
Numerical Investigation of the Relationship between Anastomosis Angle and Hemodynamics in Ridged Spiral Flow Bypass Grafts

Abstract
1. Introduction
2. Materials and Methods
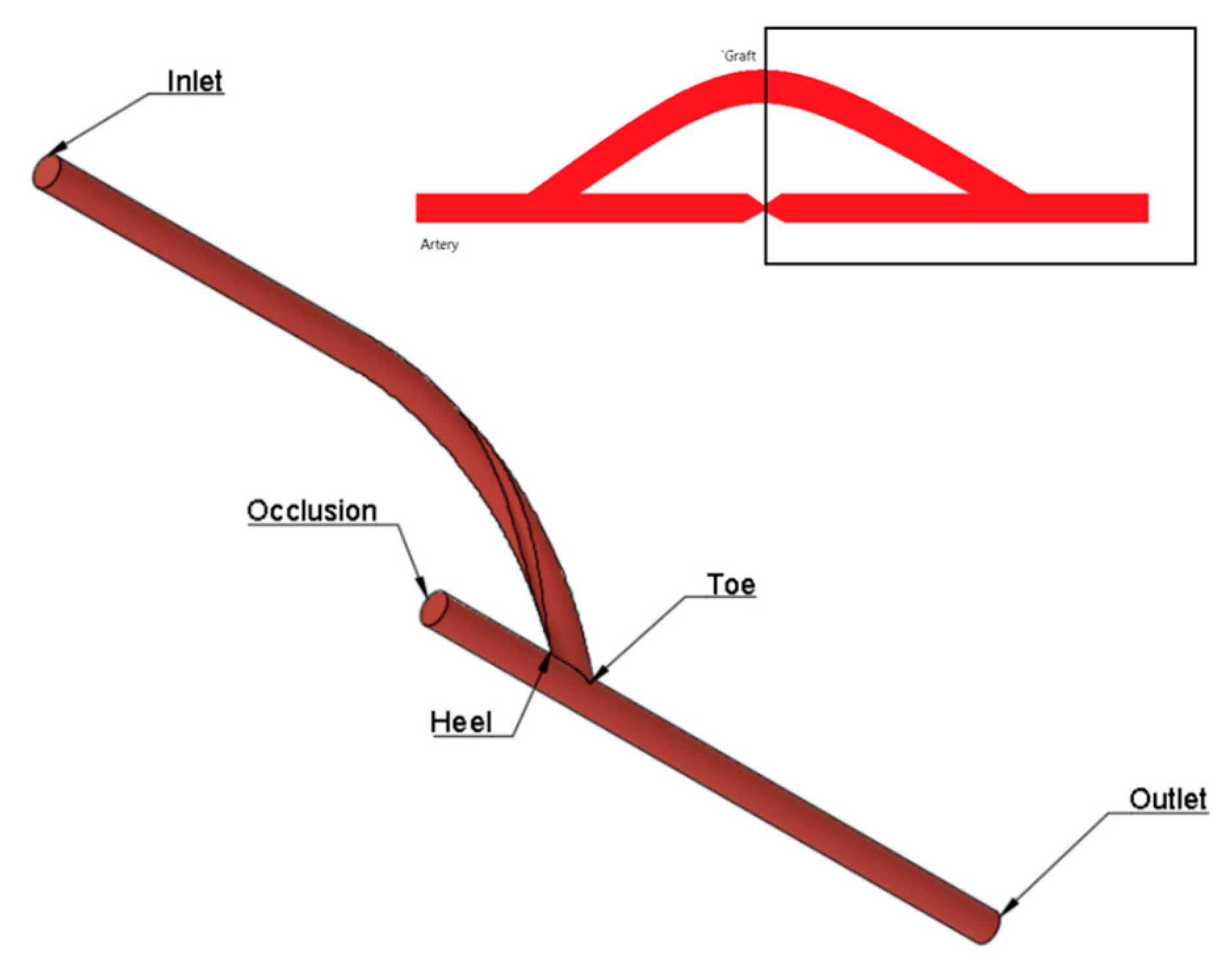
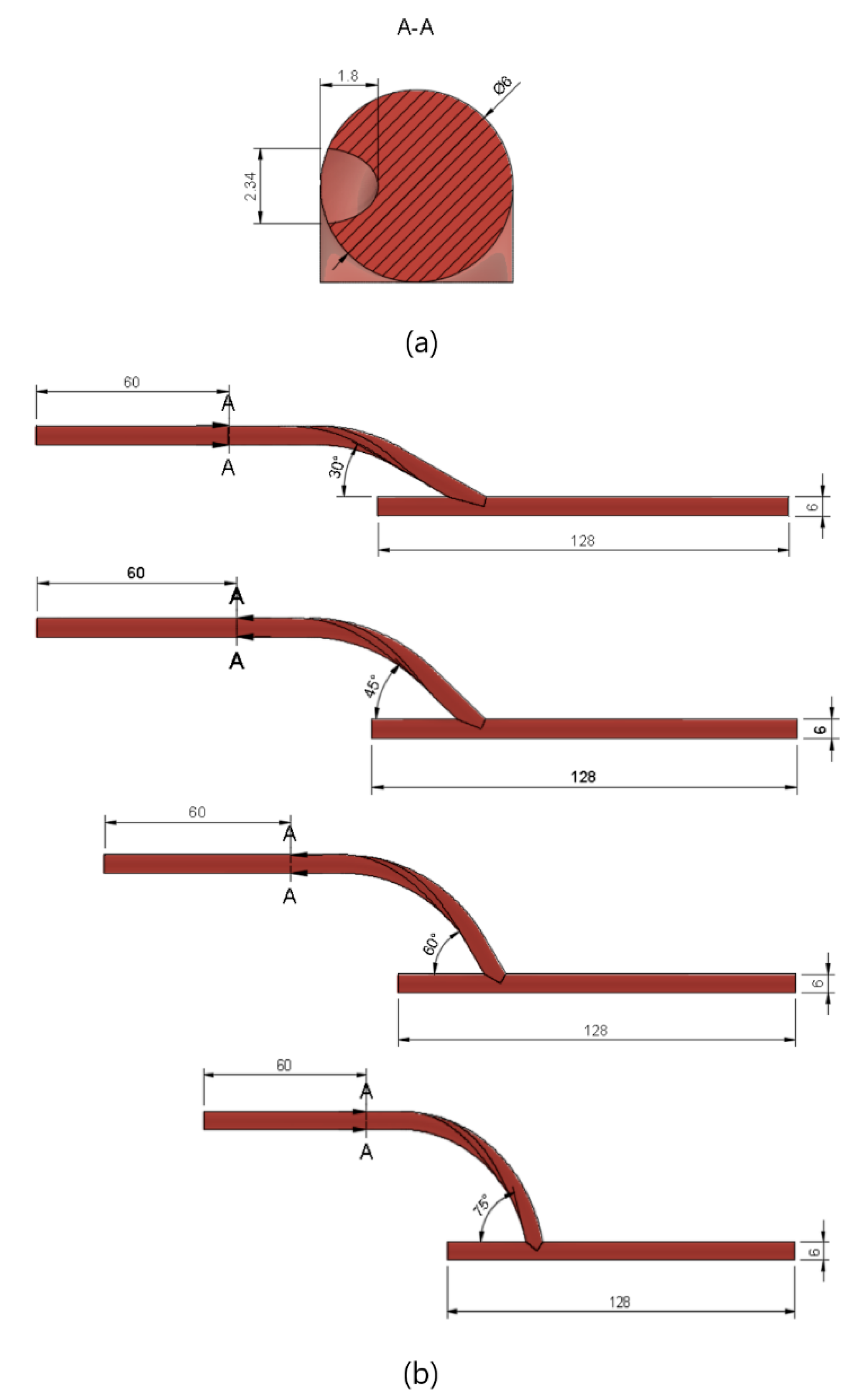
2.1. Geometry
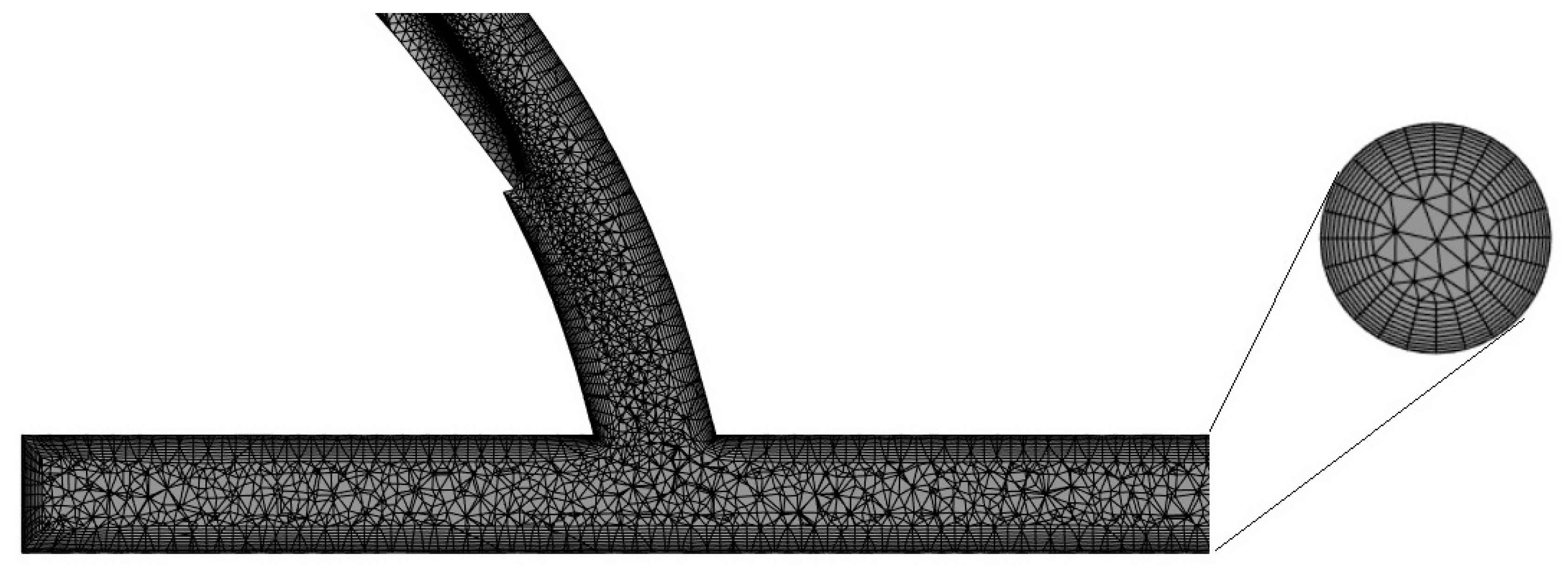
2.2. Mesh Generation
2.3. Determination of the Optimal Anastomosis Angle
2.4. Comparison of Performance between a Conventional Graft and Spiral-Flow-Inducing Graft
3. Results
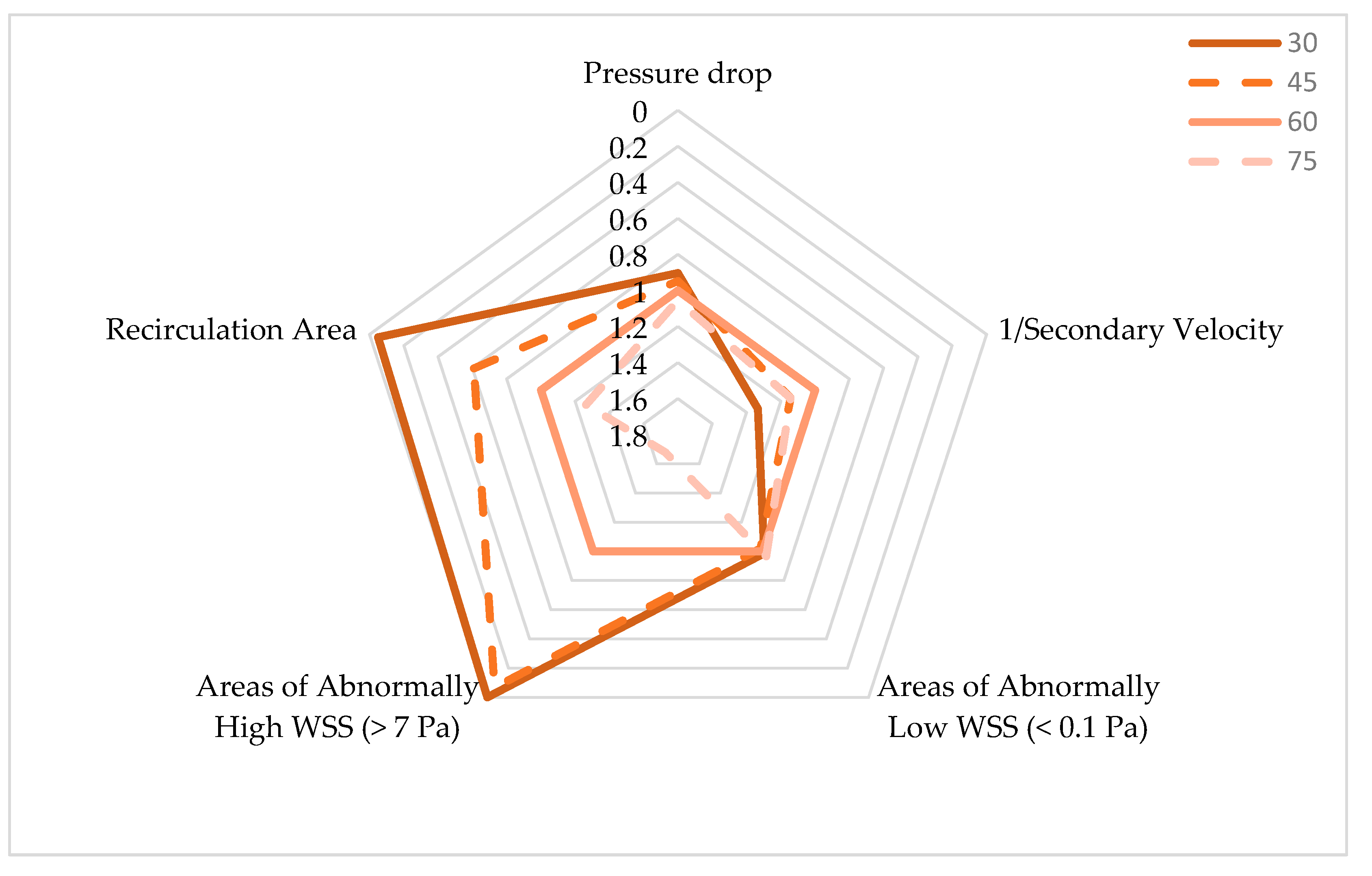
3.1. Optimization of Anastomosis Angle
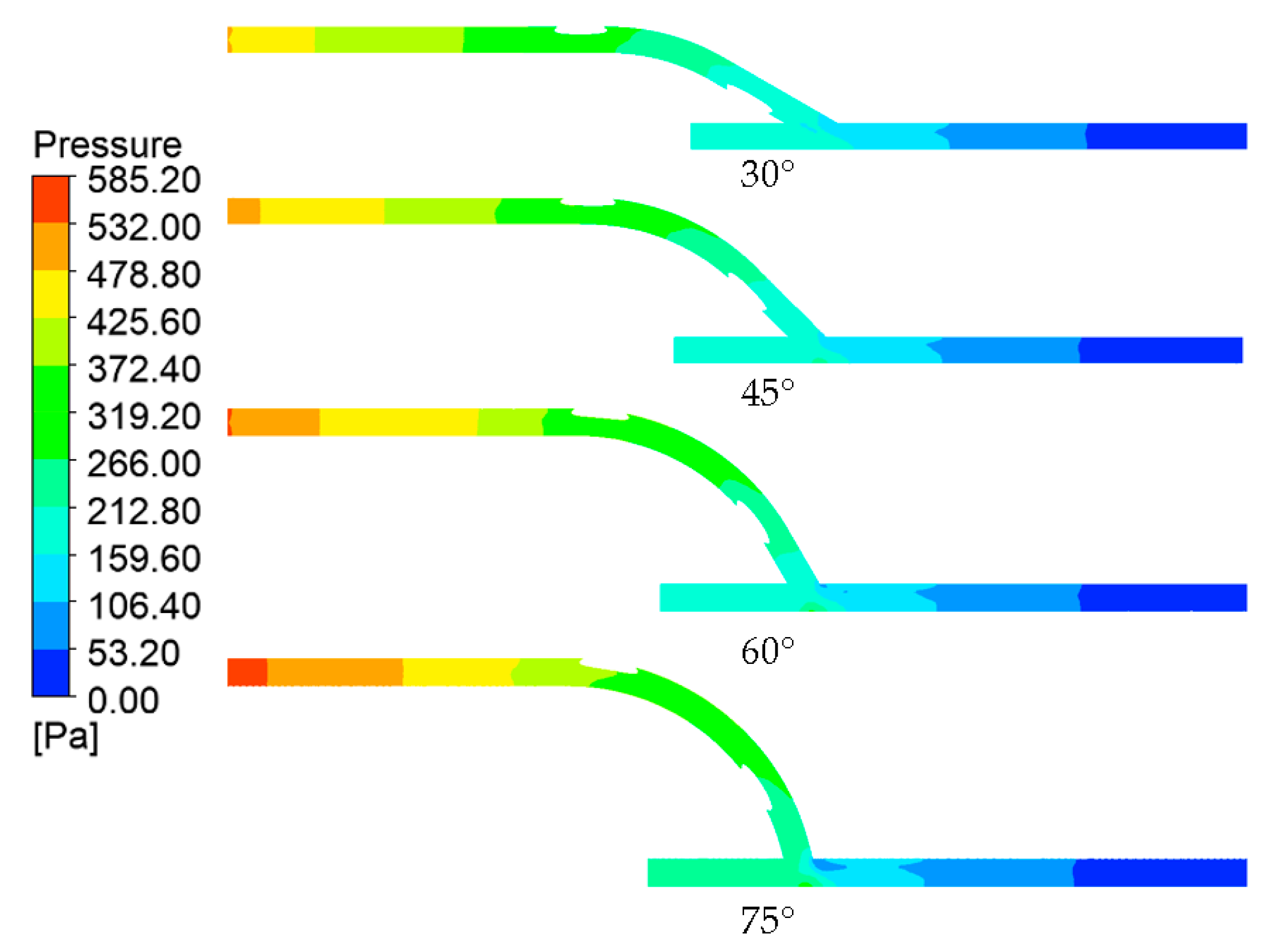
3.1.1. Pressure Drop
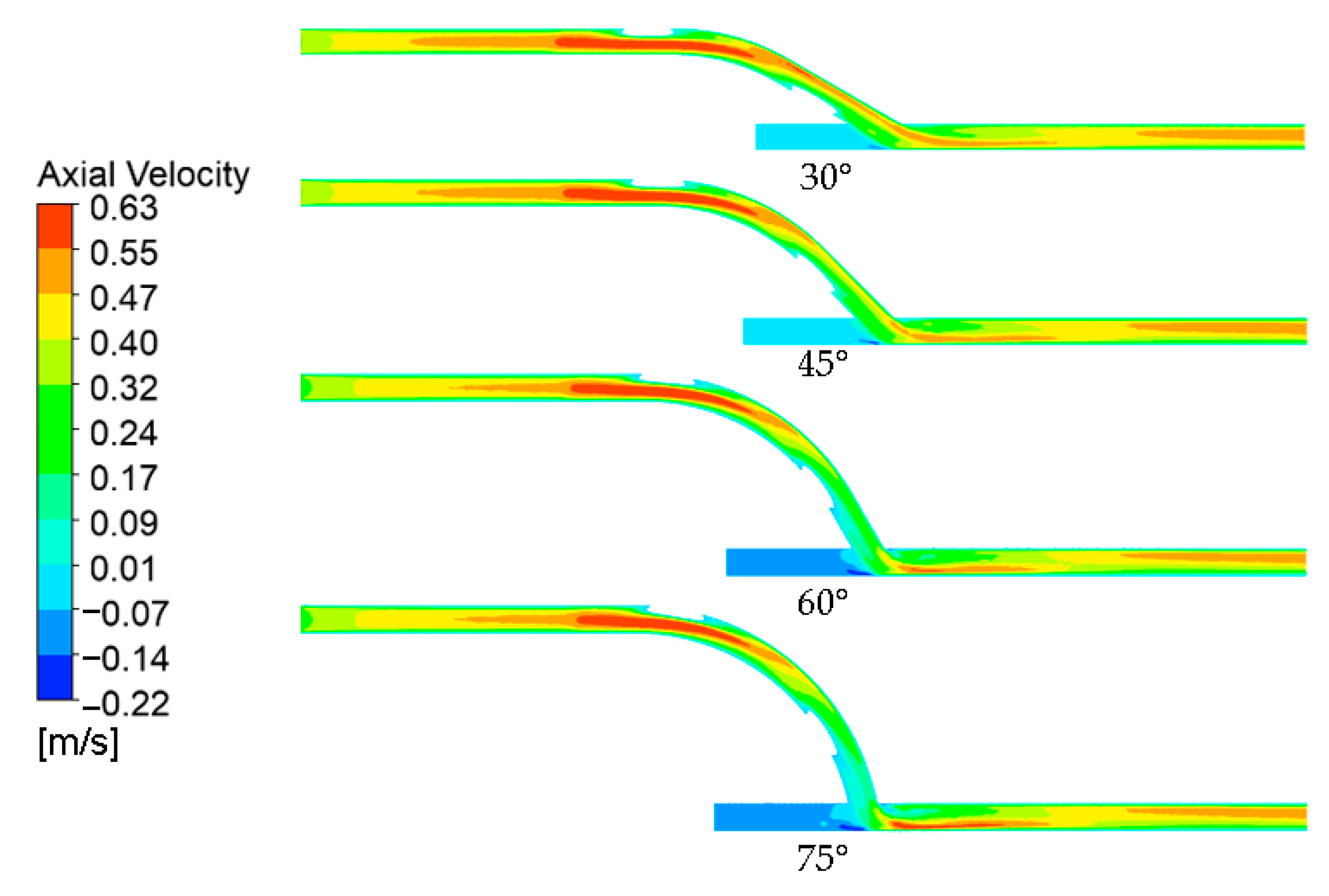
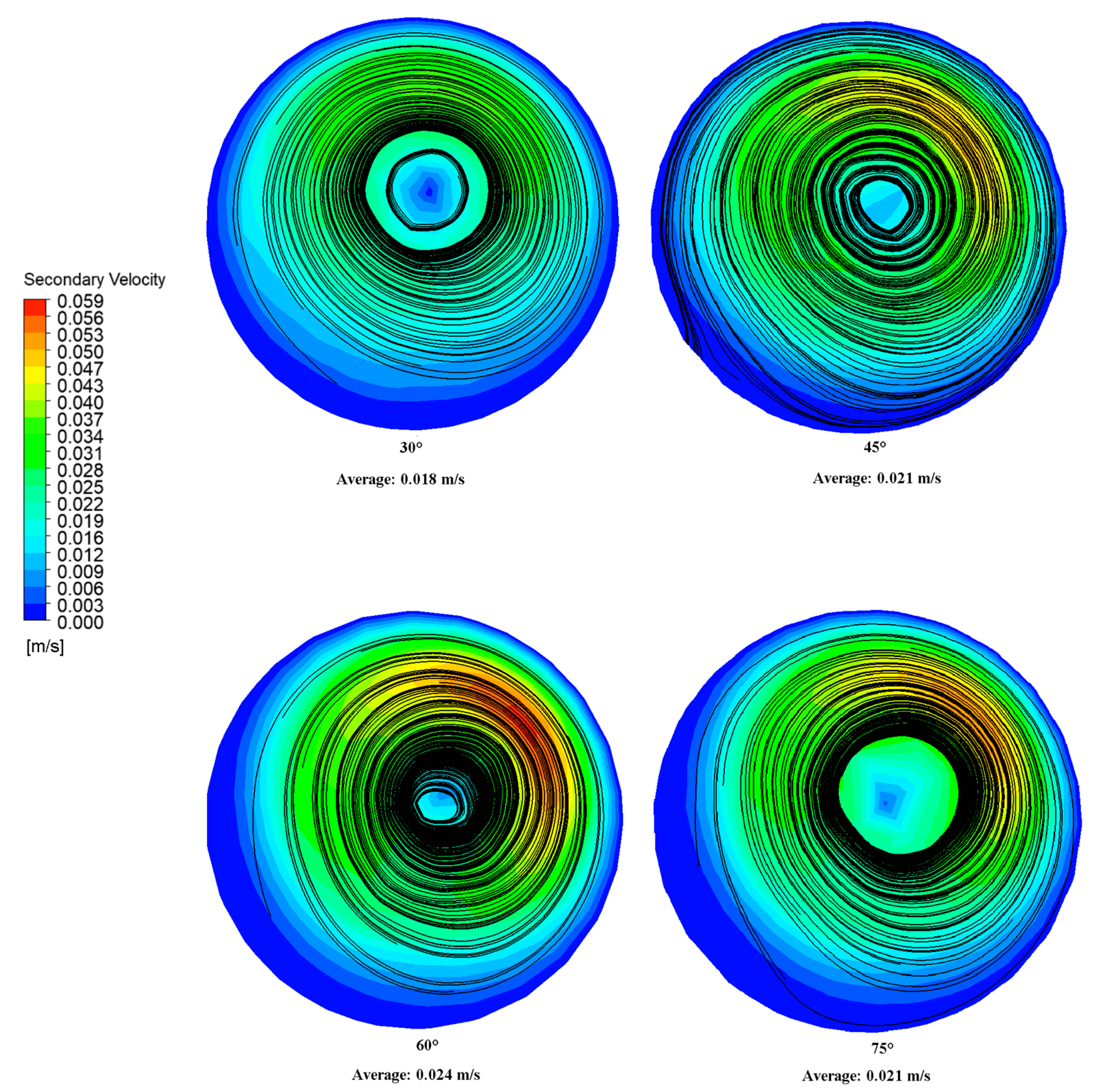
3.1.2. Axial Velocity and Secondary Velocity
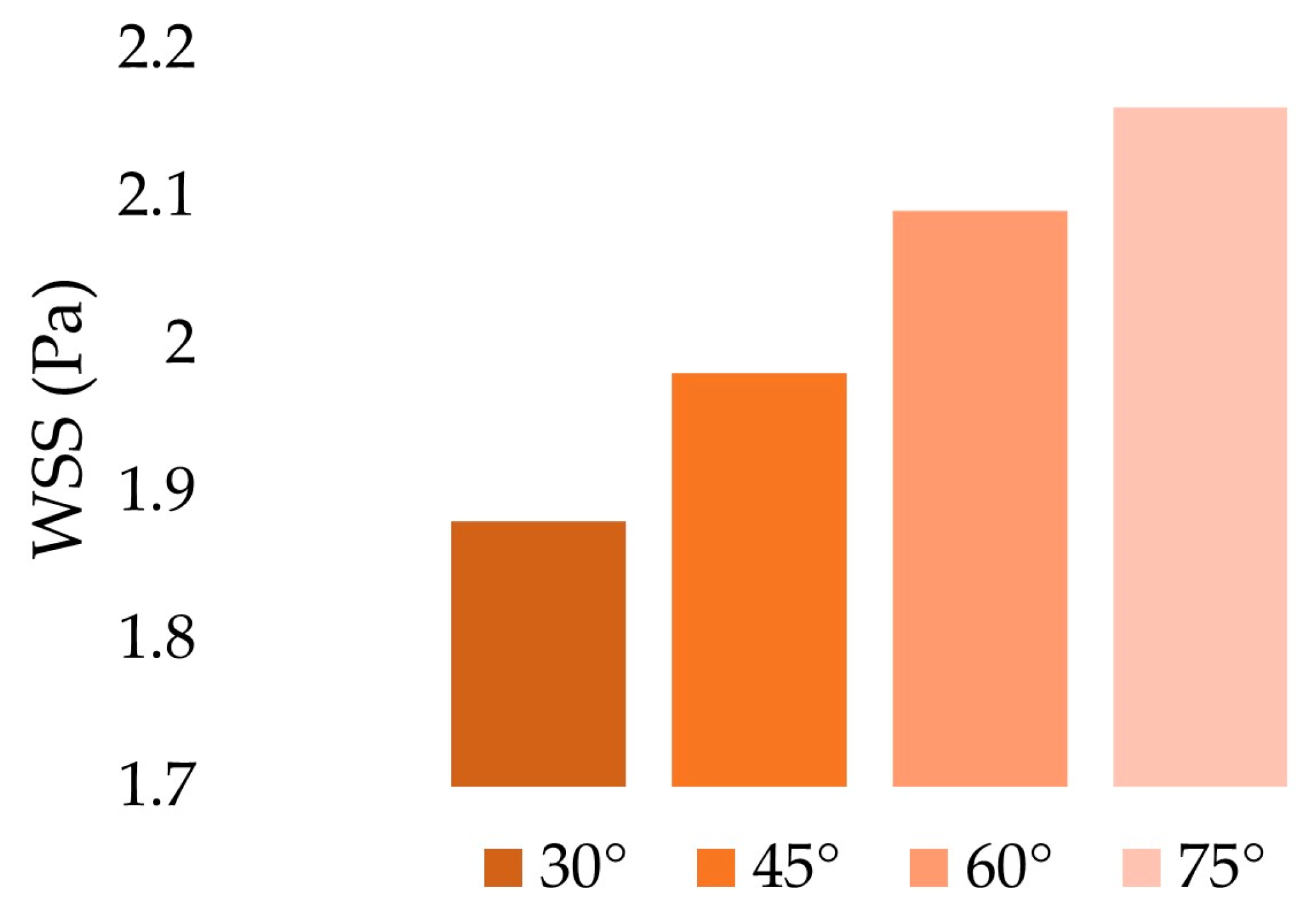
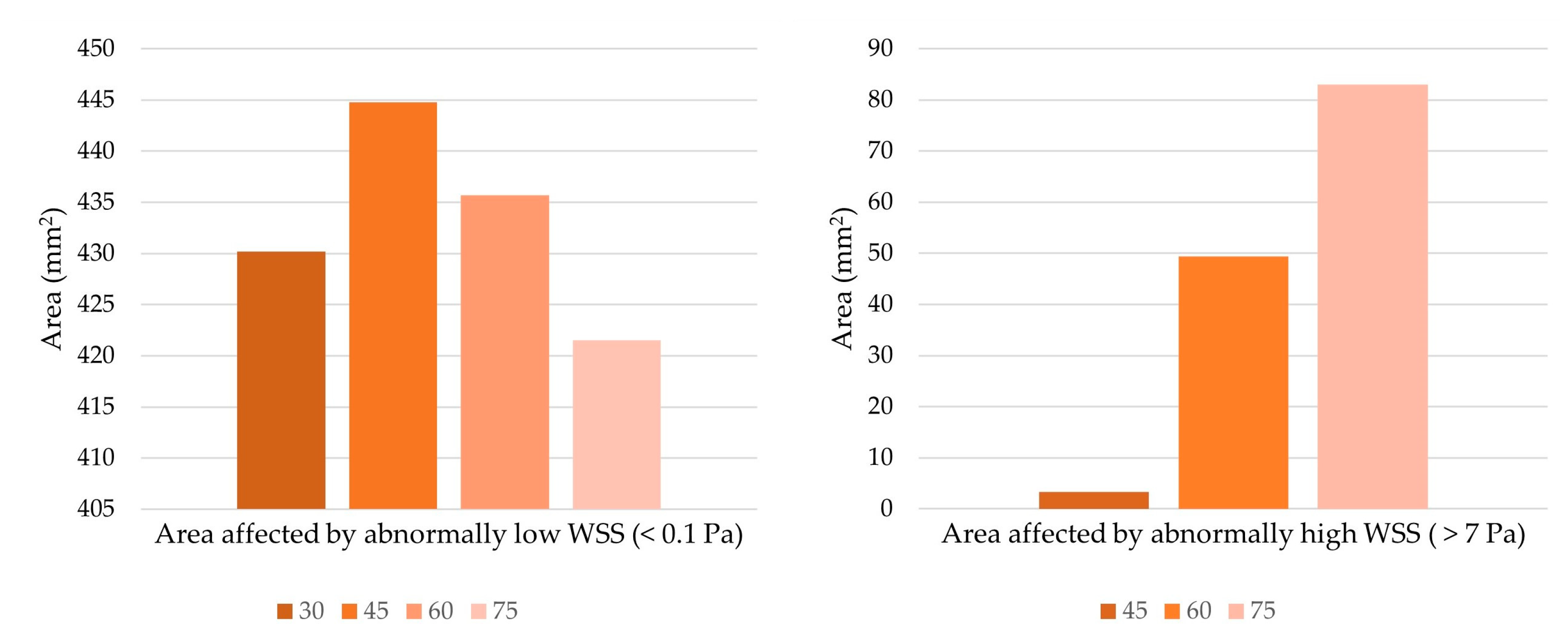
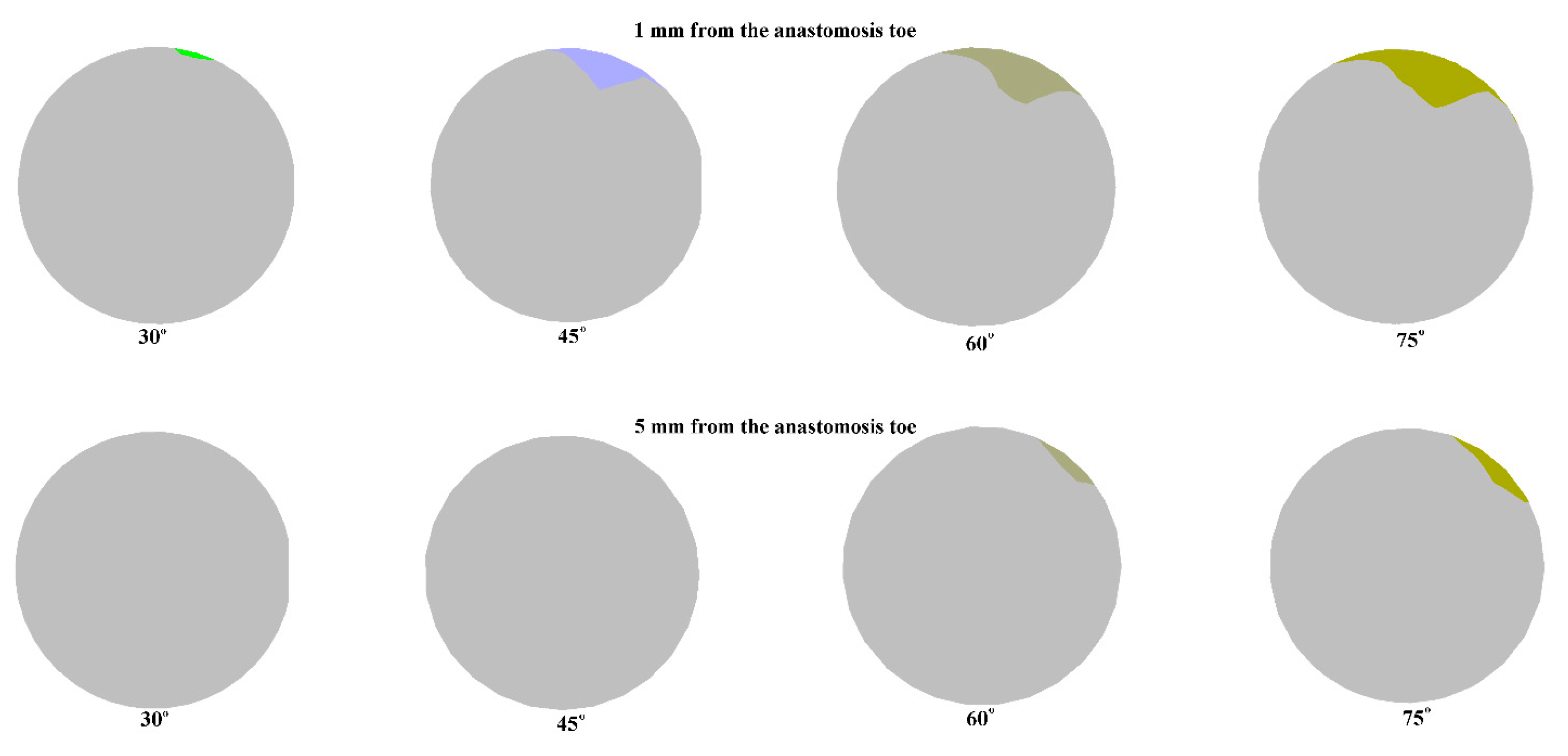
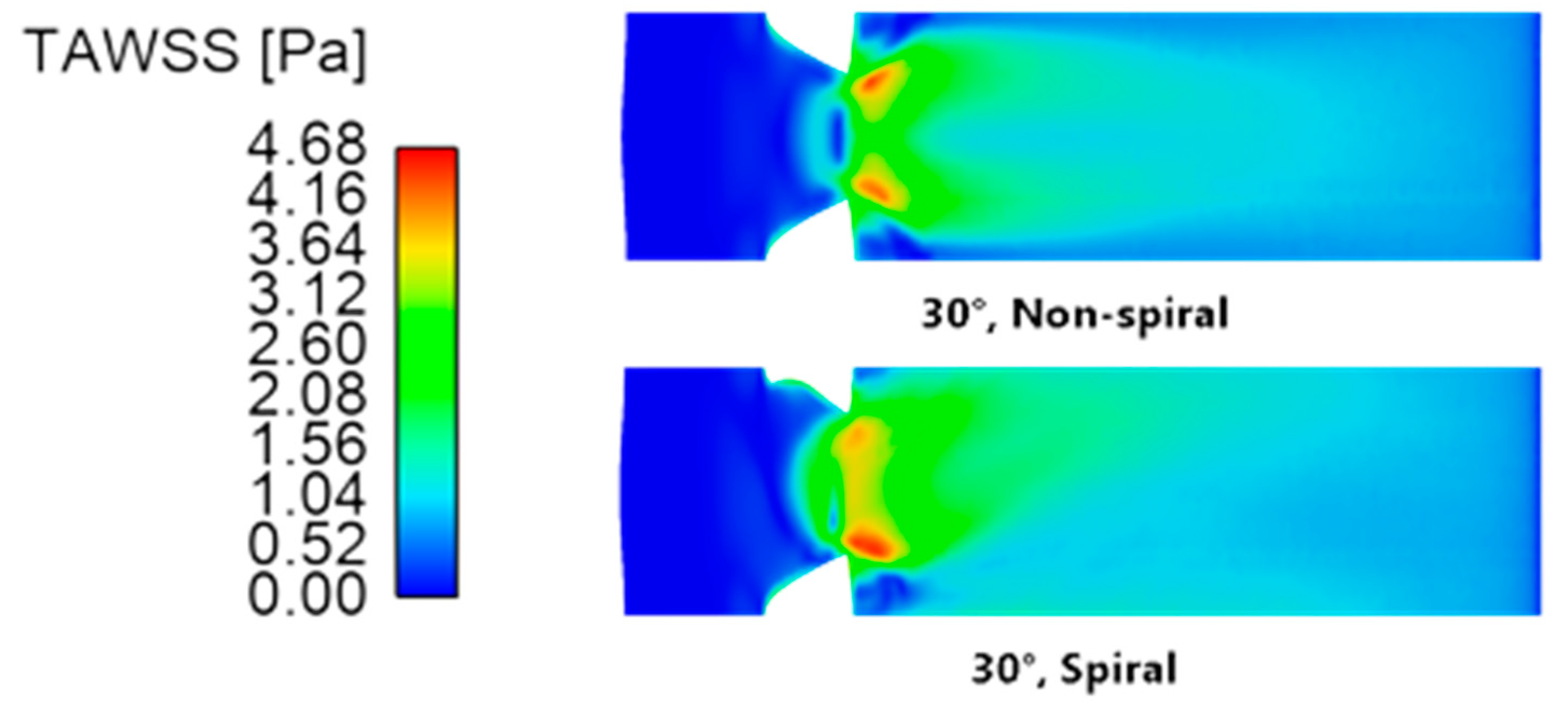
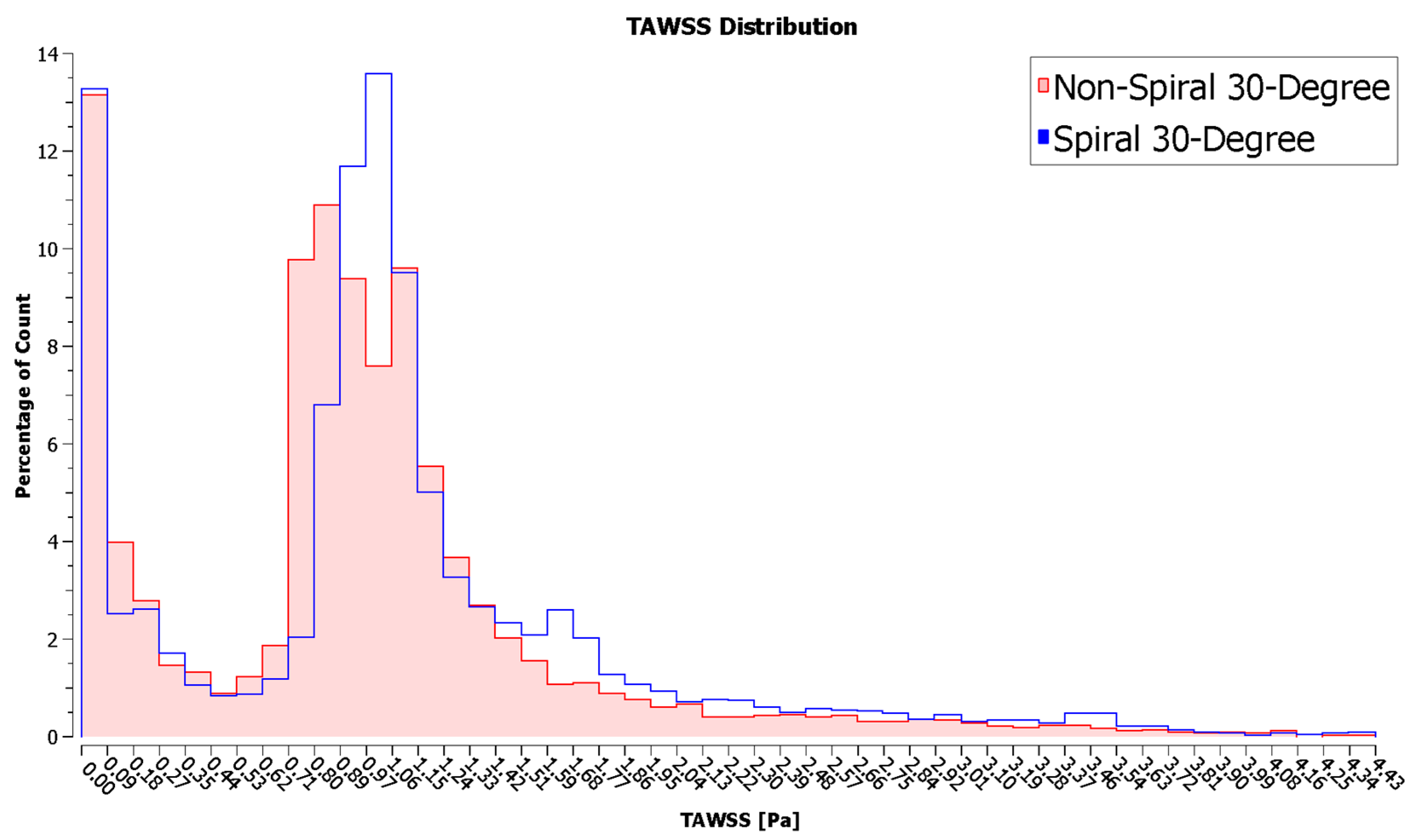
3.1.3. Wall Shear Stress
3.1.4. Recirculation
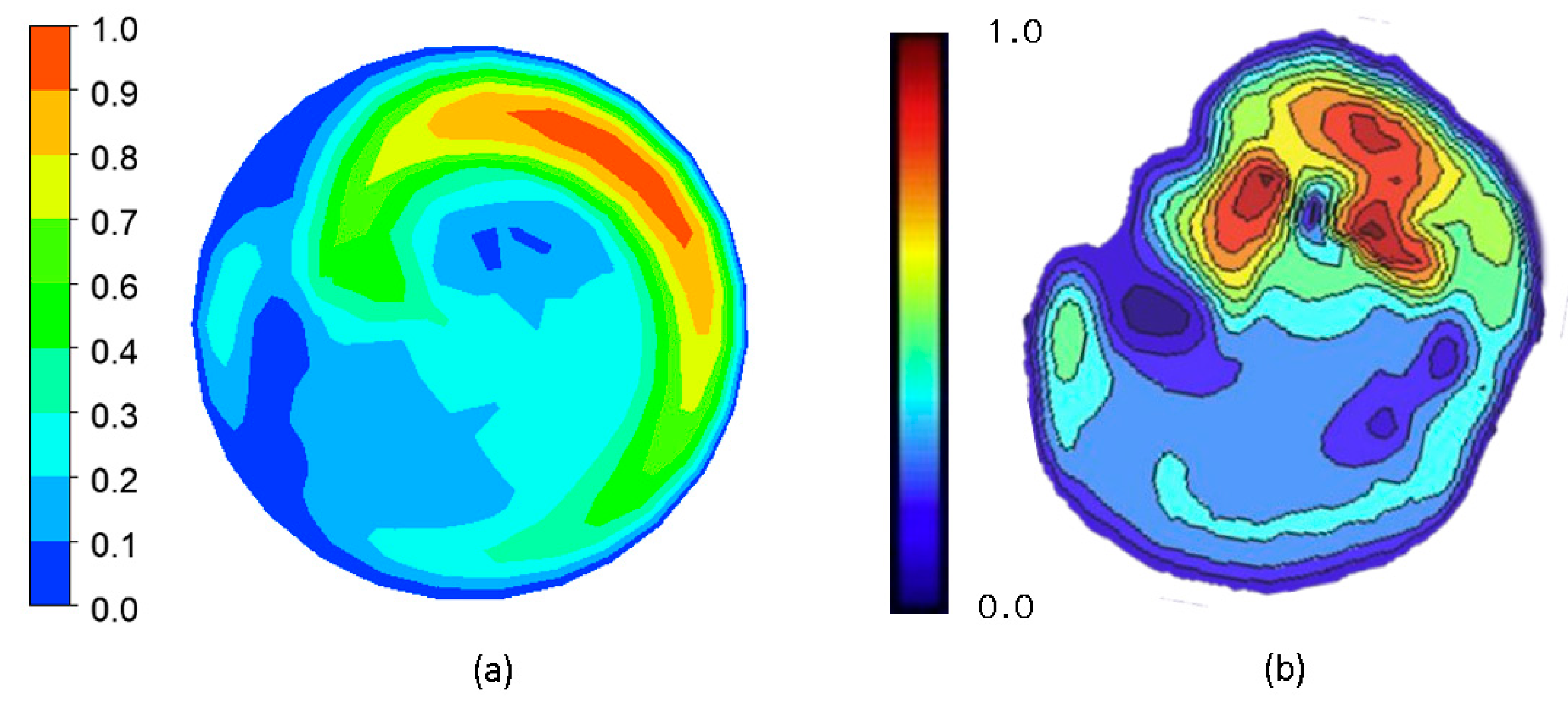
3.2. Data Validation
4. Discussion
4.1. Optimal Anastomosis Angle
4.2. Comparison of Spiral-Flow-Inducing Graft Design vs. Conventional Graft Design
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Aaronson, P.I.; Ward, J.T.; Connolly, M.J. The Cardiovascular System at a Glance, 4th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2012. [Google Scholar]
- Pashneh-Tala, S.; MacNeil, S.; Claeyssens, F. The Tissue-Engineered Vascular Graft—Past, Present, and Future. Tissue Eng. Part B Rev. 2016, 22, 68–100. [Google Scholar] [CrossRef] [PubMed]
- Braga, S.F.; Neves, J.R.; Ferreira, J.; Carrilho, C.; Simões, J.C.; Mesquita, A. Neointimal Hyperplasia. Port. J. Card. Thorac. Vasc. Surg. 2021, 26, 213–217. [Google Scholar] [CrossRef]
