

Interaction of Selected Commercial Antiseptics with Natural Products against Methicillin-Resistant Staphylococcus aureus Strain

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacterial Strain and Culture Conditions
2.2. Tested Substances
2.3. Dilutions of the Tested Substances
2.4. Determination of Effectiveness of the Tested Substances against MRSA Standard Strain
2.5. Determination of the Effectiveness of Combined Tested Substances against MRSA Standard Strain
2.6. Statistical Analysis
3. Results
3.1. Effectiveness of Tested Substances against MRSA Standard Strain
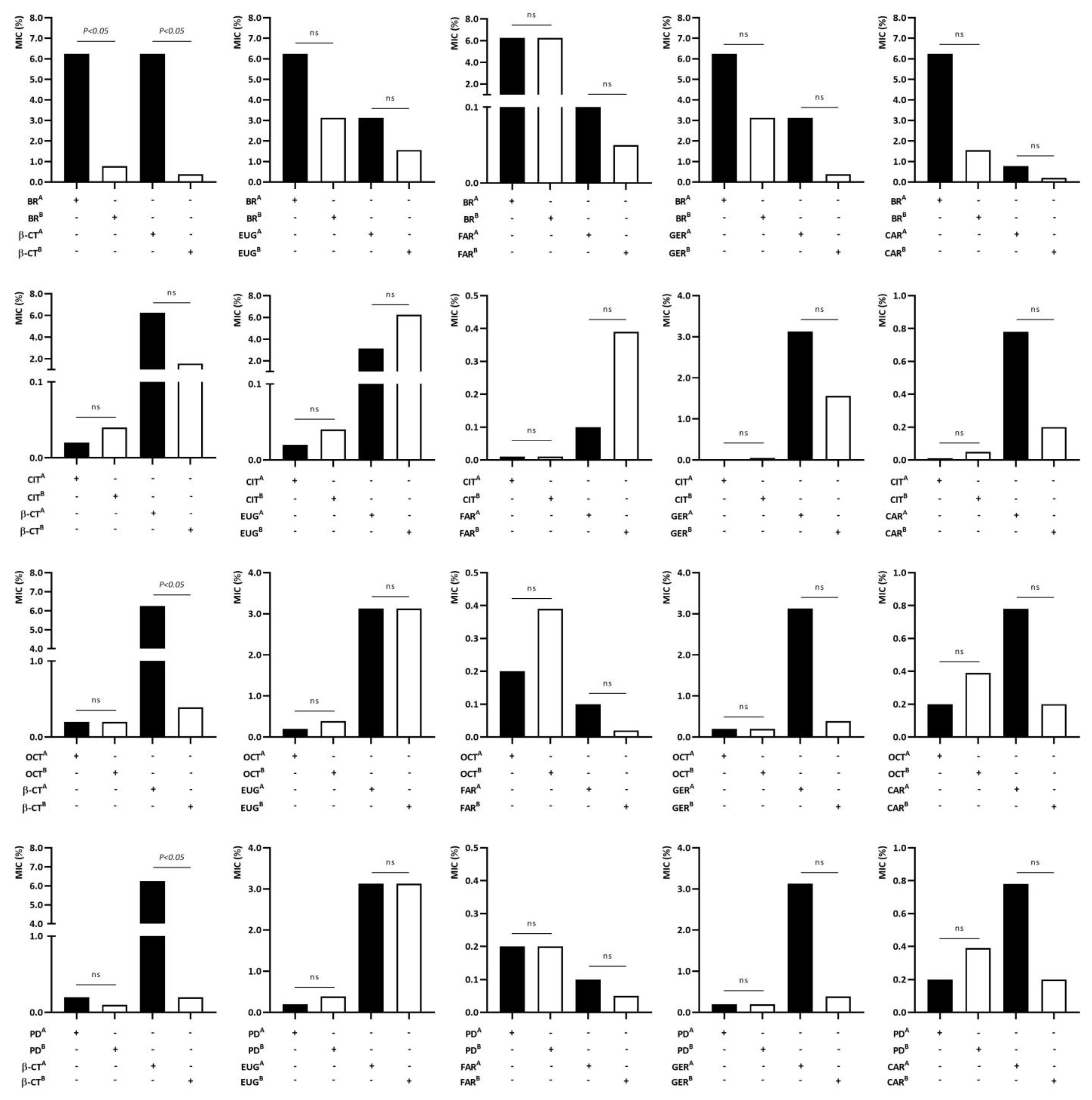
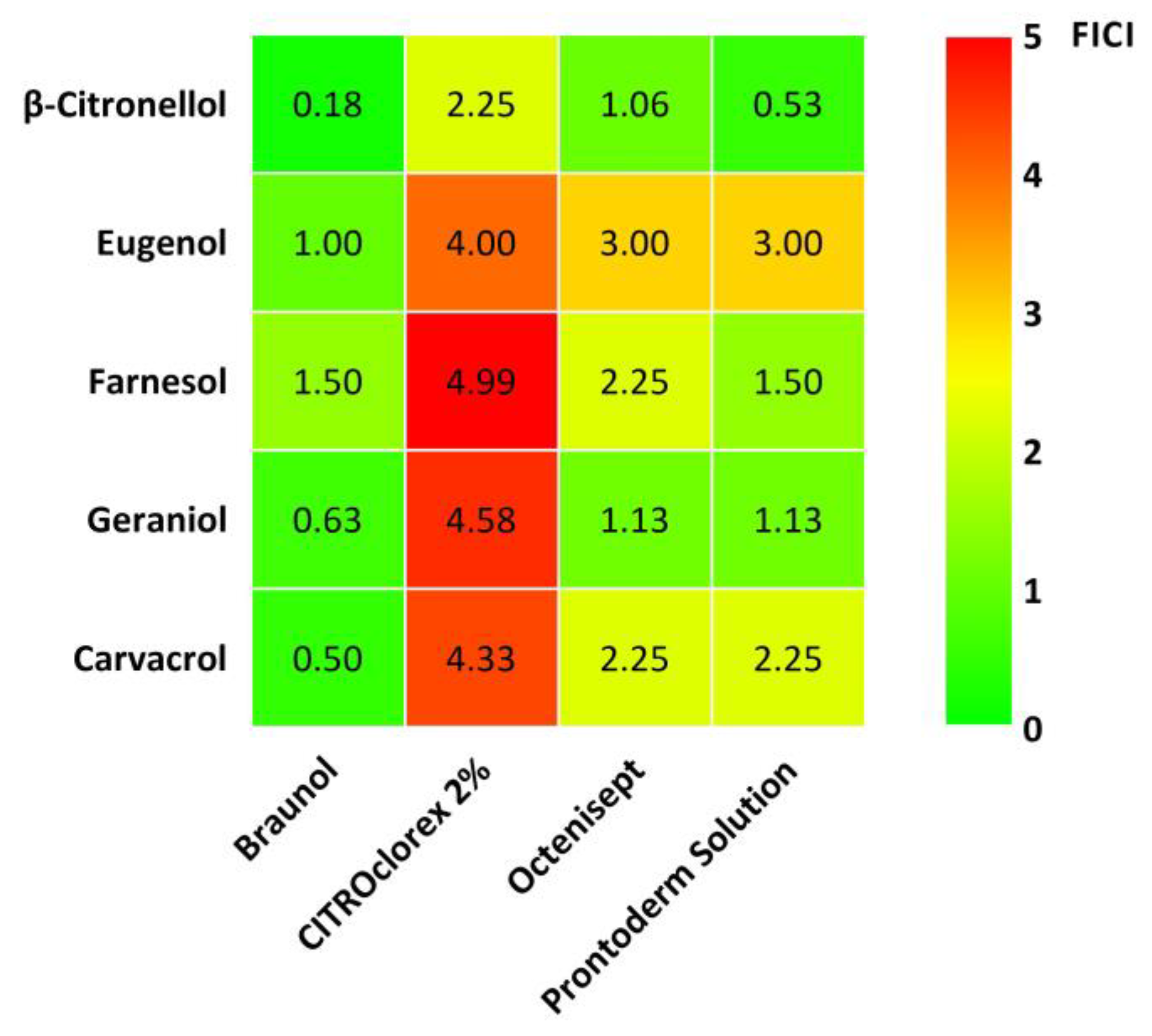
3.2. Analysis of Interaction of Commercial Antiseptics with Natural Products against MRSA Standard Strain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmad-Mansour, N.; Loubet, P.; Pouget, C.; Dunyach-Remy, C.; Sotto, A.; Lavigne, J.-P.; Molle, V. Staphylococcus aureus toxins: An update on their pathogenic properties and potential treatments. Toxins 2021, 13, 677. [Google Scholar] [CrossRef]
- Akinkunmi, E.O.; Lamikanra, A. Susceptibility of community associated methicillin resistant Staphylococcus aureus isolated from faeces to antiseptics. J. Infect. Dev. Ctries. 2012, 6, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Achraf, A.; Fatima Ezzahra, M.; Fatima Zahra, M.; Abdoullah, B.; Nour-Eddine, C.; Abdelhakim, E.; Eddine Jamal, J.; Mohamed, D. Antibacterial potent of acetylated and non-acetylated clove bud essential oils and their main compounds. Chem. Biodivers. 2023, 20, e202201034. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, P.; Łopusiewicz, Ł.; Kostek, M.; Drozłowska, E.; Pruss, A.; Wojciuk, B.; Sienkiewicz, M.; Zielińska-Bliźiewska, H.; Dołęgowska, B. The antibacterial activity of lavender essential oil alone and in combination with octenidine dihydrochloride against MRSA strains. Molecules 2020, 25, 95. [Google Scholar] [CrossRef]
- Frank, D.N.; Feazel, L.M.; Bessesen, M.T.; Prise, C.S.; Janoff, E.N.; Pace, N.R. The human nasal microbiota and Staphylococcus aureus carriage. PLoS ONE 2010, 5, e10598. [Google Scholar] [CrossRef]
