
The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of Volunteers and Groups
- (1)
- based on foot geometry parameters—transverse flat foot according to the Wejsflog index (W):
- transverse flat foot (TF),
- normal transverse arch (TNA).
- (2)
- based on the force of pressure on the ground (P) in the forefoot area:
- insufficient pressure in the forefoot (TIP),
- normal pressure in the forefoot (TNP),
- excessive pressure in the front area (TEP).
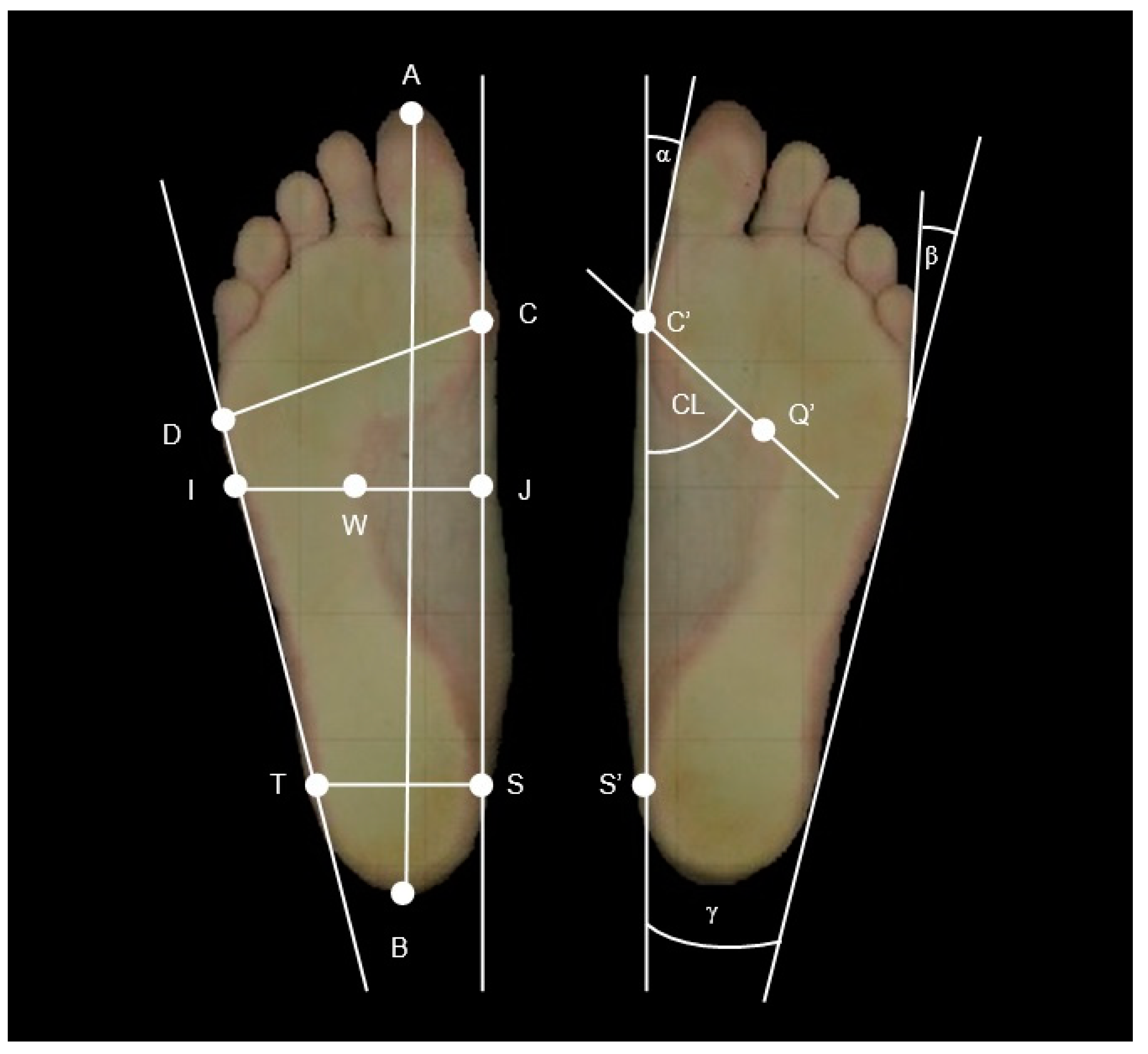
2.2. Podoscope Examination
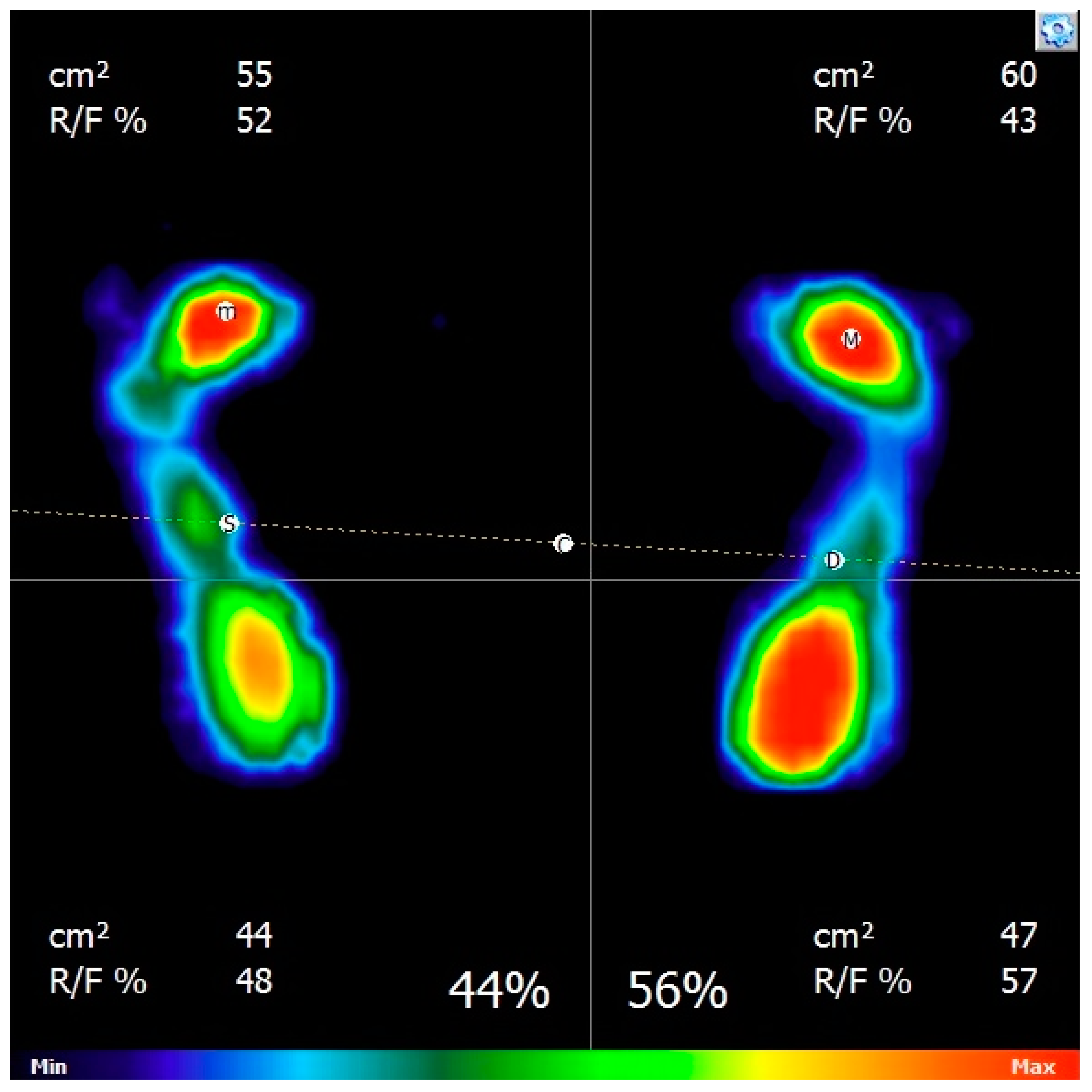
2.3. Baropodometric Examination
2.4. Podiatric Procedures
2.5. Statistical Analysis
3. Results
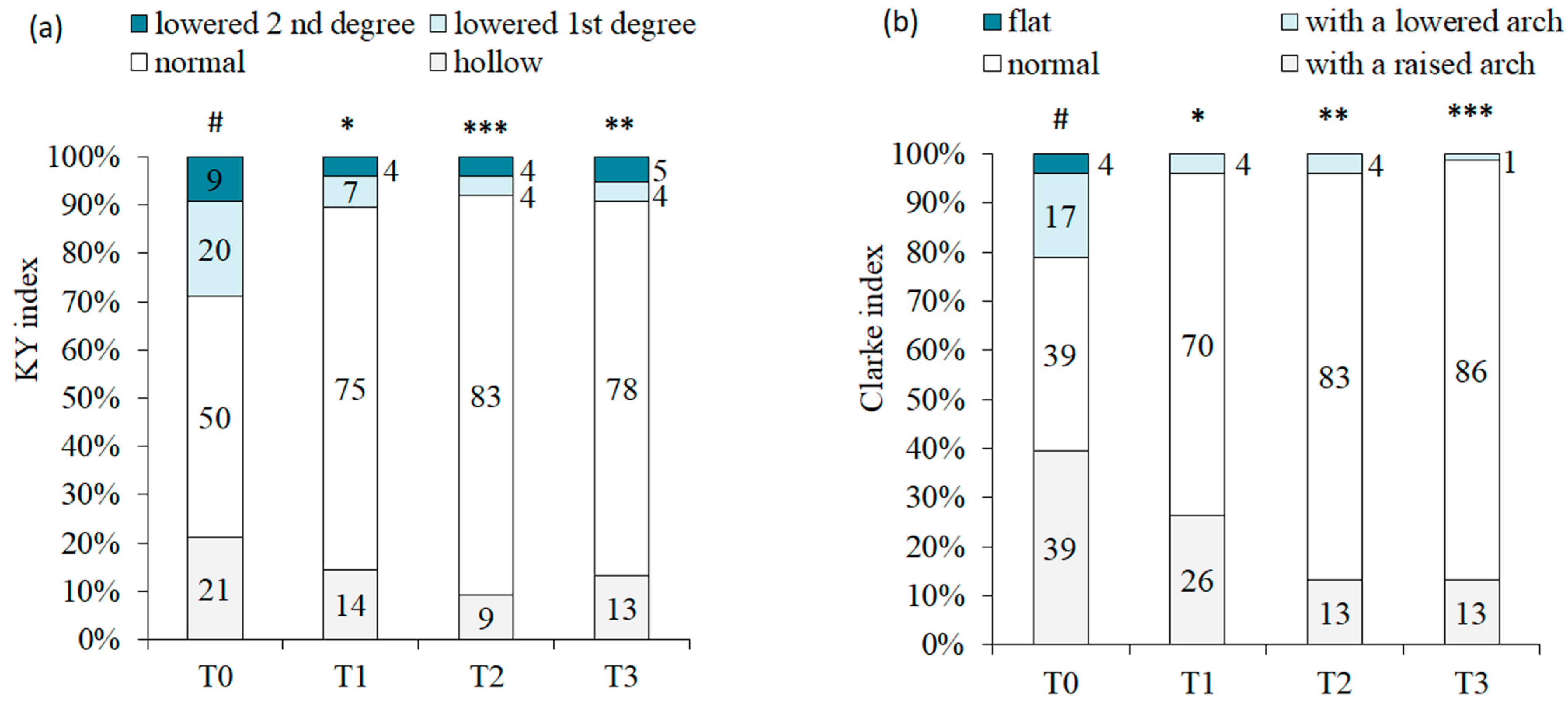
3.1. Evaluation of Changes in Podoscopic Parameters
3.2. Evaluation of Changes in Baropodometric Parameters
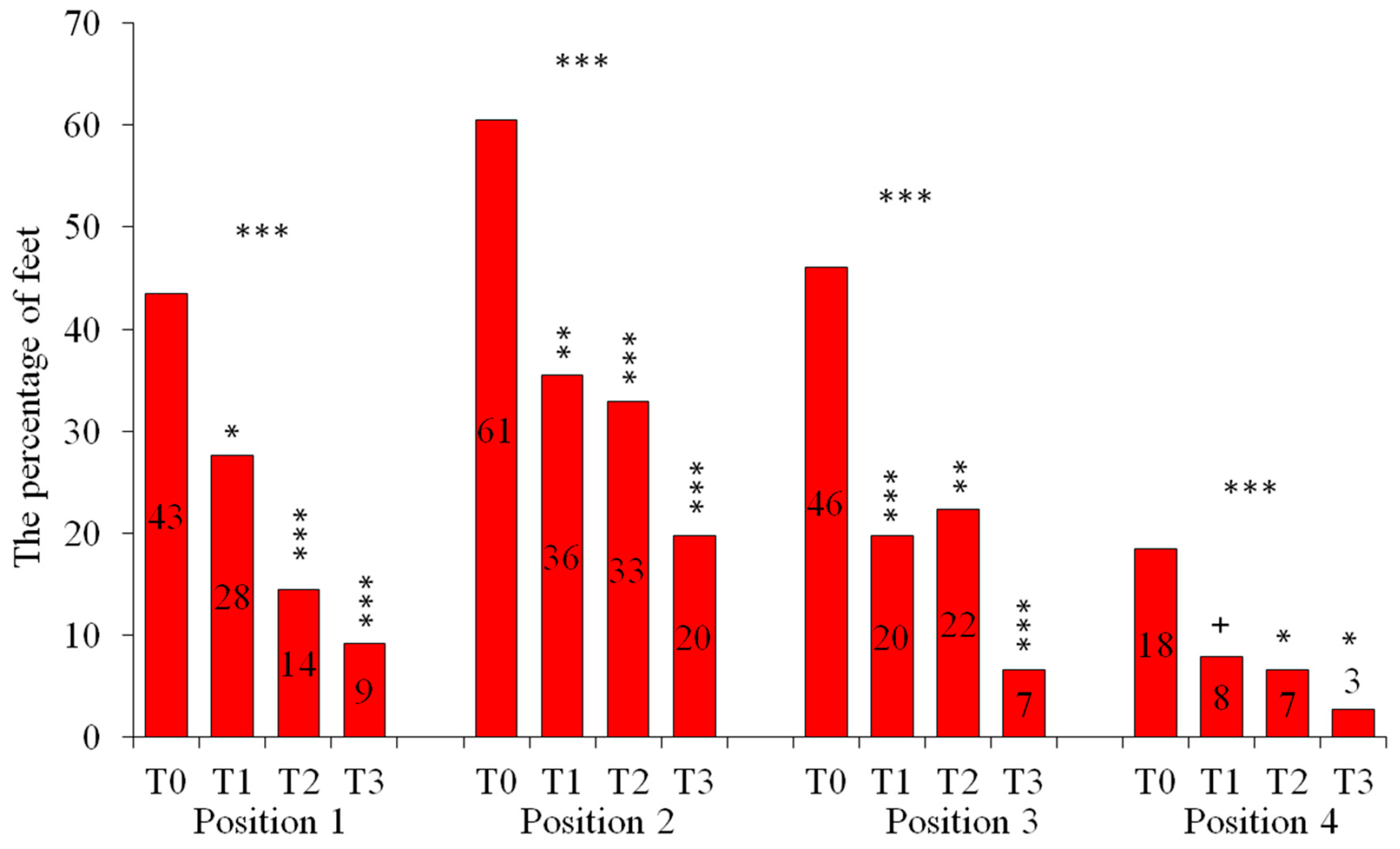
3.3. Assessment of the Presence of Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, H.Y.; Lee, D.T.; Leung, E.M.; Man, C.-W.; Lai, K.-M.; Leung, M.-W.; Wong, I.K. The effects of a foot and toenail care protocol for older adults. Geriatr. Nurs. 2012, 33, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Holloway, S.; Mahoney, K. Periwound skin care considerations for older adults. Br. J. Community Nurs. 2021, 26, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, P.; Mutka, K.; Michalak, M.; Kopciuch, D.; Paczkowska, A.; Zaprutko, T.; Kus, K. Patients’ awareness of the prevention and treatment of the selected podiatry diseases. J. Cosmet. Dermatol. 2022, 21, 2889–2896. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.A.; Soler, F.C. Effect of debridement of plantar hyperkeratoses on gait in older people—An exploratory trial. Arch. Gerontol. Geriatr. 2018, 78, 7–13. [Google Scholar] [CrossRef]
