Abstract
Varicose veins in the lower limb are a common and progressive venous disorder that can significantly reduce patients’ quality of life and pose a threat to their overall health if left untreated. However, current treatment approaches often involve invasive intervention. High-intensity focused ultrasound (HIFU) technology has the potential to treat varicose veins non-invasively, but most systems are bulky and expensive. This study proposes an innovative, integrated system that uses a 4.5 MHz therapeutic probe guided by a 12 MHz ultrasound imaging probe to treat varicose veins in the lower limb. The system aims to achieve high accuracy in repeated treatments by using a high-speed scanning positioning structure, increasing the imaging framerate, and reducing the system’s overall volume. The system’s accuracy is evaluated through reset error tests on an acrylic board, and its effectiveness is tested through in vivo experiments on rabbit marginal ear veins. Tests on porcine arteries are conducted to identify suitable focal points for vascular treatment. The experimental results demonstrate the system’s high accuracy, with a reset error of less than 0.07 mm, and an obvious shrinkage of the predetermined treatment area of the marginal ear veins after therapy. The study identifies that setting the focus on the vascular wall can improve the efficiency of vascular treatment, resulting in significant vasoconstriction changes. These experimental findings provide sufficient evidence for the system’s potential for clinical application in vascular treatment.
1. Introduction
Varicose veins of the lower limb are a common venous disease that disproportionately affects individuals who maintain a sedentary or physically demanding lifestyle. The primary etiology of the disease is the prolonged impairment of venous blood flow, resulting in blood accumulation and stasis within the veins and consequent venous reflux, increased venous pressure, and valve damage. Epidemiological studies conducted abroad have revealed an overall incidence rate of 29.5–39.0% among women and 10.4–23.0% among men [1]. As the disease is progressive, its initial clinical presentation is often insidious, with symptoms such as lower limb fatigue, heaviness, and ankle edema arising in the later stages. Left untreated, long-term blood stasis may cause skin pigmentation, venous ulcers, and thrombophlebitis, significantly impacting the patient’s quality of life [2].
In the early stages of lower-limb varicose veins, patients may alleviate the condition and prevent further deterioration by wearing elastic stockings. However, surgical intervention becomes necessary as the condition worsens. Historically, high ligation and stripping of the great saphenous vein has been the primary surgical approach [3], involving suturing the vessels at their source and simultaneously stripping and removing the trunk vessels, along with the rest of the non-functional superficial veins. However, patients are at risk of infection and other complications due to the large surgical incision [4]. With the advancement of minimally invasive technology, treatment has shifted from open surgery to minimally invasive procedures that feature smaller incisions and faster recovery times. Currently, minimally invasive treatments include modified great saphenous vein high ligation and stripping, endovenous thermal ablation (EVTA), and injection sclerotherapy [5,6]. While thermal ablation and other techniques have demonstrated their clinical effectiveness in treating varicose veins, they are not universally applicable. In particular, veins that are less than 3.5 mm in diameter and situated deep within the skin are not suitable for thermal ablation. Furthermore, minimally invasive procedures require experienced physicians to achieve high success rates, and there is a risk of distant thromboembolic or other potentially lethal complications [7,8,9,10,11]. As a result, the development of non-invasive methods for treating varicose veins in the lower extremities through in vitro closure is a desirable goal.
In recent years, non-invasive therapies have become increasingly attractive for treating lower-limb varicose veins, with ultrasound-guided high-intensity focused Ultrasound (HIFU) therapy being a new focus [12,13,14,15,16]. HIFU technology is an effective non-invasive technique for precisely destroying deep target tissues. Its therapeutic principle is to concentrate energy at a focus using a concave HIFU probe, thereby producing a range of effects, including thermal, mechanical, and cavitation effects, that lead to precise tissue necrosis and vascular fibrosis. Some scholars have reported using HIFU in animal studies and clinical settings in a small number of patients to ablate varicose veins [17,18]. In clinical trials, the therapy is accurately targeted to the vein of interest using ultrasound imaging guidance, with five successful cases reported. HIFU technology is an effective non-invasive technique for precisely destroying deep target tissues. In the abovementioned study, a conventional B-mode linear array probe was used to guide the focusing therapeutic probe. Due to the volume and weight limitation of the linear array imaging probe, the whole system often required the assistance of a mechanical arm to ensure accuracy [13]. Although handheld operation is more convenient for doctors to adjust the treatment plan during treatment, considering that the entire treatment cycle of focused ultrasound therapy for lower extremity veins is relatively long, holding such a large device for a long time puts a heavy burden on the doctor. Because of these problems, the system has not been well popularized. On the other hand, portable focusing therapeutic probes used in lower-limb varicose veins have been reported; however, their success rates are low due to the lack of effective miniaturized imaging guidance [19,20,21]. Therefore, it is imperative to develop an ultrasound-guided miniaturized therapy system that is tailored to the vascular characteristics of varicose veins in the lower limbs.
This study presents a novel system for venous varicose ultrasound therapy that employs high-frequency ultrasound guidance. The system integrates a 12 MHz mid-high frequency single-element imaging probe and a 4.5 MHz focusing therapeutic probe, as well as an accurate scanning and positioning structure. One of the key benefits of this system is its ability to achieve high-speed scanning and positioning, while also providing high-framerate imaging that can effectively deal with the tortuous and complex morphology of veins, thus facilitating accurate treatment. Additionally, this system boasts a compact structure and miniature size, in contrast to the conventional B-mode linear array probe-guided focusing therapeutic probe.