- Flouchi, R.; Elmniai, A.; Hibatallah, A.; Fahsi, K.; Touzani, I.; Fikri-Benbrahim, K. The relationship between nasal carriage of Staphylococcus aureus and surgical site infections in a Hospital Center in Morocco. Int. J. Microbiol. 2021, 26, 5585588. [Google Scholar] [CrossRef] [PubMed]
- Steingrimsson, S.; Gottfredsson, M.; Kristinsson, K.G.; Gudbjartsson, T. Deep sternal wound infections following open heart surgery in Iceland: A population-based study. Scand. Cardiovasc. J. 2008, 42, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J. Best products for skin antisepsis. Am. J. Infect. Control 2019, 47S, A17–A22. [Google Scholar] [CrossRef]
- Lepelletier, D.; Maillard, J.Y.; Pozzetto, B.; Simon, A. Povidone iodine: Properties, mechanisms of action, and role in infection control and Staphylococcus aureus decolonization. Antimicrob. Agents Chemother. 2020, 64, e00682-20. [Google Scholar] [CrossRef]
- Bigliardi, P.L.; Alsagoff, S.A.L.; El-Kafrawi, H.Y.; Pyon, J.-K.; Wa, C.T.C.; Villa, M.A. Povidone iodine in wound healing: A review of current concepts and practices. Int. J. Surg. 2017, 44, 260–268. [Google Scholar] [CrossRef]
- Vercammen, Y.; Dauwe, D.; De Vlieger, G.; Houthoofd, S.; Desmet, L.; Casaer, M.P. Povidone iodine disinfection associated with hypothyroidism and potentially contributing to prolonged kidney failure. Case Rep. Crit. Care. 2021, 2021, 5528210. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Zhou, L.; Fan, C.; Wang, L.; Lin, X.; Wen, Y.; Su, L.; Dong, H. Bimetal-organic framework/GOx-based hydrogel dressings with antibacterial and inflammatory modulation for wound healing. Acta Biomater. 2023, 158, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, T.; Szkaradkiewicz, A. Chlorhexidine—Pharmaco-biological activity and application. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1321–1326. [Google Scholar] [PubMed]
