.4 | To verify the WBV exercise on muscle strength and proprioception. | Xendon® platform VibM, Sweden. Side-Alternating | f: 25 to 30 Hz A: n/d aPeak: n/d | 8 weeks (2 days) 6 to 9 bouts: 30 s to 70 s/bout Rest: 30 s to 70 s | Isokinetic dynamometry TDPM WOMAC |
| Abbasi et al., 2017. [40] Iran. | N: 37 Male and Female WBVG: 63.6 ± 3 Placebo group: 68 ± 2.1 CG: 63.5 ± 4.8 | WBVG: 28.4 ± 2.4 Placebo group: 29.8 ± 2 CG: 29.7 ± 1.8 | To determine whether WBV is effective on electromyographic activity of the muscles of the lower limbs in KOA individuals. | Fitvibe® Gymna Uniphy NV, Bilzen, Belgium Vertical Vibration | f: 30 Hz A: 3 mm aPeak: 5.3 g | 4 weeks (3 days) 6 to 15 bouts: 1 min/bout Rest: 1 min | sEMG |
| Moreira-Marconi et al., 2020. [34] Brazil. | N: 19 Male and Female WBVG: 64.1 ± 8.5 CG: 66.8 ± 8.5 | WBVG: 34.9 ± 8.6 CG: 33.7 ± 6.9 | To evaluate the effectiveness of WBV on the functionality of lower limbs by the electromyographic profile of the vastus lateralis muscles during the 5CST in KOA individuals. | Novaplate® Fitness Evolution, São Paulo, Brazil. Side-alternating | f: 5 to 14 Hz A: 1.25, 2.5, 3.75 mm aPeak: 0.12 to 2.95 g | 5 weeks (2 days) 3 bouts: 3 min/bout Rest: 1 min | 5CST sEMG |
| Moura-Fernandes et al., 2020. [39] Brazil. | N: 37 Male and Female WBVG: 62.3 ± 2.5 CG: 68 ± 2 | WBVG: 34.7 ± 2.1 CG: 31.7 ± 1.2 | To analyze the acute effects of WBV exercise on pain levels, functionality, and rating of exertion of elderly obese KOA individuals. | Nova Plate® Fitness Evolution, São Paulo, Brazil. Side-alternating | f: 5 to 14 Hz A: 1.25, 2.5, 3.75 mm aPeak: 0.12, 0.25, and 0.37 g | 1 Day 3 bouts: 3 min/bout Rest: 1 min | ODI Lequesne’s Functional Index TUG BORG scale ATF |
| Lai et al., 2021. [41] China. | N: 81 Male and Female WBVG: 63.5 ± 4.9 Health Education: 63.6 ± 4.8 Strength Training: 64.8 ± 4 | WBVG: 24.2 ± 2.7 Health Education: 23.4 ± 2.9 Strength Training: 23 ± 2.9 | To investigate the therapeutic effect of WBV training on the neuromuscular function of KOA individuals. | i-vib5050® Sport Platform, China. Vertical vibration | f: 20 Hz A: 2 mm aPeak: 1.6 g | 8 weeks (3 day) 6 to 15 bouts: 30 s to 1 min/bout Rest: 30 s to 60 s | TUG 6MWD |
| Authors/Year Country | Participants/Groups/Mean Age (Years) | BMI (kg/m2–Mean ± SD) | Aim | Vibration Device | Exposure Variable | Period (Days) Bouts Rest Time | Tools Used to Assess the Functional Capacity |
|---|---|---|---|---|---|---|---|