This article proceeds to present the key elements of the proposed integrated system, followed by an assessment of the reset error using acrylic boards. The accuracy of the treatment is then evaluated using rabbit marginal ear veins. To further refine the system, the focus point appropriate for vascular treatment is identified via experiments involving porcine arteries.
2. Materials and Methods
2.1. Design of the Integrated Probe
The integrated probe prototype is depicted in Figure 1a, which displays a single-element imaging probe positioned within the central hole of a spherical-focused therapeutic probe. The therapeutic probe operates at a center frequency of 4.5 MHz, while the imaging probe operates at 12 MHz. Two probes were fixed to the mechanical structure by connectors. Compared to the therapy system guided by a linear array B-mode imaging probe, the volume is significantly reduced, which is depicted in Figure 1b.
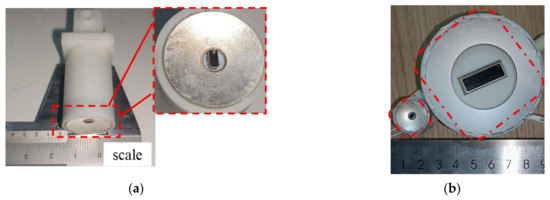
Figure 1.
Prototype probe for integrated ultrasound imaging and therapy: (a) system guided by a single-element imaging probe; (b) dimensional comparison, the right is a system guided by a B-mode imaging probe.
The imaging probe utilized in this study was a 12 MHz single-element probe, which was located horizontally in the central hole of the therapeutic probe for imaging the treatment focus. The echo amplitude and spectrum of the imaging probe can be observed in Figure 2. The use of this frequency probe allowed for effective imaging of shallow and complex tortuous venous morphology, while also allowing for the detection of potential deep venous thrombosis. This is advantageous for the development of a comprehensive treatment plan due to the probe’s excellent imaging depth and resolution.
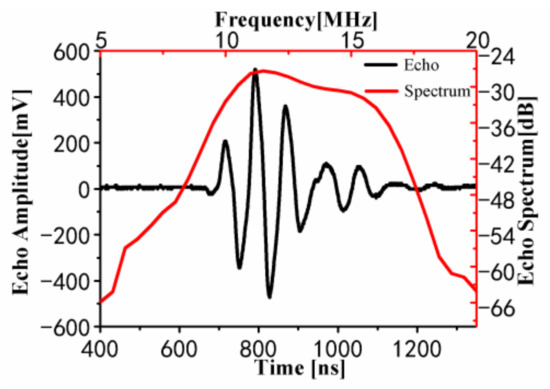
Figure 2.
Echo test results of the 12 MHz imaging probe.
The use of HIFU treatment requires the selection of an appropriate frequency for the therapeutic probe. Generally, the therapeutic probe frequency is set between 1 and 3 MHz [22]. However, some studies have suggested that higher frequency focused ultrasound probes can achieve better treatment outcomes for vascular treatments [23]. Therefore, this system developed three higher-frequency focused ultrasound probes with the same physical parameters, including diameter and curvature, except for the frequency, at 3 MHz, 4.5 MHz, and 7.5 MHz. The increase in the excitation frequency of the transducer in most human tissues leads to a power-law increase in absorption and attenuation. An increase in absorption coefficient results in a larger sound absorption and heating rate, while an increase in attenuation coefficient decreases the penetration depth. Therefore, in this experiment, both the heating rate and the penetration depth of blood vessels under ultrasound exposure need to be considered simultaneously.
In previous studies, the primary reason for the contraction and closure of blood vessels under ultrasound exposure was determined to be the high-temperature denaturation reaction of collagen in the blood vessels [24,25]. To compare the effect of these three treatment probes on protein denaturation, a one-minute treatment comparison experiment was conducted using 15 W of sound power to excite these probes with a sinusoidal wave on a PAA phantom. The PAA phantom was made of polyacrylamide gel with 30% added serum, whose acoustic parameters were similar to those of ex vivo liver and muscle tissue [26]. When the temperature of the PAA phantom reaches 60 °C or above, it changes from transparent to opaque white. Additionally, 60 °C is the critical temperature for irreversible coagulation necrosis of cells. Therefore, a PAA phantom is often used in HIFU ablation experiments, and the ablation range can be determined by observing the white area inside the PAA phantom. Each frequency of the focused ultrasound transducer underwent three experiments, and the average width, height, and area of the resulting lesions were calculated. The results are shown in Figure 3.
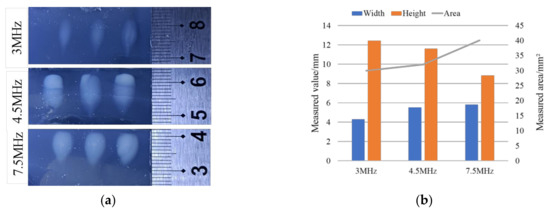
Figure 3.
PAA phantom treatment experiment: (a) physical pictures of treatment results; (b) damage measurement results of the PAA phantom.
To test the protein heating rate generated by the three different frequency probes during treatment, a thermocouple was embedded in the PAA phantom at the focus of the probe, and the temperature rise was recorded and plotted using a communication converter. Subsequently, the same method as the aforementioned experiment was used for one minute of treatment. Multiple thermocouple temperature rise tests were conducted for each frequency of the focusing probe, and a stable group was selected as a representative after multiple experiments, as shown in Figure 4.