- Kõljalg, S.; Naaber, P.; Mikelsaar, M. Antibiotic resistance as an indicator of bacterial chlorhexidine susceptibility. J. Hosp. Infect. 2002, 51, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Babalska, Z.; Korbecka-Paczkowska, M.; Karpiński, T. Wound antiseptics and European guidelines for antiseptic application in wound treatment. Pharmaceuticals 2021, 14, 1253. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, T. Efficacy of octenidine against Pseudomonas aeruginosa strains. Eur. J. Biol. Res. 2019, 9, 135–140. [Google Scholar]
- Bock, L.J.; Ferguson, P.M.; Clarke, M.; Pumpitakkul, V.; Wand, M.E.; Fady, P.-E.; Allison, L.; Fleck, R.A.; Shepherd, M.J.; Mason, A.J.; et al. Pseudomonas aeruginosa adapts to octenidine via a combination of efflux and membrane remodelling. Commun. Biol. 2021, 4, 1058. [Google Scholar] [CrossRef]
- Al-Doori, Z.; Goroncy-Bermes, P.; Gemmell, C.G.; Morrison, D. Low-level exposure of MRSA to octenidine dihydrochloride does not select for resistance. J. Antimicrob. Chemother. 2007, 59, 1280–1281. [Google Scholar] [CrossRef]
- Bührer, C.; Bahr, S.; Siebert, J.; Wettstein, R.; Geffers, C.; Obladen, M. Use of 2% 2-phenoxyethanol and 0.1% octenidine as antiseptic in premature newborn infants of 23–26 weeks gestation. J. Hosp. Infect. 2002, 51, 305–307. [Google Scholar] [CrossRef]
- Barusova, S.A.; Daurova, F. Antimicrobial preparation Octenisept efficacy study in treatment of inflammatory parodontal diseases. Stomatologiia 2009, 88, 45–49. [Google Scholar]
- Kampf, G. Antiseptic Stewardship: Biocide Resistance and Clinical Implications; Springer International Publishing: Cham, Switzerland, 2018. [Google Scholar]
- Huang, J.-M.; Ko, P.-J.; Huang, C.-L.; Wen, P.-W.; Chen, C.-H.; Shih, M.-H.; Linn, W.-C.; Huang, F.-C. Cytochrome P450 monooxygenase of Acanthamoeba castellanii participates in resistance to polyhexamethylene biguanide treatment. Parasite 2021, 28, 77. [Google Scholar] [CrossRef]
- Kaehn, K. Polihexanide: A safe and highly effective biocide. Skin Pharmacol. Physiol. 2010, 23, 7–16. [Google Scholar] [CrossRef]
- Block, M.S.; Rowan, B.G. Hypochlorous acid: A review. J. Oral Maxillofacial Sur. 2020, 78, 1461–1466. [Google Scholar] [CrossRef]