| Rabini et al., 2015. [14] Italy. | N: 50 Male and Female LVTG: 73.7 ± 5.2 CG: 75 ± 5.7 | LVTG: >30 CG: >30 | To evaluate the effects of local muscle vibration on physical functioning in patients with symptomatic KOA. | -Cro®System, NEMOCO srl, Italy (device) | f: 100 Hz A: 0.2–0.5 mm aPeak: 20.4 to 81.6 g | 3 consecutive days. 3 bouts 10 min/ bout rest: 1 min | WOMAC SPPB POMA |
| Benedetti et al., 2017 [13] Italy. | N: 30 Male and Female LVTG: 61.8 ± 5.8 NMES: 55.7 ± 9.1 | LVTG: 26.1 ± 2.9 NMES: 26 ± 2.8 | To investigate the clinical effectiveness of high-frequency LVT on quadriceps muscle in patients with KOA and to disentangle, by means of surface electromyography (sEMG). | -Pneumatic vibrator powered by compressed air (Vibra Plus; A Circle s.p.a). | f: 150 Hz A: N/R aPeak: N/R | -2 weeks (5 days) 1 bout -20 min/bout -rest: 0 min | WOMAC ROM TUG Stair Climbing Test sEMG |
| Pasterczyk-Szczurek et al., 2023. [32] Poland. | N: 32 Male and Female LVTG: 63.6 ± 7.6 CG: 64.8 ± 10.8 | LVTG: 31 ± 5.6 CG: 31.3 ± 5.5 | To determine the impact of vibrations of variable frequency and low amplitude on pain perception and mobility in patients suffering from KOA. | -RAM Vitberg© Base Module and Vitberg© Knee Module. | f: 5–50 Hz A: 0–0.2 mm aPeak: 1.38 g | -3 weeks (5 days). 1 bout: 60 min/bout rest: N/R. | TUG KOOS questionnaire ROM sEMG |
| Barati et al., 2023. [33] Iran. | N: 14 Female Vibratory orthosis group: 55.6 ± 3.7 Conventional orthosis group: 57.2 ± 3.8 | Vibratory orthosis group: 20.2 ± 2.2 Conventional orthosis group: 21.3 ± 2.1 | To determine whether equipping an unloader knee orthosis with vibrators improves its effectiveness in pain, stiffness, function, and reducing the moment of knee adduction. | -Vibratory unloader knee orthosis. | f: 30 Hz A: 1.6 mm aPeak: 5.8 g | -6 weeks (5 h for week). -300 min/week rest: N/R. | WOMAC 6 camera Qualisys motion capture system |
3.3. Main Findings Related to the Functional Capacity
3.4. Findings Related to Pain
3.5. Methodological Quality
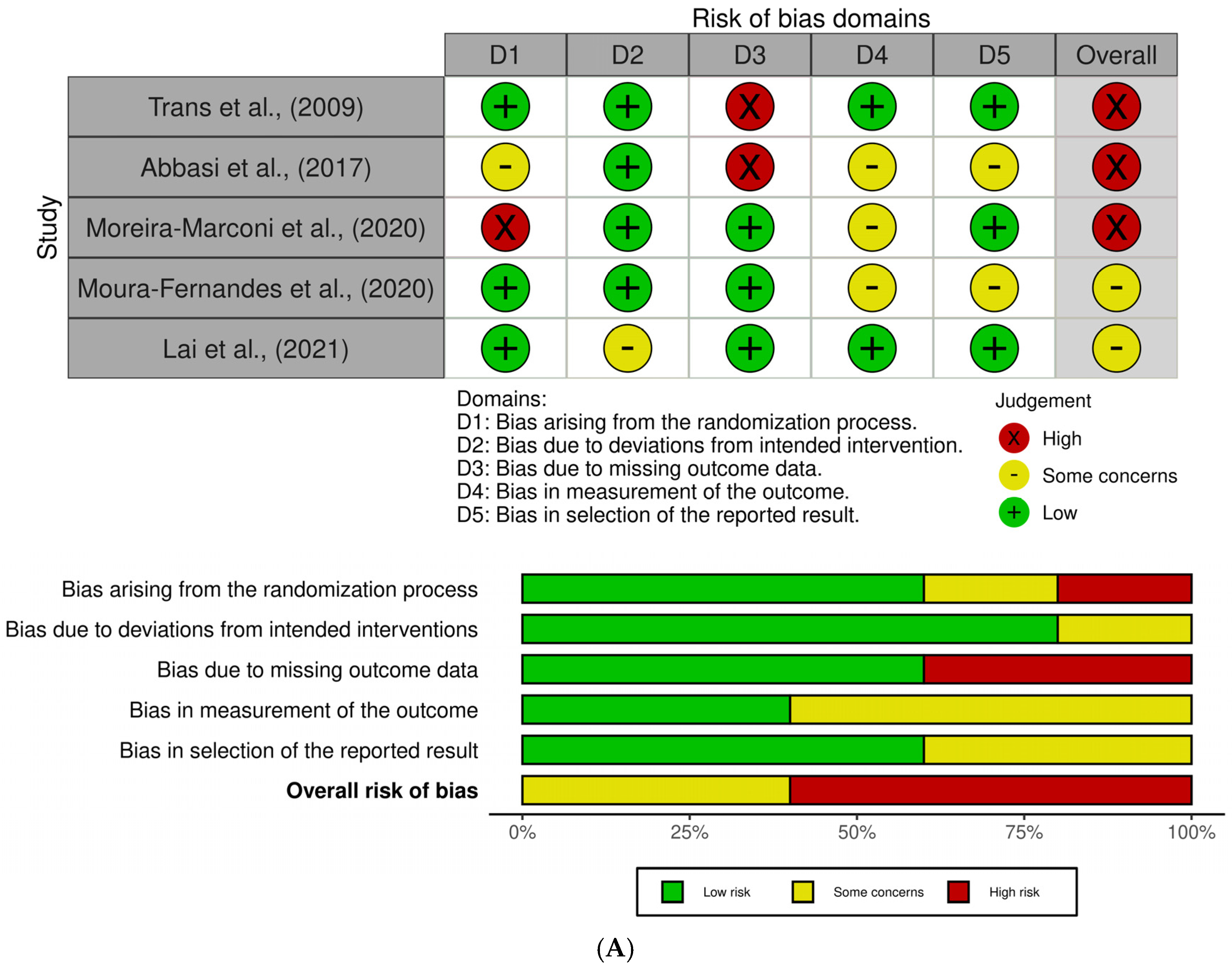
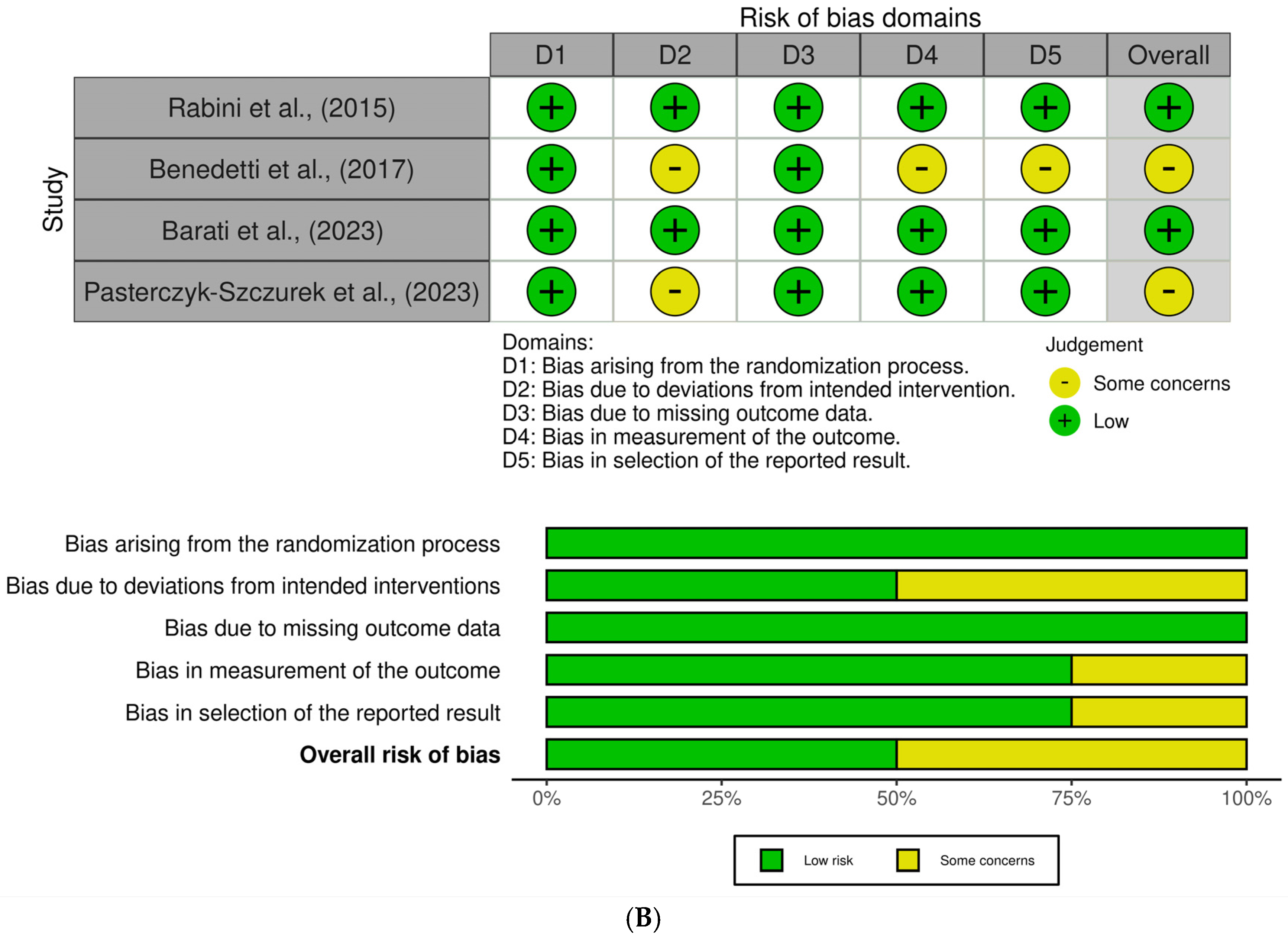
3.6. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bonanni, R.; Cariati, I.; Romagnoli, C.; D’arcangelo, G.; Annino, G.; Tancredi, V. Whole body vibration: A valid alternative strategy to exercise? J. Funct. Morphol. Kinesiol. 2022, 7, 99. [Google Scholar] [CrossRef] [PubMed]
- Kalaoglu, E.; Bucak, O.F.; Kokce, M.; Ozkan, M.; Cetin, M.; Atasoy, M.; Ayture, L.; Karacan, I. Whole body vibration activates the tonic vibration reflex during voluntary contraction. J. Phys. Ther. Sci. 2023, 35, 408–413. [Google Scholar] [CrossRef]
