
Therapeutic Effectiveness of Postural Treatment on Youth Swimmers’ Anterior Shoulder Pain—An Interventional Study

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Design and Procedures
3. Measures
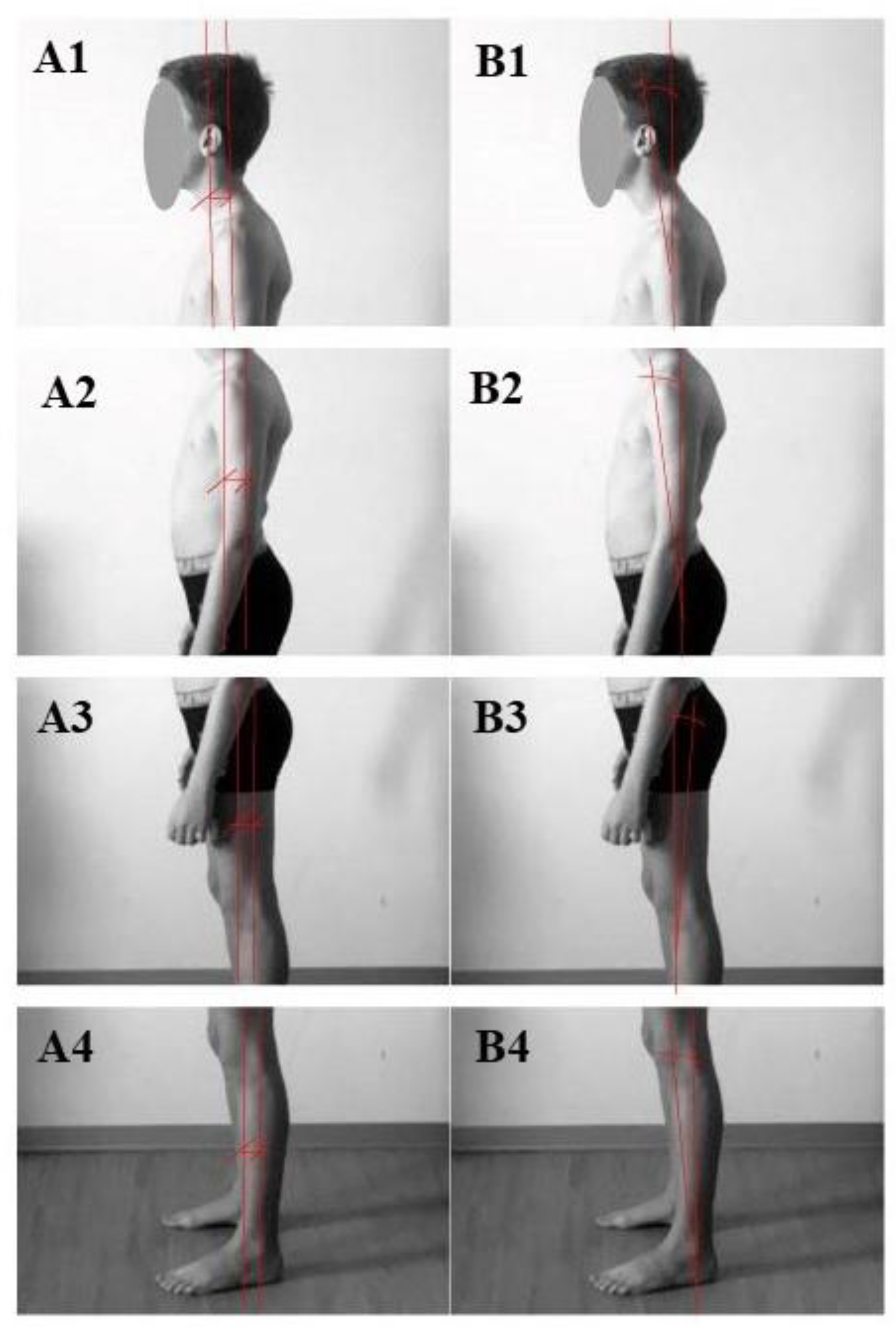
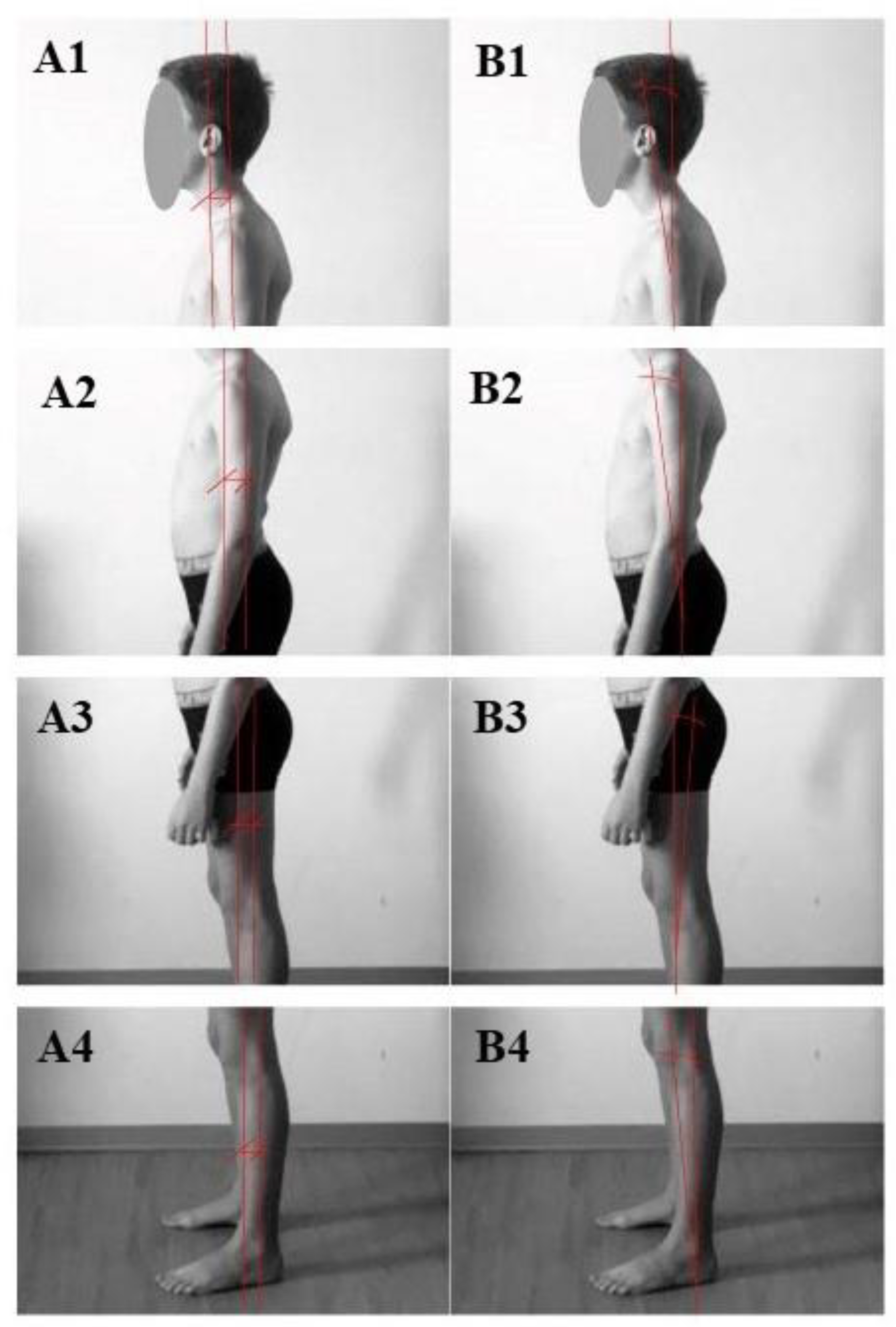
3.1. Standing Posture Analysis
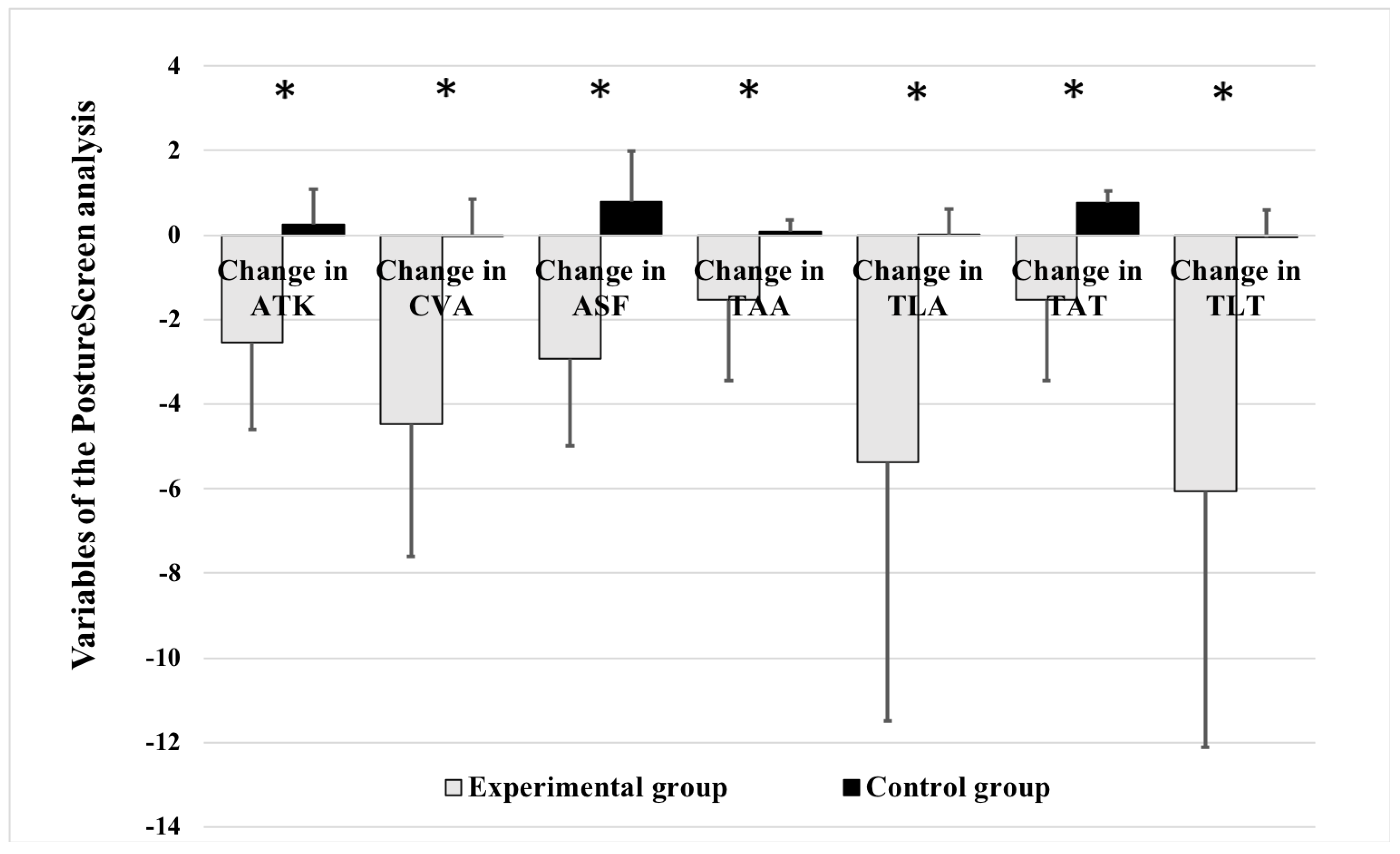
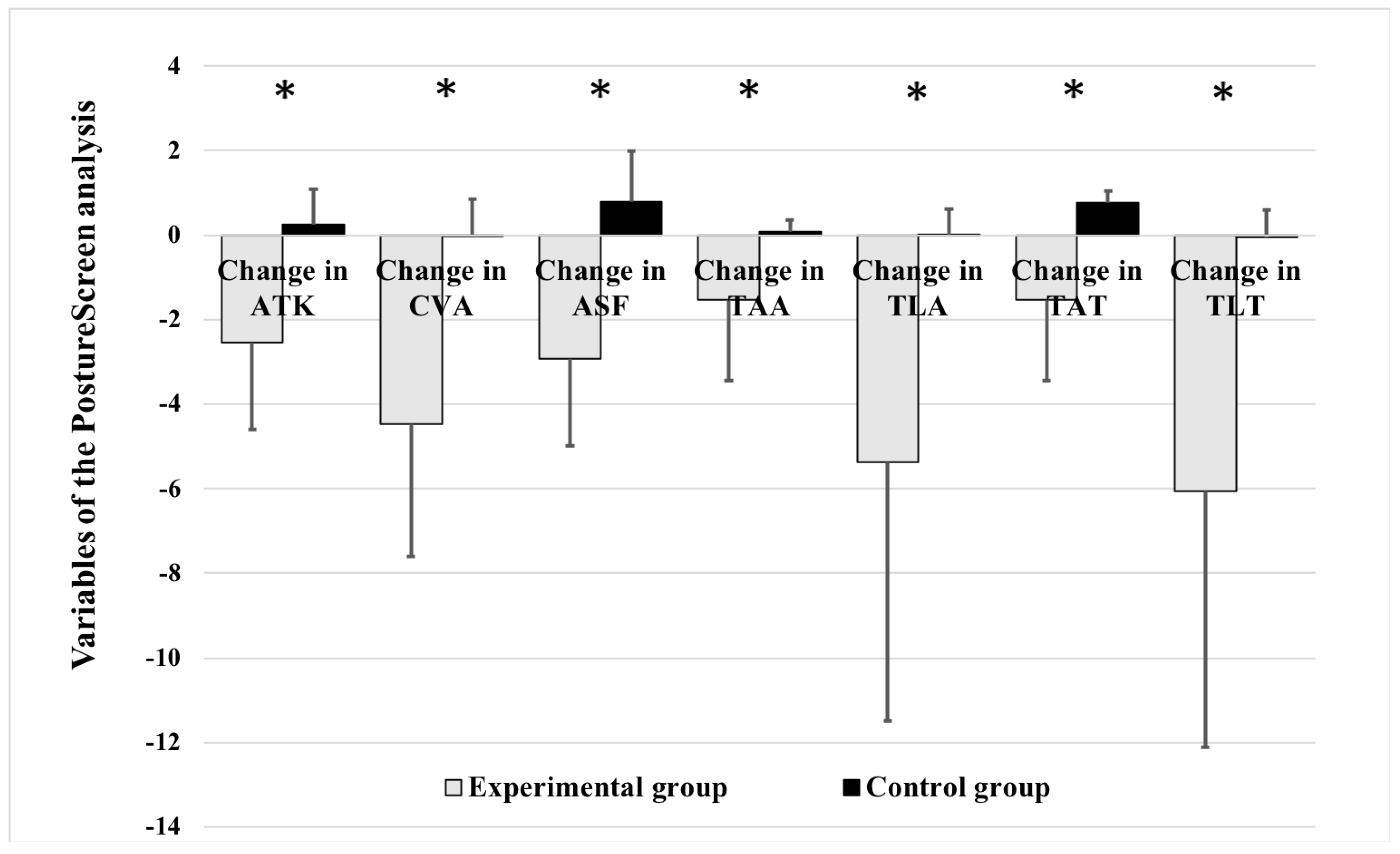
- Angulation of thoracic kyphosis (ATK): the convex curvature of the dorsal spine and normally is between 20 to 40 degrees [35]. It is also calculated by anatomical landmarks using the PSM algorithm.
- Cervicovertebral angulation (CVA): the angle formed by a horizontal line drawn through the seventh cervical (C7) vertebra and a