
Ultrasound-Based Deep Learning Models Performance versus Expert Subjective Assessment for Discriminating Adnexal Masses: A Head-to-Head Systematic Review and Meta-Analysis
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
- Primary diagnostic prospective or retrospective studies evaluating deep learning models for the diagnosis of adnexal masses and comparing them to expert evaluation.
- Collected Data allows the construction of a 2 × 2 table to estimate true positive, true negative, false positive, and false negative cases for any of the index tests assessed.
- The reference test was considered histological confirmation.
- Studies not related to the topic.
- Studies evaluating AI or ML other than DL.
- Secondary studies (other meta-analysis or systematic reviews) or those where insufficient data were provided.
- Studies where other imaging studies such as MRI or CT were considered.
- Articles that did not compare deep learning results with those obtained by expert examiners.
- Studies where histological confirmation was not the gold standard or was not available.
- Studies combining evaluation of biomarkers to ultrasonography.
2.3. Data Extraction and Management
2.4. Qualitative Synthesis
2.5. Quantitative Synthesis
3. Results
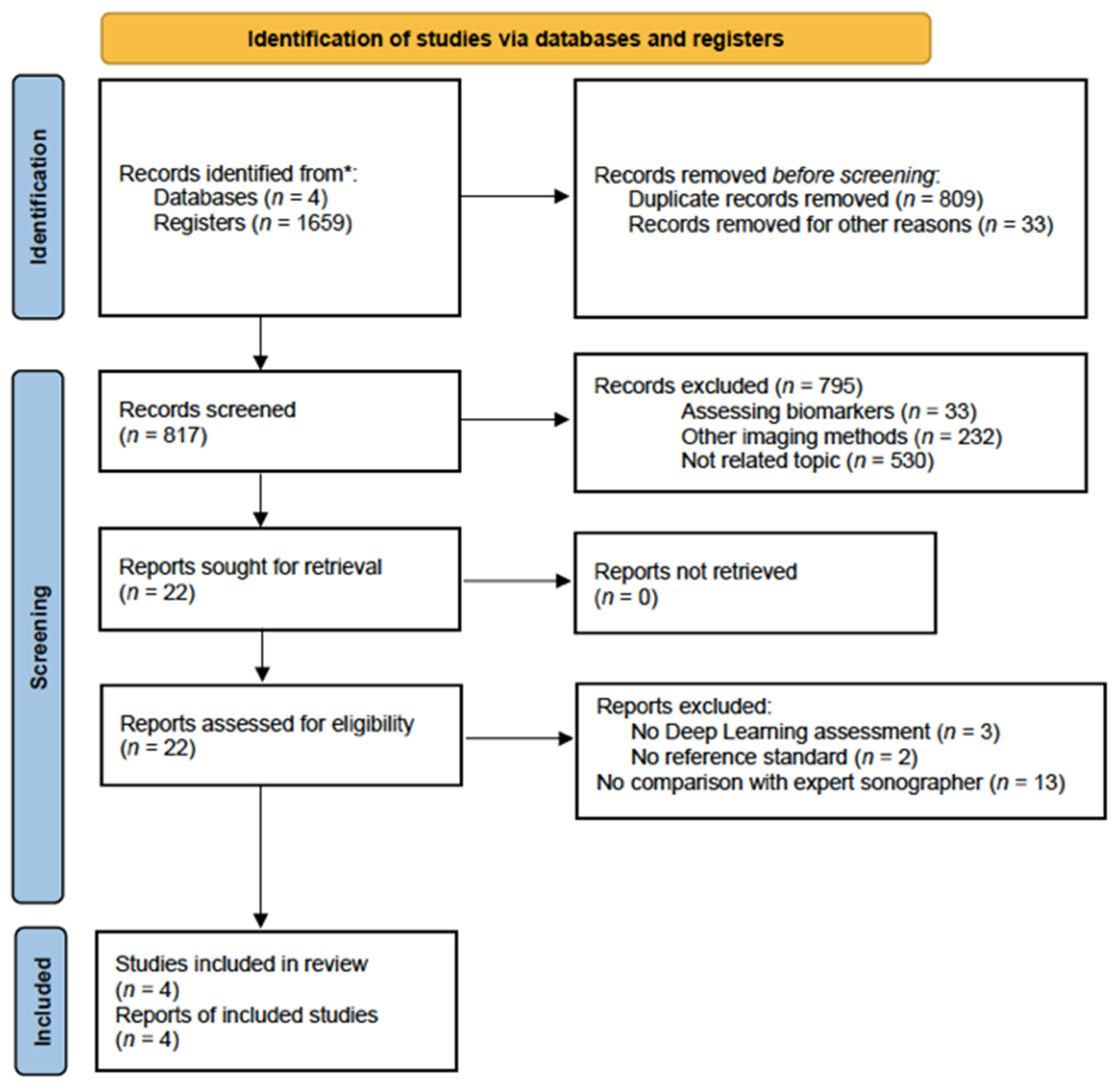
3.1. Search Results
3.2. Characteristics of Studies
3.3. Qualitative Synthesis
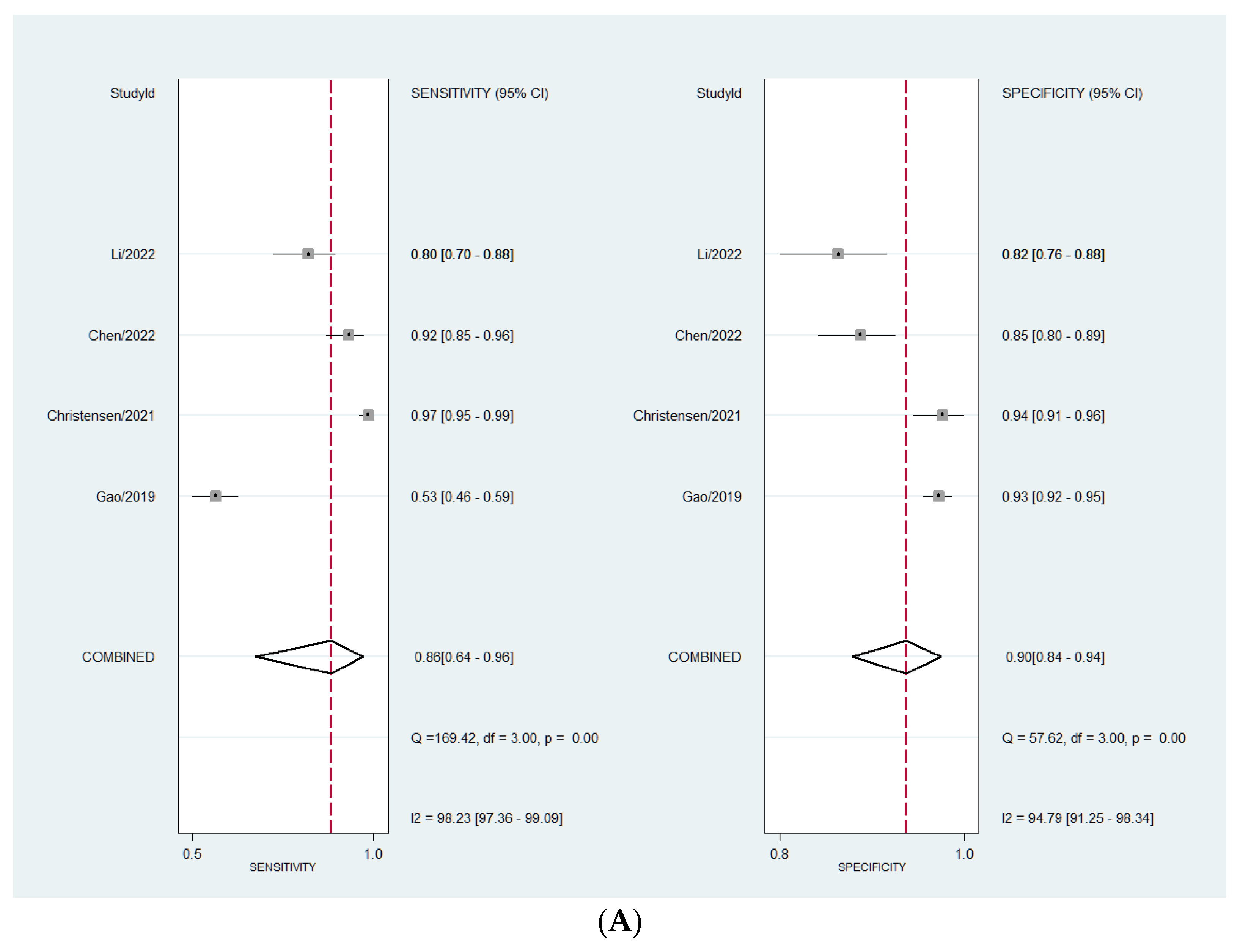
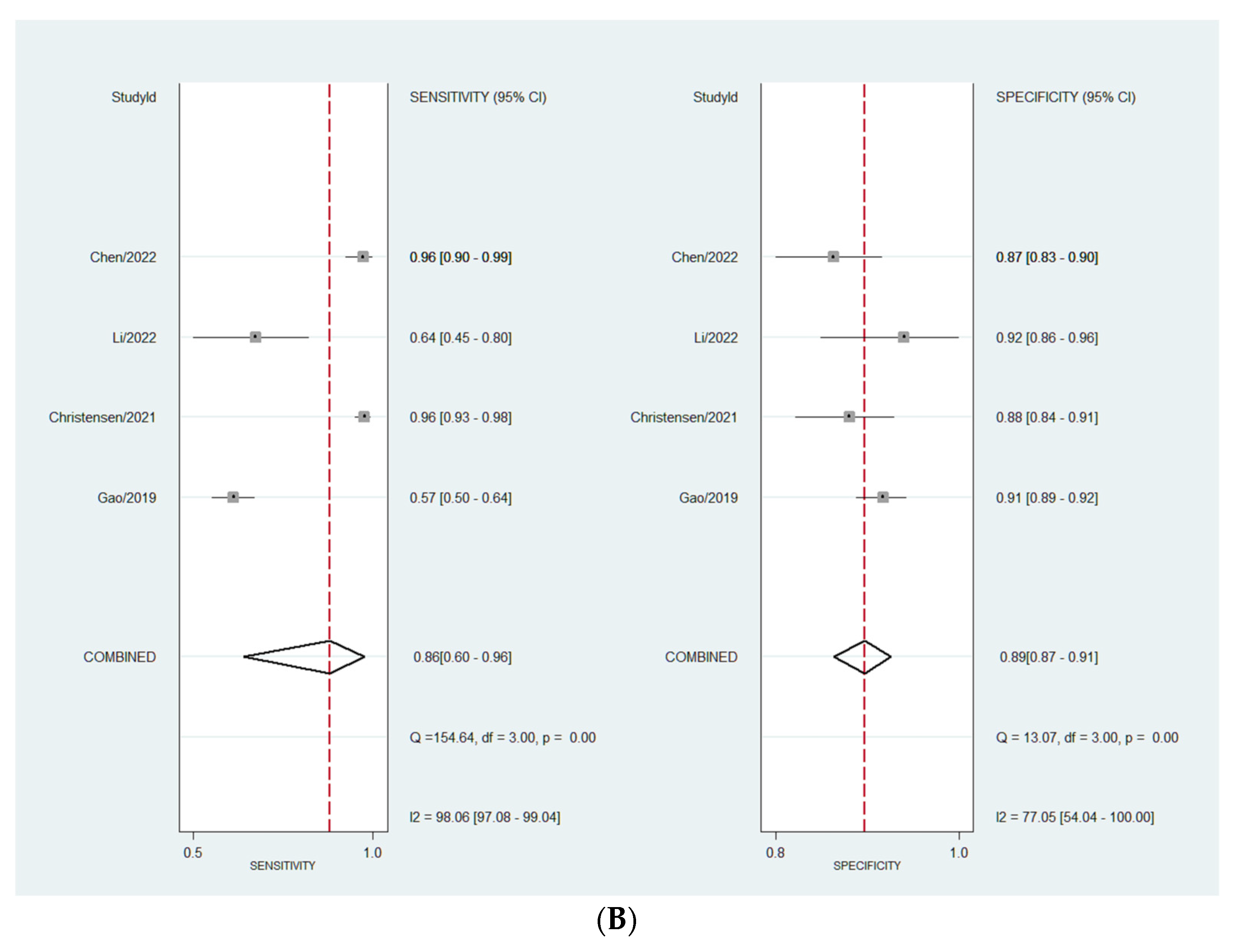
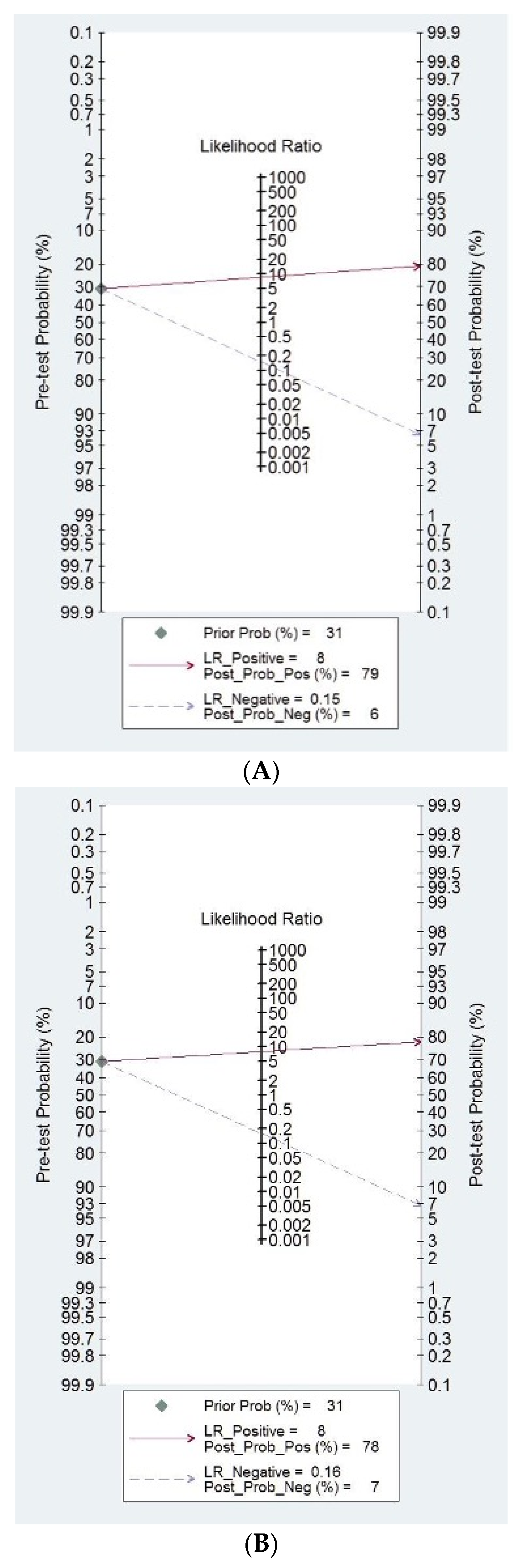
3.4. Quantitative Synthesis
4. Discussion
4.1. Summary of Findings
4.2. Interpretation of Findings in Clinical Context
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grimes, D.A.; Hughes, J.M. Use of multiphasic oral contraceptives and hospitalizations of women with functional ovarian cysts in the United States. Obstet. Gynecol. 1989, 73, 1037–1039. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Olartecoechea, B.; Guerriero, S.; Jurado, M. Expectant management of adnexal masses in selected premenopausal women: A prospective observational study. Ultrasound Obstet. Gynecol. 2013, 41, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Froyman, W.; Landolfo, C.; De Cock, B.; Wynants, L.; Sladkevicius, P.; Testa, A.C.; Van Holsbeke, C.; Domali, E.; Fruscio, R.; Epstein, E. Risk of complications in patients with conservatively managed ovarian tumours (IOTA5): A 2-year interim analysis of a multicentre, prospective, cohort study. Lancet Oncol. 2019, 20, 448–458. [Google Scholar] [CrossRef]
- Glanc, P.; Benacerraf, B.; Bourne, T.; Brown, D.; Coleman, B.G.; Crum, C.; Dodge, J.; Levine, D.; Pavlik, E.; Ueland, F.R. First International Consensus Report on Adnexal Masses: Management Recommendations. J. Ultrasound Med. 2017, 36, 849–863. [Google Scholar] [CrossRef]
