




Validation of a Simple Device for the Evaluation of Ankle Plantar- and Dorsi-Flexor Forces Consistent with Standard Clinical Evaluations
 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
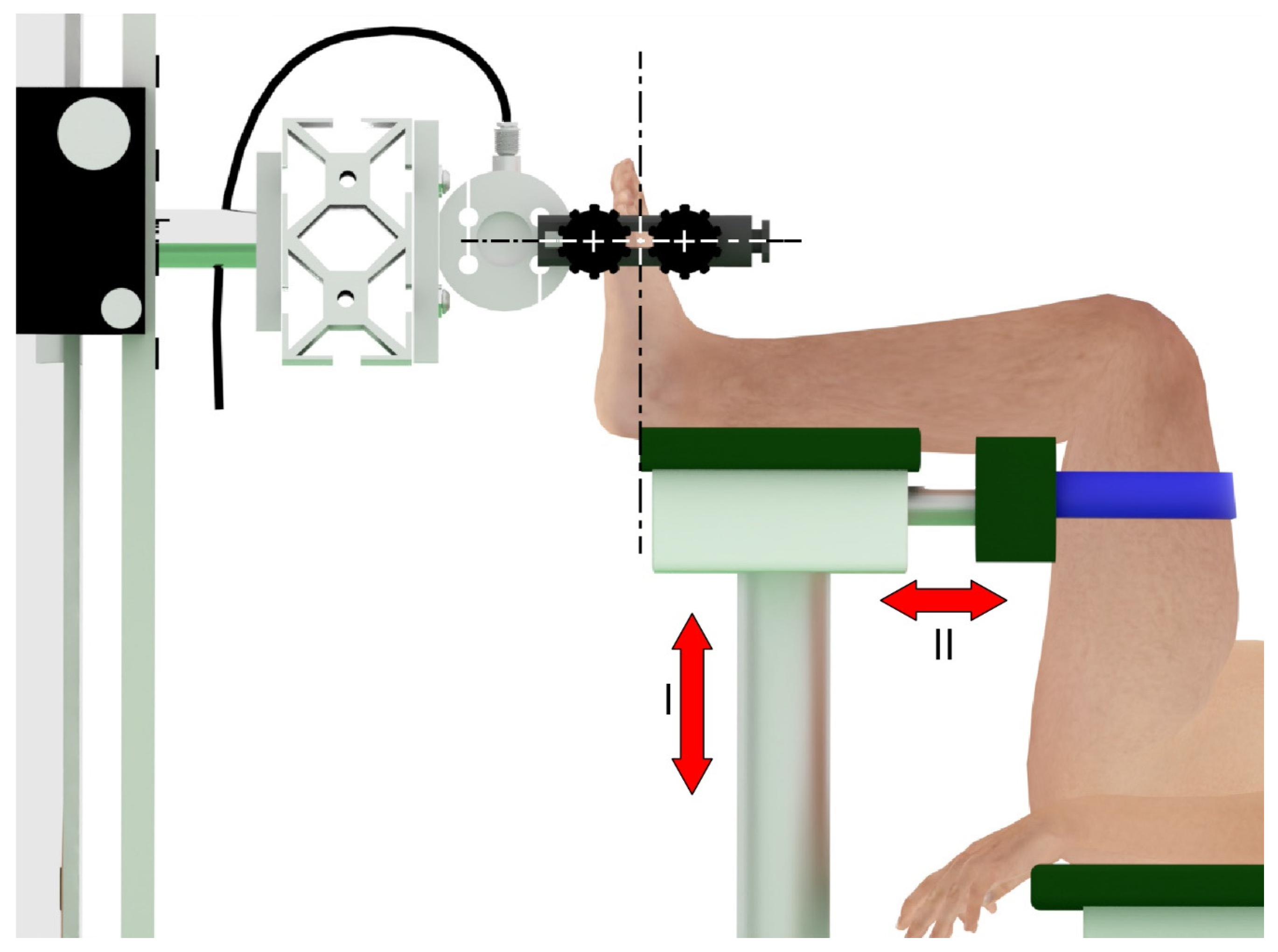
2.1. Experimental Setup
2.2. Repeatability Study
2.3. Pilot Study
3. Results
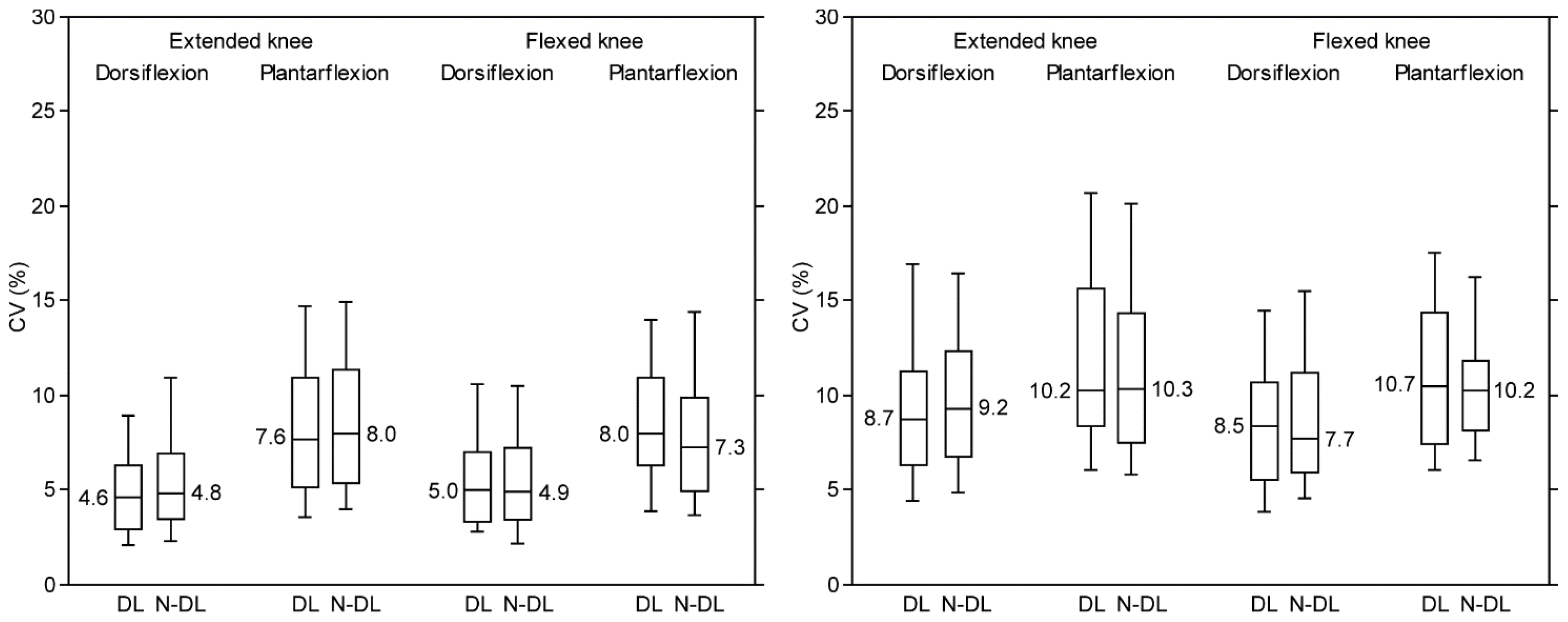
3.1. Repeatability Study
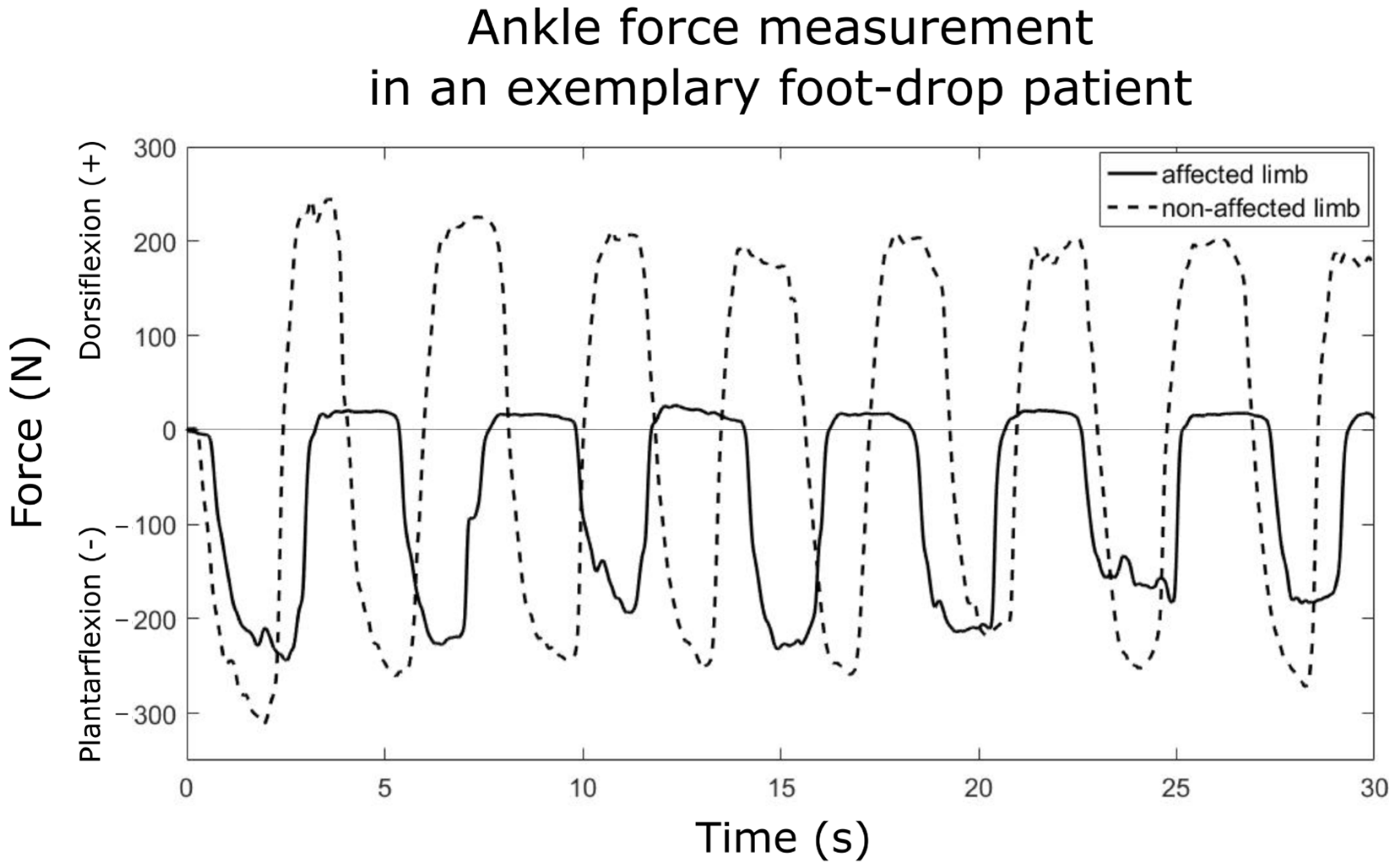
3.2. Pilot Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Additional Details about the AFT Design

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dominant Leg | Non-Dominant Leg | |
|---|---|---|
| Foot length (cm) | 25.4 ± 2.0 | 25.4 ± 2.0 |
| Foot width (cm) | 9.5 ± 0.7 | 9.6 ± 0.7 |
| 1st metatarsal–malleoli distance (cm) | 12.6 ± 0.7 | 12.8 ± 0.9 |
| 1st metatarsal–malleoli distance (%foot length) | 50 ± 2.0 | 50 ± 2.0 |
References
- Pirker, W.; Katzenschlager, R. Gait Disorders in Adults and the Elderly: A Clinical Guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Neptune, R.R.; Kautz, S.A.; Zajac, F.E. Contributions of the Individual Ankle Plantar Flexors to Support, Forward Progression and Swing Initiation during Walking. J. Biomech. 2001, 34, 1387–1398. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.H.; Cooper, L.; Daniel, D. The Role of the Ankle Plantar Flexors in Normal Walking. J. Bone Jt. Surg. Ser. A 1980, 62, 354–363. [Google Scholar] [CrossRef]