- Cochrane, D.J. Vibration exercise: The potential benefits. Int. J. Sports Med. 2011, 32, 75–99. [Google Scholar] [CrossRef]
- Cardinale, M.; Wakeling, J. Whole body vibration exercise: Are vibrations good for you? Br. J. Sports Med. 2005, 39, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Sá-Caputo, D.C.; Seixas, A.; Taiar, R.; Bernardo-Filho, M. Vibration Therapy for Health Promotion. Complement. Ther. 2022, 1, 213. [Google Scholar] [CrossRef]
- Oroszi, T.; van Heuvelen, M.J.; Nyakas, C.; van der Zee, E.A. Vibration detection: Its function and recent advances in medical applications. F1000Research 2020, 9, 619. [Google Scholar] [CrossRef]
- Chang, W.-D.; Chen, S.; Tsou, Y.-A. Effects of whole-body vibration and balance training on female athletes with chronic ankle instability. J. Clin. Med. 2021, 10, 2380. [Google Scholar] [CrossRef]
- Souron, R.; Besson, T.; Millet, G.Y.; Lapole, T. Acute and chronic neuromuscular adaptations to local vibration training. Eur. J. Appl. Physiol. 2017, 117, 1939–1964. [Google Scholar] [CrossRef]
- Pujari, A.N.; Neilson, R.D.; Cardinale, M. Effects of different vibration frequencies, amplitudes and contraction levels on lower limb muscles during graded isometric contractions superimposed on whole body vibration stimulation. J. Rehabil. Assist. Technol. Eng. 2019, 6, 2055668319827466. [Google Scholar] [CrossRef]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef]
- Paineiras-Domingos, L.L.; Guedes-Aguiar, E.O.; Monteiro-Oliveira, B.B.; Torres-Nunes, L.; de Souza, L.F.F.; Paiva, D.N.; Sá-Caputo, D.C.; Taiar, R.; Bernardo-Filho, M. Whole-body vibration exercises improving the functionality of the Chronic Obstructive Pulmonary Disease individuals: A quasi-experimental non-randomized clinical trial comparing two different postures. BJMVB 2024, 2, 13–23. [Google Scholar]
- Wu, S.; Ning, H.-T.; Xiao, S.-M.; Hu, M.-Y.; Wu, X.-Y.; Deng, H.-W.; Feng, H. Effects of vibration therapy on muscle mass, muscle strength and physical function in older adults with sarcopenia: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Boccia, G.; Cavazzuti, L.; Magnani, E.; Mariani, E.; Rainoldi, A.; Casale, R. Localized muscle vibration reverses quadriceps muscle hypotrophy and improves physical function: A clinical and electrophysiological study. Int. J. Rehabil. Res. 2017, 40, 339–346. [Google Scholar] [CrossRef]
- Rabini, A.; De Sire, A.; Marzetti, E.; Gimigliano, R.; Ferriero, G.; Piazzini, D.B.; Gimigliano, F. Effects of focal muscle vibration on physical functioning in patients with knee osteoarthritis: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 513–520. [Google Scholar] [PubMed]