- Stein, E.B.; Hansen, J.M.; Maturen, K.E. Fertility-Sparing Approaches in Gynecologic Oncology: Role of Imaging in Treatment Planning. Radiol. Clin. N. Am. 2020, 58, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Webb, P.M.; Jordan, S.J. Epidemiology of epithelial ovarian cancer. Best. Pract. Res. Clin. Obstet. Gynaecol. 2016, S1521-S6934, 30091–30098. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Jacobs, I.J.; Menon, U.; Ryan, A.; Gentry-Maharaj, A.; Burnell, M.; Kalsi, J.K.; Amso, N.N. Ovarian cancer screening and mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomized controlled trial. Lancet 2016, 387, 945–956. [Google Scholar] [CrossRef]
- Kim, B.R.; Kim, H.; Joo, S.G.; Jang, E.J.; Jo, J.; Lee, H.; Ryu, H.G. Effect of Hospital Case-Volume on Mortality after Ovarian Cancer Surgery: A Population-Based Retrospective Cohort Study. Gynecol. Obstet. Investig. 2022, 87, 364–372. [Google Scholar] [CrossRef]
- Nasioudis, D.; Kahn, R.; Chapman-Davis, E.; Frey, M.K.; Caputo, T.A.; Witkin, S.S.; Holcomb, K. Impact of hospital surgical volume on complete gross resection (CGR) rates following primary debulking surgery for advanced stage epithelial ovarian carcinoma. Gynecol. Oncol. 2019, 154, 401–404. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet. Gynecol. 2016, 128, e210–e226. [Google Scholar] [CrossRef] [PubMed]
- Salvador, S.; Scott, S.; Glanc, P.; Eiriksson, L.; Jang, J.H.; Sebastianelli, A.; Dean, E. Guideline No. 403: Initial Investigation and Management of Adnexal Masses. J. Obstet. Gynaecol. Can. 2020, 42, 1021–1029.e3. [Google Scholar] [CrossRef] [PubMed]
- Yazbek, J.; Ameye, L.; Testa, A.C.; Valentin, L.; Timmerman, D.; Holland, T.K.; Van Holsbeke, C.; Jurkovic, D. Confidence of expert ultrasound operators in making a diagnosis of adnexal tumor: Effect on diagnostic accuracy and interobserver agreement. Ultrasound Obstet. Gynecol. 2010, 35, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Van Holsbeke, C.; Daemen, A.; Yazbek, J.; Holland, T.K.; Bourne, T.; Mesens, T.; Lannoo, L.; Boes, A.S.; Joos, A.; Van De Vijver, A. Ultrasound experience substantially impacts on diagnostic performance and confidence when adnexal masses are classified using pattern recognition. Gynecol. Obstet. Investig. 2010, 69, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Yazbek, J.; Raju, S.K.; Ben-Nagi, J.; Holland, T.K.; Hillaby, K.; Jurkovic, D. Effect of quality of gynaecological ultrasonography on management of patients with suspected ovarian cancer: A randomised controlled trial. Lancet Oncol. 2008, 9, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Pascual, M.A.; Graupera, B.; Aubá, M.; Errasti, T.; Olartecoechea, B.; Ruiz-Zambrana, A.; Hereter, L.; Ajossa, S.; Guerriero, S. External validation of IOTA simple descriptors and simple rules for classifying adnexal masses. Ultrasound Obstet. Gynecol. 2016, 48, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Romanelli, C.; Capezzuoli, T. Adnexal masses: What is the role of ultrasonographic imaging? Arch. Gynecol. Obstet. 2014, 290, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Sassone, A.M.; Timor-Tritsch, I.E.; Artner, A.; Westhoff, C.; Warren, W.B. Transvaginal sonographic characterization of ovarian disease: Evaluation of a new scoring system to predict ovarian malignancy. Obstet. Gynecol. 1991, 78, 70–76. [Google Scholar]