- Polkey, C.E. Book Reviews. In British Medical Bulletin; Oxford Academic: Oxford, UK, 1977; Volume 33, p. 182. [Google Scholar]
- Araújo, V.L.; Carvalhais, V.O.C.; Souza, T.R.; Ocarino, J.M.; Gonçalves, G.G.P.; Fonseca, S.T. Validity and Reliability of Clinical Tests for Assessing Passive Ankle Stiffness. Rev. Bras. Fisioter. 2011, 15, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Geboers, J.F.M.; Van Tuijl, J.H.; Seelen, H.A.M.; Drost, M.R. Effect of Immobilization on Ankle Dorsiflexion Strength. Scand. J. Rehabil. Med. 2000, 32, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Kejžar, L.; Kozinc, Ž.; Smajla, D.; Šarabon, N. Reference Values for Isometric Ankle Strength: A Scoping Literature Review and Comparison with Novel Data from 683 Athletes. Crit. Rev. Phys. Rehabil. Med. 2023, 35, 13–28. [Google Scholar] [CrossRef]
- Ancillao, A.; Palermo, E.; Rossi, S. Validation of Ankle Strength Measurements by Means of a Hand-Held Dynamometer in Adult Healthy Subjects. J. Sens. 2017, 2017, 5426031. [Google Scholar] [CrossRef]
- Moraux, A.; Canal, A.; Ollivier, G.; Ledoux, I.; Doppler, V.; Payan, C.; Hogrel, J.Y. Ankle Dorsi- and Plantar-Flexion Torques Measured by Dynamometry in Healthy Subjects from 5 to 80 Years. BMC Musculoskelet. Disord. 2013, 14, 104. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.; Thomas, M.; Bohannon, R.W. Normative Values for Isometric Muscle Force Measurements Obtained with Hand-Held Dynamometers. Phys. Ther. 1996, 76, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Xiong, R.; Sun, C.; Pang, M.; Xiang, K.; Ju, Z. Static Ankle Joint Stiffness Estimation with Relaxed Muscles through Customized Device. In Proceedings of the Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), Wuhan, China, 16–18 August 2017; pp. 485–493. [Google Scholar]
- Roy, A.; Krebs, H.I.; Williams, D.J.; Bever, C.T.; Forrester, L.W.; Macko, R.M.; Hogan, N. Robot-Aided Neurorehabilitation: A Novel Robot for Ankle Rehabilitation. IEEE Trans. Robot. 2009, 25, 569–582. [Google Scholar] [CrossRef]
- Rogati, G.; Caravaggi, P.; Leardini, A.; Erani, P.; Fognani, R.; Saccon, G.; Boriani, L.; Baleani, M. A Novel Apparatus to Assess the Mechanical Properties of Ankle-Foot Orthoses: Stiffness Analysis of the Codivilla Spring. J. Biomech. 2022, 142, 111239. [Google Scholar] [CrossRef] [PubMed]
- Van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to Determine Leg Dominance: The Agreement between Self-Reported and Observed Performance in Healthy Adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed]
- Maganaris, C.N.; Baltzopoulos, V.; Sargeant, A.J. Differences in Human Antagonistic Ankle Dorsiflexor Coactivation between Legs; Can They Explain the Moment Deficit in the Weaker Plantarflexor Leg? Exp. Physiol. 1998, 83, 843–855. [Google Scholar] [CrossRef] [PubMed]
- Vandervoort, A.A.; Chesworth, B.M.; Cunningham, D.A.; Paterson, D.H.; Rechnitzer, P.A.; Koval, J.J. Age and Sex Effects on Mobility of the Human Ankle. J. Gerontol. 1992, 47, M17–M21. [Google Scholar] [CrossRef] [PubMed]