- Wang, L.; Bassiri, M.; Najafi, R.; Najafi, K.; Yang, J.; Khosrovi, B.; Hwong, W.; Barati, E.; Belisle, B.; Celeri, C.; et al. Hypochlorous acid as a potential wound care agent: Part I. Stabilized hypochlorous acid: A component of the inorganic armamentarium of innate immunity. J. Burns Wounds 2007, 6, e5. [Google Scholar]
- Susila, A.V.; Sai, S.; Sharma, N.; Balasubramaniam, A.; Veronica, A.K.; Nivedhitha, S. Can natural irrigants replace sodium hypochlorite? A systematic review. Clin. Oral Investig. 2023, 27, 1831–1849. [Google Scholar] [CrossRef]
- Soleimani, M.; Arzani, A.; Arzani, V.; Roberts, T.H. Phenolic compounds and antimicrobial properties of mint and thyme. J. Herb. Med. 2022, 36, 100604. [Google Scholar] [CrossRef]
- Bakkali, F.; Averbeck, S.; Averbeck, D.; Idaomar, M. Biological effects of essential oils—A review. Food Chem. Toxicol. 2008, 46, 446–475. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, G.L.S.; Bezerra, L.M.D.; Ribeiro, I.L.A.; Morais, R.C.D., Jr.; Castro, R.D. Susceptibility of cariogenic microorganisms to phytoconstituents. Braz. J. Biol. 2018, 78, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Freires, I.A.; Denny, C.; Benso, B.; de Alencar, S.M.; Rosalen, P.L. Antibacterial activity of essential oils and their isolated constituents against cariogenic bacteria: A systematic review. Molecules 2015, 20, 7329–7358. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, G.; Medici, A.; Maietti, S.; Radice, M.; Muzzoli, M.; Manfredini, S.; Braccioli, E.; Bruni, R. Composition and functional properties of the essential oil of amazonian basil, Ocimum micranthum Willd., Labiatae in comparison with commercial essential oils. J. Agric. Food Chem. 2004, 52, 3486–3491. [Google Scholar] [CrossRef] [PubMed]
- Burt, S. Essential oils: Their antibacterial properties and potential applications in foods—A review. Int. J. Food Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef]
- Methods for Dilution Antimicrobial Susceptibility Test for Bacteria that Grow Aerobically; Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2009; M07-A9.