- Alcázar, J.L.; Mercé, L.T.; Laparte, C.; Jurado, M.; López-García, G. A new scoring system to differentiate benign from malignant adnexal masses. Am. J. Obstet. Gynecol. 2003, 188, 685–692. [Google Scholar] [CrossRef]
- Amor, F.; Alcázar, J.L.; Vaccaro, H.; León, M.; Iturra, A. GI-RADS reporting system for ultrasound evaluation of adnexal masses in clinical practice: A prospective multicenter study. Ultrasound Obstet. Gynecol. 2011, 38, 450–455. [Google Scholar] [CrossRef]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Van Holsbeke, C.; Paladini, D.; Van Calster, B.; Vergote, I.; Van Huffel, S. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, R.F.; Timmerman, D.; Strachowski, L.M.; Froyman, W.; Benacerraf, B.R.; Bennett, G.L.; Bourne, T.; Brown, D.L.; Coleman, B.G.; Frates, M.C.; et al. O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020, 294, 168–185. [Google Scholar] [CrossRef]
- Shrestha, P.; Poudyal, B.; Yadollahi, S.; Wright, D.; Gregory, A.; Warner, J.; Korfiatis, P.; Green, I.; Rassier, S.; Mariani, A.; et al. A systematic review on the use of artificial intelligence in gynecologic imaging. Background, state of the art, and future directions. Gynecol. Oncol. 2022, 166, 596–605. [Google Scholar] [CrossRef]
- Grigore, M.; Popovici, R.M.; Gafitanu, D.; Himiniuc, L.; Murarasu, M.; Micu, R. Logistic models and artificial intelligence in the sonographic assessment of adnexal masses—A systematic review of the literature. Med. Ultrason. 2020, 22, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Drukker, L.; Noble, J.A.; Papageorghiou, A.T. Introduction to artificial intelligence in ultrasound imaging in obstetrics and gynecology. Ultrasound Obstet. Gynecol. 2020, 56, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Sree, S.V.; Krishnan, M.M.; Saba, L.; Molinari, F.; Guerriero, S.; Suri, J.S. Ovarian tumor characterization using 3D ultrasound. Technol. Cancer Res. Treat. 2012, 11, 543–552. [Google Scholar] [CrossRef]
- Alqasemi, U.; Kumavor, P.; Aguirre, A.; Zhu, Q. Recognition algorithm for assisting ovarian cancer diagnosis from coregistered ultrasound and photoacoustic images: Ex vivo study. J. Biomed. Opt. 2012, 17, 126003. [Google Scholar] [CrossRef]
- Acharya, U.R.; Sree, V.S.; Saba, L.; Molinari, F.; Guerriero, S.; Suri, J.S. Ovarian tumor characterization and classification: A class of GyneScanTM systems. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2012, 2012, 4446–4449. [Google Scholar]
- Acharya, U.R.; Sree, S.V.; Saba, L.; Molinari, F.; Guerriero, S.; Suri, J.S. Ovarian tumor characterization and classification using ultrasound—A new online paradigm. J. Digit. Imaging 2013, 26, 544–553. [Google Scholar] [CrossRef]