- Caravaggi, P.; Zomparelli, A.; Rogati, G.; Baleani, M.; Fognani, R.; Cevolini, F.; Fanciullo, C.; Cinquepalmi, A.; Lullini, G.; Berti, L. Development of a Novel Passive-Dynamic Custom AFO for Drop-Foot Patients: Design Principles, Manufacturing Technique, Mechanical Properties Characterization and Functional Evaluation. Appl. Sci. 2022, 12, 4721. [Google Scholar] [CrossRef]
- Bartonek, Å.; Eriksson, M.; Gutierrez-Farewik, E.M. A New Carbon Fibre Spring Orthosis for Children with Plantarflexor Weakness. Gait Posture 2007, 25, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Waterval, N.F.J.; Brehm, M.A.; Harlaar, J.; Nollet, F. Individual Stiffness Optimization of Dorsal Leaf Spring Ankle–Foot Orthoses in People with Calf Muscle Weakness Is Superior to Standard Bodyweight-Based Recommendations. J. Neuroeng. Rehabil. 2021, 18, 97. [Google Scholar] [CrossRef] [PubMed]

| Condition. | Direction of Force | Side | AFT [N] | AFT [%BW] |
|---|---|---|---|---|
| Fully extended knee | Dorsiflexion | Dominant | 218 (145 296) * | 28.4 (11.3 35.9) * |
| Non-Dominant | 205 (133 281) *,^ | 27.8 (9.7 36.1) *,^ | ||
| Plantarflexion | Dominant | 201 (123 347) * | 29.5 (9.7 47.3) * | |
| Non-Dominant | 188 (106 318) *,^ | 24.0 (5.4 38.6) *,^ | ||
| Partially flexed knee | Dorsiflexion | Dominant | 206 (128 289) *,^ | 29.8 (11 37) *,^ |