- Präbst, K.; Engelhardt, H.; Ringgeler, S.; Hübner, H. Basic colorimetric proliferation assays: MTT, WST, and resazurin. Methods Mol. Biol. 2017, 1601, 1–17. [Google Scholar] [PubMed]
- Kwiatkowski, P.; Pruss, A.; Grygorcewicz, B.; Wojciuk, B.; Dołęgowska, B.; Gierdys-Kalemba, S.; Kochan, E.; Sienkiewicz, M. Preliminary study on the antibacterial activity of essential oils alone and in combination with gentamicin against extended-spectrum β-lactamase-producing and New Delhi metallo-β-lactamase-1-producing Klebsiella pneumoniae isolates. Microb. Drug Resist. 2018, 24, 1368–1375. [Google Scholar] [CrossRef]
- Mogana, R.; Adhikari, A.; Tzar, M.N.; Ramliza, R.; Wiart, C. Antibacterial activities of the extracts, fractions and isolated compounds from Canarium patentinervium Miq. against bacterial clinical isolates. BMC Complement. Med. Ther. 2020, 20, 55. [Google Scholar] [CrossRef]
- Yap, P.S.X.; Lim, S.H.E.; Hu, C.P.; Yiap, B.C. Combination of essential oils and antibiotics reduce antibiotic resistance in plasmid-conferred multidrug resistant bacteria. Phytomedicine 2013, 20, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Yang, J.; Ma, Y.; Xi, Z.; Ji, Y.; Ren, Q.; Ning, H.; Wang, S. Cotreatment with aspirin and azole drugs increases sensitivity of Candida albicans in vitro. Infect. Drug Resist. 2021, 14, 2027–2038. [Google Scholar] [CrossRef] [PubMed]
- El Dein, M.A.T.; Yassin, A.S.; El-Tayeb, O.; Kashef, M.T. Chlorhexidine leads to the evolution of antibiotic-resistant Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2349–2361. [Google Scholar] [CrossRef]
- Kampf, G. Biocidal agents used for disinfection can enhance antibiotic resistance in Gram-negative species. Antibiotics 2018, 7, 110. [Google Scholar] [CrossRef]
- Alimu, Y.; Kusuya, Y.; Yamamoto, T.; Arita, K.; Shigemune, N.; Takahashi, H.; Yaguchi, T. Mechanism of polyhexamethylene biguanide resistance in Purpureocillium lilacinum strains. Biocontrol Sci. 2022, 27, 117–130. [Google Scholar] [CrossRef]
- Dydak, K.; Junka, A.; Dydak, A.; Brożyna, M.; Paleczny, J.; Fijałkowski, K.; Kubielas, G.; Aniołek, O.; Bartoszewicz, M. In vitro efficacy of bacterial cellulose dressings chemisorbed with antiseptics against biofilm formed by pathogens isolated from chronic wounds. Int. J. Mol. Sci. 2021, 22, 3996. [Google Scholar] [CrossRef] [PubMed]
- Krasowski, G.; Junka, A.; Paleczny, J.; Czajkowska, J.; Makomaska-Szaroszyk, E.; Chodaczek, G.; Majkowski, M.; Migdał, P.; Fijałkowski, K.; Kowalska-Krochmal, B.; et al. In-vitro evaluation of polihexanide, octenidine and NaClO/HClO-based antiseptics against biofilm formed by wound pathogens. Membranes 2021, 11, 62. [Google Scholar] [CrossRef]
- Severing, A.-L.; Rembe, J.-D.; Koester, V.; Stuermer, E.K. Safety and efficacy profiles of different commercial sodium hypochlorite/hypochlorous acid solutions (NaClO/HClO): Antimicrobial efficacy, cytotoxic impact and physicochemical parameters in vitro. J. Antimicrob. Chemother. 2019, 74, 365–372. [Google Scholar] [CrossRef]
- Barakat, N.A.; Rasmy, S.A.; El-Dien, A.; Kashef, M.T. Effect of povidone-iodine and propanol-based mecetronium ethyl sulphate on antimicrobial resistance and virulence in Staphylococcus aureus. Antimicrob. Resist. Infect. Control 2022, 11, 139. [Google Scholar] [CrossRef] [PubMed]