- Acharya, U.R.; Sree, S.V.; Kulshreshtha, S.; Molinari, F.; Koh, J.E.; Saba, L.; Suri, J.S. GyneScan: An improved online paradigm for screening of ovarian cancer via tissue characterization. Technol. Cancer Res. Treat. 2014, 13, 529–539. [Google Scholar] [CrossRef]
- Acharya, U.R.; Mookiah, M.R.; Sree, S.V.; Yanti, R.; Martis, R.J.; Saba, L.; Molinari, F.; Guerriero, S.; Suri, J.S. Evolutionary algorithm- based classifier parameter tuning for automatic ovarian cancer tissue characterization and classification. Ultraschall Med. 2014, 35, 237–245. [Google Scholar] [PubMed]
- Pathak, H.; Kulkarni, V. Identification of ovarian mass through ultrasound images using machine learning techniques. In Proceedings of the 2015 IEEE International Conference on Research in Computational Intelligence and Communication Networks (ICRCICN), Kolkata, India, 20–22 November 2015; pp. 137–140. [Google Scholar]
- Aramendía-Vidaurreta, V.; Cabeza, R.; Villanueva, A.; Navallas, J.; Alcazar, J.L. Ultrasound image discrimination between benign and malignant adnexal masses based on a neural network approach. Ultrasound Med. Biol. 2016, 42, 742–752. [Google Scholar] [CrossRef]
- Martínez-Más, J.; Bueno-Crespo, A.; Khazendar, S.; Remezal-Solano, M.; Martínez-Cendán, J.P.; Jassim, S.; Du, H.; Al Assam, H.; Bourne, T. Evaluation of machine learning methods with Fourier transform features for classifying ovarian tumors based on ultrasound images. PLoS ONE 2019, 14, e0219388. [Google Scholar] [CrossRef]
- Akazawa, M.; Hashimoto, K. Artificial intelligence in ovarian cancer diagnosis. Anticancer Res. 2020, 40, 4795–4800. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, C.; Zhao, Z.; Zhang, C.; Wang, X.; Li, H.; Wu, H.; Liu, X.; Li, C.; Qi, L.; et al. Application of deep convolutional neural networks for discriminating benign, borderline, and malignant serous ovarian tumors from ultrasound images. Front. Oncol. 2021, 11, 770683. [Google Scholar] [CrossRef]
- Chiappa, V.; Bogani, G.; Interlenghi, M.; Salvatore, C.; Bertolina, F.; Sarpietro, G.; Signorelli, M.; Castiglioni, I. The Adoption of radiomics and machine learning improves the diagnostic processes of women with ovarian masses (the AROMA pilot study). J. Ultrasound. 2021, 24, 429–437. [Google Scholar] [CrossRef]
- Ștefan, P.A.; Lupean, R.A.; Mihu, C.M.; Lebovici, A.; Oancea, M.D.; Hîțu, L.; Duma, D.; Csutak, C. Ultrasonography in the diagnosis of adnexal lesions: The role of texture analysis. Diagnostics 2021, 11, 812. [Google Scholar] [CrossRef] [PubMed]
- Al-Karawi, D.; Al-Assam, H.; Du, H.; Sayasneh, A.; Landolfo, C.; Timmerman, D.; Bourne, T.; Jassim, S. An evaluation of the effectiveness of image-based texture features extracted from static B mode ultrasound images in distinguishing between benign and malignant ovarian masses. Ultrason. Imaging 2021, 43, 124–138. [Google Scholar] [CrossRef]