line joining the C7 vertebra to the tragus of the ear. A smaller CVA indicates a greater forwards head posture. A CVA less than 48–50 is defined as forward head posture [36].
- Angulation of skull flexion (ASF): defined as the angle between the horizontal line drawn across the tragus and the line drawn from the corner of the eye to the tragus.
- Total anterior angulation (TAA): the total angulated deviations of different body parts in anterior view.
- Total lateral angulation (TLA): the total angulated deviations of different body parts in lateral view.
- Total anterior translation (TAT): the total translated deviation of different body parts in anterior view.
- Total lateral translation (TLT): is the total translated deviation of different body parts in lateral view.
3.2. The Swimmer’s Functional Pain Scale
3.3. Whole-Body Postural Correction (WBPC) Training
4. Statistical Analyses
5. Results
5.1. Anthropometric Characteristics and Swim Training Load of the Participants
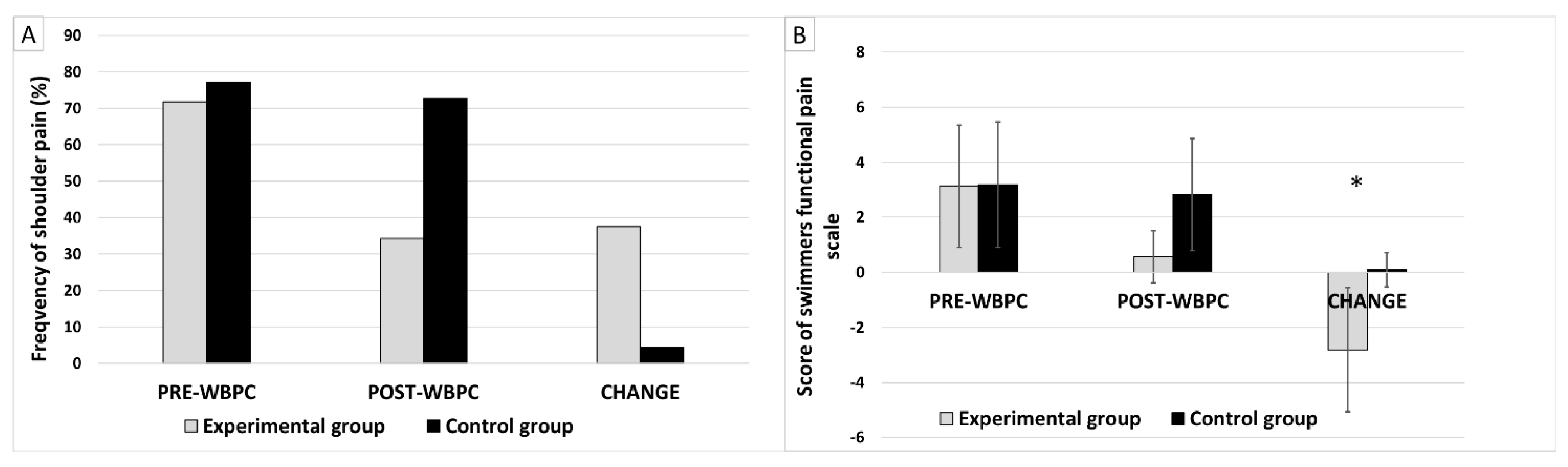
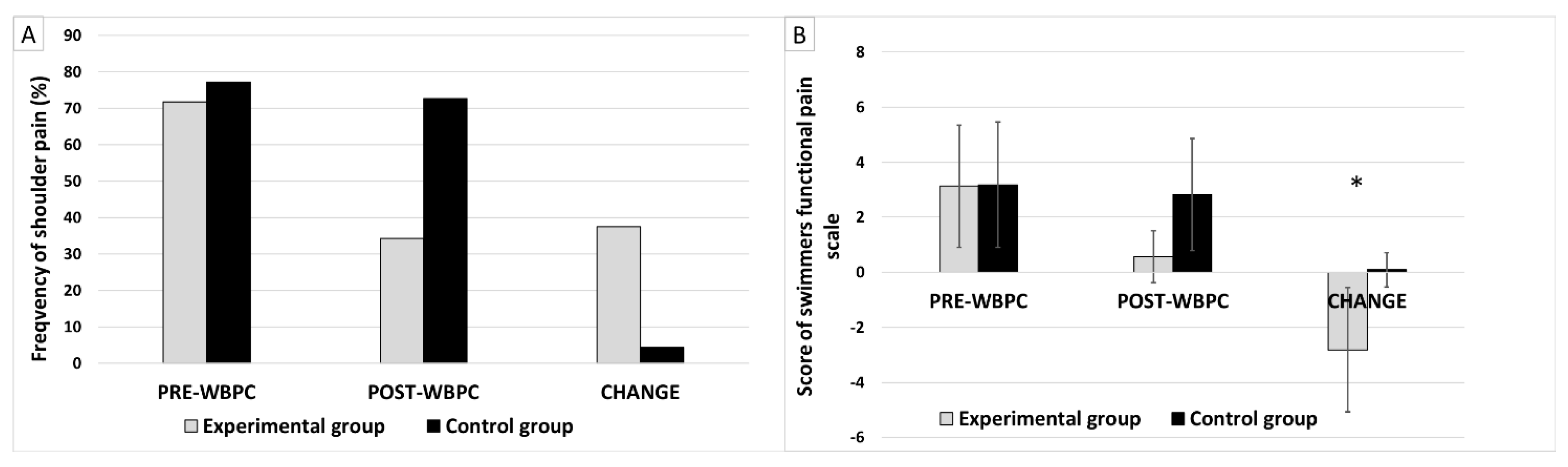
5.2. Results of the Swimmers Functional Pain Scale (SFPS)
5.3. Results of Posture Analysis
5.4. Correlation between Posture Analysis and Swimmers Functional Pain Scale (SFPS)
6. Discussion
7. Strengths and Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hashmi, A.; Waseem, A.; Jabeen, F.; Manzoor, S.; Batool, A.; Kamal, F. Disability associated with shoulder pain during the life span of