- Koburger, T.; Hübner, N.-O.; Braun, M.; Siebert, J.; Kramer, A. Standardized comparison of antiseptic efficacy of triclosan, PVP–iodine, octenidine dihydrochloride, polyhexanide and chlorhexidine digluconate. J. Antimicrob. Chemother. 2010, 65, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Dittmann, K.; Schmidt, T.; Muller, G.; Cuny, C.; Holtfreter, S.; Troitzsch, D.; Pfaff, P.; Hubner, N.-O. Susceptibility of livestock-associated methicillin-resistant Staphylococcus aureus (LA-MRSA) to chlorhexidine digluconate, octenidine dihydrochloride, polyhexanide, PVP-iodine and triclosan in comparison to hospital-acquired MRSA (HA-MRSA) and community-acquired MRSA (CA-MRSA): A standardized comparison. Antimicrob. Resist. Infect. Control 2019, 8, 122. [Google Scholar] [PubMed]
- Hirsch, T.; Koerber, A.; Jacobsen, F.; Dissemond, J.; Steinau, H.-U.; Gatermann, S.; Al-Benna, S.; Kesting, M.; Seipp, H.-M.; Steinstraesser, L. Evaluation of toxic side effects of clinically used skin antiseptics in vitro. J. Surg. Res. 2010, 164, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Mulberry, G.; Snyder, A.T.; Heilman, J.; Pyrek, J.; Stahl, J. Evaluation of a waterless, scrubless chlorhexidine gluconate/ethanol surgical scrub for antimicrobial efficacy. Am. J. Infect. Control 2001, 29, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Dopcea, G.N.; Dopcea, I.; Nanu, A.E.; Diguţă, C.F.; Matei, F. Resistance and cross-resistance in Staphylococcus spp. strains following prolonged exposure to different antiseptics. J. Glob. Antimicrob. Resist. 2020, 21, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Gallego, I.; Infiesta, L.; Viedma, E.; Perez-Montarelo, D.; Chaves, F. Chlorhexidine and mupirocin susceptibilities in methicillin-resistant Staphylococcus aureus isolates from bacteraemia and nasal colonisation. J. Glob. Antimicrob. Resist. 2016, 4, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.; Ferguson, J. Phenotypic chlorhexidine and triclosan susceptibility in clinical Staphylococcus aureus isolates in Australia. Pathology 2017, 49, 633–637. [Google Scholar] [CrossRef]
- Cieplik, F.; Jakubovics, N.S.; Buchalla, W.; Maisch, T.; Hellwig, E.; Al-Ahmad, A. Resistance toward chlorhexidine in oral bacteria—Is there cause for concern? Front. Microbiol. 2019, 10, 587. [Google Scholar] [CrossRef]
- Sauerbrei, A. Bactericidal and virucidal activity of ethanol and povidone-iodine. Microbiologyopen 2020, 9, e1097. [Google Scholar] [CrossRef]
- Rozman, U.; Duh, D.; Cimerman, M.; Turk, S.S. Hygiene of medical devices and minimum inhibitory concentrations for alcohol-based and QAC disinfectants among isolates from physical therapy departments. Int. J. Environ. Res. Public Health 2022, 19, 14690. [Google Scholar] [CrossRef]
- Hołdrowicz, A.; Narbutt, J.; Pałczyński, C.; Kupryś-Lipińska, I.; Lesiak, A. Bullous skin lesion reaction as an example of an adverse effect of a preparation containing 0.1% octenidine dihydrochloride and 2% phenoxyethanol (Octenisept®). Dermatol. Rev. 2018, 105, 753–760. [Google Scholar] [CrossRef]