- Christiansen, F.; Epstein, E.L.; Smedberg, E.; Åkerlund, M.; Smith, K.; Epstein, E. Ultrasound image analysis using deep neural networks for discriminating between benign and malignant ovarian tumors: Comparison with expert subjective assessment. Ultrasound Obstet. Gynecol. 2021, 57, 155–163. [Google Scholar] [CrossRef]
- Guo, X.; Zhao, G. Establishment and verification of logistic regression model for qualitative diagnosis of ovarian cancer based on MRI and ultrasound signs. Comput. Math. Methods Med. 2022, 2022, 7531371. [Google Scholar] [CrossRef]
- Chen, H.; Yang, B.W.; Qian, L.; Meng, Y.S.; Bai, X.H.; Hong, X.W.; He, X.; Jiang, M.J.; Yuan, F.; Du, Q.W. Deep learning prediction of ovarian malignancy at US compared with O-RADS and expert assessment. Radiology. 2022, 304, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, Y.; Zhang, M.; Zhang, P.; He, K.; Yan, F.; Li, J.; Xu, H.; Burkhoff, D.; Luo, Y.; et al. A Deep Learning Model System for Diagnosis and Management of Adnexal Masses. Cancers 2022, 14, 5291. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zeng, S.; Xu, X.; Li, H.; Yao, S.; Song, K.; Li, X.; Chen, L.; Tang, J.; Xing, H.; et al. Deep learning-enabled pelvic ultrasound images for accurate diagnosis of ovarian cancer in China: A retrospective, multicentre, diagnostic study. Lancet Digit. Health 2022, 4, e179–e187. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, n71. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 18, 529–536. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Planchamp, F.; Bourne, T.; Landolfo, C.; du Bois, A.; Chiva, L.; Cibula, D.; Concin, N.; Fischerova, D.; Froyman, W. ESGO/ISUOG/ IOTA/ESGE Consensus Statement on pre-operative diagnosis of ovarian tumors. Int. J. Gynecol. Cancer 2021, 31, 961–982. [Google Scholar] [CrossRef]
- Meys, E.M.; Kaijser, J.; Kruitwagen, R.F.; Slangen, B.F.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.Y.; Timmerman, D.; Van Gorp, T. Subjective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur. J. Cancer 2016, 58, 17–29. [Google Scholar] [CrossRef]
- Jacobs, I.; Oram, D.; Fairbanks, J.; Turner, J.; Frost, C.; Grudzinskas, J.G. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br. J. Obstet. Gynaecol. 1990, 97, 922–929. [Google Scholar] [CrossRef]
- Chacón, E.; Dasí, J.; Caballero, C.; Alcázar, J.L. Risk of Ovarian Malignancy Algorithm versus Risk Malignancy Index-I for Preoperative Assessment of Adnexal Masses: A Systematic Review and Meta-Analysis. Gynecol. Obstet. Investig. 2019, 84, 591–598. [Google Scholar] [CrossRef]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ferrazzi, E.; Ameye, L.; Konstantinovic, M.L.; Van Calster, B.; Collins, W.P.; Vergote, I.; Van Huffel, S.; et al. Logistic regression model to distinguish between the benign and malignant adnexal mass before surgery: A multicenter study by the International Ovarian Tumor Analysis Group. J. Clin. Oncol. 2005, 23, 8794–8801. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [PubMed]