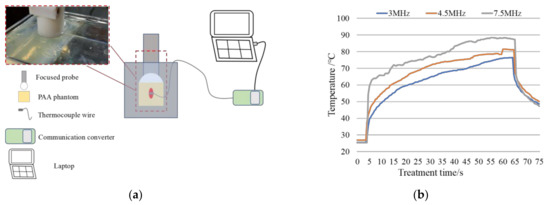
Figure 4.
Protein heating rate treatment experiment: (a) experimental platform; (b) protein heating rate measurement results.
Based on the damage results of the protein phantom and the temperature rise results obtained by thermocouple testing, it was found that the higher frequency transducer had a better temperature rise rate, as shown in Figure 4b. However, due to the attenuation effect of the high-frequency probes during propagation with the frequency increases, the shape of the focal area changed from a cone to a sphere gradually, and the treatment depth also decreased significantly, as shown in Figure 4a. Therefore, for superficial varicose veins, it is appropriate to choose a high-frequency treatment probe. In this study, a 4.5 MHz treatment probe was selected considering both the heating rate and the treatment depth, which has a balanced therapeutic effect in the experiment, as shown in Figure 3a,b. Therefore, this study chose the 4.5 MHz focusing transducer to realize the fusion transducer’s therapeutic function. On the other hand, as noted in Table 1, the central hole in the therapeutic probe results in significant sound pressure attenuation when there is water in the backing; the sound power measurement platform is shown in Figure 5. Consequently, the connection between the imaging probe and the therapeutic probe should be waterproofed.

Table 1.
The excitation sound power of 4.5 MHz probes with different configurations.
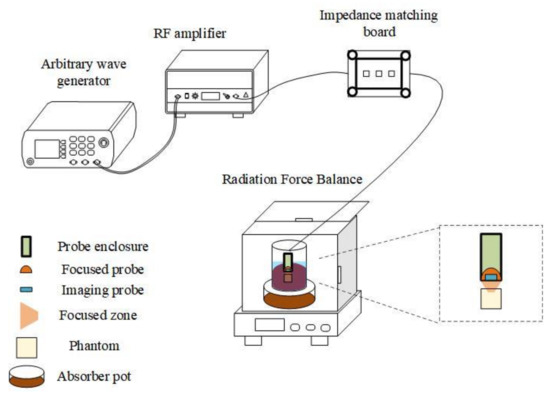
Figure 5.
Sound power measurement platform.
2.2. High-Speed Scanning Positioning Structure
The eccentric wheel structure used in the integrated system is depicted in Figure 6a, which drives the focused integrated probe and enables real-time imaging of complex venous regions at a high framerate of 30 frames per second (fps). The mechanical structure of the system utilizes a crank–slider model that converts the high-speed rotary motion of the motor into high-speed reciprocating linear motion.
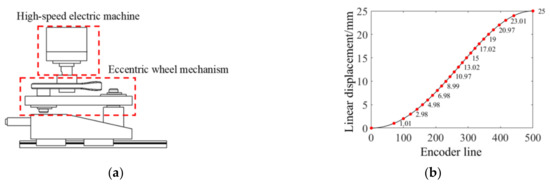
Figure 6.
High-speed scanning positioning structure: (a) wheel motion mechanism; (b) theoretical coordinates of the treatment point.
Due to the non-linear properties of the structure, compensation of the RF signal obtained by the imaging probe was necessary before image reconstruction. As the eccentric wheel mechanism was essentially a crank–slider mechanism, the RF signal collected by the probe was subjected to non-uniform interpolation based on the path characteristics of the crank–slider motion to correct image distortion before image reconstruction. Figure 6b displays the preset treatment trigger points, marked in red. To ensure an even distribution of treatment points across the 25 mm treatment area, the straight path is projected onto the rotating path. The encoder line closest to the theoretical rotation angle obtained via treatment point mapping is then selected as the treatment trigger signal. Furthermore, at the end of each cycle, the optical and electrical sensor is employed to reset the starting point of each stroke, thereby mitigating cumulative error.
2.3. Verification Experiment of the Treatment System
The repeated treatment accuracy of the integrated system is a crucial parameter in evaluating its performance. To monitor the treatment progress during therapy, the imaging function of the system is utilized. Given the movement of the focusing therapeutic probe along with the imaging probe, the ability to reset to the original treatment point after imaging plays a pivotal role in determining the efficacy of treatment. The present study employed acrylic boards and rabbit marginal ear veins to measure the reset error.
2.3.1. In Vitro Experiment
The experimental platform is shown in Figure 7. In the reset error measurement experiment, the integrated therapy system was mounted on the horizontal displacement platform and was used to treat acrylic boards. The treatment points were selected by the host computer, and after each treatment cycle was completed, the displacement platform moved the integrated system at regular intervals in the vertical direction along the treatment direction in the horizontal plane, repeating the same treatment cycle. Since the common treatment pitch was 1 mm, the linear therapy path was divided into 25 segments, resulting in 26 treatment points, each of which was treated with a pulse treatment time of 40 ms and sound power of 15 ± 1 W. Following treatment, the relative displacement between every two points on the acrylic board and the absolute displacement from the first treatment point to the measured point was measured using an optical microscope magnification.
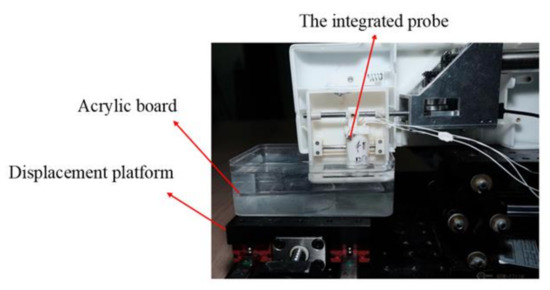
Figure 7.