competitive swimmers; A cross-sectional study. Heal. J. Physiother. Rehabil. Sci. 2022, 2, 139–145. [Google Scholar] [CrossRef]
- Tessaro, M.; Granzotto, G.; Poser, A.; Plebani, G.; Rossi, A. Shoulder Pain in Competitive Teenage Swimmers and It’s Prevention: A Retrospective Epidemiological Cross Sectional Study of Prevalence. Int. J. Sports Phys. Ther. 2017, 12, 798. [Google Scholar] [CrossRef]
- Dorssen, E.; Whiteley, R.; Mosler, A.; Ortega-Cebrian, S.; Dijkstra, P. Shoulder Injuries in Swimming—Meeting The Challenge. Aspetar Sports Med. 2014, 3, 571–580. [Google Scholar]
- Martins, L.; Paiva, J.R.M.; Freitas, A.C.T.; Miguel, L.B.; Maia, F.T. Prevalence of pain and associated factors in elite swimmers. Sci. Sports 2014, 29, e11–e14. [Google Scholar] [CrossRef]
- Thomas, S.J.; Blubello, A.; Peterson, A.; Blum, D.; Sarver, J.J.; Cobb, J.; Tate, A. Altered Functional and Stuctural Measures in Masters Swimmers With Shoulder Pain and Disability. J. Athl. Train. 2021, 56, 1313–1320. [Google Scholar] [CrossRef]
- Wanivenhaus, F.; Fox, A.M.; Chaudhury, S.; Rodeo, S.A. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health Multidiscip Approach 2012, 4, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Ostrander, T.; deGraauw, C.; Howarth, S.J.; Hogg-Johnson, S. Prevalence of shoulder problems in youth swimmers in Ontario. PubMed 2022, 66, 244–252. Available online: https://pubmed.ncbi.nlm.nih.gov/36818360 (accessed on 1 December 2022).