- Amor, F.; Vaccaro, H.; Alcázar, J.L.; León, M.; Craig, J.M.; Martinez, J. Gynecologic imaging reporting and data system: A new proposal for classifying adnexal masses on the basis of sonographic findings. J. Ultrasound Med. 2009, 28, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Kaijser, J.; Sayasneh, A.; Van Hoorde, K.; Ghaem-Maghami, S.; Bourne, T.; Timmerman, D.; Van Calster, B. Presurgical diagnosis of adnexal tumours using mathematical models and scoring systems: A systematic review and meta-analysis. Hum. Reprod. Update 2014, 20, 449–462. [Google Scholar] [CrossRef] [PubMed]
- Ilundain, A.; Salas, A.; Chacón, E.; Manzour, N.; Alcazar, J.L. IOTA Simple Rules for the differential diagnosis of ovarian adnexal masses: Systematic review and meta-analysis. Prog. Obstet. Ginecol. 2018, 61, 390–400. [Google Scholar]
- Yue, X.; Zhong, L.; Wang, Y.; Zhang, C.; Chen, X.; Wang, S.; Hu, J.; Hu, J.; Wang, C.; Liu, X. Value of Assessment of Different Neoplasias in the Adnexa in the Differential Diagnosis of Malignant Ovarian Tumor and Benign Ovarian Tumor: A Meta-analysis. Ultrasound Med. Biol. 2022, 48, 730–742. [Google Scholar] [CrossRef] [PubMed]
- Barreñada, L.; Ledger, A.; Dhiman, P.; Collins, G.; Wynants, L.; Verbakel, J.Y.; Timmerman, D.; Valentin, L.; Van Calster, B. ADNEX risk prediction model for diagnosis of ovarian cancer: Systematic review and meta-analysis of external validation studies. BMJ Med. 2024, 3, e000817. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Zou, X.; Xu, H.; Zhang, T.; Zhao, Y.; Gao, L.; Duan, W.; Ma, X.; Zhang, L. The diagnostic performance of the Gynecologic Imaging Reporting and Data System (GI-RADS) in adnexal masses. Ann. Transl. Med. 2021, 9, 398. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Rodriguez-Guzman, L.; Vara, J.; Amor, F.; Diaz, L.; Vaccaro, H. Gynecologic Imaging and Reporting Data System for classifying adnexal masses. Minerva Obstet. Gynecol. 2023, 75, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Vara, J.; Manzour, N.; Chacón, E.; López-Picazo, A.; Linares, M.; Pascual, M.Á.; Guerriero, S.; Alcázar, J.L. Ovarian Adnexal Reporting Data System (O-RADS) for Classifying Adnexal Masses: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 3151. [Google Scholar] [CrossRef]
- Lee, S.; Lee, J.E.; Hwang, J.A.; Shin, H. O-RADS US: A Systematic Review and Meta-Analysis of Category-specific Malignancy Rates. Radiology 2023, 308, e223269. [Google Scholar] [CrossRef]
- Zhang, Q.; Dai, X.; Li, W. Systematic Review and Meta-Analysis of O-RADS Ultrasound and O-RADS MRI for Risk Assessment of Ovarian and Adnexal Lesions. AJR Am. J. Roentgenol. 2023, 221, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Dhombres, F.; Bonnard, J.; Bailly, K.; Maurice, P.; Papageorghiou, A.T.; Jouannic, J.M. Contributions of Artificial Intelligence Reported in Obstetrics and Gynecology Journals: Systematic Review. J. Med. Internet Res. 2022, 24, e35465. [Google Scholar] [CrossRef] [PubMed]