The experimental platform of the reset error measurement.
2.3.2. In Vivo Experiment
In mammalian proteins, the effects of HIFU can be classified into three distinct categories. The first category involves low-intensity thermal damage, which is caused by prolonged exposure to HIFU. The second category involves high-intensity damage that occurs over a short period and is the result of cavitation. The third and final category involves moderate-intensity and -duration mechanically induced damage. When implementing vascular therapy, it is common practice to utilize low-intensity and prolonged treatment regimens. This approach is employed to achieve vessel shrinkage while simultaneously mitigating the risk of complications such as vessel rupture, which can arise as a result of cavitation and other mechanical effects [27,28,29]. In this study, we conducted an in vivo experiment on rabbit marginal ear veins using low-intensity and prolonged ultrasound therapy, utilizing its thermal effect on proteins, to assess the treatment effectiveness of the therapy system. The experimental setup comprised a laboratory lift, the integrated therapy system, a signal-triggering and -receiving device, and a displacement platform controlled by a stepper motor control box (Zolix SC300 series, Zolix, Beijing, China).
The experimental setup for verifying the accuracy of the treatment using rabbit marginal ear veins is shown in Figure 8. A New Zealand white rabbit weighing 2 kg (±0.5 kg) was anesthetized intramuscularly with ketamine (30 mg/kg) and intubated with an endotracheal tube which was ventilated with isoflurane (0.2 L/kg/min) to keep the rabbit under anesthesia throughout the procedure with an R500 small animal anesthesia machine (RWD). The fur on both sides of the ear was shaved with a hair trimmer and then carefully depilated with a depilatory cream to ensure proper acoustic coupling and prevent skin burns. One ear was immobilized in an experimental vessel filled with deionized water using medical tape, and the marginal ear vein was exposed on the integrated probe movement path. The imaging probe was used to position the protruding marginal ear vein, after which the mechanical structure drove the integrated probe to the designated treatment site. An electric power of 10 ± 1 W was applied for 4 min. After the experiment, the effectiveness was evaluated by comparing the results before and after treatment using the Vevo 2100 ultra-high resolution small animal ultrasound imaging system produced by VisualSonics with a 50 MHz linear array probe.
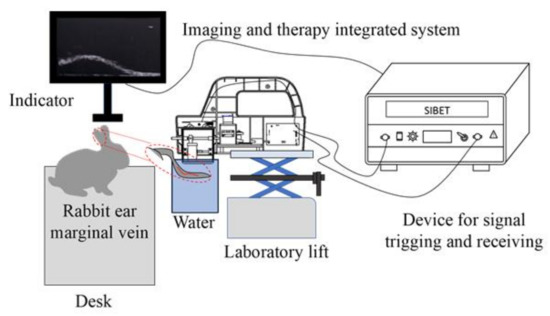
Figure 8.
The experimental platform of rabbit marginal ear veins.
Following the guidelines of the Declaration of Helsinki and approved by the Laboratory Animal Center of Huazhong University of Science and Technology (SYXK-2021-0057), an in vivo experiment on rabbits was conducted. The animals were kept under controlled environmental conditions, including a 12/12 h light/dark cycle and a temperature of 22 ± 2 °C. Food and water were well supplied during the experiment.
2.4. Ex Vivo Tissue Experiment
The selection of treatment foci is critical in determining the effectiveness of surgical outcomes due to the unique structure of blood vessels. Various treatment foci can influence treatment efficiency, and identifying the optimal treatment foci is essential to minimizing burns to neighboring tissues and the skin [30,31,32]. In this experiment, vascular constriction results with different treatment foci were tested and compared. As depicted in Figure 9, three different positions for the treatment foci were evaluated. These included the superior blood vessel wall closer to the probe in Figure 9a, the center position of the blood vessel in Figure 9b, and the inferior blood vessel wall farther from the probe in Figure 9c. The treatment probe had a focal length of 20 mm, and the height of the focused probe and the arteries were adjustable using the laboratory lift to modify the position of the focus treatment point.
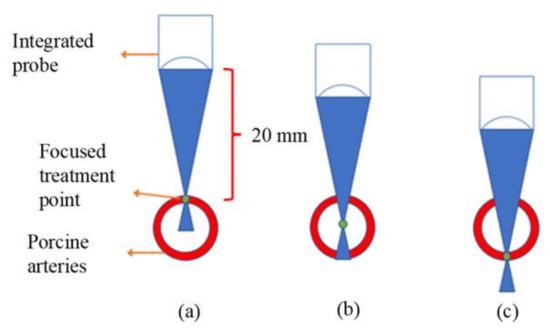
Figure 9.
Schematic diagram of different focused treatment points: (a) the treatment focus on the superior wall of the blood vessel; (b) the treatment focus on the middle of the blood vessel; (c) the treatment focus on the inferior wall of the blood vessel.