- Binns, R.L.; Ku, D.N.; Stewart, M.T.; Ansley, J.P.; Coyle, K.A. Optimal graft diameter: Effect of wall shear stress on vascular healing. J. Vasc. Surg. 1989, 10, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Hathcock, J.J. Flow Effects on Coagulation and Thrombosis. Arter. Thromb. Vasc. Biol. 2006, 26, 1729–1737. [Google Scholar] [CrossRef]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef]
- Malik, J.; Tuka, V.; Tesař, V. Local Hemodynamics of the Vascular Access for Hemodialysis. Kidney Blood Press. Res. 2009, 32, 59–66. [Google Scholar] [CrossRef]
- Totorean, A.F.; Bernad, S.I.; Hudrea, I.C.; Susan-Resiga, R.F. Competitive flow and anastomosis angle influence on bypass hemodynamics in unsteady flow conditions. AIP Conf. Proc. 2017, 1863, 030013. [Google Scholar] [CrossRef]
- Quicken, S.; de Bruin, Y.; Mees, B.; Tordoir, J.; Delhaas, T.; Huberts, W. Computational study on the haemodynamic and mechanical performance of electrospun polyurethane dialysis grafts. Biomech. Model. Mechanobiol. 2020, 19, 713–722. [Google Scholar] [CrossRef]
- Giuliano, L.V.; Buffo, A.; Vanni, M.; Frungieri, G. Micromechanics and strength of agglomerates produced by spray drying. JCIS Open 2023, 9, 100068. [Google Scholar] [CrossRef]
- Giuliano, L.V.; Buffo, A.; Vanni, M.; Lanotte, A.S.; Arima, V.; Bianco, M.; Baldassarre, F.; Frungieri, G. Response of shear-activated nanotherapeutic particles in a clot-obstructed blood vessel by CFD-DEM simulations. Can. J. Chem. Eng. 2022, 100, 3562–3574. [Google Scholar] [CrossRef]
- Ma, P.; Lai, X.; Luo, Z.; Chen, Y.; Loh, X.J.; Ye, E.; Li, Z.; Wu, C.; Wu, Y.-L. Recent advances in mechanical force-responsive drug delivery systems. Nanoscale Adv. 2022, 4, 3462–3478. [Google Scholar] [CrossRef] [PubMed]
- Houston, J.G.; Gandy, S.J.; Sheppard, D.G.; Dick, J.B.; Belch, J.J.; Stonebridge, P.A. Two-dimensional flow quantitative MRI of aortic arch blood flow patterns: Effect of age, sex, and presence of carotid atheromatous disease on prevalence of spiral blood flow. J. Magn. Reson. Imaging 2003, 18, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Baratchi, S.; Chen, Y.