| Non-Dominant | 195 (131 273) *,^ | 27.8 (8.8 34.7) *,^ | ||
| Plantarflexion | Dominant | 178 (116 316) *,^ | 27.5 (7.9 45.5) *,^ | |
| Non-Dominant | 167 (114 285) *,^ | 24.0 (7.5 36.1) *,^ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogati, G.; Caravaggi, P.; Martelli, A.; Fognani, R.; Leardini, A.; Baleani, M. Validation of a Simple Device for the Evaluation of Ankle Plantar- and Dorsi-Flexor Forces Consistent with Standard Clinical Evaluations. Appl. Sci. 2024, 14, 2461. https://doi.org/10.3390/app14062461
Rogati G, Caravaggi P, Martelli A, Fognani R, Leardini A, Baleani M. Validation of a Simple Device for the Evaluation of Ankle Plantar- and Dorsi-Flexor Forces Consistent with Standard Clinical Evaluations. Applied Sciences. 2024; 14(6):2461. https://doi.org/10.3390/app14062461
Chicago/Turabian StyleRogati, Giulia, Paolo Caravaggi, Andrea Martelli, Roberta Fognani, Alberto Leardini, and Massimiliano Baleani. 2024. "Validation of a Simple Device for the Evaluation of Ankle Plantar- and Dorsi-Flexor Forces Consistent with Standard Clinical Evaluations" Applied Sciences 14, no. 6: 2461. https://doi.org/10.3390/app14062461
APA StyleRogati, G., Caravaggi, P., Martelli, A., Fognani, R., Leardini, A., & Baleani, M. (2024). Validation of a Simple Device for the Evaluation of Ankle Plantar- and Dorsi-Flexor Forces Consistent with Standard Clinical Evaluations. Applied Sciences, 14(6), 2461. https://doi.org/10.3390/app14062461