- Stolt, M.; Suhonen, R.; Kielo, E.; Katajisto, J.; Leino-Kilpi, H. Foot health of nurses. A cross-sectional study. Int. J. Nurs. Pract. 2017, 23, 256. [Google Scholar] [CrossRef]
- Bailey, J. Nail and Foot Procedures. Prim. Care 2022, 49, 63–83. [Google Scholar] [CrossRef]
- Elwell, R. The management and treatment of hyperkeratosis. Br. J. Nurs. 2017, 27, 468–470. [Google Scholar] [CrossRef]
- Farndon, L.; Concannon, M.; Stephenson, J. A survey to investigate the association of pain, foot disability and quality of life with corns. J. Foot Ankle Res. 2015, 8, 70. [Google Scholar] [CrossRef]
- Akdemir, O.; Bilkay, U.; Tiftikcioglu, Y.O.; Ozek, C.; Yan, H.; Zhang, F.; Akin, Y. New alternative in treatment of callus. J. Dermatol. 2011, 38, 146–150. [Google Scholar] [CrossRef]
- Papaliodis, D.N.; Vanushkina, M.A.; Richardson, N.G.; DiPreta, J.A. The foot and ankle examination. Med. Clin. N. Am. 2014, 98, 181–182. [Google Scholar] [CrossRef]
- Hagedorn, T.J.; Dufour, A.B.; Riskowski, J.L.; DiPreta, J.A. Foot disorders, foot posture, and foot function: The Framingham foot study. PLoS ONE 2013, 8, e74364. [Google Scholar] [CrossRef]
- Toullec, E. Adult flatfoot. Orthop. Traumatol. Surg. Res. 2015, 101, 11–17. [Google Scholar] [CrossRef]
- Wicart, P. Cavus foot, from neonates to adolescents. Orthop. Traumatol. Surg. Res. 2012, 98, 813–828. [Google Scholar] [CrossRef]
- Menz, H.B.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Hannan, M.T. Foot posture, foot function and low back pain: The Framingham Foot Study. Rheumatology 2013, 52, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.J.; Roddy, E.; Zhang, W.; Menz, H.; Hannan, M.; Peat, G.M. The population prevalence of foot and ankle pain in middle and old age: A systematic review. Pain 2011, 152, 2870–2880. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B. Chronic foot pain in older people. Maturitas 2016, 91, 110–114. [Google Scholar] [CrossRef]