-C.; Peter, K. Helical flow: A means to identify unstable plaques and a new direction for the design of vascular grafts and stents. Atherosclerosis 2020, 300, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.H.; Tkatch, C.; Newman, R.; Grimme, W.; Vainchtein, D.; Kresh, J.Y. The mechanics of spiral flow: Enhanced washout and transport. Artif. Organs 2019, 43, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.; Javadzadegan, A.; Zhang, Z.; Afrouzi, H.H.; Omidi, M. Effect of aortic spiral blood flow on wall shear stress in stenosed left main coronary arteries with varying take-off angle, stenosis severity and eccentricity. J. Mech. Sci. Technol. 2018, 32, 4003–4011. [Google Scholar] [CrossRef]
- Hasan, M.; Alam Maruf, M.; Ali, M. Effects of non Newtonian spiral blood flow through arterial stenosis. AIP Conf. Proc. 2016, 1754, 40013. [Google Scholar] [CrossRef]
- El Sayed, H.F.; Davies, M. Early Results of Using the Spiral Flow AV Graft: Is It a Breakthrough Solution to a Difficult Problem? J. Vasc. Surg. 2015, 62, 811. [Google Scholar] [CrossRef]
- Yaseen, M.; Rawat, S.K.; Kumar, M. Hybrid nanofluid (MoS2–SiO2/water) flow with viscous dissipation and Ohmic heating on an irregular variably thick convex/concave-shaped sheet in a porous medium. Heat Transf. 2022, 51, 789–817. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, G.; Murthy, D. Experimental Investigation on Thermal Performance Characteristics of Rotating Packed Bed. Exp. Heat Transf. 2022, 36, 331–343. [Google Scholar] [CrossRef]
- Kumar, G.; Murthy, D. A multiresolution wavelet optimised finite-difference method for simulation of thermal regenerator. Therm. Sci. Eng. Prog. 2020, 19, 100669. [Google Scholar] [CrossRef]
- Yaseen, M.; Rawat, S.K.; Kumar, M. Cattaneo–Christov heat flux model in Darcy–Forchheimer radiative flow of MoS2–SiO2/kerosene oil between two parallel rotating disks. J. Therm. Anal. Calorim. 2022, 147, 10865–10887. [Google Scholar] [CrossRef]