- Jost, E.; Kosian, P.; Jimenez Cruz, J.; Albarqouni, S.; Gembruch, U.; Strizek, B.; Recker, F. Evolving the Era of 5D Ultrasound? A Systematic Literature Review on the Applications for Artificial Intelligence Ultrasound Imaging in Obstetrics and Gynecology. J. Clin. Med. 2023, 12, 6833. [Google Scholar] [CrossRef]
- Tailor, A.; Jurkovic, D.; Bourne, T.H.; Collins, W.P.; Campbell, S. Sonographic prediction of malignancy in adnexal masses using an artificial neural network. Br. J. Obstet. Gynaecol. 1999, 106, 21–30. [Google Scholar] [CrossRef]
- Timmerman, D.; Verrelst, H.; Bourne, T.H.; De Moor, B.; Collins, W.P.; Vergote, I.; Vandewalle, J. Artificial neural network models for the preoperative discrimination between malignant and benign adnexal masses. Ultrasound Obstet. Gynecol. 1999, 13, 17–25. [Google Scholar] [CrossRef]
- Biagiotti, R.; Desii, C.; Vanzi, E.; Gacci, G. Predicting ovarian malignancy: Application of artificial neural networks to transvaginal and color Doppler flow US. Radiology 1999, 210, 399–403. [Google Scholar] [CrossRef]
- Szpurek, D.; Moszynski, R.; Smolen, A.; Sajdak, S. Artificial neural network computer prediction of ovarian malignancy in women with adnexal masses. Int. J. Gynaecol. Obstet. 2005, 89, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.L.; Gong, T.T.; Liu, F.H.; Chen, H.Y.; Xiao, Q.; Hou, Y.; Huang, Y.; Sun, H.Z.; Shi, Y.; Gao, S.; et al. Artificial intelligence performance in image-based ovarian cancer identification: A systematic review and meta-analysis. E Clin. Med. 2022, 17, 101662. [Google Scholar]
- Ma, L.; Huang, L.; Chen, Y.; Zhang, L.; Nie, D.; He, W.; Qi, X. AI diagnostic performance based on multiple imaging modalities for ovarian tumor: A systematic review and meta-analysis. Front. Oncol. 2023, 13, 1133491. [Google Scholar] [CrossRef]
- Ismael, A.M.; Şengür, A. Deep learning approaches for COVID-19 detection based on chest X-ray images. Expert. Syst. Appl. 2021, 164, 114054. [Google Scholar] [CrossRef]
- Li, C.; Zhang, H.; Chen, J.; Shao, S.; Li, X.; Yao, M.; Zheng, Y.; Wu, R.; Shi, J. Deep learning radiomics of ultrasonography for differentiating sclerosing adenosis from breast cancer. Clin. Hemorheol. Microcirc. 2023, 84, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Sethy, P.K.; Behera, S.K.; Anitha, K.; Pandey, C.; Khan, M.R. Computer aid screening of COVID-19 using X-ray and CT scan images: An inner comparison. J. X-ray Sci. Technol. 2021, 29, 197–210. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study Design | N Patients | Benign | Malignant and Borderline | Nº Centers | Age (Years) * | Reference Standard | Deep Learning Architecture | Time until Surgery (Days) ** |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gao [44] | 2022 | China | Retrospective | 1224 | 991 | 233 | 10 | External dataset1: 43 (32–52) External dataset2: 38 (27–48) | Histology | DCNN | NR |
| Christiansen [40] | 2021 | Sweden | Retrospective | 634 | 325 | 309 | 2 | NR | Histology | DNN: (VGG16, ResNet50 and MobileNet) | 120 |