- Rao, S.; Riskowski, J.L.; Hannan, M.T. Musculoskeletal conditions of the foot and ankle: Assessments and treatment options. Best Pract. Res. Clin. Rheumatol. 2012, 26, 345–368. [Google Scholar] [CrossRef] [PubMed]
- Drzał-Grabiec, J.; Podgórska, J.; Rykała, J.; Walicka-Cupryś, K.; Truszczyńska, A. Zmiany w ukształtowaniu stóp u osób starszych. Post Rehab. 2013, 4, 13–19. [Google Scholar]
- Stolt, M.; Suhonen, R.; Puukka, P.; Viitanen, M.; Voutilainen, P.; Leino-Kilpi, H. Foot health and self-care activities of older people in home care. J. Clin. Nurs. 2012, 21, 3082–3095. [Google Scholar] [CrossRef]
- Guidozzi, F. Foot problems in older women. Climacteric 2017, 20, 518–521. [Google Scholar] [CrossRef]
- Awale, A.; Hagedorn, T.J.; Dufour, A.B.; Menz, H.B.; Casey, V.A.; Hannan, M.T. Foot Function, Foot Pain, and Falls in Older Adults: The Framingham Foot Study. Gerontology 2017, 63, 318–324. [Google Scholar] [CrossRef]
- Murahashi, Y.; Iba, K.; Teramoto, A.; Takahashi, K.; Okada, Y.; Kamiya, T.; Takashima, H.; Watanabe, K.; Ohnishi, H.; Yamashita, T. Relationship Between Plantar Callosity and Foot Deformity in Hallux Valgus Using Weightbearing Computed Tomography. J. Foot Ankle Surg. 2021, 60, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Favero, L.; Stecco, C.; Aldegheri, R. Hypermobility of the first ray in ballet dancer. Muscles Ligaments Tendons J. 2013, 21, 282–288. [Google Scholar]
- Fernández- Seguín, L.M.; Diaz Mancha, J.A.; Sánchez Rodríguez, R.; Escamilla Martínez, E.; Gómez Martín, B.; Ramos Ortega, J. Comparison of plantar pressures and contact area between normal and cavus foot. Gait Posture 2014, 39, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Skopljak, A.; Muftic, M.; Sukalo, A.; Masic, I. Pedobarography in diagnosis and clinical application. Acta Inform. Med. 2014, 22, 374–378. [Google Scholar] [CrossRef]