- van Heuvelen, M.J.G.; Rittweger, J.; Judex, S.; Sañudo, B.; Seixas, A.; Fuermaier, A.B.M.; Tucha, O.; Nyakas, C.; Marín, P.J.; Taiar, R.; et al. Reporting Guidelines for Whole-Body Vibration Studies in Humans, Animals and Cell Cultures: A Consensus Statement from an International Group of Experts. Biology 2021, 10, 965. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef]
- Giorgino, R.; Albano, D.; Fusco, S.; Peretti, G.M.; Mangiavini, L.; Messina, C. Knee Osteoarthritis: Epidemiology, Pathogenesis, and Mesenchymal Stem Cells: What Else Is New? An Update. Int. J. Mol. Sci. 2023, 24, 6405. [Google Scholar] [CrossRef]
- Alcalde, G.E.; Fonseca, A.C.; Bôscoa, T.F.; Gonçalves, M.R.; Bernardo, G.C.; Pianna, B.; Carnavale, B.F.; Gimenes, C.; Barrile, S.R.; Arca, E.A. Effect of aquatic physical therapy on pain perception, functional capacity and quality of life in older people with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2017, 18, 317. [Google Scholar] [CrossRef]
- Yang, G.; Wang, J.; Liu, Y.; Lu, H.; He, L.; Ma, C.; Zhao, Z. Burden of Knee Osteoarthritis in 204 Countries and Territories, 1990–2019: Results from the Global Burden of Disease Study 2019. Arthritis Care Res. 2023, 75, 2489–2500. [Google Scholar] [CrossRef]
- Heidari, M.B. Knee osteoarthritis prevalence, risk factors, pathogenesis and feature part I. Casp. J. Intern. Med. 2011, 2, 205–212. [Google Scholar]
- Quicke, J.; Conaghan, P.; Corp, N.; Peat, G. Osteoarthritis year in review 2021: Epidemiology & therapy. Osteoarthr. Cartil. 2022, 30, 196–206. [Google Scholar] [CrossRef]
- Caiado, V.S.; Santos, A.C.G.; Moreira-Marconi, E.; Moura-Fernandes, M.C.; Seixas, A.; Taiar, R.; Lacerda, A.C.R.; Sonza, A.; Mendonça, V.A.; Sá-Caputo, D.C.; et al. Effects of Physical Exercises Alone on the Functional Capacity of Individuals with Obesity and Knee Osteo-arthritis: A Systematic Review. Biology 2022, 11, 1391. [Google Scholar] [CrossRef]
- Yeoh, P.S.Q.; Lai, K.W.; Goh, S.L.; Hasikin, K.; Hum, Y.C.; Tee, Y.K.; Dhanalakshmi, S. Emergence of Deep Learning in Knee Osteoarthritis Diagnosis. Comput. Intell. Neurosci. 2021, 1, 4931437. [Google Scholar] [CrossRef] [PubMed]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef]
- Pedersen, M.M.; Mongelard, K.B.G.; Mørup-Petersen, A.; Christensen, K.B.; Odgaard, A. Clinicians’ heuristic assessments of radiographs compared with Kellgren-Lawrence and Ahlbäck ordinal grading: An exploratory study of knee radiographs using paired comparisons. BMJ Open 2021, 11, e041793. [Google Scholar] [CrossRef] [PubMed]