To facilitate ultrasonic imaging observation, fresh porcine arteries with a diameter of 3–5 mm were used as experimental materials. The experimental platform was similar to that used in the rabbit experiment, except for the experimental objective. The porcine arteries were obtained from a slaughterhouse, soaked in physiological saline, and used for experiments within three hours of acquisition. Anticoagulant bovine blood was injected into the arteries, and the two ends were cauterized with an electric iron to simulate a similar vascular environment and prevent the anticoagulated bovine blood from spilling out during treatment. The imaging function of the integrated system was utilized to achieve the positioning of each focus on the artery, and the position was changed by adjusting the height of the laboratory lift. The therapeutic probe was maintained at a constant distance of 20 mm from the designated treatment point throughout the entire experiment. A continuous sine wave was used as the excitation, with the output sound power of the focusing treatment probe set to 15 ± 1 W due to the thickness of the arterial wall. During the cumulative 5 min treatment process, the therapy was paused at 1 min, 3 min, and 5 min, respectively, and the effect images of different focusing foci at the same treatment time were obtained using the imaging function of the integrated system. The integrated probe was then returned to its original position by the mechanical structure. After the treatment of the three vessels, the acquired ultrasound images by the imaging probe were compared to determine the optimal focus with the best effect. The Vevo 2100 was also used for verification after the experiment.
3. Results and Discussion
3.1. Results of the Treatment System Validation Experiments
3.1.1. Results of In Vitro Experiment
This study conducted a treatment reset error experiment, with the results presented in Figure 10, and the measured relative and absolute displacements shown in the chart in Figure 11. Both the relative and absolute errors of the three measured displacements are small, and the repeated displacement deviation during treatment meets the treatment requirements. However, the relative error of the 23rd displacement is relatively large, with a maximum error of 0.07 mm between two extreme points, likely due to mechanical structure errors near the end of treatment causing jitter and affecting treatment accuracy. Notably, the displacement measurement results of the 7th, 8th, and 15th segments suggest that one displacement error is larger than the other two, but this is initially believed to be a measurement error.
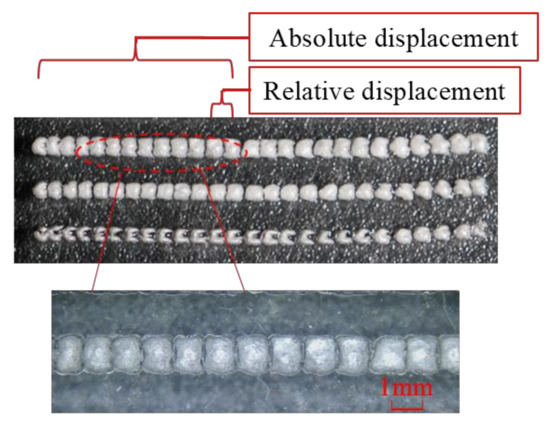
Figure 10.
The picture of the in vitro experiment results.
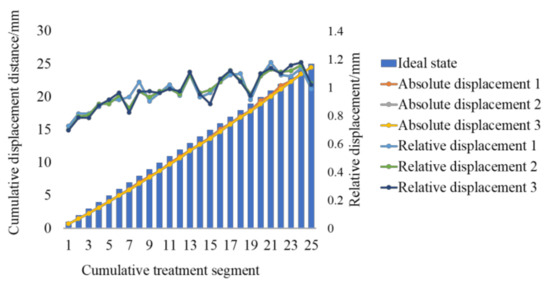
Figure 11.
Error statistics results.
On the other hand, the relative error and absolute error of the three displacement measurements have some deviations from the ideal state, as shown in Figure 11. The whole displacement process shows an overall upward trend, and the maximum cumulative error is 1.2 mm. The primary reason for this result is that the therapeutic probe is not placed parallel to the treatment area during treatment; a horizontal calibration module could be added to address this problem.
3.1.2. In Vitro Validation Experiments for Treatment Accuracy
Figure 12a shows the ear margin vein of the rabbit to be treated after fur removal, and Figure 12b reveals that the skin in the treated area is in a white degeneration state compared with other areas in the path of the vein. This indicates that the treatment area is limited to the vascular area and does not cause burning of the surrounding tissue. The white degeneration state is believed to be a type of skin burn. Figure 13a displays an ultrasound image of the marginal ear vein in an untreated rabbit ear, while Figure 8b shows the same vein after treatment. Contraction and deformation of the blood vessel wall can be observed at the treatment point in Figure 13b. Furthermore, the internal diameters of the blood vessels were measured using the built-in measurement system of the Vevo 2100. The diameter of the untreated area was approximately 0.49 mm. After treatment, the blood vessel contracted to 0.22 mm, and the shrinkage rate was approximately 55%, which is consistent with the observed vascular degeneration results in Figure 12b. This confirms the accuracy of the treatment.
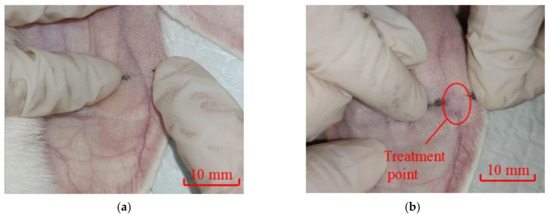
Figure 12.
Comparison of rabbit marginal ear vein: (a) before treatment; (b) after treatment.
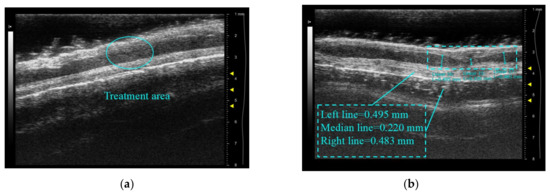
Figure 13.
The contrast image of rabbit ear vein contraction: (a) before treatment; (b) after treatment.
In in vitro validation experiments, due to the small size and slow blood flow speed of the rabbit ear margin veins compared to human veins, the temperature rises in the area quickly, and contraction of the superior and inferior vascular walls is observed. It is also found that if the treatment power is increased to pursue fast treatment, not only would the tissue and skin near the blood vessel be burned, but also the blood vessel would be directly ruptured and cause massive bleeding. Further research and consideration are needed to balance the treatment power and adopt appropriate cooling measures to protect the skin from burns.