- Rosário, J.L. A review of the utilization of baropodometry in postural assessment. J. Bodyw. Mov. Ther. 2014, 18, 215–219. [Google Scholar] [CrossRef]
- Menz, H.B. Biomechanics of the Ageing Foot and Ankle: A Mini-Review. Gerontology 2015, 61, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Schulze, C.; Lindner, T.; Woitge, S.; Finze, S.; Mittelmeier, W.; Bader, R. Effects of wearing different personal equipment on force distribution at the plantar surface of the foot. Sci. World J. 2013, 16, 827671. [Google Scholar] [CrossRef]
- Gijon-Nogueron, G.; Garcia-Paya, I.; Ortega-Avila, A.B.; Paez-Moguer, J.; Cervera-Marin, J.A. Changes in the parameters of gait after a mechanical debridement of a plantar callosities. J. Tissue Viability 2015, 24, 12–16. [Google Scholar] [CrossRef]
- Hashmi, F.; Nester, C.J.; Wright, C.R.; Lam, S. The evaluation of three treatments for plantar callus: A three-armed randomised, comparative trial using biophysical outcome measures. Trials 2016, 17, 251. [Google Scholar] [CrossRef]
- Hashmi, F.; Nester, C.; Wright, C.; Newton, V.; Lam, S. Characterising the biophysical properties of normal and hyperkeratotic foot skin. J. Foot Ankle Res. 2015, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Corradin, M.; Trepin Kuete Kanah, W.; Dalmau-Pastor, M.; Zornetta, A.; Volpin, A.; Ruggieri, P. Medium-Long-Term Clinical and Radiographic Outcomes of Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Central Primary Metatarsalgia: Do Maestro Criteria Have a Predictive Value in the Preoperative Planning for This Percutaneous Technique? Biomed. Res. Int. 2018, 15, 1947024. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group/ Subgroup | No. of Volunteers | No. of Feet | Age (Years) | BMI (kg/m2) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | SD | Min | Max | Avg. | SD | Min | Max | |||