- Lespasio, M.J.; Piuzzi, N.S.; Husni, M.E.; Muschler, G.F.; Guarino, A.; Mont, M.A. Knee Osteoarthritis: A Primer. Perm. J. 2017, 21, 16–183. [Google Scholar] [CrossRef]
- Wolf, D.F.; Carvalho, C.; Padovez, R.d.F.C.M.; de Oliveira, M.P.B.; Serrão, P.R.M.d.S. Effects of physical exercise on muscle function of the knee, pain and quality of life in postmenopausal women with knee osteoarthritis: A systematic review with meta-analysis. Musculoskelet. Sci. Pr. 2024, 71, 102929. [Google Scholar] [CrossRef]
- Mood, A.C.; Justine, M.; A Bukry, S.; Mohan, V. The association of fatigue severity with pain level, obesity indices and functional performances in women with knee osteoarthritis. Med. J. Malays. 2024, 79, 1–7. [Google Scholar]
- Dantas, L.O.; Salvini, T.d.F.; McAlindon, T.E. Knee osteoarthritis: Key treatments and implications for physical therapy. Braz. J. Phys. Ther. 2021, 25, 135–146. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Trans, T.; Aaboe, J.; Henriksen, M.; Christensen, R.; Bliddal, H.; Lund, H. Effect of whole body vibration exercise on muscle strength and proprioception in females with knee osteoarthritis. Knee 2009, 16, 256–261. [Google Scholar] [CrossRef]
- Pasterczyk-Szczurek, A.; Golec, J.; Golec, E. Effect of low-magnitude, variable-frequency vibration therapy on pain threshold levels and mobility in adults with moderate knee osteoarthritis—Randomized controlled trial. BMC Musculoskelet. Disord. 2023, 24, 1–9. [Google Scholar] [CrossRef]
- Barati, K.; Kamyab, M.; Takamjani, I.E.; Bidari, S.; Parnianpour, M. Effect of equipping an unloader knee orthosis with vibrators on pain, function, stiffness and knee adduction moment in people with knee osteoarthritis: A pilot randomized trial. Gait Posture 2023, 99, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Marconi, E.; Teixeira-Silva, Y.; de Meirelles, A.G.; Moura-Fernandes, M.C.; Lopes-Souza, P.; Reis-Silva, A.; Marchon, R.M.; Guedes-Aguiar, E.d.O.; Paineiras-Domingos, L.L.; Sá-Caputo, D.d.C.d.; et al. Effect of whole-body vibration on the functional responses of the patients with knee osteoarthritis by the electromyographic profile of the vastus lateralis muscles during the five-repetition chair stand test: A randomized crossover trial. Appl. Sci. 2020, 10, 4302. [Google Scholar] [CrossRef]
- Qiu, C.G.; Chui, C.S.; Chow, S.K.H.; Cheung, W.-H.; Wong, R.M.Y. Effects of Whole-Body Vibration Therapy on Knee Osteoarthritis: A Sys-tematic Review and Meta-Analysis of Randomized Controlled Trials. J. Rehabil. Med. 2022, 54, jrm00266. [Google Scholar] [CrossRef] [PubMed]