- Renzoni, A.; von Dach, E.; Landelle, C.; Diene, S.M.; Manzano, C.; Gonzales, R.; Abdelhady, W.; Randall, C.P.; Bonetti, E.J.; Baud, D.; et al. Impact of exposure of methicillin-resistant Staphylococcus aureus to polyhexanide in vitro and in vivo. Antimicrob. Agents Chemother. 2017, 61, e00272-17. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Tejedor, F.; González-García, P.; Mayordomo, R. Solubilization in vitro of tea tree oil and first results of antifungal effect in onychomycosis. Enferm. Infecc. Microbiol. Clin. 2020, 39, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Lopus, M. Nano-ayurvedic medicine and its potential in cancer treatment. J. Integr. Med. 2023, 21, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Bonikowski, R.; Świtakowska, P.; Sienkiewicz, M.; Zakłos-Szyda, M. Selected compounds structurally related to acyclic sesquiterpenoids and their antibacterial and cytotoxic activity. Molecules 2015, 20, 11272–11296. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Feng, K.; Zheng, Q.; Tan, W.; Zhong, W.; Liao, C.; Liu, Y.; Li, S.; Hu, W. Preparation and characterization of geraniol nanoemulsions and its antibacterial activity. Front. Microbiol. 2022, 13, 1080300. [Google Scholar] [CrossRef]
- Medeiros Leite, A.; de Oliveira Lima, E.; Leite de Souza, E.; de Fatima Formiga Melo Diniz, M.; Nogueira Trajano, V.; Almeida de Medeiros, I. Inhibitory effect of beta-pinene, alpha-pinene and eugenol on the growth of potential infectious endocarditis causing Gram-positive bacteria. Rev. Bras. Cienc. Farm. 2007, 43, 121–126. [Google Scholar] [CrossRef]
- El Atki, Y.; Aouam, I.; Taroq, A.; Kamari, F.; Timinouni, M.; Lyoussi, B.; Abdellaoui, A. Antibacterial effect of combination of cinnamon essential oil and thymol, carvacrol, eugenol, or geraniol. J. Rep. Pharm. Sci. 2020, 9, 104–109. [Google Scholar] [CrossRef]
- Mohammed, M.J.; Al-Bayati, F.A. Isolation and identification of antibacterial compounds from Thymus kotschyanus aerial parts and Dianthus caryophyllus flower buds. Phytomedicine 2009, 16, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Mulyaningsih, S.; Sporer, F.; Reichling, J.; Wink, M. Antibacterial activity of essential oils from Eucalyptus and of selected components against multidrug-resistant bacterial pathogens. Pharm. Biol. 2011, 49, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.; Lopez-Romero, J.C.; Oliveira, D.; Giaouris, E.; Simões, M. Prevention, removal and inactivation of Escherichia coli and Staphylococcus aureus biofilms using selected monoterpenes of essential oils. J. Appl. Microbiol. 2017, 123, 104–115. [Google Scholar] [CrossRef]
- Li, Q.; Yu, S.; Han, J.; Wu, J.; You, L.; Shi, X.; Wang, S. Synergistic antibacterial activity and mechanism of action of nisin/carvacrol combination against Staphylococcus aureus and their application in the infecting pasteurized milk. Food Chem. Toxicol. 2022, 380, 132009. [Google Scholar] [CrossRef]
- Heckler, C.; Sant’anna, V.; Brandelli, A.; Malheiros, P.S. Combined effect of carvacrol, thymol and nisin against Staphylococcus aureus and Salmonella Enteritidis. An. Acad. Bras. Cienc. 2021, 93, 20210550. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.M.; Patel, H.C. Systematic review and meta-analysis of preoperative antisepsis with combination chlorhexidine and povidone-iodine. Surg. J. 2016, 2, e70–e77. [Google Scholar] [CrossRef] [PubMed]
- Figueroa Roberto, R.; Andrew Rowan, F.; Nallur, D.; Durbin-Johnson, B.; Javidan, Y.; Otto Klineberg, E. Povidone-iodine irrigation combined with vancomycin powder lowers infection rates in pediatric deformity surgery. Spine Deform. 2021, 9, 1315–1321. [Google Scholar] [CrossRef] [PubMed]