- Li, Y.; Shi, G.; Du, J.; Wang, J.; Bian, P. Analysis and preparation of rotational flow mechanism of artificial blood vessel with spiral folds on inner wall. Biomech. Model. Mechanobiol. 2018, 18, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Soler, A.; Kabinejadian, F.; Slevin, M.A.; Bartolo, P.J.; Keshmiri, A. Optimisation of a Novel Spiral-Inducing Bypass Graft Using Computational Fluid Dynamics. Sci. Rep. 2017, 7, 1865. [Google Scholar] [CrossRef]
- Kabinejadian, F.; McElroy, M.; Ruiz-Soler, A.; Leo, H.L.; Slevin, M.A.; Badimon, L.; Keshmiri, A. Numerical Assessment of Novel Helical/Spiral Grafts with Improved Hemodynamics for Distal Graft Anastomoses. PLoS ONE 2016, 11, e0165892. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yang, G.; Nan, S.; Qi, Y.; Pang, Y.; Shi, Y. The effect of anastomotic angle and diameter ratio on flow field in the distal end-to-side anastomosis. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2020, 234, 377–386. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Li, M.-C.; Lan, C.-W.; Lee, W.-J.; Lee, C.-J.; Wu, C.-H.; Tang, J.-M.; Niu, Y.-Y.; Lin, Y.-P.; Shiu, Y.-T.; et al. The Anastomotic Angle of Hemodialysis Arteriovenous Fistula Is Associated with Flow Disturbance at the Venous Stenosis Location on Angiography. Front. Bioeng. Biotechnol. 2020, 8, 846. [Google Scholar] [CrossRef]
- Williams, D.; Leuthardt, E.C.; Genin, G.M.; Zayed, M. Tailoring of arteriovenous graft-to-vein anastomosis angle to attenuate pathological flow fields. Sci. Rep. 2021, 11, 12153. [Google Scholar] [CrossRef]
- Koksungnoen, S.; Rattanadecho, P.; Wongchadakul, P. 3D numerical model of blood flow in the coronary artery bypass graft during no pulse and pulse situations: Effects of an anastomotic angle and characteristics of fluid. J. Mech. Sci. Technol. 2018, 32, 4545–4552. [Google Scholar] [CrossRef]