| Chen [42] | 2022 | China | Retrospective | 422 | 304 | 118 | 1 | 46.8 (18–85) | Histology | CNN (ResNet-18) | 30 |
| Li [43] | 2022 | China | Retrospective | 261 | 177 | 84 | 3 | External 1: 48.87 (15, 77) External 2: 43.26 (19, 50) | Histology | CNN (ResNet-18) | NR |
| Author | Training SET | Internal Validation Set | Test Set | External Validation Set 1 | External Validation Set 2 | |
|---|---|---|---|---|---|---|
| Christensen [40] | ||||||
| Histology | 314 B/194 M | 60 B/40 M | 75 B/75 M | |||
| Images per histology | NR | NR | NR | ND | ND | |
| Chen [42] | ||||||
| Histology | 213 B/83 M | 30 B/11 M | 61 B/24 M | ND | ND | |
| Images per histology | NR | NR | NR | |||
| Li [43] | ||||||
| Histology | 882 B/217 M | 389 B/71 M | ND | 147 B/51 M | 231 B/33 M | |
| Images per histology | 2227 B/2270 M | 941 B/276 M | ND | 329 B/161 M | 634 B/127 M | |
| Gao [44] | ||||||
| Histology | 101,777 B/3755 M | 602 B/266 M | ND | 268 B/67 M | 723 B/166 M | |
| Images per histology | 541,442 B/344,488 M | 5385 B/3031 M | ND | 933 B/486 M | 5257 B/1253 M |
| Author | Year | Patient Selection | Index Test | Reference Standard | Flow and Timing |
|---|---|---|---|---|---|
| Christiansen [40] | 2021 | High risk | Low risk | Low risk | High risk |
| Chen [42] | 2022 | High risk | Low risk | Low risk | Low risk |
| Li [43] | 2022 | High risk | Low risk | Low risk | Unclear |
| Gao [44] | 2022 | High risk | Low risk | Low risk | Unclear |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lourenço, M.; Arrufat, T.; Satorres, E.; Maderuelo, S.; Novillo-Del Álamo, B.; Guerriero, S.; Orozco, R.; Alcázar, J.L. Ultrasound-Based Deep Learning Models Performance versus Expert Subjective Assessment for Discriminating Adnexal Masses: A Head-to-Head Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 2998. https://doi.org/10.3390/app14072998
Lourenço M, Arrufat T, Satorres E, Maderuelo S, Novillo-Del Álamo B, Guerriero S, Orozco R, Alcázar JL. Ultrasound-Based Deep Learning Models Performance versus Expert Subjective Assessment for Discriminating Adnexal Masses: A Head-to-Head Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(7):2998. https://doi.org/10.3390/app14072998
Chicago/Turabian StyleLourenço, Mariana, Teresa Arrufat, Elena Satorres, Sara Maderuelo, Blanca Novillo-Del Álamo, Stefano Guerriero, Rodrigo Orozco, and Juan Luis Alcázar. 2024. "Ultrasound-Based Deep Learning Models Performance versus Expert Subjective Assessment for Discriminating Adnexal Masses: A Head-to-Head Systematic Review and Meta-Analysis" Applied Sciences 14, no. 7: 2998. https://doi.org/10.3390/app14072998
APA StyleLourenço, M., Arrufat, T., Satorres, E., Maderuelo, S., Novillo-Del Álamo, B., Guerriero, S., Orozco, R., & Alcázar, J. L. (2024). Ultrasound-Based Deep Learning Models Performance versus Expert Subjective Assessment for Discriminating Adnexal Masses: A Head-to-Head Systematic Review and Meta-Analysis. Applied Sciences, 14(7), 2998. https://doi.org/10.3390/app14072998