- Barati, K.; Esfandiari, E.; Kamyab, M.; Takamjani, I.E.; Atlasi, R.; Parnianpour, M.; Yazdi, H.; Shahali, S.; Bidari, S. The effect of local muscle vibration on clinical and biomechanical parameters in people with knee osteoarthritis: A systematic review. Med. J. Islam. Repub. Iran 2021, 35, 124. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Moura-Fernandes, M.C.; Moreira-Marconi, E.; de Meirelles, A.G.; Reis-Silva, A.; de Souza, L.F.F.; da Silva, A.L.P.; de Oliveira, B.B.M.; Gama, M.A.d.S.; de Oliveira, A.C.C.; Batouli-Santos, D.; et al. Acute effects of whole-body vibration exercise on pain level, functionality, and rating of exertion of elderly obese knee osteoarthritis individuals: A randomized study. Appl. Sci. 2020, 10, 5870. [Google Scholar] [CrossRef]
- Abbasi, E.; Kahrizi, S.; Razi, M.; Faghihzadeh, S. The effect of whole-body vibration training on the lower extremity muscles’ electromyographic activities in patients with knee osteoarthritis. Med. J. Islam. Repub. Iran 2017, 31, 718–727. [Google Scholar] [CrossRef]
- Lai, Z.; Lee, S.; Chen, Y.; Wang, L. Comparison of whole-body vibration training and quadriceps strength training on physical function and neuromuscular function of individuals with knee osteoarthritis: A randomised clinical trial. J. Exerc. Sci. Fit. 2021, 19, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Maleki-Fischbach, M.; Jordan, J.M. New developments in osteoarthritis. Sex differences in magnetic resonance imaging-based biomarkers and in those of joint metabolism. Arthritis Res. Ther. 2010, 12, 212. [Google Scholar] [CrossRef] [PubMed]
- Tschon, M.; Contartese, D.; Pagani, S.; Borsari, V.; Fini, M. Gender and Sex Are Key Determinants in Osteoarthritis Not Only Confounding Variables. A Systematic Review of Clinical Data. J. Clin. Med. 2021, 10, 3178. [Google Scholar] [CrossRef]
- Wang, P.; Yang, L.; Li, H.; Lei, Z.; Yang, X.; Liu, C.; Jiang, H.; Zhang, L.; Zhou, Z.; Reinhardt, J.; et al. Effects of whole-body vibration training with quadriceps strengthening exercise on functioning and gait parameters in patients with medial compartment knee osteoarthritis: A randomised controlled preliminary study. Physiotherapy 2015, 102, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Yang, L.; Liu, C.; Wei, X.; Yang, X.; Zhou, Y.; Jiang, H.; Lei, Z.; Reinhardt, J.D.; He, C. Effects of Whole Body Vibration Exercise associated with Quadriceps Resistance Exercise on functioning and quality of life in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2016, 30, 1074–1087. [Google Scholar] [CrossRef]