| AV | 100 | 200 | 68.0 | 6.5 | 50.0 | 85.0 | 33.1 | 5.3 | 21.8 | 46.4 |
| T | 38 | 76 | 66.5 | 7.6 | 50.0 | 83.0 | 32.1 | 5.6 | 23.5 | 46.4 |
| TF | 21 | 42 | 68.9 | 6.6 | 56.0 | 83.0 | 33.0 | 5.6 | 24.4 | 46.4 |
| TNA | 17 | 34 | 63.9 | 7.9 | 50.0 | 78.0 | 31.0 | 5.4 | 23.5 | 40.8 |
| TIP | 16 | 32 | 66.1 | 9.6 | 51.0 | 83.0 | 31.7 | 4.9 | 23.5 | 40.9 |
| TNP | 16 | 32 | 67.6 | 4.7 | 58.0 | 74.0 | 33.5 | 6.0 | 25.5 | 46.4 |
| TEP | 6 | 12 | 65.3 | 8.3 | 50.0 | 71.0 | 29.6 | 6.0 | 24.3 | 39.2 |
| C | 40 | 80 | 69.3 | 6.0 | 54.0 | 85.0 | 33.8 | 5.3 | 21.8 | 43.9 |
| NT | 22 | 44 | 68.3 | 4.8 | 55.0 | 77.0 | 33.3 | 4.6 | 25.8 | 43.8 |
| Parameter | T | C | NT | p + | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | SD | Avg. | SD | Avg. | SD | T vs. C | T vs. NT | C vs. NT | ||
| Foot length (cm) | 24.2 | 1.1 | 24.1 | 1.0 | 24.1 | 1.1 | ns | ns | ns | |
| Foot width (cm) | 9.7 | 0.5 | 9.5 | 0.5 | 9.6 | 0.4 | * | ns | ns | |
| Length of the medial longitudinal arch (cm) | 12.9 | 0.6 | 12.9 | 0.5 | 12.9 | 0.6 | ns | ns | ns | |
| Hallux valgus angle α (°) | 18.4 | 10.9 | 14.4 | 8.8 | 17.6 | 10.8 | * | ns | ns | |
| Varus angle of the fifth toe β (°) | 17.2 | 4.4 | 14.6 | 4.7 | 14.5 | 4.1 | ** | * | ns | |
| Parameter | Foot | % | % | % | p ++ | |||||
| Sztriter–Godunow index (KY) | hollow | 21 | 15 | 32 | * | ns | ** | |||
| normal | 50 | 60 | 45 | |||||||
| lowered 1st degree | 20 | 8 | 11 | |||||||
| lowered 2nd degree | 9 | 18 | 11 | |||||||
| Clarke Angle index (CL) | with a raised arch | 39 | 30 | 27 | ns | ns | ns | |||
| normal | 39 | 49 | 52 | |||||||
| with a lowered arch | 17 | 19 | 20 | |||||||
| flat | 4 | 3 | 0 | |||||||
