


Are Clinical Balance Measures Linked to Cycling Performance?
 , , and
, , and
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Setup and Procedure
2.1.1. Balance Error Scoring System (BESS)
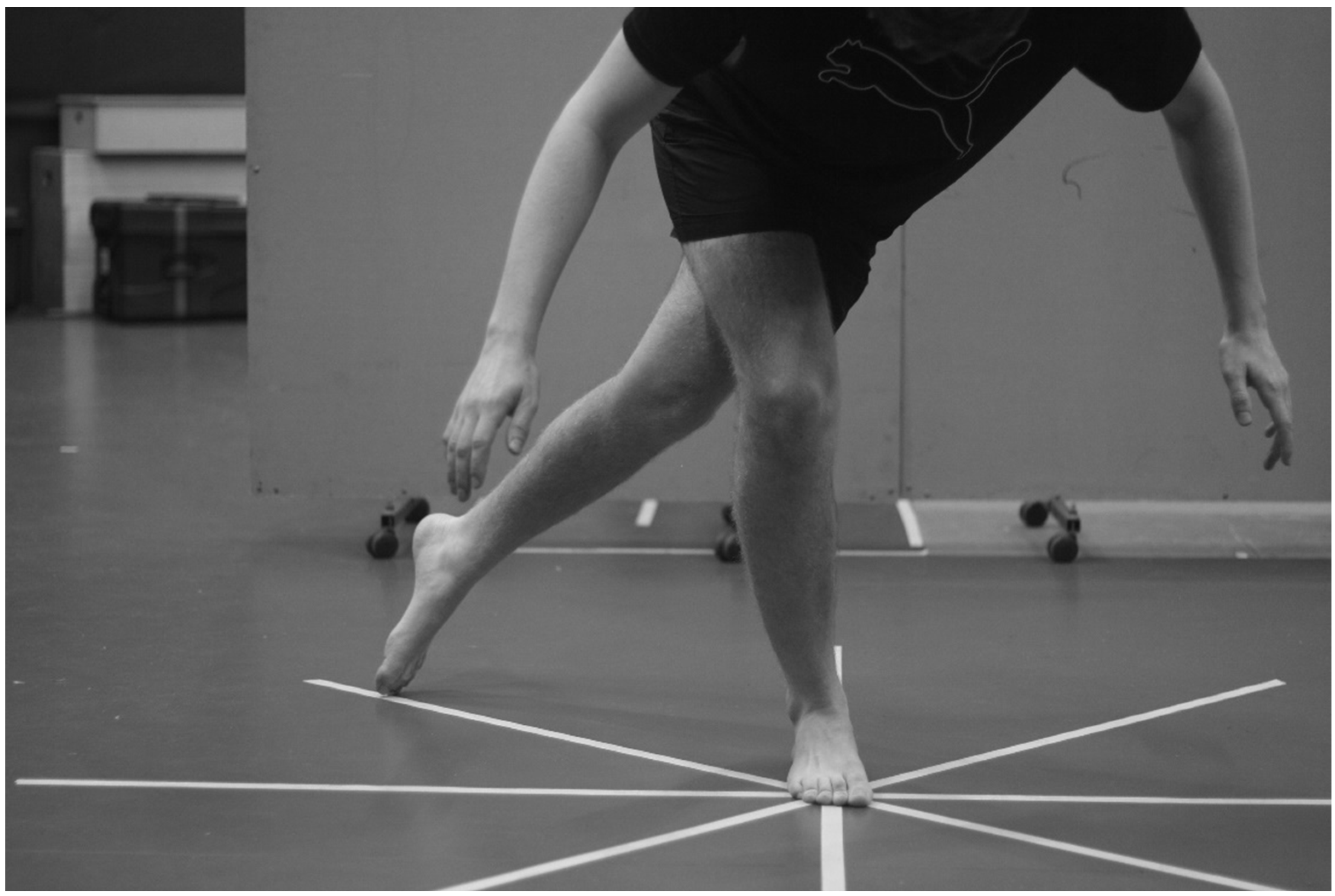
2.1.2. Star Excursion Balance Test (SEBT)
2.1.3. The Lateral Reach Test (LRT)
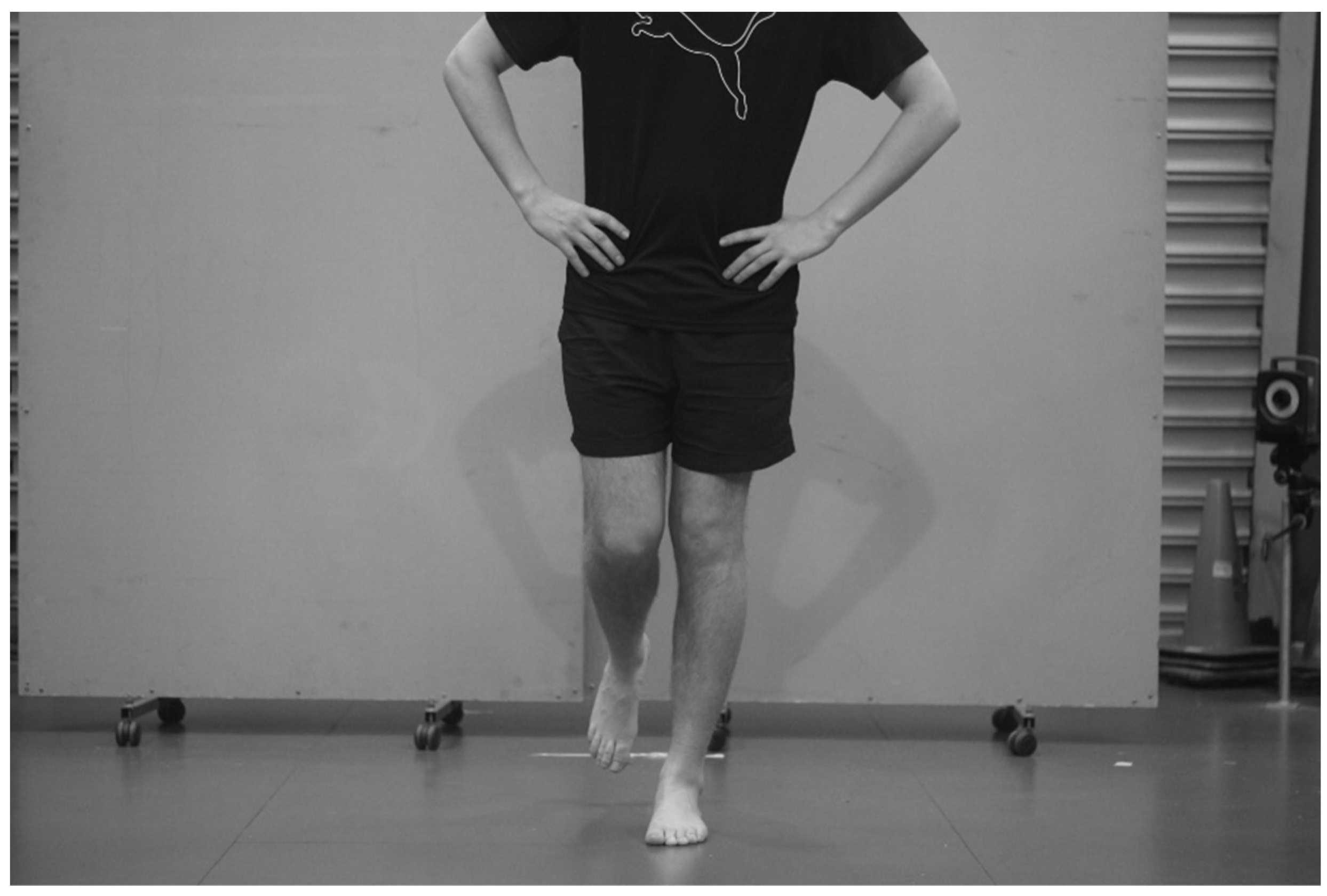
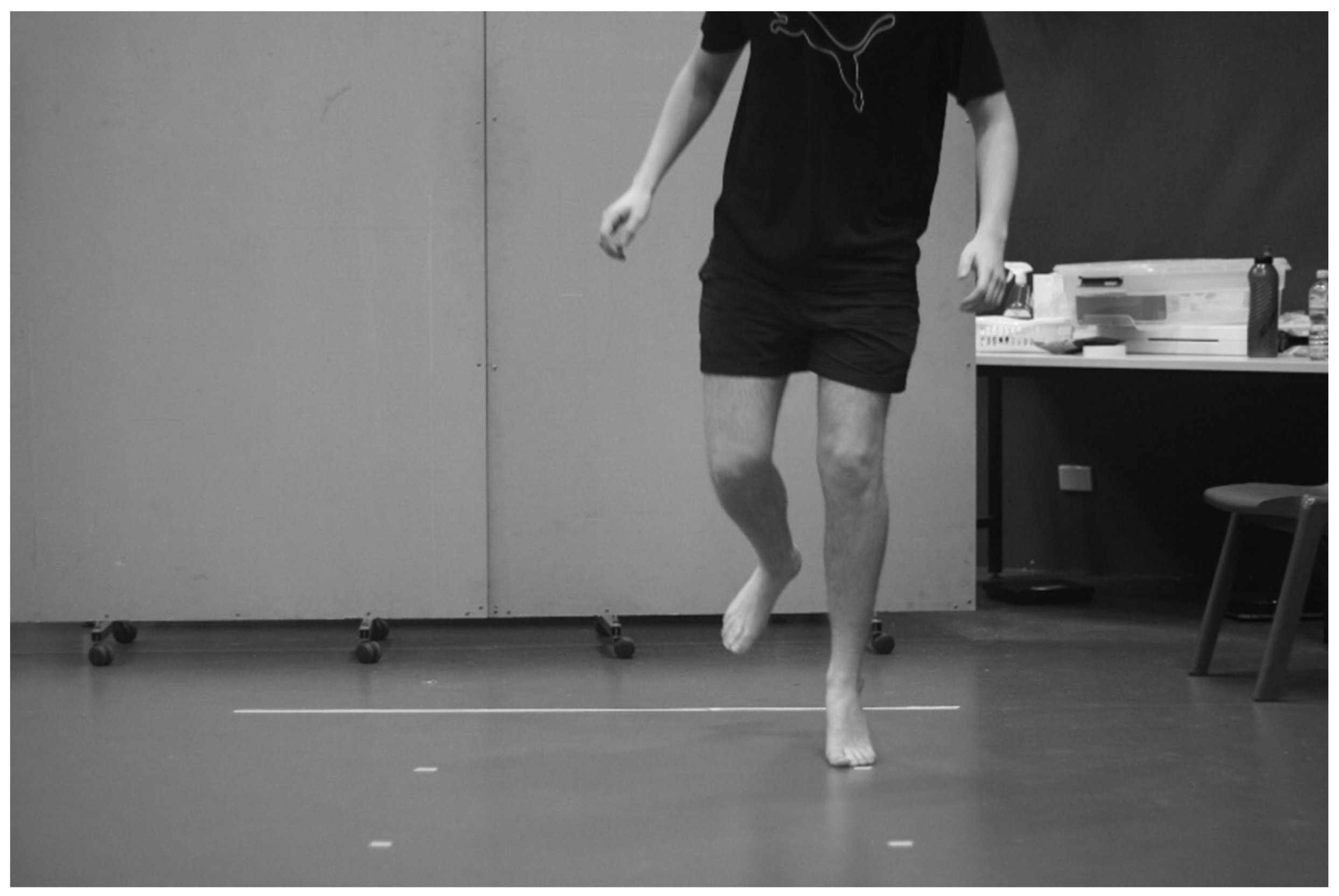
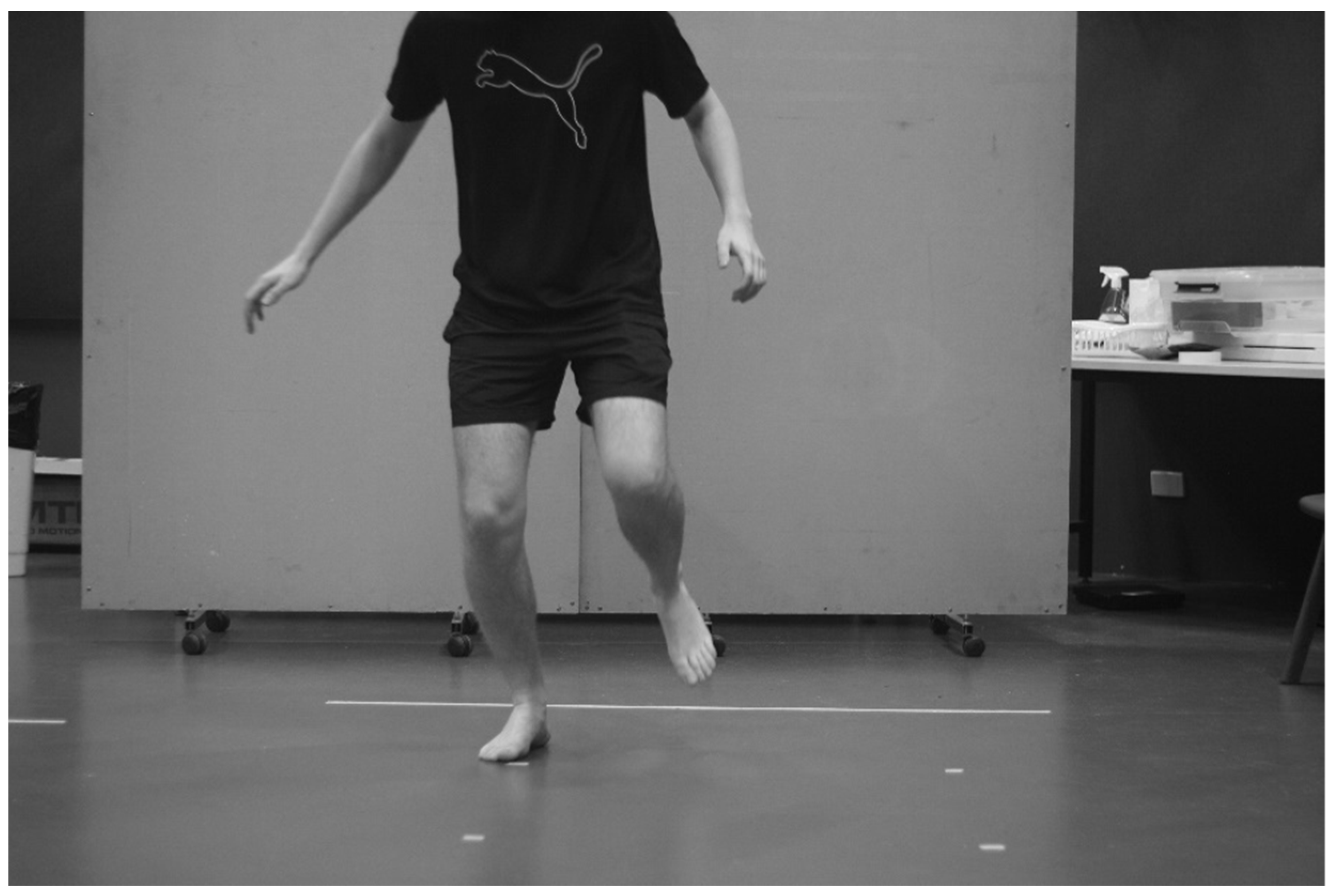
2.1.4. The Modified Bass Test of Dynamic Balance (BASS)
2.1.5. Data Extraction
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations and Future Lines of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Standardised Clinical Balance Test Instructions
Appendix A.1. The Balance Error Scoring System (BESS)
“This balance test is called the BESS. This stands for balance error scoring system. The test involves you maintaining your balance while standing still. The test has different conditions: standing with your feet together, standing on one leg and standing with one foot in front of the other. These conditions will be repeated on flat ground, and on a foam block. At the beginning of each trial, I will ask you to adopt the standard starting position. This involves standing up straight with your hands on your hips. When I say go, you will close your eyes and try to remain balanced. Each trial will run for 20 s. During this 20 s period I will count the number of balance errors that you commit. A balance error entails bending your hip forwards or to the side more than 30°, moving your hands off your hips, lifting your heels or forefoot off the ground, opening your eyes, stepping/stumbling/falling out of position, or failure to return to the starting position after five seconds.I ask that once you commit an error, you return to the standard position as quickly as you are able; however, ensure you do not rush and further disrupt your balance. Continue to do your best until the 20 s have elapsed. I will let you know when to stop. I will demonstrate each position to you before we begin. We will repeat the test twice. Before we begin, do you have any questions?”