- Lai, Z.; Lee, S.; Hu, X.; Wang, L. Effect of adding whole-body vibration training to squat training on physical function and muscle strength in individuals with knee osteoarthritis. J. Musculoskelet. Neuronal. Interact. 2019, 19, 333–341. [Google Scholar]
- Rice, D.A.; McNair, P.J.; Lewis, G.N. Mechanisms of quadriceps muscle weakness in knee joint osteoarthritis: The effects of prolonged vibration on torque and muscle activation in osteoarthritic and healthy control subjects. Arthritis Res. Ther. 2011, 13, R151. [Google Scholar] [CrossRef]
- Kitay, G.; Koren, M.; Helfet, D.; Parides, M.; Markenson, J. Efficacy of combined local mechanical vibrations, continuous passive motion and thermotherapy in the management of osteoarthritis of the knee. Osteoarthr. Cartil. 2009, 17, 1269–1274. [Google Scholar] [CrossRef]
- Petit, P.-D.; Pensini, M.; Tessaro, J.; Desnuelle, C.; Legros, P.; Colson, S.S. Optimal whole-body vibration settings for muscle strength and power enhancement in human knee extensors. J. Electromyogr. Kinesiol. 2010, 20, 1186–1195. [Google Scholar] [CrossRef]
- Karatrantou, K.; Gerodimos, V.; Dipla, K.; Zafeiridis, A. Whole-body vibration training improves flexibility, strength profile of knee flexors, and hamstrings-to-quadriceps strength ratio in females. J. Sci. Med. Sport 2013, 16, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.R.; Roper, J.A.; Tillman, M.D. Does acute whole-body vibration training improve the physical performance of people with knee osteoarthritis? J. Strength Cond. Res. 2012, 26, 2983–2989. [Google Scholar] [CrossRef] [PubMed]
| Databases | Search Strategies |
|---|---|
| PubMed/MEDLINE | (vibration OR “local muscle vibration” OR “vibration therapy” OR “whole body vibration” OR “orthotic device” OR “local vibration”) AND (“knee osteoarthritis” OR “knee osteoarthritides” OR “osteoarthritis of knee” OR “osteoarthritis of the knee”) |
| PEDro | “knee osteoarthritis” AND “vibration” |
| SCOPUS | (vibration OR “local muscle vibration” OR “vibration therapy” OR “whole body vibration” OR “orthotic device” OR “local vibration”) AND (“knee osteoarthritis” OR “knee osteoarthritides” OR “osteoarthritis of knee” OR “osteoarthritis of the knee”) |
| Embase | (‘knee osteoarthritis’/exp OR ‘knee osteoarthritis’) AND (‘vibration’/exp OR vibration) |
| Web of Science | (vibration OR “local muscle vibration” OR “vibration therapy” OR “whole body vibration” OR “orthotic device” OR “local vibration”) AND (“knee osteoarthritis” OR “knee osteoarthritides” OR “osteoarthritis of knee” OR “osteoarthritis of the Knee”) |