3.2. Results of Porcine Arteries Experiments
Figure 14a demonstrates that when the treatment focus is positioned on the superior wall of the blood vessel, the area of high-brightness degeneration of the vessel appears solely on the superior surface portion of the vessel. Moreover, an elongated treatment period does not notably affect the inferior side of the vessel wall. The degeneration changes are more pronounced between 1 and 3 min of treatment time, after which there is less variation.
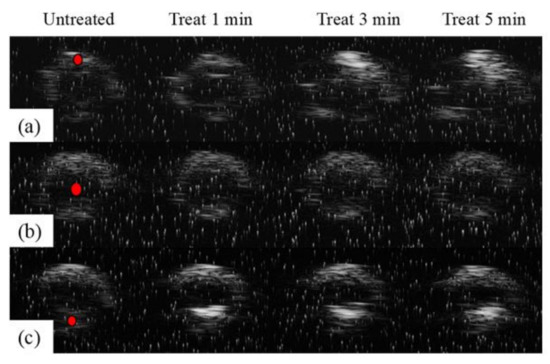
Figure 14.
Results of different treatment foci on the ultrasound imaging function of the integrated system: (a) the treatment focus on the superior wall of the blood vessel; (b) the treatment focus on the middle of the blood vessel; (c) the treatment focus on the inferior wall of the blood vessel.
In Figure 14b, when the treatment focus is located at the center of the vessel, the results exhibit no significant contraction or degeneration in the overall area of the vessel, nor any high-brightness degeneration. Consequently, positioning the focus in the middle of the vessel may not be suitable for a thick vessel with blood.
As shown in Figure 14c, when the treatment focus is located on the inferior wall of the blood vessel, it is found that the area of high-brightness degeneration is only present on the inferior surface of the vessel, and prolonged treatment also has no significant effect on the superior surface. Similarly, more pronounced degeneration happens from 1 min to 3 min of treatment time, after which there is less change.
The comparison results demonstrate that degeneration and deformation are more likely to occur when the focal point is situated on the blood vessel wall. Due to the blood’s higher specific heat capacity, this may lead to less overall vasoconstriction for the same treatment energy. Consequently, it is reasonable to select the vessel wall as the focal point’s location. Meanwhile, since skin burning may occur when the treatment point is placed on the superior wall, it is preferable to place the treatment point on the inferior wall to effectively prevent skin burns. On the other hand, when the treatment time lasts for 3 min, the degeneration degree of each treatment point shows no further change. This indicates that for vessels that have reached the threshold of local degeneration, the position of the therapeutic probe needs to be adjusted to avoid areas of fibrosis if they are to shrink further. It is suitable that limiting the treatment time to 1–3 min is better for the treatment of vessels with similar diameters.
Figure 15 displays a comparison of vascular imaging before and after treatment of the inferior tube wall using a commercial Vevo 2100 small animal ultrasound system in combination with a 50 MHz center frequency linear array imaging probe. The untreated porcine artery area in Figure 15a is approximately 6.54 mm2, with a maximum diameter of 3.143 mm and a minimum diameter of 2.648 mm. The treated pig artery section is displayed in Figure 15b, with an area of approximately 4.898 mm2, a maximum diameter of 3.027 mm, and a minimum diameter of 1.987 mm. The cross-sectional area decreases by 25% after the treatment, while the minimum diameter decreases by 24%. The inferior wall of the vessel indicates notable shrinkage, consistent with the result of the high-light denaturation on the inferior surface of the vessel after treatment in Figure 14c, thereby confirming the effectiveness of this innovative high-frequency ultrasound-guided integrated system for varicose vein ultrasound therapy under similar working conditions.
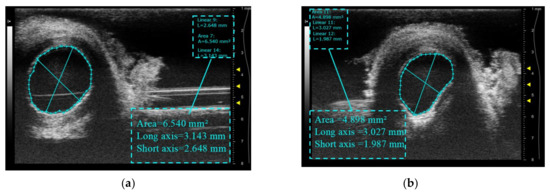
Figure 15.
Cross-sectional ultrasound comparison images of blood vessels before and after treatment: (a) before treatment; (b) after treatment.
4. Conclusions
In this study, a novel high-frequency ultrasound-guided integrated system is developed for varicose vein ultrasound therapy, which effectively reduces the overall dimension while ensuring a high framerate to ensure the accuracy of repeated treatment. The effectiveness of the system is verified by in vitro, ex vivo, and in vivo experiments, the results show that the reset error is lower than 0.7 mm, and the preset treatment area of the rabbit marginal ear veins has shrunk. At the same time, it is also found that setting the focus of the therapeutic probe on the inferior blood vessel wall farther from the probe can not only ensure therapeutic efficiency but also alleviate possible skin burning. It has been found in previous animal and clinical experiments that the use of focused ultrasound therapy for lower extremity varicose veins has a higher recurrence rate, which may be related to the method of extracorporeal focused ultrasound therapy itself [13,15,21,33]. On the other hand, even with clinical surgery to completely strip the relevant veins, there is no guarantee that there is no possibility of recurrence [17,34,35,36,37]. In comparison, this non-invasive extracorporeal treatment method can compensate for the shortcomings in recurrence rate control through repeated treatments, ultimately achieving the goal of a complete cure. Compared with existing treatment methods, the proposed portable integrated system in this study offers a simpler and safer alternative. Future research will focus on improving the performance of vascular closure by refining the selection of treating parameters.