- Dey, S.; Ibtida, T.; Roy, C.K.; Sakib, N. Effect of Varying Anastomosis Angles for Non-Newtonian Pulsatile Blood Flow through Artery Bypass Graft Models: An LES Study. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP 2020), Dhaka, Bangladesh, 5–7 June 2020; pp. 1494–1497. [Google Scholar] [CrossRef]
- Klein, W.M.; Bartels, L.W.; Bax, L.; van der Graaf, Y.; Mali, W.P. Magnetic resonance imaging measurement of blood volume flow in peripheral arteries in healthy subjects. J. Vasc. Surg. 2003, 38, 1060–1066. [Google Scholar] [CrossRef]
- Lorente, S.; Hautefeuille, M.; Sanchez-Cedillo, A. The liver, a functionalized vascular structure. Sci. Rep. 2020, 10, 16194. [Google Scholar] [CrossRef]
- Inumaru, J.; Hara, S.; Hasegawa, T. Future perspective and remarks. In Advances in Power Boilers; Elsevier: Amsterdam, The Netherlands, 2021; pp. 461–478. [Google Scholar] [CrossRef]
- Mouketou, F.N.; Kolesnikov, A. Modelling and simulation of multiphase flow applicable to processes in oil and gas in-dustry. Chem. Prod. Process Model. 2019, 14, 20170066. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, D.; Wang, W.; Zhu, Z. Numerical Investigation and Optimization of the Flow Characteristics of Bend Pipe with Different Bending Angles. Processes 2022, 10, 1510. [Google Scholar] [CrossRef]
- Dutra, R.F.; Zinani, F.S.F.; Rocha, L.A.O.; Biserni, C. Constructal design of an arterial bypass graft. Heat Transf. 2020, 49, 4019–4039. [Google Scholar] [CrossRef]
- Impiombato, A.N.; Zinani, F.S.F.; Rocha, L.A.O.; Biserni, C. Pulsatile flow through an idealized arterial bypass graft: An application of the constructal design method. J. Braz. Soc. Mech. Sci. Eng. 2021, 43, 370. [Google Scholar] [CrossRef]
- ANSYS Inc. ANSYS CFD-Post User’s Guide; Swanson Analysis Systems: Housto, PA, USA, 2017. [Google Scholar]