| Wejsflog index (W) | properly arched | 41 | 49 | 43 | ns | ns | ns | |||
| flat transversely | 59 | 51 | 57 | |||||||
| Heel angle gamma (γ) | slim | 54 | 75 | 70 | * | *** | ** | |||
| normal | 42 | 23 | 30 | |||||||
| flat transversely | 4 | 3 | 0 | |||||||
| T | F | NA | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | SD | p | Post hoc | Avg. | SD | p | Post hoc | Avg. | SD | p | Post hoc | ||
| Foot length (cm) | T0 | 24.15 | 1.14 | ns | 23.70 | 1.01 | ** | 24.81 | 1.01 | ns | |||
| T1 | 24.15 | 1.13 | ns | 23.71 | 1.03 | ns | 24.79 | 0.96 | ns | ||||
| T2 | 24.15 | 1.13 | ns | 23.72 | 1.03 | ns | 24.78 | 0.98 | ns | ||||
| T3 | 24.18 | 1.11 | ns | 23.76 | 1.01 | * | 24.79 | 0.95 | ns | ||||
| Foot width (cm) | T0 | 9.73 | 0.53 | ** | 9.90 | 0.53 | * | 9.47 | 0.43 | ns | |||
| T1 | 9.76 | 0.53 | * | 9.94 | 0.53 | ns | 9.51 | 0.41 | ns | ||||
| T2 | 9.76 | 0.53 | * | 9.94 | 0.53 | ns | 9.50 | 0.42 | ns | ||||
| T3 | 9.78 | 0.52 | *** | 9.96 | 0.52 | ** | 9.52 | 0.42 | ns | ||||
| Length of the medial longitudinal arch (cm) | T0 | 12.93 | 0.61 | ns | 12.70 | 0.54 | + | 13.25 | 0.55 | ns | |||
| T1 | 12.97 | 0.74 | ns | 12.70 | 0.54 | ns | 13.37 | 0.81 | ns | ||||
| T2 | 12.93 | 0.59 | ns | 12.71 | 0.53 | ns | 13.25 | 0.53 | ns | ||||
| T3 | 12.94 | 0.58 | ns | 12.73 | 0.54 | ns | 13.25 | 0.50 | ns | ||||
| Hallux valgus angle α (°) | T0 | 18.38 | 10.90 | *** | 22.44 | 11.20 | *** | 12.48 | 7.26 | ns | |||
| T1 | 17.61 | 11.01 | * | 21.56 | 11.57 | ns | 11.87 | 7.03 | ns | ||||
| T2 | 17.61 | 10.63 | * | 21.42 | 10.98 | + | 12.06 | 7.22 | ns | ||||
| T3 | 16.87 | 10.73 | *** | 20.51 | 11.34 | *** | 11.58 | 7.09 | ns | ||||
| Varus angle of the fifth toe β (°) | T0 | 17.21 | 4.40 | *** | 18.07 | 4.21 | *** | 15.97 | 4.43 | *** | |||
| T1 | 15.97 | 4.16 | *** | 16.49 | 4.27 | ** | 15.23 | 3.93 | ns | ||||