Author Contributions
Conceptualization, J.X., Y.J. and Y.C.; methodology, J.X.; software, Y.J. and X.L.; validation, J.X., W.H. and J.L.; formal analysis, J.X.; investigation, J.X.; data curation, J.X. and Y.X.; writing—original draft preparation, J.X.; writing—review and editing, Y.J. and Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
Quancheng 5150 Project; Suzhou science and technology plan project (Grant NO. SZS201903) and Jiangsu Science and Technology Project (Grant NO. BE2022117); Shandong Natural Science Foundation, ZR2022QF105.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the laboratory animal center of Huazhong University of Science and Technology (SYXK-2021-0057).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Thanks to the laboratory animal center of Huazhong University of Science and Technology for providing the experimental platform. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Leopardi, D.; Hoggan, B.L.; Fitridge, R.A.; Woodruff, P.W.H.; Maddern, G.J. Systematic Review of Treatments for Varicose Veins. Ann. Vasc. Surg. 2009, 23, 264–276. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Silverstein, M.D.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J. Risk factors for deep vein thrombosis and pulmonary embolism—A population-based case-control study. Arch. Intern. Med. 2000, 160, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.Y.; Qiu, T.; Bu, X.Q.; Li, X.T.; Liang, G.Z.; Zhang, H.; Niu, L.Y.; Zhao, H.; Zhang, F.X. A national survey on management of varicose veins in China. J. Vasc. Surg.-Venous Lymphat. Disord. 2018, 6, 338–346.e1. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.Y.; Zhang, X.J.; Li, J.H.; Huang, M. Comparison of high ligation and stripping of the great saphenous vein combined with foam sclerotherapy versus conventional surgery for the treatment of superficial venous varicosities of the lower extremity. Int. J. Clin. Exp. Med. 2015, 8, 7843–7848. [Google Scholar]
- Wittens, C.; Davies, A.H.; Bwkgaard, N.; Broholm, R.; Cavezzi, A.; Chastanet, S.; De Wolf, M.; Eggen, C.; Giannoukas, A.; Gohel, M.; et al. Editor’s Choice—Management of Chronic Venous Disease Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2015, 49, 678–737. [Google Scholar] [CrossRef]
- Bozkurt, A.K.; Lawaetz, M.; Danielsson, G.; Lazaris, A.M.; Pavlovic, M.; Olariu, S.; Rasmussen, L. European College of Phlebology guideline for truncal ablation. Phlebology 2020, 35, 73–83. [Google Scholar] [CrossRef]
- Dillavou, E.D.; Harlander-Locke, M.; Labropoulos, N.; Elias, S.; Ozsvath, K.J. Current state of the treatment of perforating veins. J. Vasc. Surg.-Venous Lymphat. Disord. 2016, 4, 131–135. [Google Scholar] [CrossRef]
- Levy, J.; Khakoo, S.; Barton, R.; Vicary, R. Fatal injection sclerotherapy of a bleeding peptic-ulcer. Lancet 1991, 337, 504. [Google Scholar] [CrossRef]
- Schuman, B.M. The systemic complications of sclerotherapy of esophageal-varices. Gastrointest. Endosc. 1985, 31, 348–349. [Google Scholar] [CrossRef]
- Strussky, L.P.; Asabaev, A.S.; Vakhidov, A.V. Endoscopic sclerotherapy in treatment of portal-hypertension. Klin. Meditsina 1991, 69, 87–89. [Google Scholar]
- Siribumrungwong, B.; Noorit, P.; Wilasrusmee, C.; Leelahavarong, P.; Thakkinstian, A.; Teerawattananon, Y. Cost-utility analysis of great saphenous vein ablation with radiofrequency, foam and surgery in the emerging health-care setting of Thailand. Phlebology 2016, 31, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Barnat, N.; Grisey, A.; Gerold, B.; Yon, S.; Anquez, J.; Aubry, J.F. Efficacy and safety assessment of an ultrasound-based thermal treatment of varicose veins in a sheep model. Int. J. Hyperth. 2020, 37, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Barnat, N.; Grisey, A.; Gerold, B.; Yon, S.; Anquez, J.; Aubry, J.F. Vein wall shrinkage induced by thermal coagulation with high-intensity-focused ultrasound: Numerical modeling and in vivo experiments in sheep. Int. J. Hyperth. 2020, 37, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
- Obermayer, A.; Aubry, J.F.; Barnat, N. Extracorporeal Treatment with High Intensity Focused Ultrasound of an Incompetent Perforating Vein in a Patient with Active Venous Ulcers. Ejves Vasc. Forum 2021, 50, 1–5. [Google Scholar] [CrossRef]
- Barnat, N.; Grisey, A.; Lecuelle, B.; Anquez, J.; Gerold, B.; Yon, S.; Aubry, J.F. Noninvasive vascular occlusion with HIFU for venous insufficiency treatment: Preclinical feasibility experience in rabbits. Phys. Med. Biol. 2019, 64, 025003. [Google Scholar] [CrossRef]
- Strunk, H.M.; Lutzow, C.; Henseler, J.; Mucke, M.; Rauch, M.; Marx, C.; Schild, H.H.; Marinova, M. Mesenteric Vessel Patency Following HIFU Therapy in Patients with Locally Invasive Pancreatic Cancer. Ultraschall Med. 2018, 39, 650–658. [Google Scholar] [CrossRef]