- Ruvolo, G.; Pisano, C.; Bertoldo, F.; Russo, M.; Verzicco, R.; Nardi, P. A mathematical model to evaluate hemodynamic effects of the graft anastomosis in coronary surgery. Pol. J. Cardio-Thoracic Surg. 2019, 16, 106–108. [Google Scholar] [CrossRef]
- Katritsis, D.; Kaiktsis, L.; Chaniotis, A.; Pantos, J.; Efstathopoulos, E.P.; Marmarelis, V. Wall Shear Stress: Theoretical Considerations and Methods of Measurement. Prog. Cardiovasc. Dis. 2007, 49, 307–329. [Google Scholar] [CrossRef]
- Khan, M.O.; Tran, J.S.; Zhu, H.; Boyd, J.; Packard, R.R.S.; Karlsberg, R.P.; Kahn, A.M.; Marsden, A.L. Low Wall Shear Stress Is Associated with Saphenous Vein Graft Stenosis in Patients with Coronary Artery Bypass Grafting. J. Cardiovasc. Transl. Res. 2020, 14, 770–781. [Google Scholar] [CrossRef]
- Kim, J.T.; Kim, H.; Ryou, H.S. Hemodynamic Analysis on the Anastomosis Angle in Arteriovenous Graft Using Multiphase Blood Model. Appl. Sci. 2021, 11, 8160. [Google Scholar] [CrossRef]
- Javadzadegan, A.; Yong, A.S.C.; Chang, M.; Ng, A.C.C.; Yiannikas, J.; Ng, M.K.C.; Behnia, M.; Kritharides, L. Flow recirculation zone length and shear rate are differentially affected by stenosis severity in human coronary arteries. Am. J. Physiol. Circ. Physiol. 2013, 304, H559–H566. [Google Scholar] [CrossRef]
- Ko, T.; Ting, K.; Yeh, H. Numerical investigation on flow fields in partially stenosed artery with complete bypass graft: An in vitro study. Int. Commun. Heat Mass Transf. 2007, 34, 713–727. [Google Scholar] [CrossRef]
- Sunamura, M.; Ishibashi, H.; Karino, T. Flow patterns and preferred sites of intimal thickening in bypass-grafted arteries. Int. Angiol. 2012, 31, 187–197. Available online: https://europepmc.org/article/med/22466986 (accessed on 6 October 2022). [PubMed]
- Reininger, A.J.; Heinzmann, U.; Reininger, C.B.; Friedrich, P.; Wurzinger, L.J. Flow mediated fibrin thrombus formation in an endothelium-lined model of arterial branching. Thromb. Res. 1994, 74, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Ghista, D.N.; Kabinejadian, F. Coronary artery bypass grafting hemodynamics and anastomosis design: A biomedical engineering review. Biomed. Eng. Online 2013, 12, 129. [Google Scholar] [CrossRef] [PubMed]