| T2 | 15.33 | 4.54 | *** | 16.16 | 4.46 | *** | 14.13 | 4.46 | *** | ||||
| T3 | 15.39 | 4.44 | *** | 16.24 | 4.98 | *** | 14.16 | 3.21 | *** | ||||
| Parameter | T | C | NT | p + | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | SD | Avg. | SD | Avg. | SD | T vs. C | T vs. NT | C vs. NT | ||
| Total feet pressure surface (cm2) | 113.7 | 27.6 | 114.5 | 22.4 | 115.5 | 25.7 | ns | ns | ns | |
| Area of pressure front zone (cm2) | 61.2 | 17.4 | 61.5 | 14.2 | 62.8 | 17.5 | ns | ns | ns | |
| Pressure of the front zone of the foot (%) | 40.7 | 11.1 | 40.3 | 9.3 | 40.6 | 10.9 | ns | ns | ns | |
| Foot area | Pressure category | % | % | % | p ++ | |||||
| Front of the foot | insufficient | 45 | 45 | 43 | ns | ns | ns | |||
| normal | 38 | 44 | 36 | |||||||
| excessive | 17 | 11 | 20 | |||||||
| Rear of the foot | insufficient | 17 | 11 | 20 | ns | ns | ns | |||
| normal | 38 | 44 | 36 | |||||||
| excessive | 45 | 45 | 43 | |||||||
| EP | NP | IP | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | SD | p | Post hoc | Avg. | SD | p | Post hoc | Avg. | SD | p | Post hoc | ||
| Total area of the load area (cm2) | T0 | 112.3 | 20.0 | ns | ns | 127.2 | 30.1 | ns | ns | 102.7 | 23.0 | ns | ns |
| T1 | 118.7 | 18.7 | ns | 123.6 | 38.6 | ns | 104.2 | 21.9 | ns | ||||
| T2 | 110.4 | 23.9 | ns | 122.1 | 31.0 | ns | 108.9 | 24.9 | ns | ||||
| T3 | 112.1 | 21.0 | ns | 122.5 | 29.3 | ns | 108.0 | 23.4 | ns | ||||
| Surface loaded front area of the foot (cm2) | T0 | 65.3 | 12.6 | ns | ns | 69.9 | 17.4 | ns | ns | 52.2 | 14.6 | ns | ns |
| T1 | 67.2 | 10.8 | ns | 69.4 | 19.0 | ns | 54.0 | 14.0 | ns | ||||
| T2 | 63.9 | 14.5 | ns | 66.4 | 18.0 | ns | 56.2 | 14.9 | ns | ||||
| T3 | 63.3 | 12.7 | ns | 66.4 | 18.6 | ns | 55.8 | 15.2 | ns | ||||
| Load the front area of the foot (%) | T0 | 56.62 | 6.25 | * | ns | 44.97 | 3.32 | ns | ns | 31.06 | 6.56 | ns | ns |