- Whiteley, M.S. High intensity focused ultrasound (HIFU) for the treatment of varicose veins and venous leg ulcers—A new non-invasive procedure and a potentially disruptive technology. Curr. Med. Res. Opin. 2020, 36, 509–512. [Google Scholar] [CrossRef]
- Charrel, T.; Greillier, B. HIFU Varicose Vein Treatment Using Veinsound Device Feasibility Study on Sheep. FocUS Arch. 2021. [Google Scholar] [CrossRef]
- Henderson, P.W.; Lewis, G.K.; Shaikh, N.; Sohn, A.; Weinstein, A.L.; Olbricht, W.L.; Spector, J.A. A portable high-intensity focused ultrasound device for noninvasive venous ablation. J. Vasc. Surg. 2010, 51, 707–711. [Google Scholar] [CrossRef]
- Hwang, J.H.; Zhou, Y.F.; Warren, C.; Brayman, A.A.; Crum, L.A. Targeted Venous Occlusion Using Pulsed High-Intensity Focused Ultrasound. IEEE Trans. Biomed. Eng. 2010, 57, 37–40. [Google Scholar] [CrossRef]
- Senoo, N.; Suzuki, J.; Yoshinaka, K.; Deguchi, J.; Takagi, S.; Miyata, T.; Matsumoto, Y. Development of Noninvasive Vascular Occlusion Method with HIFU. In Proceedings of the 9th International Symposium on Therapeutic Ultrasound, Aix en Provence, France, 24–26 September 2009; p. 153. [Google Scholar]
- Mitragotri, S. Innovation—Healing sound: The use of ultrasound in drug delivery and other therapeutic applications. Nat. Rev. Drug Discov. 2005, 4, 255–260. [Google Scholar] [CrossRef]
- Hynynen, K.; Jolesz, F.A. Demonstration of potential noninvasive ultrasound brain therapy through an intact skull. Ultrasound Med. Biol. 1998, 24, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Agah, R.; Pearce, J.A.; Welch, A.J.; Motamedi, M. Rate process model for arterial tissue thermal damage: Implications on vessel photocoagulation. Lasers Surg. Med. 1994, 15, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, R.; Sasaki, K.; Ishikawa, T.; Suzuki, M.; Umemura, S.-I.; Kushima, M.; Okai, T. Arterial blood flow occlusion by high intensity focused ultrasound and histologic evaluation of its effect on arteries and surrounding tissues. J. Med. Ultrason. 2002, 29, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Takegami, K.; Kaneko, Y.; Watanabe, T.; Maruyama, T.; Matsumoto, Y.; Nagawa, H. Polyacrylamide gel containing egg white as new model for irradiation experiments using focused ultrasound. Ultrasound Med. Biol. 2004, 30, 1419–1422. [Google Scholar] [CrossRef]
- Hoerig, C.L.; Serrone, J.C.; Burgess, M.T.; Zuccarello, M.; Mast, T.D. Prediction and suppression of HIFU-induced vessel rupture using passive cavitation detection in an ex vivo model. J. Ther. Ultrasound 2014, 2, 14. [Google Scholar] [CrossRef]
- Vaezy, S.; Zderic, V. Hemorrhage control using high intensity focused ultrasound. Int. J. Hyperth. 2007, 23, 203–211. [Google Scholar] [CrossRef]
- Yue, Y.; Chen, W.; Wang, Z. The impact of microbubbles-mediated intermitten HIFU on bloodflow in femoral artery of rabbit. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi = J. Biomed. Eng. 2010, 27, 58–61. [Google Scholar]
- Jiang, C.P. Vessel phantom fabrication using rapid prototyping technique for investigating thermal dosage profile in HIFU surgery. Rapid Prototyp. J. 2010, 16, 417–423. [Google Scholar] [CrossRef]
- Pichardo, S.; Milleret, R.; Curiel, L.; Pichot, O.; Chapelon, J.Y. In vitro experimental study on the treatment of superficial venous insufficiency with high-intensity focused ultrasound. Ultrasound Med. Biol. 2006, 32, 883–891. [Google Scholar] [CrossRef]
- Yang, W.J.; Zhou, Y.F. Effect of pulse repetition frequency of high-intensity focused ultrasound on in vitro thrombolysis. Ultrason. Sonochem. 2017, 35, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Croucher, A.; Whiteley, M.; Abu-Bakr, O. One-year results of treatment of incompetent truncal veins and incompetent perforators using high intensity focused ultrasound (HIFU). Phlebology 2022, 37, 23–24. [Google Scholar]
- Ahmed, T.; Portnoy, R.; Chachati, G.; Chait, J.; Alsheekh, A.; Kibrik, P.; Marks, N.; Hingorani, A.; Ascher, E. Correlation of body mass index with recanalization risk after endovenous thermal ablation. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 10, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.R.; Loson, V.; Coria, A.; Fosser, C.M.; Dotta, M.; Katsini, R.; Pared, C.; Moreno, H.B.; Martínez, H. Secondary Ablation of Recanalized Saphenous Vein after Endovenous Thermal Ablation. Ann. Vasc. Surg. 2020, 68, 172–178. [Google Scholar] [CrossRef]
- Mitton, D.; Thornton, M.; Beard, J. Retrograde stripping of recurrent varicose veins. Eur. J. Vasc. Endovasc. Surg. 2001, 22, 90–91. [Google Scholar] [CrossRef]
- Gao, R.D.; Qian, S.Y.; Wang, H.H.; Liu, Y.S.; Ren, S.Y. Strategies and challenges in treatment of varicose veins and venous insufficiency. World J. Clin. Cases 2022, 10, 5946–5956. [Google Scholar] [CrossRef]















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).