- Sein, M.S.; Walton, J.; Linklater, J.; Appleyard, R.; Kirkbride, B.; Kuah, D.; Murrell, G.A.C. Shoulder pain in Elite Swimmers: Primarily Due to Swim-volume.induced Supraspinatus Tendinopathy. Br. J. Sport. 2010, 44, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Tovin, B.J. Prevention and Treatment of Swimmer’s Shoulder. N. Am. J. Sports Phys. Ther. 2006, 1, 166–175. [Google Scholar]
- Feijen, S.; Struyf, T.; Kuppens, K.; Tate, A.; Struyf, F. Prediction of shoulder pain in Youth Competitive Swimmers: The development and internal validation of a Prognostic Prediction model. Am. J. Sports Med. 2020, 49, 154–161. [Google Scholar] [CrossRef]
- Bradley-Smith, E.-M. A Systematic Review of the Aetiology of Shoulder Injuries and the Associated Preventative Strategies within Competitive Swimmers. Bachelor’s Thesis, Doncaster Collage, Doncaster, UK, 2014. [Google Scholar]
- Feijen, S.; Tate, A.; Kuppens, K.; Struyf, T.; Claes, A.; Struyf, F. Interrater and Interrater Reliability of a Passive Shoulder Flexion Range of Motion Measurement for Latisimus Dorsi Flexibility in Young Competitive Swimmers. J. Sport Rehabil. 2020, 29, 855–858. [Google Scholar] [CrossRef]
- McKenzie, A.; Larequi, S.-A.; Hams, A.; Headrick, J.; Whiteley, R.; Duhig, S. Shoulder pain and injury risk factors in competitive swimmers: A systematic review. Scand. J. Med. Sci. Sports 2023, 33, 2396–2412. [Google Scholar] [CrossRef]
- Naderi, A.; Bagheri, S.; Rezvani, M.H. Comparison of Shoulder Posture and Scapular Kinematic among Swimmers with and without Shoulder Pain. Int. J. Health Stud. 2019, 5, 31–34. [Google Scholar]
- Tate, A.; Turner, G.N.; Knab, S.E.; Jorgensen, C.; Strittmatter, A.P.; Michener, L.A. Risk factors associated with shoulder pain and disability across the lifespan of competitive swimmers. J. Athl. Train. 2012, 47, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Kluemper, M.; Uhl, T.L.; Hazelrigg, H. Effect of stretching and strengthening shoulder muscles on forward shoulder posture in competitive swimmers. J. Sport Rehabil. 2006, 15, 58–70. [Google Scholar] [CrossRef]
- Lynch, S.S.; Thigpen, C.A.; Mihalik, J.; Prentice, W.E.; Padua, D. The effect of an exercise intervention on forward head and rounded shoulder postures is elite swimmers. Br. J. Sports Med. 2010, 44, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Kendall, F.P.; McCreary, E.K.; Kendall, H.O. Muscles, Testing and Function, 3rd ed.; Williams & Wilkins: Baltimore, MD, USA, 1983. [Google Scholar]
- McLaine, S.J.; Bird, M.; Ginn, K.A.; Hartley, T.F.; Fell, J.W. Shoulder extension strength: A potential risk factor for shoulder pain in young swimmers? J. Sci. Med. Sport 2019, 22, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Drigny, J.; Gauthier, A.; Reboursière, E.; Guermont, H.; Grémeaux, V.; Édouard, P. Shoulder muscle imbalance as a risk for shoulder injury in elite adolescent swimmers: A prospective study. J. Hum. Kinet. 2020, 75, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Barassi, G.; Di Simone, E.; Supplizi, M.; Prosperi, L.; Marinucci, C.; Pellegrino, R.; Galasso, P.; Guerri, S.; Della Rovere, M.; Younes, A.; et al. Bio-Physico-Metric approach: Integrated postural assessment in musculoskeletal dysfunctions. J. Biol. Regul. Homeost. Agents 2022, 36, 129–135. [Google Scholar] [CrossRef]
- Saggini, R.; Anastasi, G.P.; Battilomo, S.; Maietta Latessa, P.; Costanzo, G.; Di Carlo, F.; Festa, F.; Giardinelli, G.; Macrì, F.; Mastropasqua, L.; et al. Consensus paper on postural dysfunction: Recommendations for prevention, diagnosis and therapy. J. Biol. Regul. Homeost. Agents 2021, 35, 441–456. [Google Scholar] [CrossRef] [PubMed]
- Botha, C.; Rossouw, F.; Meyer, P.; Camacho, T. Comparative upper-quarter posture analysis of female adolescent freestyle swimmers and non-swimmers. Eur. J. Sport Sci. 2022, 23, 36–43. [Google Scholar] [CrossRef]