Appendix A.2. Star Excursion Balance Test (SEBT)
“This test is called the star excursion balance test. It will involve you reaching in eight different directions with your leg in order to test your balance. The test will involve this section of tape that you can see on the floor. I will ask that you stand in the middle of the pattern, with the ball of your foot on the section where the tape intersects. Start with your right foot, and then we will perform on your left foot. This test requires that you reach as far as you can with your non-stance foot and lightly tap the most distant part of the tape that you can while maintaining your balance. Then, return your reaching foot to the middle, and move to the next piece of tape in an anti-clockwise direction. You will start by reaching towards the front piece of tape. You may have up to 15 s of rest between each trial if you wish. The test is completed once you have successfully reached in each direction. I need you to maintain your balance during this test and I will ask you to repeat the trial if you fail to maintain balance on your stance foot, lift or move your stance foot from the starting position, touch down too firmly with your reaching foot, or fail to return your reach foot to the starting position.I will demonstrate the test and then give you four practice trials per direction per leg. We will then conduct three measured trials per leg. During the test I will follow your movements and take recordings with a pencil. I will give you a two-to-three-minute rest in between each trial while I record your results. Do you have any questions before we begin?”
Appendix A.3. The Lateral Reach Test (LRT)
“This next test called the lateral reach test. It is going to look at your ability to lean to the left and to the right while maintaining your balance. You will take your position standing side-on to the board with your feet shoulder-width apart. Keep your non-test arm at your sides. Place the arm closest to the board up to shoulder height. During this time, I will make a measurement of the arm. I will then ask you to reach as far along the line of tape as possible while keeping your feet on the ground and keeping your balance. If you lose your balance, we will repeat the trial. If you move your non-test arm or lift your feet off the floor we will repeat the trial. I will demonstrate the test, then you will receive three practice trials. We will then perform two measured trials. Before you begin do you have any questions?”
Appendix A.4. The Modified Bass Test of Dynamic Balance (BASS)
“The next test is called the modified bass test of dynamic balance. The test involves you hopping between a series of markers while maintaining your balance. The markers are numbered, and laid out on the floor in front of you. You will start at the marker that says “start” by balancing on your right foot. You will then hop onto your left foot onto the area marked ‘1’. You will then hop onto your right foot onto the area marked ‘2’. You will continue to hop to each numbered marker, alternating between left and right single-leg balance until you reach the last marker, number ten. At each marker I ask that you aim to completely cover the marker with your foot, and remain balanced on the ball of your foot for five seconds at each marker before continuing. I will be playing a metronome during the test, so count five beats of the metronome before moving to the next marker. I will deduct marks for the following errors:Landing errors will result in a 5-point deduction: failing to stop and maintain balance upon landing, touching your heel or any body part on the ground apart from the ball of your foot, and failing to completely cover the square with ball of your foot. You will receive three points for partial covering. You will be allowed to reposition during the five-second balance phase if required.Balance errors will result in a one-point deduction for every second that the error is committed, up to a maximum of five points: touching your heel or any body part on the ground apart from the ball of your foot and moving your foot while in balance position. If you completely lose your balance (i.e., stumble away from the marker), step back to the previous marker, step to the correct marker and continue the test.I ask that you perform this test to the best of your ability. The test is scored out of 100, with 10 points available per marker. I will demonstrate the test; then, you will have two practice trials of your own. We will then conduct three testing trials and I will record your score for each of these three trials. Before we begin, do you have any questions?”