| T1 | 53.69 | 6.54 | ns | 44.24 | 7.03 | ns | 33.12 | 6.28 | ns | ||||
| T2 | 53.15 | 10.78 | ns | 43.34 | 6.60 | ns | 33.47 | 6.36 | ns | ||||
| T3 | 47.77 | 7.21 | ** | 42.24 | 7.03 | ns | 33.68 | 7.90 | ns | ||||
| The Presence of Pain | T | C | NT | p | ||
|---|---|---|---|---|---|---|
| % | T vs. C | T vs. NT | C vs. NT | |||
| Pain when standing on straight legs (position 1) | 43 | 30 | 23 | ns | * | ns |
| Increased pain when loading the forefoot (position 2) | 61 | 38 | 48 | ** | ns | ns |
| Stabbing in the forefoot when walking (position 3) | 46 | 14 | 14 | *** | *** | ns |
| Pain when loading the hindfoot (position 4) | 18 | 18 | 16 | ns | ns | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antończak, P.P.; Hartman-Petrycka, M.; Garncarczyk, A.; Adamczyk, K.; Wcisło-Dziadecka, D.; Błońska-Fajfrowska, B. The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women. Appl. Sci. 2023, 13, 4319. https://doi.org/10.3390/app13074319
Antończak PP, Hartman-Petrycka M, Garncarczyk A, Adamczyk K, Wcisło-Dziadecka D, Błońska-Fajfrowska B. The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women. Applied Sciences. 2023; 13(7):4319. https://doi.org/10.3390/app13074319
Chicago/Turabian StyleAntończak, Paweł Piotr, Magdalena Hartman-Petrycka, Agnieszka Garncarczyk, Katarzyna Adamczyk, Dominika Wcisło-Dziadecka, and Barbara Błońska-Fajfrowska. 2023. "The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women" Applied Sciences 13, no. 7: 4319. https://doi.org/10.3390/app13074319
APA StyleAntończak, P. P., Hartman-Petrycka, M., Garncarczyk, A., Adamczyk, K., Wcisło-Dziadecka, D., & Błońska-Fajfrowska, B. (2023). The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women. Applied Sciences, 13(7), 4319. https://doi.org/10.3390/app13074319