- Bak, K. The Practical Management of Swimmer’s Painful Shoulder: Etiology, Diagnosis, and Treatment. Clin. J. Sport Med. 2010, 20, 386–390. [Google Scholar] [CrossRef]
- Senthil, P.; Sudhakar, S.; Porcelvan, S.; Tgt, F.; Rathnamala, D.; Radhakrishnan, R. Implication of Posture Analysing Software to Evaluate the Postural Changes after Corrective Exercise Strategy on Subjects with Upper Body Dysfunction-A Randomized Controlled Trial. J. Clin. Diagn. Res. 2017, 11, YC01–YC04. [Google Scholar] [CrossRef] [PubMed]
- Kaliyaperumal, A.B.; Sekar, K.; Manickavelu, P.; Senthilmurugan, S. Effect of Muscle Energy Technique and Stabilization Exercise on Forward Neck and Rounded Shoulder for Elite Swimmers. Indian J. Physiother. Occup. Ther.-Int. J. 2023, 17, 1–6. [Google Scholar] [CrossRef]
- Almeida, G.P.L.; Souza, V.M.; Barbosa, G.; Santos, M.B.; Saccol, M.F.; Cohen, M. Swimmer’s shoulder in young athlete: Rehabilitation with emphasis on manual therapy and stabilization of shoulder complex. Man. Ther. 2011, 16, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Aspenes, S.T.; Karlsen, T. Exercise-Training Intervention studies in competitive swimming. Sports Med. 2012, 42, 527–543. [Google Scholar] [CrossRef] [PubMed]
- Hibberd, E.; Oyama, S.; Spang, J.T.; Prenzice, W.; Myers, J.B. Effect of a 6-week Strenghtening Program on Shoulder and Scapular-Stabilizer Strength and Scapular Kinematics in Division I Collegiate Swimmers. J. Sport Rehabil. 2012, 21, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.W. Medical care of the aquatics athlete. Curr. Sports Med. Rep. 2015, 14, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Ruivo, R.M.; Pedro Pezarat-Correia, P.; Carita, A.I. Effects of a Resistance and Stretching Training Program on Forward Head and Protracted Shoulder Posture in Adolescents. J. Manip. Physiol. Ther. 2016, 40, 1–10. [Google Scholar] [CrossRef]
- Sousa, J.P.; Malta, J.; Carrageta, A.; Batalha, N. Effect of a compensatory dry-land training program on shoulder posture and scapular position of competitive female swimmers. Rev. Investig. Act. Acuáticas 2019, 3, 45–52. [Google Scholar] [CrossRef]
- Boland, D.M.; Neufeld, E.V.; Ruddell, J.; Dolezal, B.A.; Cooper, C.B. Inter- and intra-rater agreement of static posture analysis using a mobile application. J. Phys. Ther. Sci. 2016, 28, 3398–3402. [Google Scholar] [CrossRef]
- Szucs, K.A.; Donoso, E.A. Rater reliability and construct validity of a mobile application for posture analysis. J. Phys. Ther. Sci. 2018, 30, 31–36. [Google Scholar] [CrossRef]
- Lewis, J.S.; Valentine, R.E. Clinical measurement of the thoracic kyphosis. A study of the intra-rater reliability in subjects with and without shoulder pain. BMC Musculoskelet Disord. 2010, 11, 39. [Google Scholar] [CrossRef]
- Verma, S.L.; Shaikh, J.; Mahato, R.K.; Sheth, M.S. Prevalence of forward head posture among 12–16 year old school going students: A cross sectional study. Appl. Med. Res. 2018, 4, 18–21. [Google Scholar] [CrossRef]
- Drake, S.M.; Krabak, B.; Edelman, G.T.; Pounders, E.; Robinson, S.; Wixson, B. Development and validation of a s Swimmer’s Functional Pain Scale. J. Swim. Res. 2015, 23, 21–32. [Google Scholar]
- Krüger, K.; Stüwer, K.; Michaud, M. An Evidence-based Shoulder Injury Prevention Intervention for Competitive Swimmers. Professional Assignment Project III-2. 2010. Available online: https://www.semanticscholar.org/paper/A-evidence-based-shoulder-injury-prevention-for-Kruger-Stuwer/cf9725fd4adec88204d08a82bc3ac60c0f93e847 (accessed on 1 December 2022).
- Lenhard, W.; Lenhard, A. Computation of Effect Sizes. Psychometrica. 2022. Available online: https://www.psychometrica.de/effect_size.html (accessed on 1 December 2022).