Appendix B. Balance Error Scoring System Setup


Appendix C. Star Excursion Balance Test Setup

Appendix D. The Lateral Reach Test Setup

Appendix E. The Modified Bass Test of Dynamic Balance Setup

References
- Cain, S.M.; Ashton-Miller, J.A.; Perkins, N.C. On the skill of balancing while riding a bicycle. PLoS ONE 2016, 11, e0149340. [Google Scholar] [CrossRef] [PubMed]
- Kooijman, J.D.G.; Schwab, A.L. A review on bicycle and motorcycle rider control with a perspective on handling qualities. Veh. Syst. Dyn. 2013, 51, 1722–1764. [Google Scholar] [CrossRef]
- Meijaard, J.P.; Papadopoulos, J.M.; Ruina, A.; Schwab, A.L. Linearized dynamics equations for the balance and steer of a bicycle: A benchmark and review. Proc. R. Soc. A Math. Phys. Eng. Sci. 2007, 463, 1955–1982. [Google Scholar] [CrossRef]
- Haeberle, H.S.; Navarro, S.M.; Power, E.J.; Schickendantz, M.S.; Farrow, L.D.; Ramkumar, P.N. Prevalence and epidemiology of injuries among elite cyclists in the Tour de France. Orthop. J. Sport. Med. 2018, 6, 1–5. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Hospitalised Injury Due to Land Transport Crashes; Australian Institute of Health and Welfare: Darlinghurst, Australia, 2018. Available online: https://www.aihw.gov.au/reports/injury/hospitalised-injury-due-to-land-transport-crashes/contents/table-of-contents (accessed on 29 July 2021).
- Eley, R.; Vallmuur, K.; Catchpoole, J. Value of emergency department triage data to describe and understand patterns and mechanisms of cycling injuries. Emerg. Med. Australas. 2019, 31, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Prati, G.; Puchades, V.M.; Pietrantoni, L. Cyclists as a minority group? Transp. Res. Part F Traffic Psychol. Behav. 2017, 47, 34–41. [Google Scholar] [CrossRef]
- Barrios, C.; Bernardo, N.D.; Vera, P.; Laíz, C.; Hadala, M. Changes in sports injuries incidence over time in world-class road cyclists. Int. J. Sport. Med. 2015, 36, 241–248. [Google Scholar] [CrossRef]
- Silberman, M.R. Bicycling injuries. Curr. Sport. Med. Rep. 2013, 12, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C. Balance ability and athletic performance. Sport. Med. 2011, 41, 221–232. [Google Scholar] [CrossRef]
- Riemann, B.L.; Guskiewicz, K.M.; Shields, E.W. Relationship between clinical and forceplate measures of postural stability. J. Sport Rehabil. 1999, 8, 71–82. [Google Scholar] [CrossRef]
- Riemann, B.L.; Guskiewicz, K.M. Effects of mild head injury on postural stability as measured through clinical balance testing. J. Athl. Train. 2000, 35, 19–25. Available online: https://search-proquest-com.dbgw.lis.curtin.edu.au/docview/206657864/fulltextPDF/A344911D7B6405BPQ/1?accountid=10382# (accessed on 10 June 2024). [PubMed]