- Noel, D.J.; Keevil, C.W.; Wilks, S.A. Synergism versus additivity: Defining the interactions between common disinfectants. mBio 2021, 12, e0228121. [Google Scholar] [CrossRef]
- Gottardi, W. The influence of the chemical behaviour of iodine on the germicidal action of disinfectant solutions containing iodine. J. Hosp. Infect. 1985, 6, 1–11. [Google Scholar] [CrossRef]
- Mohammadi Nejad, S.; Özgüneş, H.; Başaran, N. Pharmacological and toxicological properties of eugenol. Turk. J. Pharm. Sci. 2017, 14, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-M.; Ko, Y.J.; Lee, S.-B.; Jang, S.J. Adjuvant antimicrobial activity and resensitization efficacy of geraniol in combination with antibiotics on Acinetobacter baumannii clinical isolates. PLoS ONE 2022, 17, e0271516. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Pommel, L.; Bukiet, F.; About, I. Influence of the powder/liquid ratio on the properties of zinc oxide-eugenol-based root canal sealers. Dent. Mater. 2004, 20, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Slamenova, D.; Horváthová, E.; Sramková, M.; Marsálková, L. DNA-protective effects of two components of essential plant oils carvacrol and thymol on mammalian cells cultured in vitro. Neoplasma 2007, 54, 108–112. [Google Scholar]

{kind=link}
{kind=link}
| Substance | MIC (%) | MBC (%) | MBC/MIC Ratio | Effectiveness |
|---|---|---|---|---|
| Commercial antiseptics | ||||
| Braunol | 6.25 ± 0.00 | 12.5 ± 0.00 | 2 | BB |
| CITROclorex 2% | 0.01 ± 0.00 | 0.10 ± 0.00 | 8 | BS |
| Octenisept | 0.20 ± 0.00 | 1.56 ± 0.00 | 8 | BS |
| Prontoderm Solution | 0.20 ± 0.00 | 1.17 ± 0.55 | 6 | BS |
| Microdacyn 60 Wound Care | >50.0 | >50.0 | - | - |
| Natural products | ||||
| β-citronellol | 6.25 ± 0.00 | 6.25 ± 0.00 | 1 | BB |
| Eugenol | 3.13 ± 0.00 | 3.13 ± 0.00 | 1 | BB |
| Eucalyptol | >50.0 | >50.0 | - | - |
| Farnesol | 0.10 ± 0.00 | 0.78 ± 0.00 | 8 | BS |
| Geraniol | 3.13 ± 0.00 | 3.13 ± 0.00 | 1 | BB |
| Carvacrol | 0.78 ± 0.00 | 0.78 ± 0.00 | 1 | BB |
| Limonene | >50.0 | >50.0 | - | - |
| (-)-Menthone | >50.0 | >50.0 | - | - |
| Linalyl acetate | >50.0 | >50.0 | - | - |
| trans-Anethole | >50.0 | >50.0 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sienkiewicz, M.; Młodzińska, P.; Kilanowicz, A.; Dudzińska, E.; Kwiatkowski, P. Interaction of Selected Commercial Antiseptics with Natural Products against Methicillin-Resistant Staphylococcus aureus Strain. Appl. Sci. 2024, 14, 2060. https://doi.org/10.3390/app14052060
Sienkiewicz M, Młodzińska P, Kilanowicz A, Dudzińska E, Kwiatkowski P. Interaction of Selected Commercial Antiseptics with Natural Products against Methicillin-Resistant Staphylococcus aureus Strain. Applied Sciences. 2024; 14(5):2060. https://doi.org/10.3390/app14052060
Chicago/Turabian StyleSienkiewicz, Monika, Paulina Młodzińska, Anna Kilanowicz, Ewa Dudzińska, and Paweł Kwiatkowski. 2024. "Interaction of Selected Commercial Antiseptics with Natural Products against Methicillin-Resistant Staphylococcus aureus Strain" Applied Sciences 14, no. 5: 2060. https://doi.org/10.3390/app14052060
APA StyleSienkiewicz, M., Młodzińska, P., Kilanowicz, A., Dudzińska, E., & Kwiatkowski, P. (2024). Interaction of Selected Commercial Antiseptics with Natural Products against Methicillin-Resistant Staphylococcus aureus Strain. Applied Sciences, 14(5), 2060. https://doi.org/10.3390/app14052060