| Reference | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Trans et al., 2009 [31] | 7/10 | ||||||||||
| Abbasi et al., 2017 [40] | 8/10 | ||||||||||
| Moreira-Marconi et al., 2020 [34] | 6/10 | ||||||||||
| Moura-Fernandes et al., 2020 [39] | 7/10 | ||||||||||
| Lai et al., 2021 [41] | 8/10 | ||||||||||
| 100% | 60% | 100% | 60% | 0% | 0% | 100% | 100% | 100% | 100% |
| Reference | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rabini et al. 2015 [14] | 9/10 | ||||||||||
| Benedetti et al. 2017 [13] | 4/10 | ||||||||||
| Barati et al. 2023 [33] | 3/10 | ||||||||||
| Pasterczyk-Szczurek et al. 2023 [32] | 6/10 | ||||||||||
| 100% | 25% | 25% | 50% | 0% | 25% | 75% | 100% | 50% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melo-Lima, P.; Cardoso, A.L.B.D.; Coelho-Oliveira, A.C.; Reis-Silva, A.; Batouli-Santos, D.; Alhammad, A.; Valério-Penha, A.G.; Sá-Caputo, D.C.; Bernardo-Filho, M.; Taiar, R. Effects of Systemic and Local Vibration Therapies on the Functional Capacity of Knee Osteoarthritis Individuals: A Systematic Review of Randomized Clinical Trials. Appl. Sci. 2025, 15, 5349. https://doi.org/10.3390/app15105349
Melo-Lima P, Cardoso ALBD, Coelho-Oliveira AC, Reis-Silva A, Batouli-Santos D, Alhammad A, Valério-Penha AG, Sá-Caputo DC, Bernardo-Filho M, Taiar R. Effects of Systemic and Local Vibration Therapies on the Functional Capacity of Knee Osteoarthritis Individuals: A Systematic Review of Randomized Clinical Trials. Applied Sciences. 2025; 15(10):5349. https://doi.org/10.3390/app15105349
Chicago/Turabian StyleMelo-Lima, Philipe, André L. B. D. Cardoso, Ana Carolina Coelho-Oliveira, Aline Reis-Silva, Daniel Batouli-Santos, Ayman Alhammad, Ana Gabriellie Valério-Penha, Danúbia C. Sá-Caputo, Mario Bernardo-Filho, and Redha Taiar. 2025. "Effects of Systemic and Local Vibration Therapies on the Functional Capacity of Knee Osteoarthritis Individuals: A Systematic Review of Randomized Clinical Trials" Applied Sciences 15, no. 10: 5349. https://doi.org/10.3390/app15105349
APA StyleMelo-Lima, P., Cardoso, A. L. B. D., Coelho-Oliveira, A. C., Reis-Silva, A., Batouli-Santos, D., Alhammad, A., Valério-Penha, A. G., Sá-Caputo, D. C., Bernardo-Filho, M., & Taiar, R. (2025). Effects of Systemic and Local Vibration Therapies on the Functional Capacity of Knee Osteoarthritis Individuals: A Systematic Review of Randomized Clinical Trials. Applied Sciences, 15(10), 5349. https://doi.org/10.3390/app15105349