- Kinzey, S.J.; Armstrong, C.W. The reliability of the star-excursion test in assessing dynamic balance. J. Orthop. Sport. Phys. Ther. 1998, 27, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Purohit, R.D.; Sadhale, A. Co-relation between static and dynamic balance in healthy individuals between 18-25 years using one leg stance test and multi directional reach test. Indian J. Physiother. Occup. Ther. 2014, 8, 89–93. Available online: https://search-proquest-com.dbgw.lis.curtin.edu.au/docview/1538320335/fulltextPDF/A2D6A6E46F4D4B88PQ/1?accountid=10382# (accessed on 9 June 2024). [CrossRef]
- Ambegaonkar, J.P.; Caswell, S.V.; Winchester, J.B.; Shimokochi, Y.; Cortes, N.; Caswell, A.M. Balance comparisons between female dancers and active nondancers. Res. Q. Exerc. Sport 2013, 84, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Ambegaonkar, J.P.; Redmond, C.J.; Winter, C.; Cortes, N.; Ambegaonkar, S.J.; Thompson, B.; Guyer, S.M. Ankle stabilizers affect agility but not vertical jump or dynamic balance performance. Foot Ankle Spec. 2011, 4, 354–360. [Google Scholar] [CrossRef]
- Elliott, J.; Anderson, R.; Collins, S.; Heron, N. Sports-related concussion (SRC) assessment in road cycling: A systematic review and call to action. BMJ Open Sport Exerc. Med. 2019, 5, e000525. [Google Scholar] [CrossRef] [PubMed]
- Marin-Perianu, R.; Marin-Perianu, M.; Havinga, P.; Taylor, S.; Begg, R.; Palaniswami, M.; Rouffet, D. A performance analysis of a wireless body-area network monitoring system for professional cycling. Pers. Ubiquitous Comput. 2013, 17, 197–209. [Google Scholar] [CrossRef]
- Cockcroft, J.; Scheffer, C. Determining the feasibility of measuring outdoor road cycling kinematics using inertial motion capture technology. SAIEE Afr. Res. J. 2011, 102, 31–39. [Google Scholar] [CrossRef]
- Gribble, P.A.; Hertel, J. Considerations for normalizing measures of the Star Excursion Balance Test. Meas. Phys. Educ. Exerc. Sci. 2003, 7, 89–100. [Google Scholar] [CrossRef]
- Finnoff, J.T.; Peterson, V.J.; Hollman, J.H.; Smith, J. Intrarater and interrater reliability of the balance error scoring system (BESS). Pm&r 2009, 1, 50–54. [Google Scholar] [CrossRef]
- Bell, D.R.; Guskiewicz, K.M.; Clark, M.A.; Padua, D.A. Systematic review of the balance error scoring system. Sport. Health 2011, 3, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.G.; Herrington, L.C. Between-session reliability of the star excursion balance test. Phys. Ther. Sport 2010, 11, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Brauer, S.; Burns, Y.; Galley, P. Lateral reach: A clinical measure of medio-lateral postural stability. Physiother. Res. Int. 1999, 4, 81–88. Available online: https://search-proquest-com.dbgw.lis.curtin.edu.au/docview/215212279/fulltextPDF/5A08E3C4635E444DPQ/1?accountid=10382 (accessed on 9 June 2024). [CrossRef]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. Available online: https://www.sma.org.sg/smj/4412/4412bs1.pdf (accessed on 1 June 2024).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; Available online: https://books.google.com.au/books?hl=en&lr=&id=rEe0BQAAQBAJ&oi=fnd&pg=PP1&ots=swWSMuQRo7&sig=atG2PGBReLXr8roeZfXg-g3w5Dc&redir_esc=y#v=onepage&q&f=false (accessed on 17 September 2021).