- Keynton, R.S.; Rittgers, S.E.; Shu, M.C.S. The Effect of Angle and Flow Rate Upon Hemodynamics in Distal Vascular Graft Anastomoses: An In Vitro Model Study. J. Biomech. Eng. 1991, 113, 458–463. [Google Scholar] [CrossRef]
- Staalsen, N.-H.; Ulrich, M.; Winther, J.; Pedersen, E.M.; How, T.; Nygaard, H. The anastomosis angle does change the flow fields at vascular end-to-side anastomoses in vivo. J. Vasc. Surg. 1995, 21, 460–471. [Google Scholar] [CrossRef]
- Kokkalis, E.; Hoskins, P.R.; Corner, G.A.; Stonebridge, P.A.; Doull, A.J.; Houston, J.G. Secondary Flow in Peripheral Vascular Prosthetic Grafts Using Vector Doppler Imaging. Ultrasound Med. Biol. 2013, 39, 2295–2307. [Google Scholar] [CrossRef]
- Malvè, M.; Finet, G.; Lagache, M.; Coppel, R.; Pettigrew, R.I.; Ohayon, J. Hemodynamic disturbance due to serial stenosis in human coronary bifurcations: A computational fluid dynamics study. In Biomechanics of Coronary Atherosclerotic Plaque: From Model to Patient; Academic Press: Cambridge, MA, USA, 2021; pp. 225–250. [Google Scholar] [CrossRef]
- McGah, P.M.; Leotta, D.F.; Beach, K.W.; Riley, J.J.; Aliseda, A. A Longitudinal Study of Remodeling in a Revised Peripheral Artery Bypass Graft Using 3D Ultrasound Imaging and Computational Hemodynamics. J. Biomech. Eng. 2011, 133, 041008. [Google Scholar] [CrossRef]
- Jackson, M.; Wood, N.B.; Zhao, S.; Augst, A.; Wolfe, J.H.; Gedroyc, W.M.; Hughes, A.D.; Thom, S.A.; Xu, X.Y. Low wall shear stress predicts subsequent development of wall hypertrophy in lower limb bypass grafts. Artery Res. 2009, 3, 32–38. [Google Scholar] [CrossRef]
- Dongha, H.; Hwang, D.; Choi, W.-R.; Baek, J.; Lee, S.J. Fluid-Dynamic Optimal Design of Helical Vascular Graft for Stenotic Disturbed Flow. PLoS ONE 2014, 9, e111047. [Google Scholar] [CrossRef]