- Akyurek, E.; Alpözgen, A.Z.; Akgül, T. The preliminary results of physiotherapy scoliosis-specific exercises on spine joint position sense in adolescent idiopathic scoliosis: A randomized controlled trial. Prosthet. Orthot. Int. 2022, 46, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Tokgüz, G.; Aydin, Ö. Comparison of Body Posture Analysis of 11-13 Year Old Soccer Players and Handball Players. J. Glob. Sport Educ. Res. 2022, 2, 87–97. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| 1st Session | 2nd Session | 3rd Session | |
|---|---|---|---|
| Training period (week) | 8 | 8 | 8 |
| Training frequency (times/week) | 3 | 3 | 3 |
| Training duration (min/day) | 30 | 30 | 30 |
| Content of intervention training | 1a: core strengthening: abdominal, paravertebral and gluteal exercises | 1a: same as 1st session | 1a: core strengthening:abdominal, paravertebral and gluteal exercises with fitball |
| 1b: shoulder strengthening: scapular retraction and depression exercises and complex shoulder workout (m.trap.med and inf., m.serratus ant., mm.rhomboidei, m.delt., mm.rotator cuff) | 1b: same exercises with resistance band | 1b: same as 2nd session | |
| 2: core stability exercises | 2: core stability exercises with movements of extremities and trunk | 2: core stability exercises with fitball | |
| 3: stretching exercises m.trap.sup., m.lat.dorsi, mm.pect | 3: same as 1st session | 3: same as 1st session | |
| Sets/reps or Set/duration | 1a–1b: 3/20 2: 5/30 s 3: 3/30 s | 1a–1b: 3/20 2: 5/30 s 3: 3/30 s | 1a–1b: 3/20 2: 5/30 s 3: 3/30 s |
| Rest between sets (s) | 30 | 30 | 30 |
| EXP (n = 32) | CON (n = 22) | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p Value | |
| Age (years) | 13.80 | 1.89 | 14.04 | 1.67 | 0.636 |
| Height (cm) | 169.18 | 8.77 | 166.07 | 9.42 | 0.227 |
| Weight (kg) | 56.93 | 11.62 | 56.54 | 11.58 | 0.902 |
| BMI (kg/m2) | 19.72 | 2.60 | 20.27 | 2.54 | 0.446 |
| Years of swimming | 6.93 | 1.79 | 7.04 | 2.05 | 0.843 |
| Training duration (min/day) | 105.00 | 15.24 | 103.63 | 15.28 | 0.749 |
| Change in ATK | Change in CVA | Change of ASF | Change of TAA | Change of TLA | Change of TAT | Chang of TLT | |
|---|---|---|---|---|---|---|---|
| Change of SFPS score | r = 0.438 | r = 0.448 | r = 0.498 | r = 0.189 | r = 0.230 | r = 0.415 | r = 0.280 |
| p value | p < 0.001 ** | p < 0.000 ** | p < 0.001 ** | p = 0.174 | p = 0.098 | p = 0.002 * | p = 0.042 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabó, D.; Kiss, G.; Tékus, E.; Mayer, P.; Váczi, M.; Fekete, J.D.; Novográdecz, G.; Lázár, I.; Gocze, K.; Vermes, C.; et al. Therapeutic Effectiveness of Postural Treatment on Youth Swimmers’ Anterior Shoulder Pain—An Interventional Study. Appl. Sci. 2024, 14, 1486. https://doi.org/10.3390/app14041486
Szabó D, Kiss G, Tékus E, Mayer P, Váczi M, Fekete JD, Novográdecz G, Lázár I, Gocze K, Vermes C, et al. Therapeutic Effectiveness of Postural Treatment on Youth Swimmers’ Anterior Shoulder Pain—An Interventional Study. Applied Sciences. 2024; 14(4):1486. https://doi.org/10.3390/app14041486
Chicago/Turabian StyleSzabó, Dorottya, Gabriella Kiss, Eva Tékus, Petra Mayer, Márk Váczi, Judit Diana Fekete, Gergely Novográdecz, István Lázár, Katalin Gocze, Csaba Vermes, and et al. 2024. "Therapeutic Effectiveness of Postural Treatment on Youth Swimmers’ Anterior Shoulder Pain—An Interventional Study" Applied Sciences 14, no. 4: 1486. https://doi.org/10.3390/app14041486
APA StyleSzabó, D., Kiss, G., Tékus, E., Mayer, P., Váczi, M., Fekete, J. D., Novográdecz, G., Lázár, I., Gocze, K., Vermes, C., & Mintál, T. (2024). Therapeutic Effectiveness of Postural Treatment on Youth Swimmers’ Anterior Shoulder Pain—An Interventional Study. Applied Sciences, 14(4), 1486. https://doi.org/10.3390/app14041486