- Zignoli, A.; Biral, F.; Fornasiero, A.; Sanders, D.; Erp, T.V.; Mateo-March, M.; Fontana, F.Y.; Artuso, P.; Menaspà, P.; Quod, M.; et al. Assessment of bike handling during cycling individual time trials with a novel analytical technique adapted from motorcycle racing. Eur. J. Sport Sci. 2022, 22, 1355–1363. [Google Scholar] [CrossRef]
- Daneshfar, A.; Petersen, C.; Gahreman, D.; Knechtle, B. Power analysis of field-based Bicycle Motor Cross (BMX). Open Access J. Sport. Med. 2020, 11, 113–121. [Google Scholar] [CrossRef]
- Zemková, E. Sport-specific balance. Sport. Med. 2014, 44, 579–590. [Google Scholar] [CrossRef]
- Bressel, E.; Yonker, J.C.; Kras, J.; Heath, E.M. Comparison of static and dynamic balance in female collegiate soccer, basketball, and gymnastics athletes. J. Athl. Train. 2007, 42, 42–46. Available online: https://www.proquest.com/docview/206650796/fulltextPDF/76D1B54BB88C4091PQ/1?accountid=10382# (accessed on 2 June 2024). [PubMed]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted-Kramer, L.C. Simplifying the star excursion balance test: Analyses of subjects with and without chronic ankle instability. J. Orthop. Sport. Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef]
- Yuksel, E.; Ozcan Kahraman, B.; Nalbant, A.; Kocak, U.Z.; Unver, B. Functional reach and lateral reach tests in turkish children. Phys. Occup. Ther. Pediatr. 2017, 37, 389–398. [Google Scholar] [CrossRef]
- DeWaard, B.P.; Bentrup, B.R.; Hollman, J.H.; Brasseur, J.E. Relationship of the functional reach and lateral reach tests in elderly females. J. Geriatr. Phys. Ther. 2002, 25, 4–9. Available online: https://www.proquest.com/docview/213624216/fulltextPDF/6A5654CAE6C243BBPQ/2?accountid=10382 (accessed on 30 May 2024). [CrossRef]
- Popov, A.A.; Rowell, S.; Meijaard, J.P. A review on motorcycle and rider modelling for steering control. Veh. Syst. Dyn. 2010, 48, 775–792. [Google Scholar] [CrossRef]
- Nashner, L.M. Practical Biomechanics and Physiology of Balance; Plural Publishing Inc.: San Diego, CA, USA, 2014; Available online: https://books.google.com.au/books?id=lSzJDwAAQBAJ&printsec=frontcover&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false (accessed on 26 September 2021).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Balance Error Scoring System (Errors) | |
|---|---|
| Bipedal | 0 ± 0 |
| Bipedal on foam | 0 ± 0 |
| Unipedal | 2 ± 1 |
| Unipedal on foam | 7 ± 1 |
| Tandem | 1 ± 1 |
| Tandem on foam | 5 ± 2 |
| Variable One | Variable Two | Spearman’s Correlations (r) |
|---|---|---|
| Mean corner speed | Lap time | −0.88 |
| Mean corner speed | Mean velocity | 0.87 |
| Mean corner speed | Median velocity | 0.84 |
| Maximum corner speed | Lap time | −0.82 |
| Maximum corner speed | Median velocity | 0.80 |
| Maximum corner speed | Mean velocity | 0.78 |
| Mean corner speed | Mean lap time | −0.75 |
| Maximum corner speed | Maximum velocity | 0.73 |
| Maximum corner speed | Mean lap time | −0.72 |
| Mean corner speed | Maximum velocity | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harris, T.; Netto, K.; Hillier, C.M.; Burgess, S.; Rosalie, S.M. Are Clinical Balance Measures Linked to Cycling Performance? Appl. Sci. 2024, 14, 6379. https://doi.org/10.3390/app14146379
Harris T, Netto K, Hillier CM, Burgess S, Rosalie SM. Are Clinical Balance Measures Linked to Cycling Performance? Applied Sciences. 2024; 14(14):6379. https://doi.org/10.3390/app14146379
Chicago/Turabian StyleHarris, Tasman, Kevin Netto, Caitlin M. Hillier, Sharni Burgess, and Simon M. Rosalie. 2024. "Are Clinical Balance Measures Linked to Cycling Performance?" Applied Sciences 14, no. 14: 6379. https://doi.org/10.3390/app14146379
APA StyleHarris, T., Netto, K., Hillier, C. M., Burgess, S., & Rosalie, S. M. (2024). Are Clinical Balance Measures Linked to Cycling Performance? Applied Sciences, 14(14), 6379. https://doi.org/10.3390/app14146379