- Bernad, S.I.; Bosioc, A.I.; Bernad, E.S.; Craina, M.L. Helical type coronary bypass graft performance: Experimental investigations. Bio-Med. Mater. Eng. 2015, 26, S477–S486. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angle (Degrees) | Total Pressure Drop (Pa) |
|---|---|
| 30 | 474.8 |
| 45 | 498.39 |
| 60 | 526.22 |
| 75 | 554.61 |
| Variable | Data from Literature (One Circular Ridge, Oriented at 180°) | CFD Result (One Elliptical Ridge, Oriented at 180°) | Percentage Difference (%) |
|---|---|---|---|
| Pressure drop (Pa) | 545.86 | 526.22 | 3.66 |
| Secondary velocity (m/s) | 0.022 | 0.024 | 8.70 |
| WSS (Pa) | 2.432 | 2.09 | 15.13 |
| Recirculation Plane 1 (%) | 5.31 | 5.21 | 1.90 |
| Recirculation Plane 2 (%) | 3.52 | 1.00 | 111.50 |
| Configuration | Maximum (Pa) | Area Average (Pa) |
|---|---|---|
| Non-spiral | 4.679 | 0.944 |
| Spiral | 4.663 | 1.067 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apan, J.J.; Tayo, L.; Honra, J. Numerical Investigation of the Relationship between Anastomosis Angle and Hemodynamics in Ridged Spiral Flow Bypass Grafts. Appl. Sci. 2023, 13, 4046. https://doi.org/10.3390/app13064046
Apan JJ, Tayo L, Honra J. Numerical Investigation of the Relationship between Anastomosis Angle and Hemodynamics in Ridged Spiral Flow Bypass Grafts. Applied Sciences. 2023; 13(6):4046. https://doi.org/10.3390/app13064046
Chicago/Turabian StyleApan, Jhon Jasper, Lemmuel Tayo, and Jaime Honra. 2023. "Numerical Investigation of the Relationship between Anastomosis Angle and Hemodynamics in Ridged Spiral Flow Bypass Grafts" Applied Sciences 13, no. 6: 4046. https://doi.org/10.3390/app13064046
APA StyleApan, J. J., Tayo, L., & Honra, J. (2023). Numerical Investigation of the Relationship between Anastomosis Angle and Hemodynamics in Ridged Spiral Flow Bypass Grafts. Applied Sciences, 13(6), 4046. https://doi.org/10.3390/app13064046